
Skin nonmelanocytic tumor
Premalignant / in situ
Squamous cell carcinoma in situ / Bowen disease
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 21 January 2025
Last staff update: 21 January 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma in situ / Bowen disease

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Hamilton C, Ray J, Asadbeigi SN. Squamous cell carcinoma in situ / Bowen disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticcisgeneral.html. Accessed March 30th, 2025.
Definition / general
- Characterized by full thickness involvement of the epidermis by dysplastic squamous cells
- Bowen disease and squamous cell carcinoma in situ (SCCIS) are used interchangeably to describe epidermal SCCIS of both sun damaged and sun protected skin (J Cutan Aesthet Surg 2021;14:449)
Essential features
- Squamous cell carcinoma in situ is squamous cell carcinoma (SCC) confined to the epidermis and superficial adnexal epithelium
- Full thickness epidermal squamous cell dysplasia
- Disordered maturation with atypical keratinocytes (Front Med (Lausanne) 2023;10:1281540)
- No invasion of the underlying dermis (Indian Dermatol Online J 2022;13:177)
Terminology
- Bowen disease
- Intraepidermal carcinoma
- Erythroplasia (of Queyrat)
- If at glans penis (Ann Dermatol 2009;21:419)
ICD coding
Epidemiology
- More frequent in
- White, fair skinned people
- M = F (World J Clin Cases 2019;7:2910)
- > 60 years of age
- Risk factors
- High sun / ultraviolet (UV) exposure
- Immunosuppression
- Arsenic
- Human papillomavirus (HPV) infections (Breast J 2020;26:1234)
Sites
- Can occur anywhere
- More common in sun exposed skin but also occurs in non-sun exposed areas
- Commonly involved areas: head and neck, lower limbs, upper limbs (J Am Acad Dermatol 1992;27:406)
- Less commonly involved areas: subungual, periungual, genital and perianal sites
Pathophysiology
- Poorly characterized
- May often relate to TP53 mutations, which are present in 7 - 45% of SCCIS cases (Biomedicines 2021;9:171)
Etiology
- Multifactorial
- Ultraviolet radiation damages the skin cell nucleic acids, leading to the mutation and cloning of the p53 gene (StatPearls: Intraepidermal Carcinoma [Accessed 9 October 2024])
- Diseases or drugs capable of suppressing immune responses to skin damage also can trigger the mutation of squamous cells
- Arsenic exposure causes oxidative stress, antioxidant depletion, immune dysfunction, genotoxicity, impaired DNA repair and disrupted signal transduction (Toxicol Appl Pharmacol 2023;479:116730)
- HPV in predominantly genital and periungual lesions but it is also reported in extragenital cases
- HPV16 as the most prevalent subtype (Int J Cancer 1983;32:563)
Clinical features
- Usual presentation is a solitary, slow growing, scaly, erythematous patch or plaque
- Variable in size (millimeters to centimeters)
- Can remain unchanged for many years
- Can have a crusting, pigmented or verrucous appearance and can resemble psoriasis
- Dermoscopic features can include scale, glomerular vessels, yellow crust, hemorrhage, hypopigmentation and linear irregular vessels (World J Clin Cases 2019;7:2910)
- Pigmented variants exist and may clinically resemble melanoma (Int J Dermatol 2020;59:e316)
Diagnosis
- Characteristic clinical features
- Definitive diagnosis is made by shave, punch or excisional biopsies (Indian Dermatol Online J 2022;13:177)
Prognostic factors
- ~3 - 5% of all SCCIS lesions progress to invasive SCC (Br J Hosp Med (Lond) 2022;83:1)
- Invasion risk is slightly higher in genital SCCIS (Br J Dermatol 2007;156:11)
- 8 proteins (TNC, FSCN1, SERPINB1, ACTN1, RAB31, COL3A1, COL1A1, CD36) are associated with invasion and metastasis in SCCIS (J Transl Med 2022;20:416)
Case reports
- 32 year old woman with scaly plaque on left hand (J Cutan Aesthet Surg 2021;14:449)
- 48 year old man with erythematous patch on left hand (World J Clin Cases 2019;7:2910)
- 57 year old woman with SCCIS of the left nipple (Breast J 2020;26:1234)
- 85 year old White woman with red scaly plaques (JAAD Case Rep 2022;26:57)
- 90 year old woman with progressively enlarging pink mass (JAAD Case Rep 2024;51:54)
Treatment
- Small, isolated lesions of SCCIS can be treated with surgical excision, curettage and electrodesiccation (C&E), cryosurgery, topical fluorouracil or imiquimod (Cochrane Database Syst Rev 2013;2013:CD007281)
- Large lesions (> 3 cm) may be treated with photodynamic therapy (if available) or topical fluorouracil (J Am Acad Dermatol 2024;90:58)
Clinical images
Contributed by Chad Hamilton, D.O.

Posterior helix
Images hosted on other servers:

Brown scaly patch

Dermoscopy with glomerular vessels
Gross description
- Slightly raised, large, scaly, erythematous plaque with irregular border
- Usually single patch or verrucous growth (J Cutan Aesthet Surg 2021;14:449)
Microscopic (histologic) description
- General histologic features
- By definition, requires full thickness keratinocyte atypia, although may be surrounded by normal keratinocytes
- Also involves the intraepidermal portions of the skin adnexa
- Commonly has parakeratosis and could be associated with hyperkeratosis
- Architectural and cellular atypia, apoptotic cells, individual cell dyskeratosis
- Markedly altered maturation but usually still some surface keratinization and intercellular bridges present
- Marked nuclear atypia, including nuclear hyperchromasia and multinucleation (Breast J 2020;26:1234)
- Numerous mitotic figures, atypical mitotic figures
- May extend into eccrine sweat glands (not considered invasive disease)
- Variable melanin, variable lymphocytic infiltrate
- May have hemangiomatous vascular proliferation, amyloid globules, adnexal differentiation
- Genital lesions: koilocytosis can be present
- Histologic subtypes
- Clear cell variant: cytoplasmic vacuoles; can show pagetoid cells or ground glass cytoplasm (Biomedicines 2021;9:171)
- Pagetoid: single nests of melanocytes with large and clear cytoplasm
- Verrucous (S Afr Med J 1987;71:527)
- Pigmented: has an increase in melanin pigment deposition
- Helpful key phrases
- Eyeliner sign: a layer of cytologically bland keratinocytes with small ovoid nuclei is often present below the atypical keratinocytes, often focal (Am J Dermatopathol 2024;46:193)
- Windswept appearance: disordered cells with loss of polarity (Indian Dermatol Online J 2014;5:526)
Microscopic (histologic) images
Contributed by Jayden Ray, D.O., Chad Hamilton, D.O., Amy Lynn, M.D., Andrey Bychkov, M.D., Ph.D. and Jijgee Munkhdelger, M.D., Ph.D.
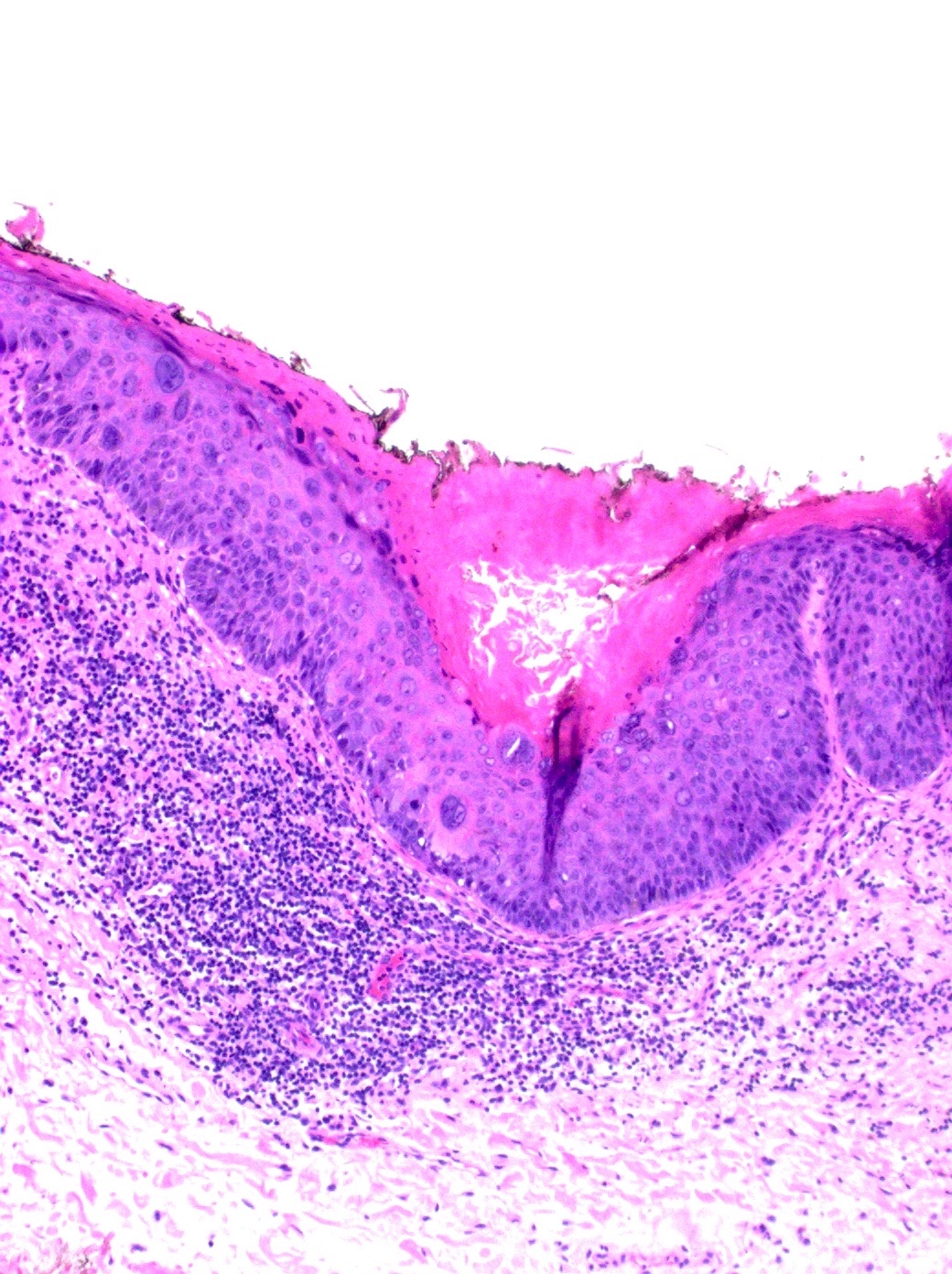
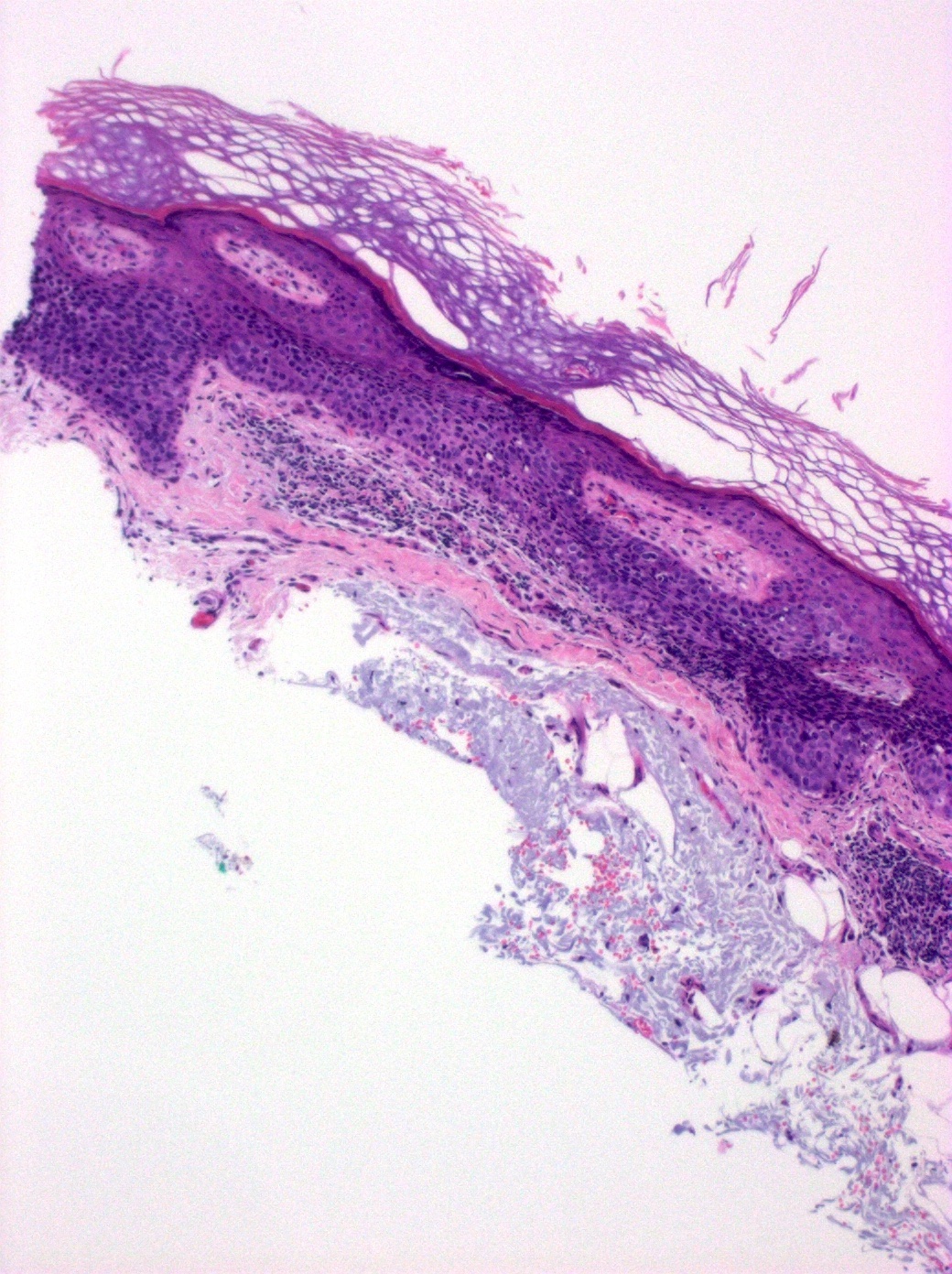
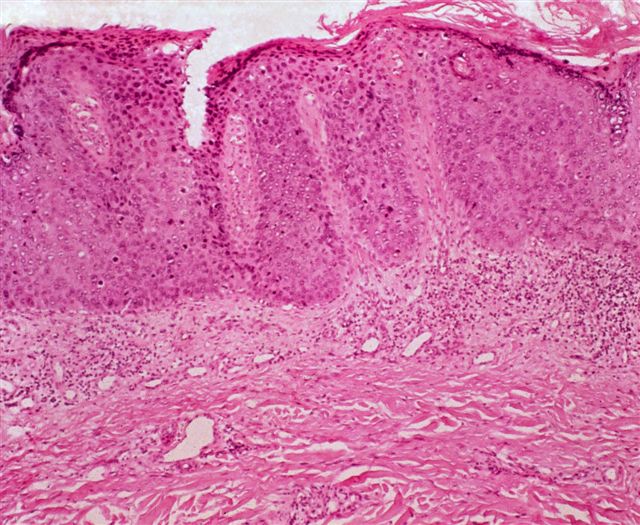
Full thickness atypia

Solar elastosis
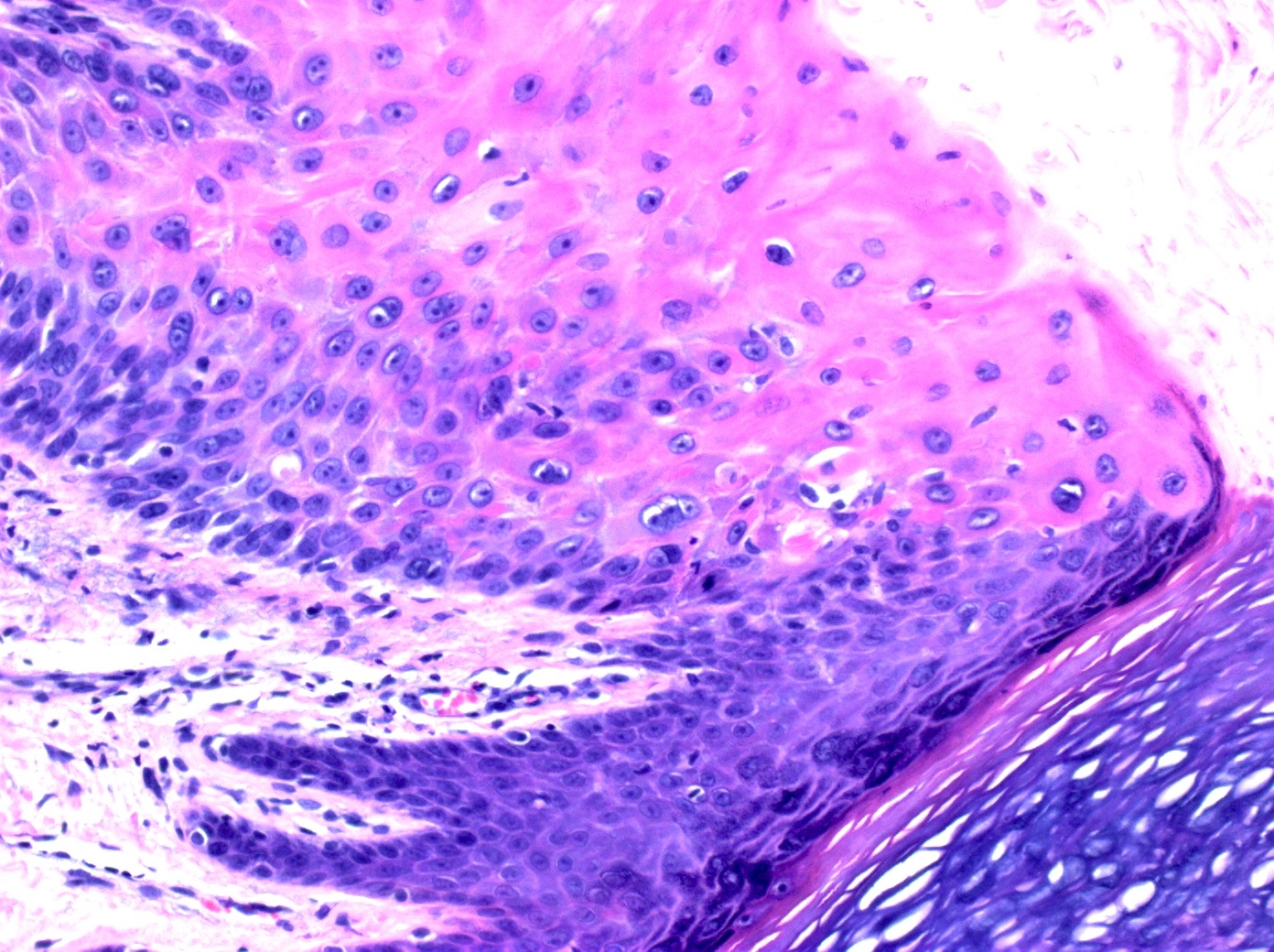
Cytoplasmic vacuoles
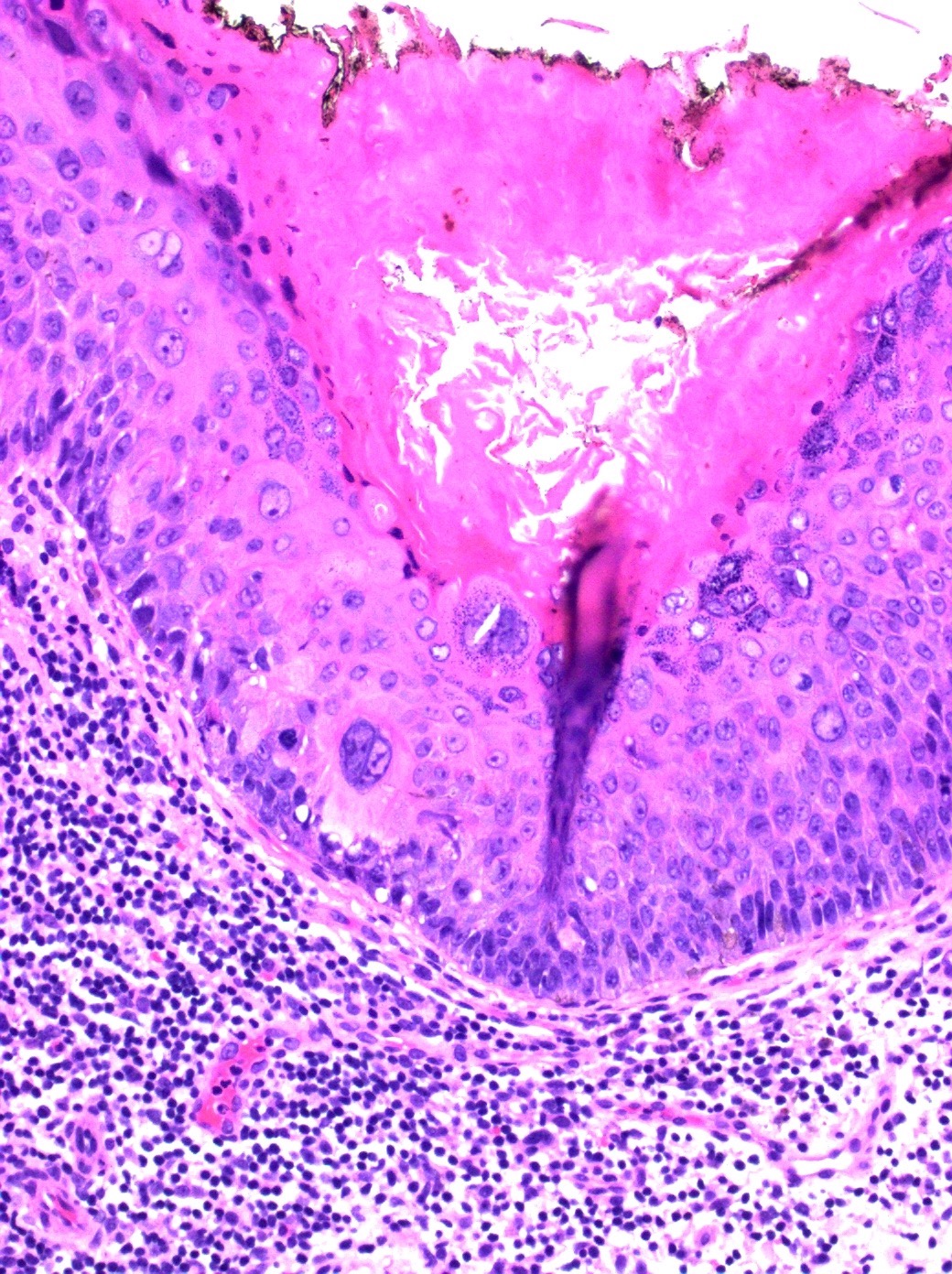
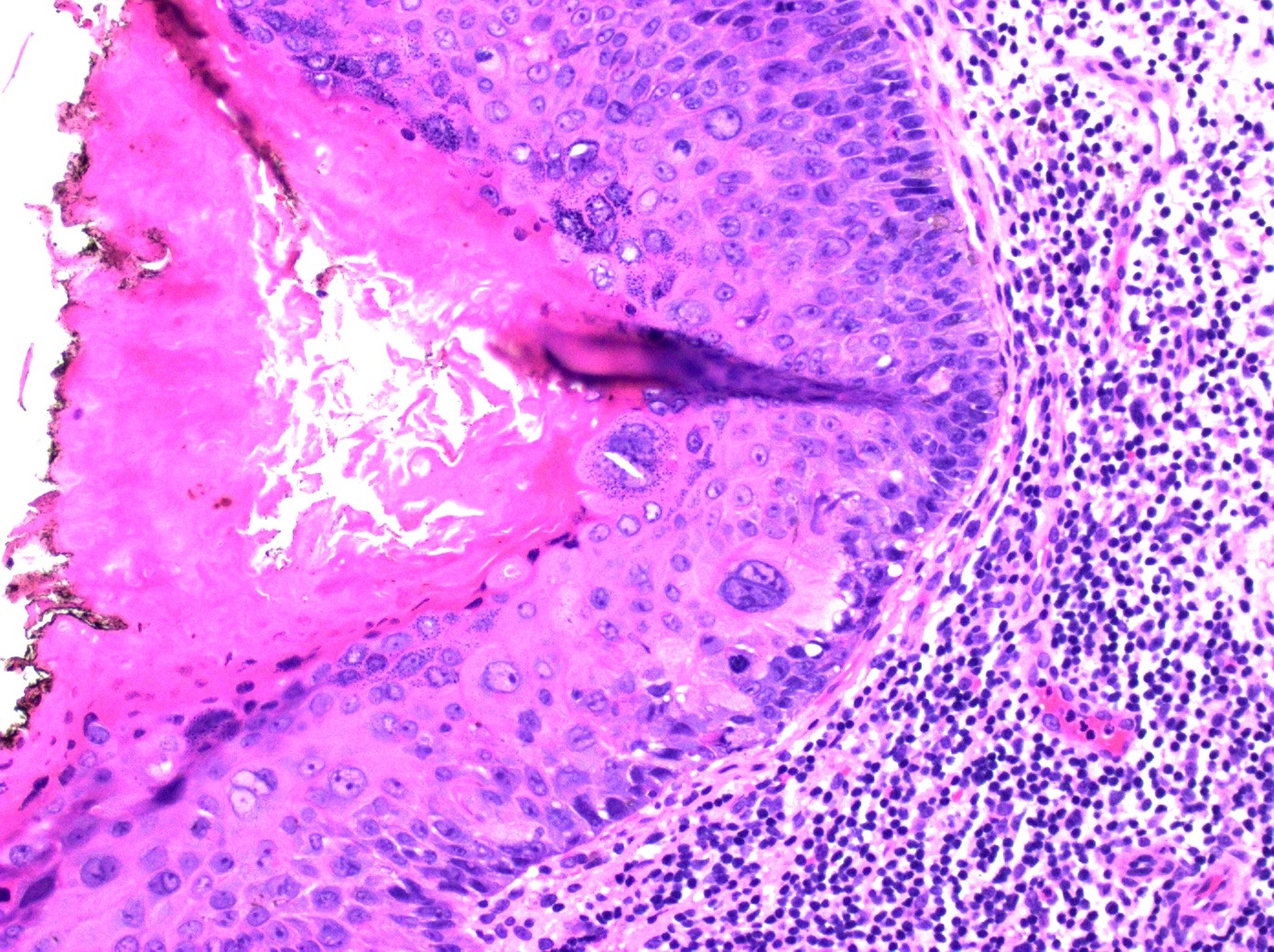
Markedly aberrant maturation
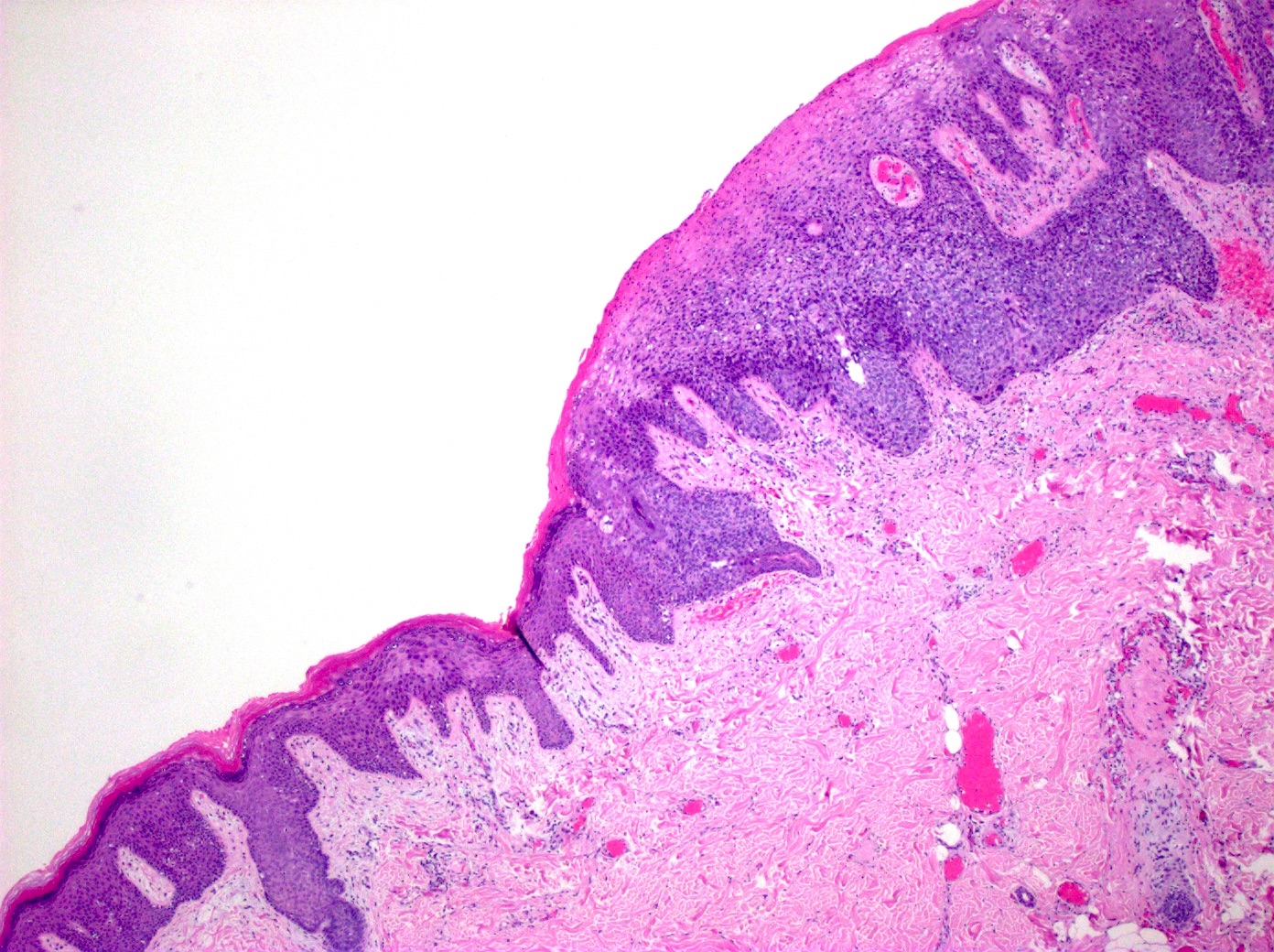
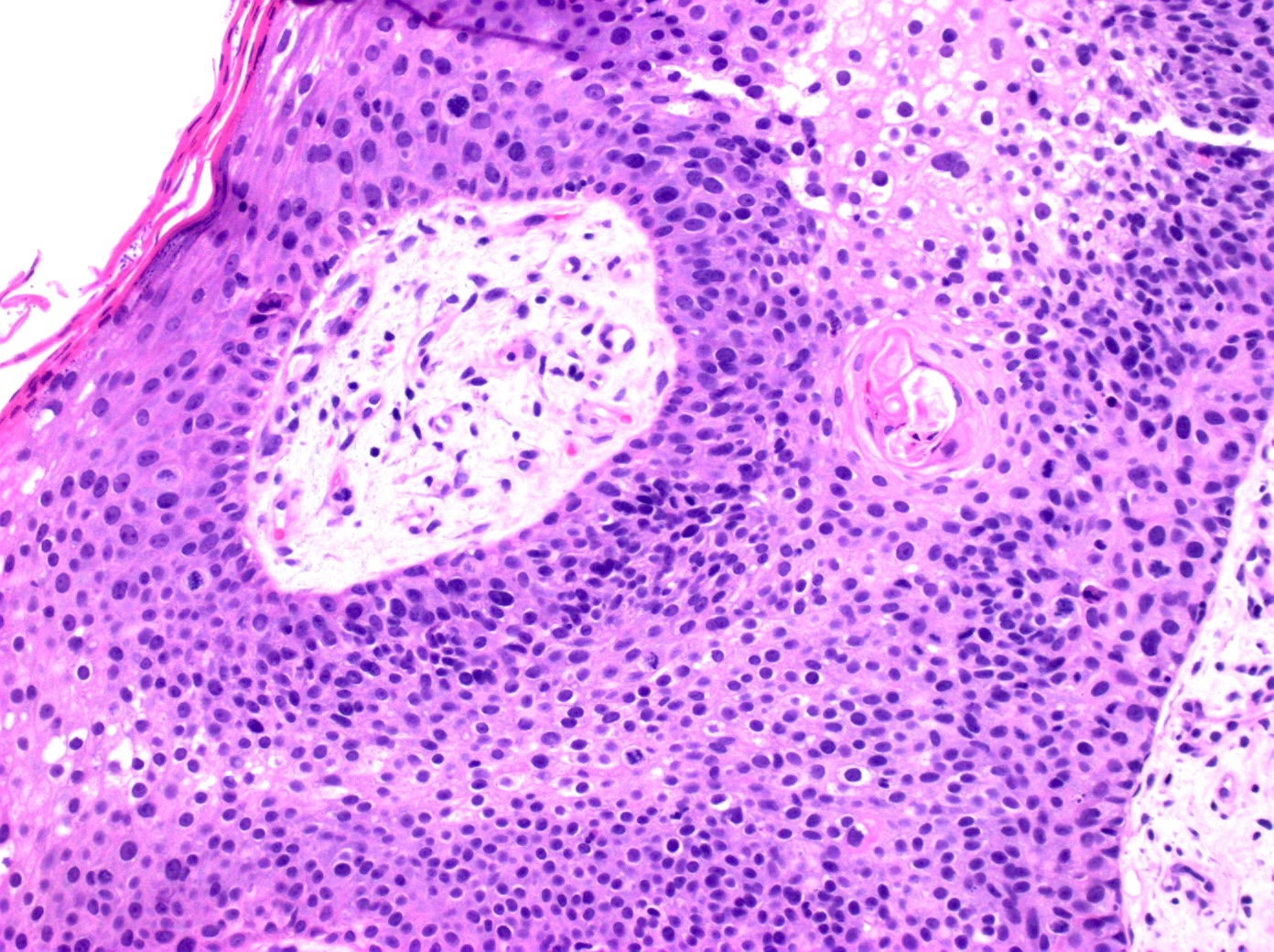
Sharply delineated lesion
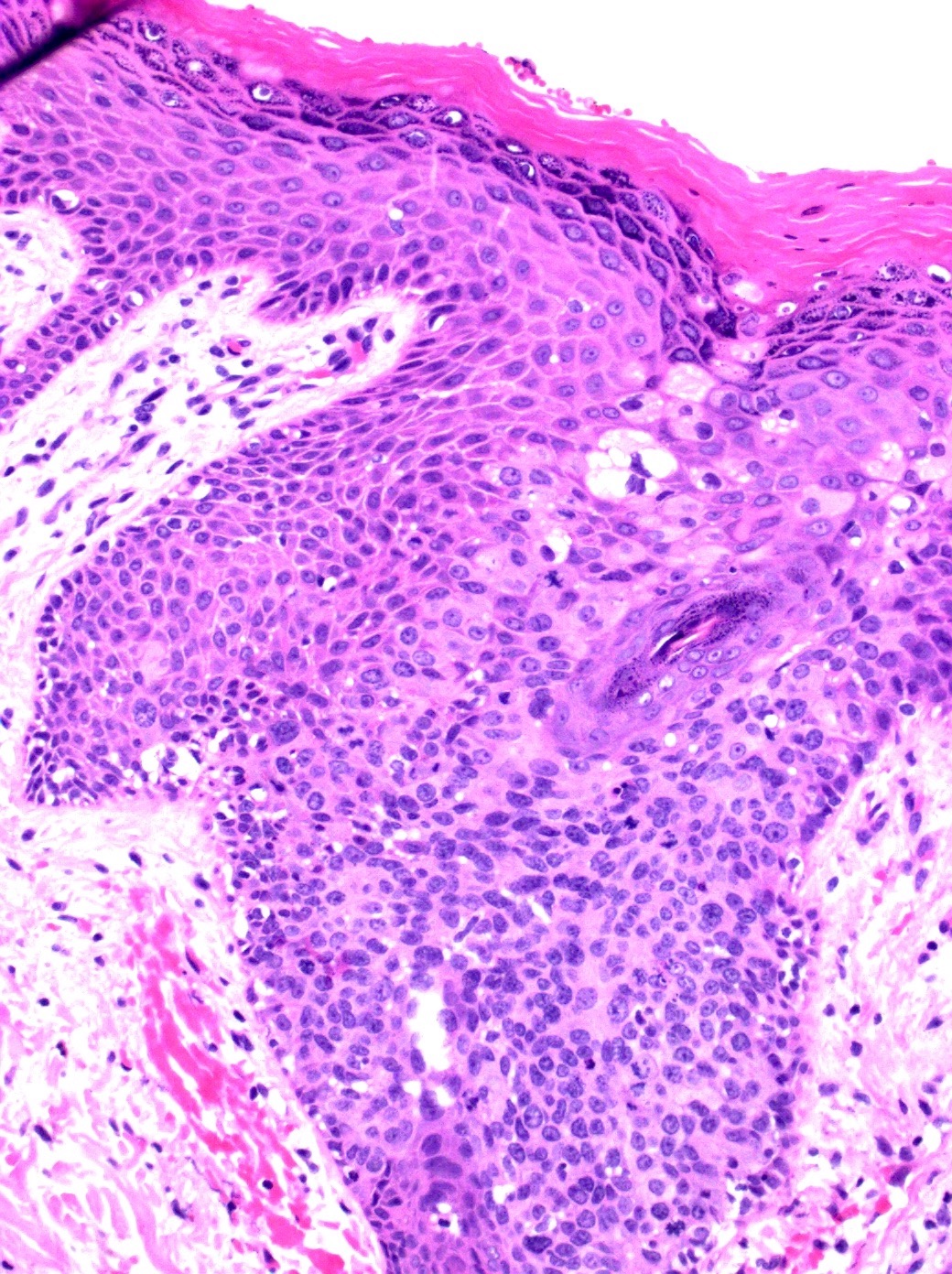
Nuclear atypia
Actinic keratosis for comparison
Actinic keratosis
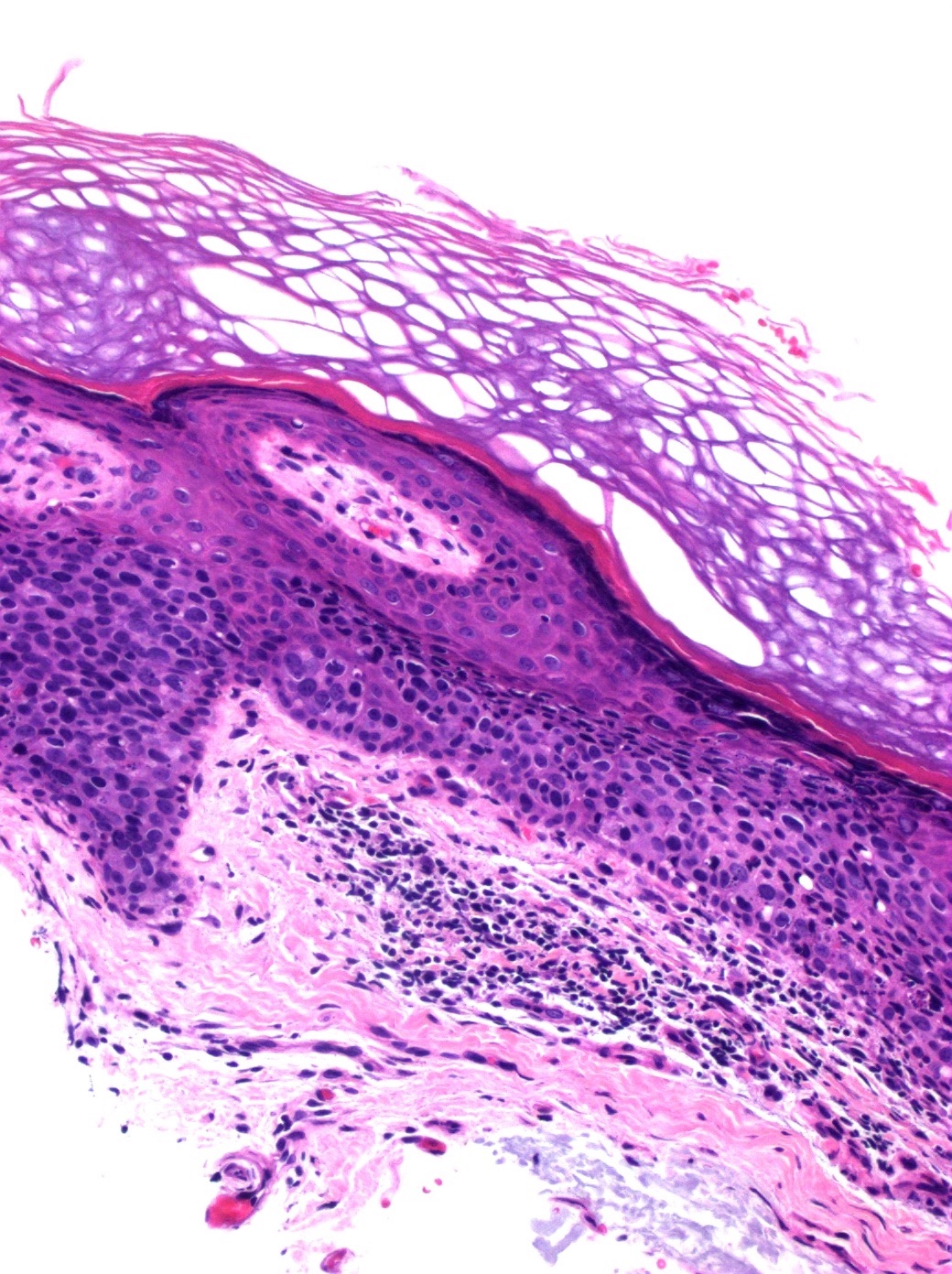
Markedly aberrant maturation
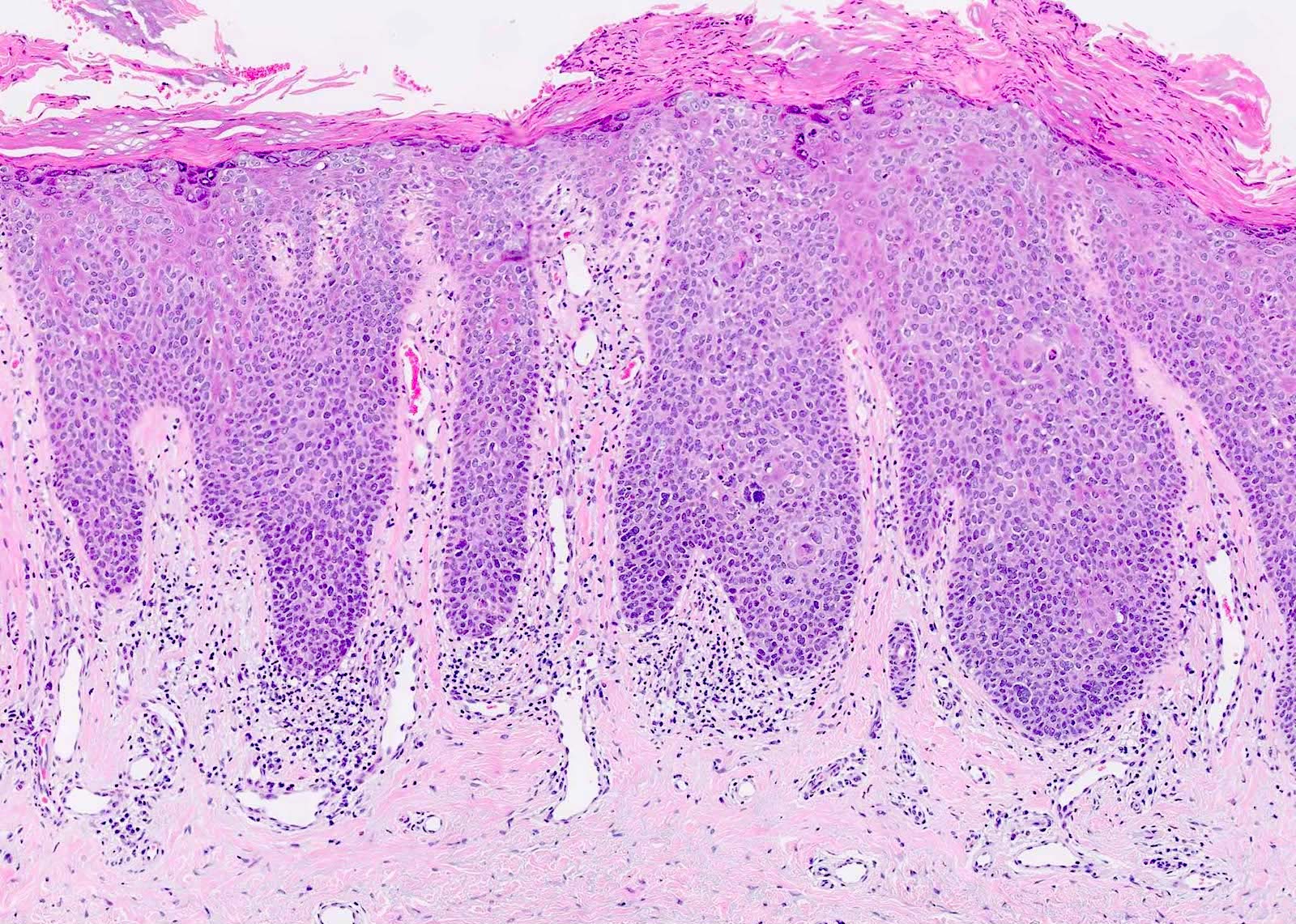
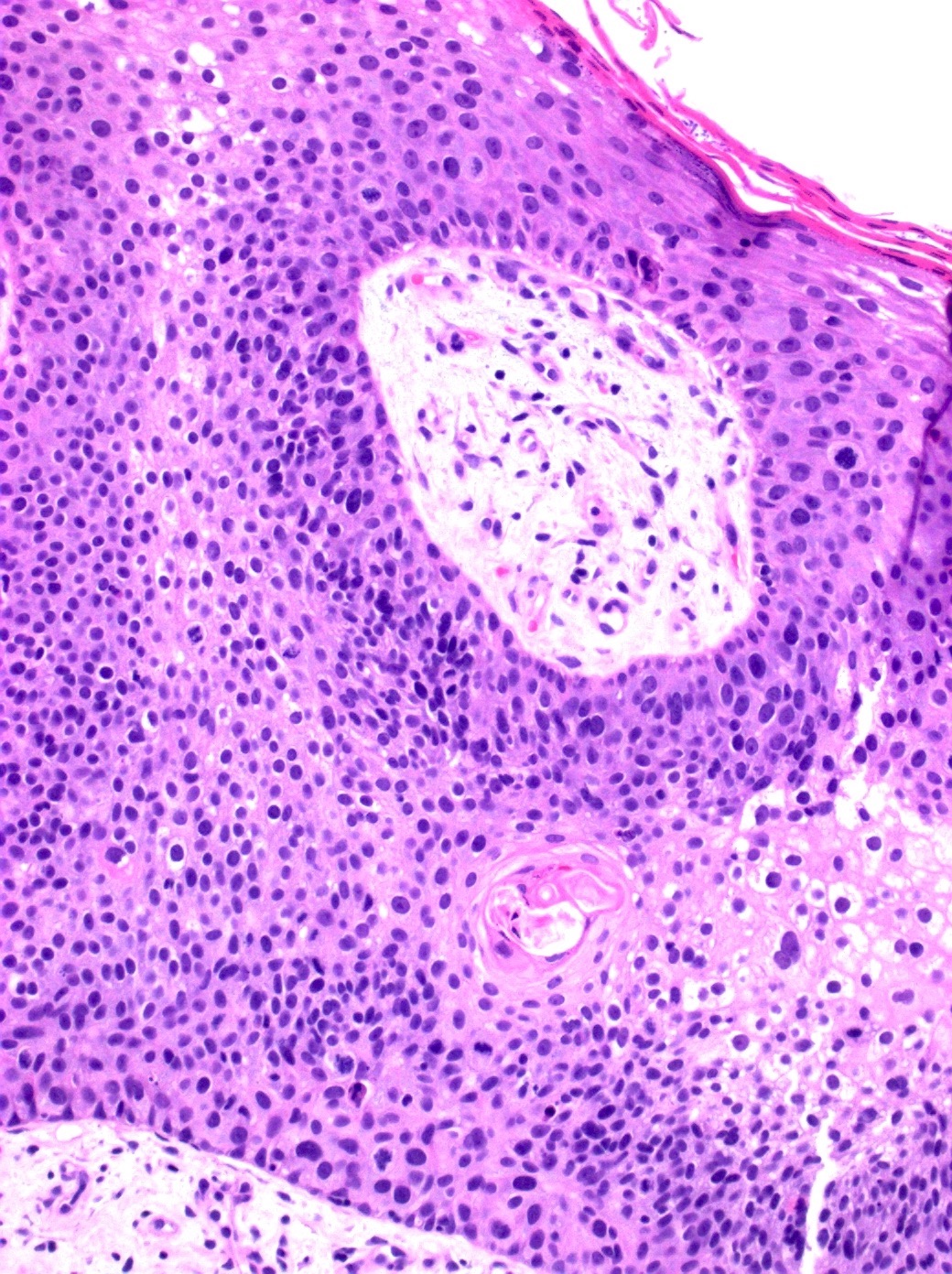
Full thickness atypia
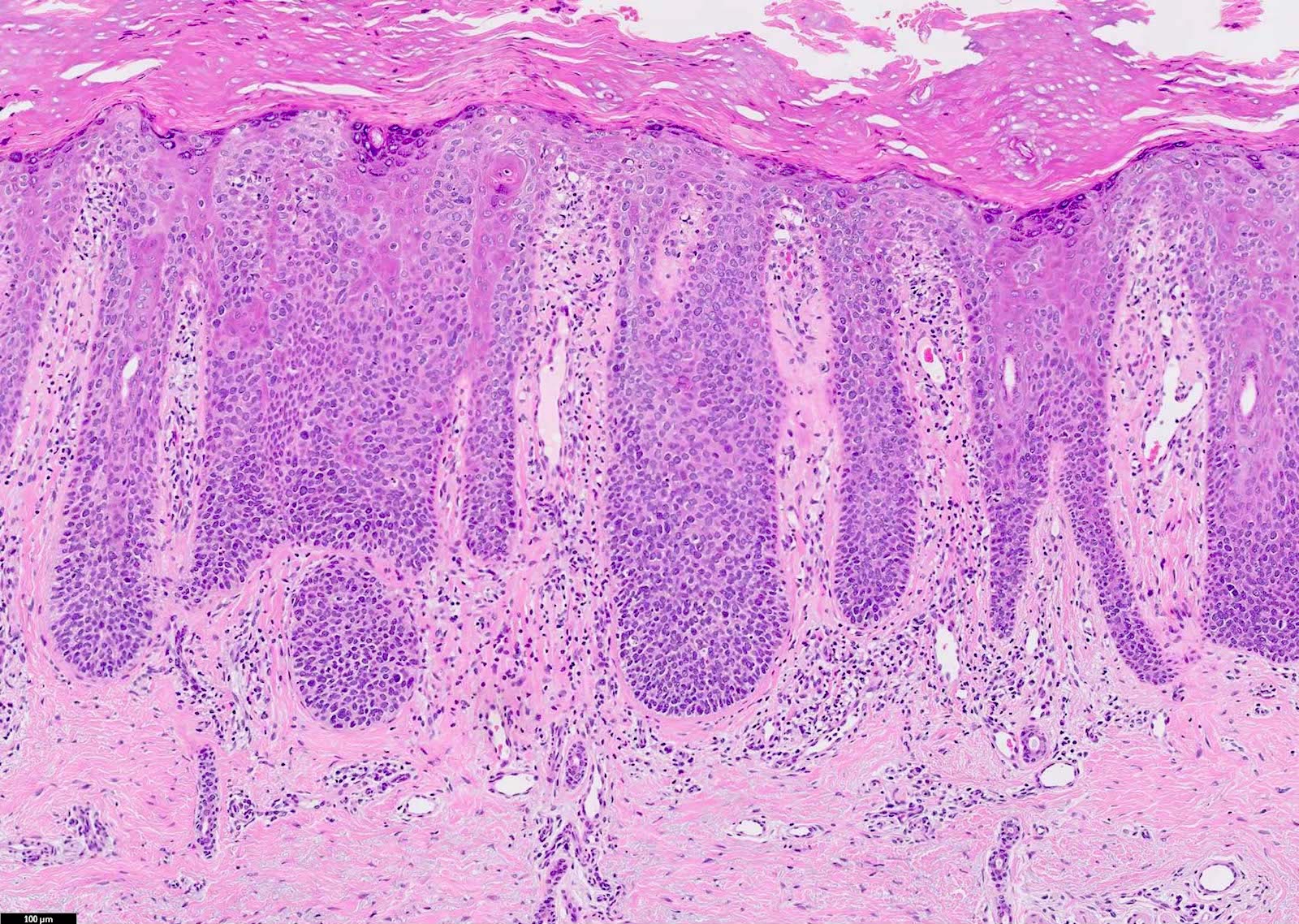
Hyperkeratosis and acanthosis
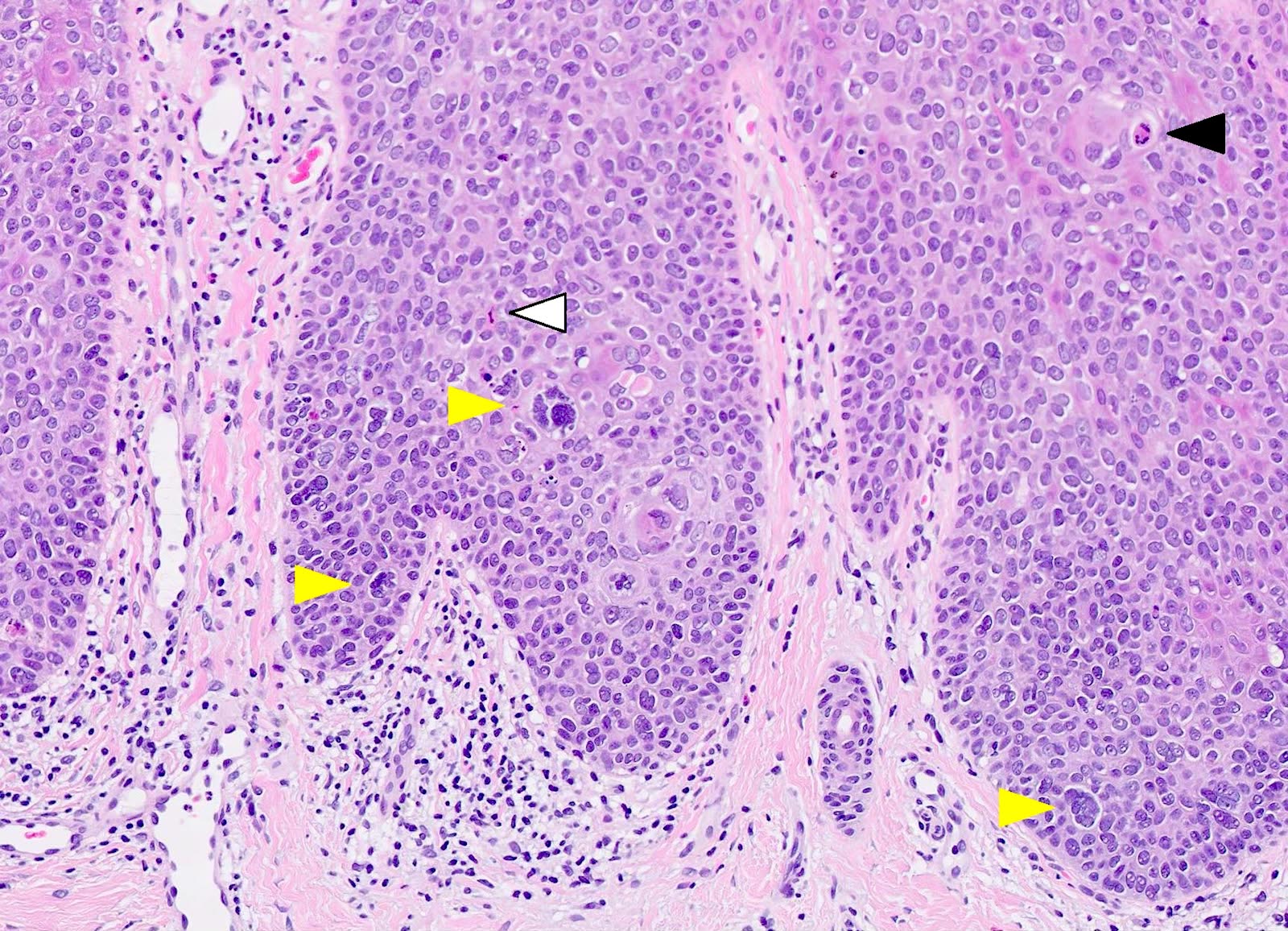
Pleomorphism, multinucleation
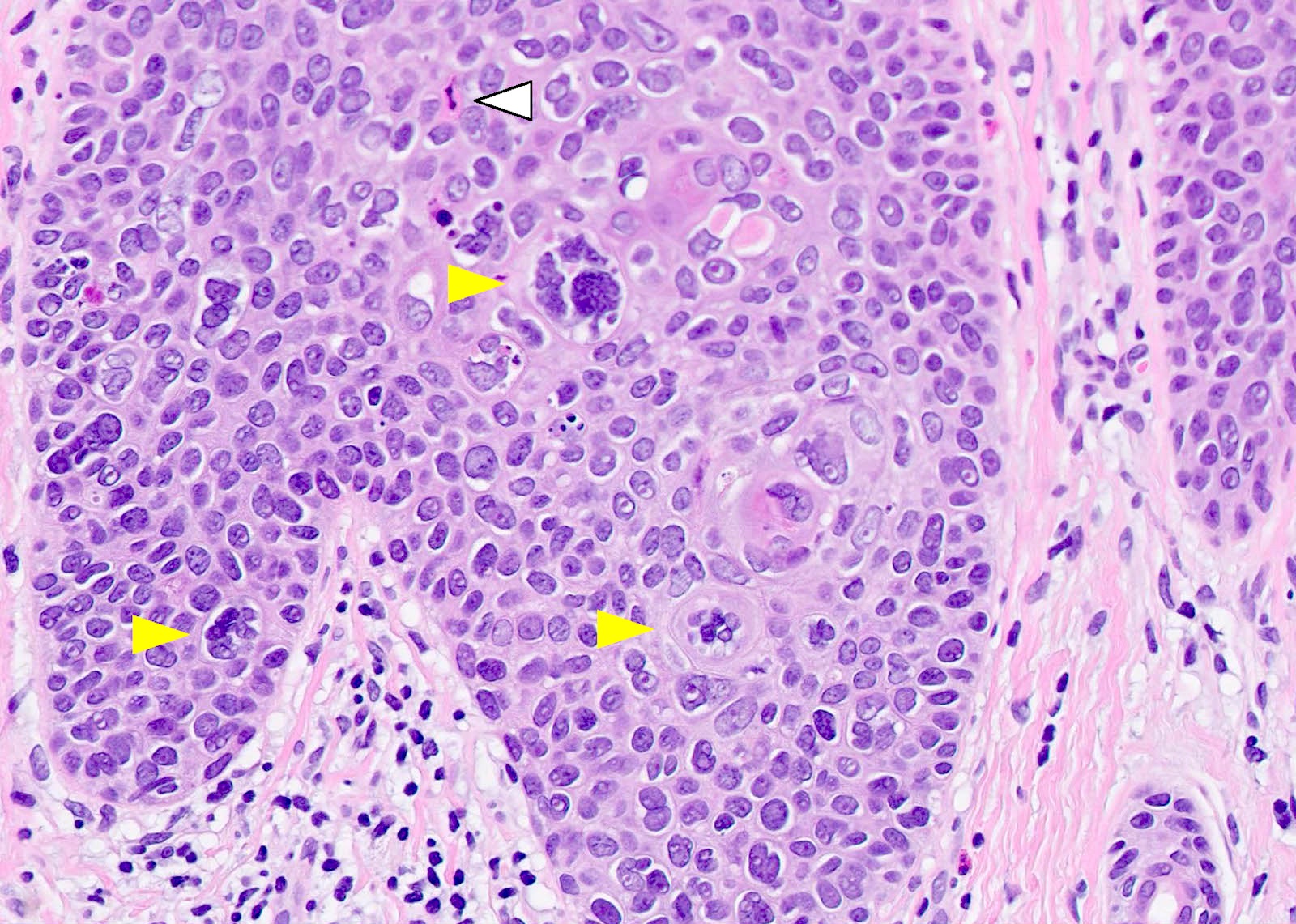
Marked nuclear atypia
Positive stains
- Pancytokeratin
- p40
- p63
- CK5/6
- EMA: variable
- Increased Ki67 expression
- p16: in lesions associated with HPV
- PAS: positive in cases with vacuolated keratinocytes
- Reference: Am J Surg Pathol 2014;38:257
Negative stains
Videos
SCCIS by Dr. Jerad Gardner
Sample pathology report
- Skin, left forearm, shave biopsy:
- Squamous cell carcinoma in situ (Bowen disease)
- Margins are free of involvement
- Microscopic description: The epidermis is acanthotic and exhibits parakeratosis. The keratinocytes display significant atypia and are enlarged with hyperchromatic nuclei. There is a lack of polarity and the atypia involves the full thickness of the epidermis. A mild inflammatory infiltrate is present.
Differential diagnosis
- Actinic keratosis:
- No full thickness atypia of keratinocytes
- Basal epidermal layer in SCCIS shows little to no visible atypia
- SCCIS typically involves the hair follicle, adjacent follicular epithelium and skin adnexa, whereas actinic keratosis does not tend to involve the adnexa
- Superficially invasive squamous cell carcinoma:
- Invasion of tumor cells through the basement membrane into the dermis
- Superficially invasive SCC shows more resemblance to the precursor actinic keratosis lesions rather than SCCIS
- Clonal seborrheic keratosis:
- Borst-Jadassohn phenomenon (sharply defined nests of keratinocytes within the epidermis), which is known as clonal seborrheic keratosis, can be confused with SCCIS
- Minimal atypia / mitotic activity and absence of nuclear crowding help with differentiation
- Paget disease:
- Bowenoid actinic keratosis:
- Can be histologically indistinguishable from SCCIS
- SCCIS and Bowenoid actinic keratosis are different based on the presence or absence of dysplasia in the follicular epithelium; Bowenoid actinic keratosis shows partial thickness atypia with less severity of atypia (J Eur Acad Dermatol Venereol 2010;24:228)
- Melanoma in situ:
- SCCIS can resemble melanoma in situ, especially in cases with pagetoid Bowen disease or Bowen disease with focal clear cell changes
- Immunohistochemistry with melanocytic markers can help with differentiation
Board review style question #1
Which of the following immunohistochemistry stains would help differentiate squamous cell carcinoma in situ (SCCIS) from Paget disease?
- CK7 and CK5/6
- Ki67
- S100 and SOX10
- Synaptophysin and chromogranin
Board review style answer #1
A. CK7 and CK5/6. CK7 will be positive in Paget disease but negative in SCCIS. CK5/6 will be negative in Paget disease but positive in SCCIS. Answer C is incorrect because these are markers for melanoma. Answer D is incorrect because these are neuroendocrine markers. Answer B is incorrect because Ki67 will tell you the proliferation index but will not differentiate SCCIS from Paget disease.
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
Board review style question #2

Which of the following is a risk factor for developing squamous cell carcinoma in situ (SCCIS)?
- Antihistamine use
- Arsenic exposure
- Herpes simplex virus (HSV)
- Lack of time outdoors
Board review style answer #2
B. Arsenic exposure causes oxidative stress and can cause SCCIS. Answer C is incorrect because HSV does not cause SCCIS; however, human papillomavirus (HPV) is a known cause of SCCIS. Answer D is incorrect because a lack of time outdoors is not a known risk factor of SCCIS; however, ultraviolet (UV) radiation is a known risk factor for SCCIS. Answer A is incorrect because antihistamine use is not a known risk factor for SCCIS. Drugs or diseases that cause immunosuppression are, however, a known risk factor for SCCIS.
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
Board review style question #3
What is the key histologic finding that differentiates the image above from actinic keratosis?
- Atypical mitosis
- Dermal lymphocytic infiltrate
- Full thickness atypia
- Multinucleated cells
Board review style answer #3
C. Full thickness atypia. The image displays squamous cell carcinoma in situ (SCCIS). Full thickness atypia is a key characteristic of SCCIS and is needed to differentiate SSCIS from actinic keratosis. Answer A is incorrect because actinic keratosis and SCCIS can display atypical mitosis. Answer D is incorrect because actinic keratosis and SCCIS can both have multinucleated cells. Answer B is incorrect because SCCIS and actinic keratosis can both have dermal lymphocytic infiltrate, which is not a necessary finding for either of these diagnoses.
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
Comment Here
Reference: Squamous cell carcinoma in situ / Bowen disease
