
Skin nonmelanocytic tumor
Benign (nonmelanocytic) epidermal tumors or tumor-like lesions
Seborrheic keratosis
Editorial Board Member: Viktoryia Kozlouskaya, M.D., Ph.D.


Last author update: 17 May 2022
Last staff update: 6 February 2025
Copyright: 2001-2025, PathologyOutlines.com, Inc.
PubMed search: Seborrheic keratosis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Mullins CI, Boswell E. Seborrheic keratosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticSK.html. Accessed March 28th, 2025.
Definition / general
- Common, benign keratinocyte proliferation of middle aged and elderly
Essential features
- Benign
- Clinical: waxy, brown slow growing papule
- Histologic:
- Proliferation of basaloid keratinocytes without atypia
- Acanthosis and hyperkeratosis most often with horn pseudocysts
Terminology
- Senile wart
- Seborrheic wart
ICD coding
- ICD-10: L82 - seborrheic keratosis
Epidemiology
- Most common benign skin tumor
- Age > 50; incidence increases with age
- M = F
- Lighter skinned individuals (StatPearls: Seborrheic Keratosis [Accessed 28 September 2021])
Sites
- Head, neck, trunk (most common)
- Genitals (rare)
- Never on palms, soles or mucosal surfaces
- Reference: StatPearls: Seborrheic Keratosis [Accessed 28 September 2021]
Pathophysiology
- Immature benign keratinocyte proliferation
- Multiple somatic mutations (Oncotarget 2017;8:36639)
- Most common: FGFR3, PIK3CA and HRAS
- Amyloid precursor protein (APP) (Acta Derm Venereol 2018;98:594)
- Expression increases in sun exposed areas and with age
- May contribute to seborrheic keratosis formation
Etiology
- Aging
- Chronic UV light exposure
Clinical features
- Single or multiple
- Papules or plaques with a stuck on appearance (well demarcated edges)
- Brown-black or gray in color
- Waxy or greasy with cerebriform surface
- Millimeters, up to a centimeter
- Larger have been reported (rare)
- Slow growing
- Irritated / inflamed seborrheic keratosis (World J Nucl Med 2021;20:309)
- Can be irregular and ulcerated (mimics carcinoma)
- Dermatosis papulosa nigra (StatPearls: Dermatosis Papulosa Nigra [Accessed 3 May 2022])
- Multiple seborrheic keratosis on the face (usually cheeks)
- Present in adolescents
- More common those of Asian and African descent
- Leser-Trélat sign: (Cleve Clin J Med 2017;84:918)
- Sudden appearance of multiple seborrheic keratoses, rapid increase in size, pruritic
- Paraneoplastic phenomenon typically associated with gastrointestinal adenocarcinoma
Diagnosis
- Clinical:
- Dermoscopy: small keratin filled cysts, fissures, ridges, small vessels with perivascular halo (F1000Res 2019;8:1520)
- Biopsy often performed on irritated lesions or those with rapid growth (Ann Dermatol 2016;28:152)
- Histologic findings confirm diagnosis
Prognostic factors
- Benign
- Leser-Trélat sign may indicate underlying malignancy
Case reports
- 16 year old boy with multiple brown-black, oval shaped, stuck on lesions on his face (Clin Case Rep 2023;11:e7697)
- 49 year old woman with a slowly growing papule (Chin Med J (Engl) 2020;133:2139)
- 51 year old man with sudden onset of multiple seborrheic keratoses (Cleve Clin J Med 2021;88:428)
- 62 year old woman with a cheek lesion (Int J Surg Case Rep 2021;84:106175)
- 65 year old man with an auricular mass (Ear Nose Throat J 2019;98:560)
Treatment
- Not necessary (StatPearls: Seborrheic Keratosis [Accessed 28 September 2021])
- Usually for cosmetics or patient preference
- Cryotherapy (most common)
- Superficial curettage, excision
- Topical hydrogen peroxide solution
Clinical images
Images hosted on other servers:

Papules

Sharply circumscribed

Leser-Trélat sign
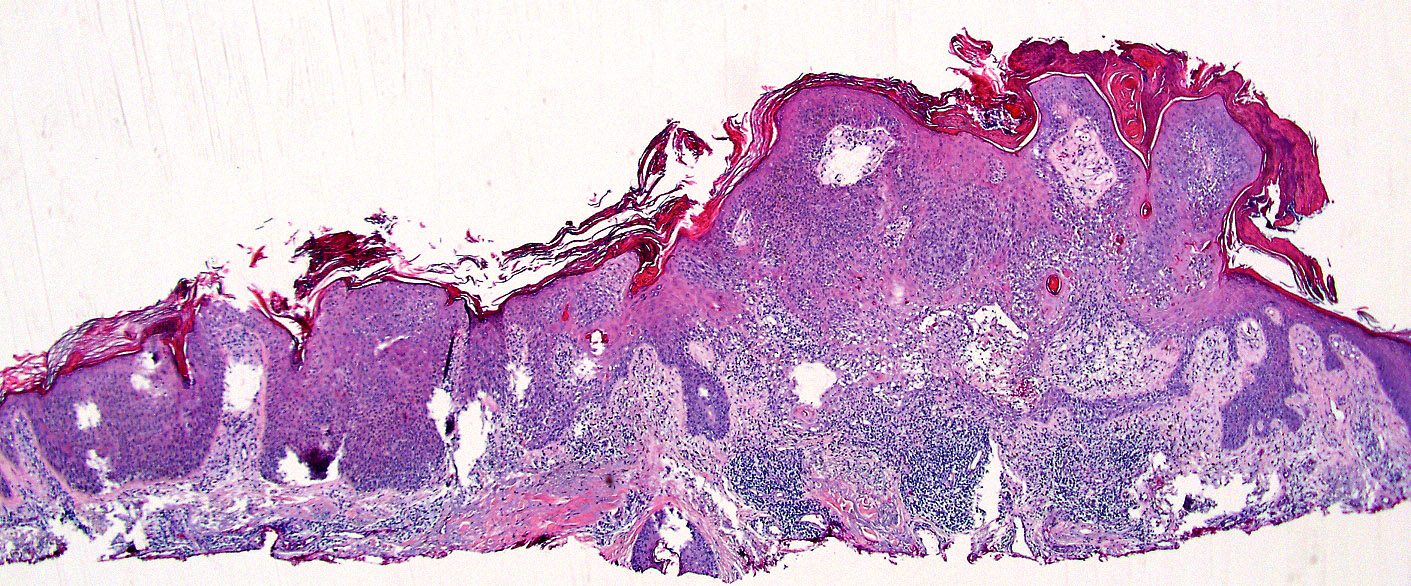
Microscopic (histologic) description
- General (shared) features:
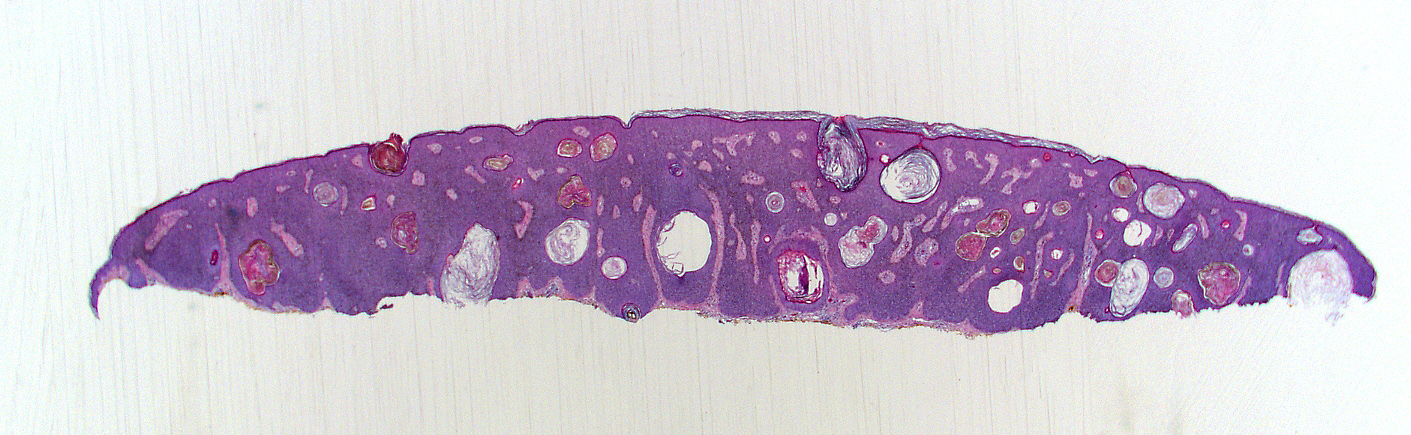
- Intraepidermal, well demarcated edges with a flat base
- String sign: can draw a horizontal line along the base of the lesion
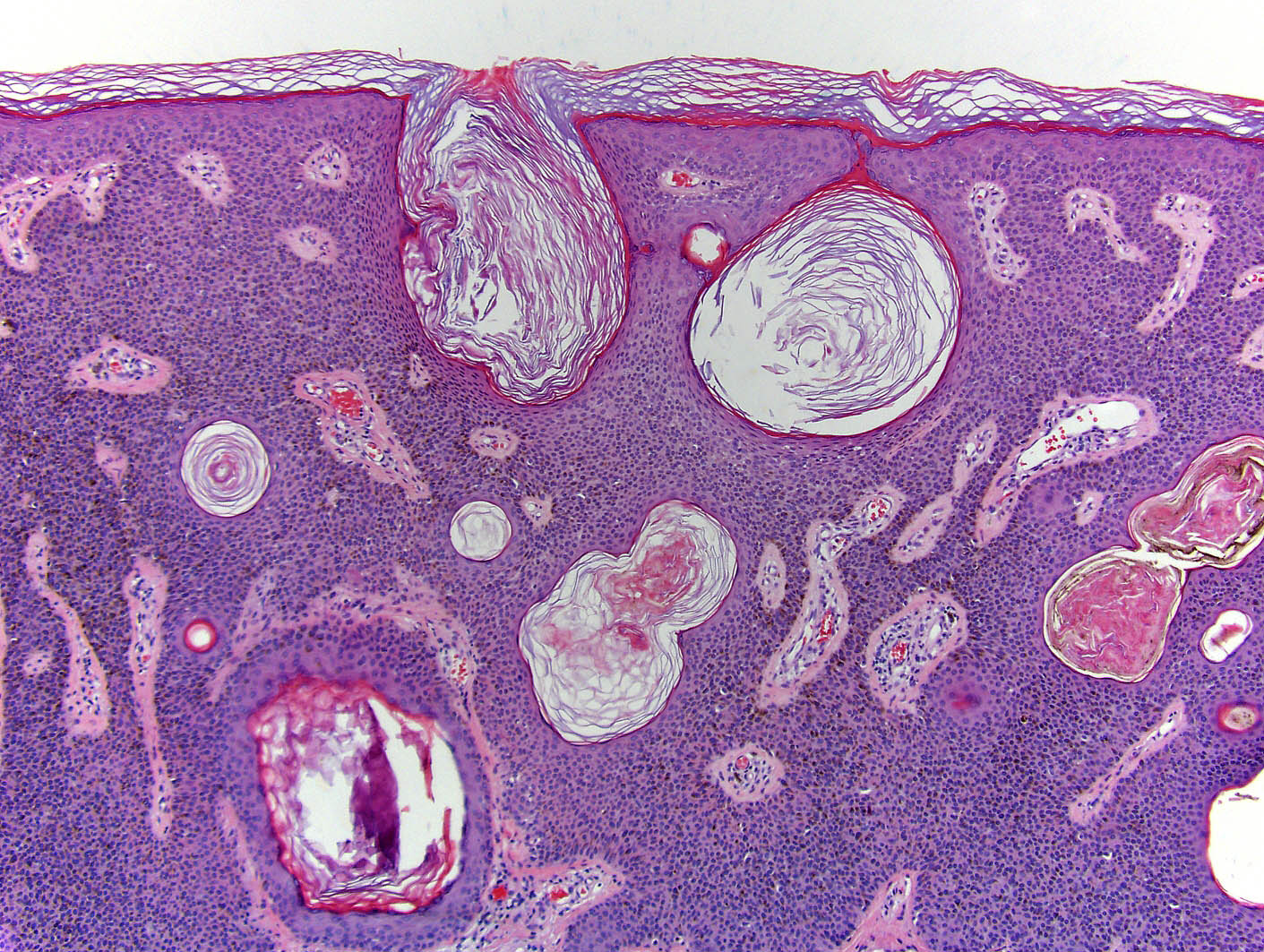
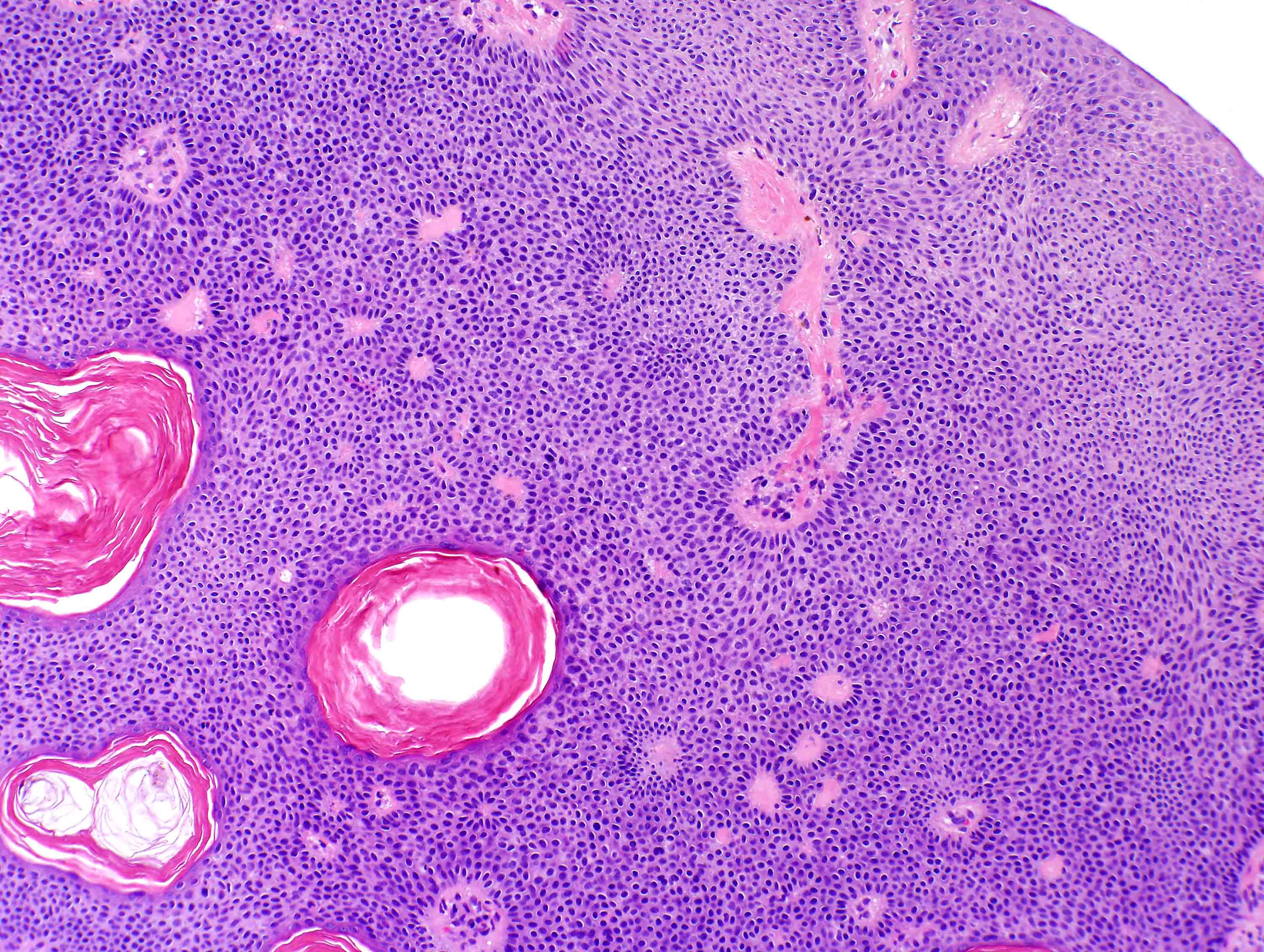
- Basaloid keratinocyte proliferation without dysplasia
- Hyperkeratotic with horn pseudocyst formation (intralesional cysts of loose keratin)
- Multiple variants (no clinical or prognostic significance)
- Often overlapping features
- Intraepidermal, well demarcated edges with a flat base
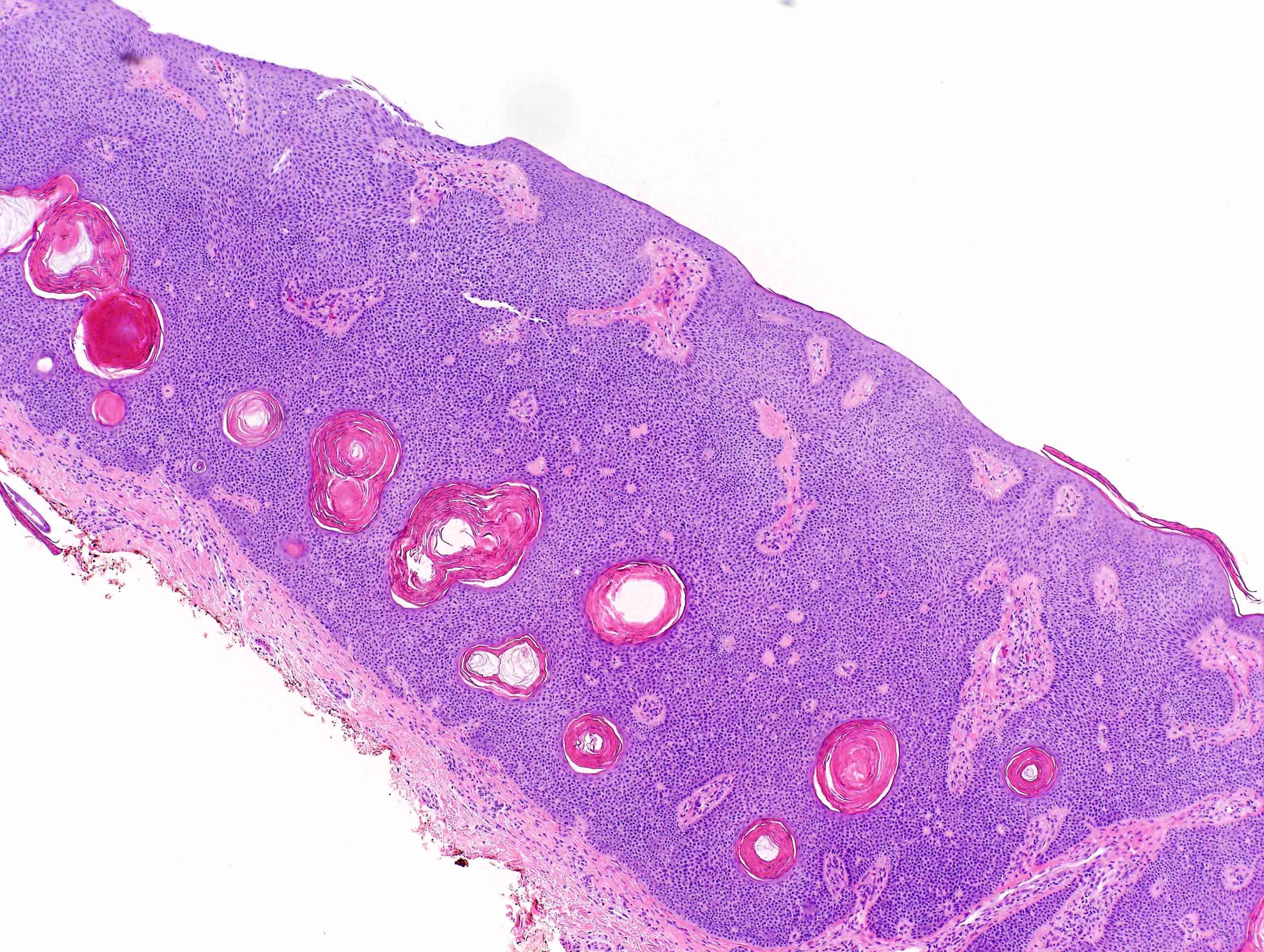
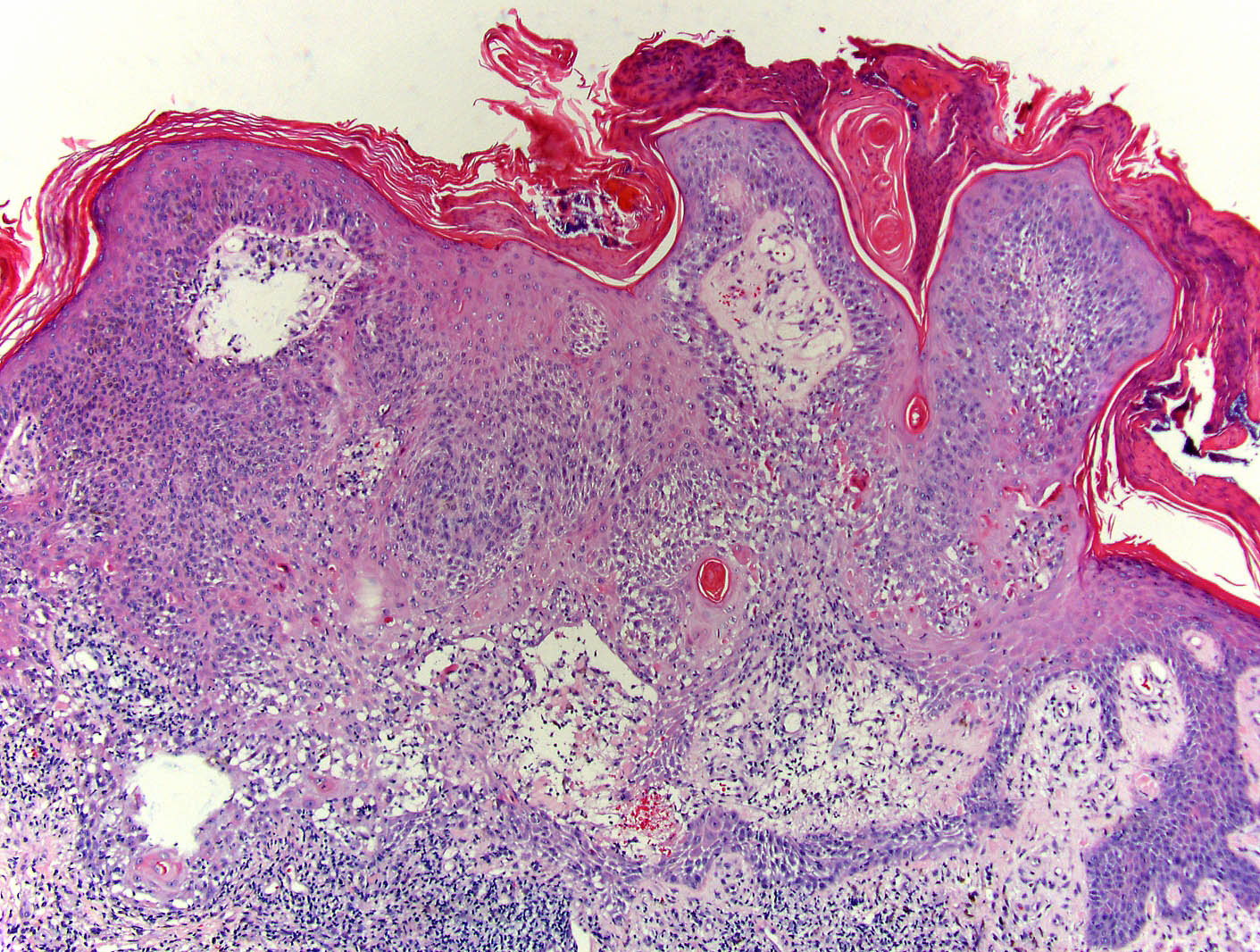
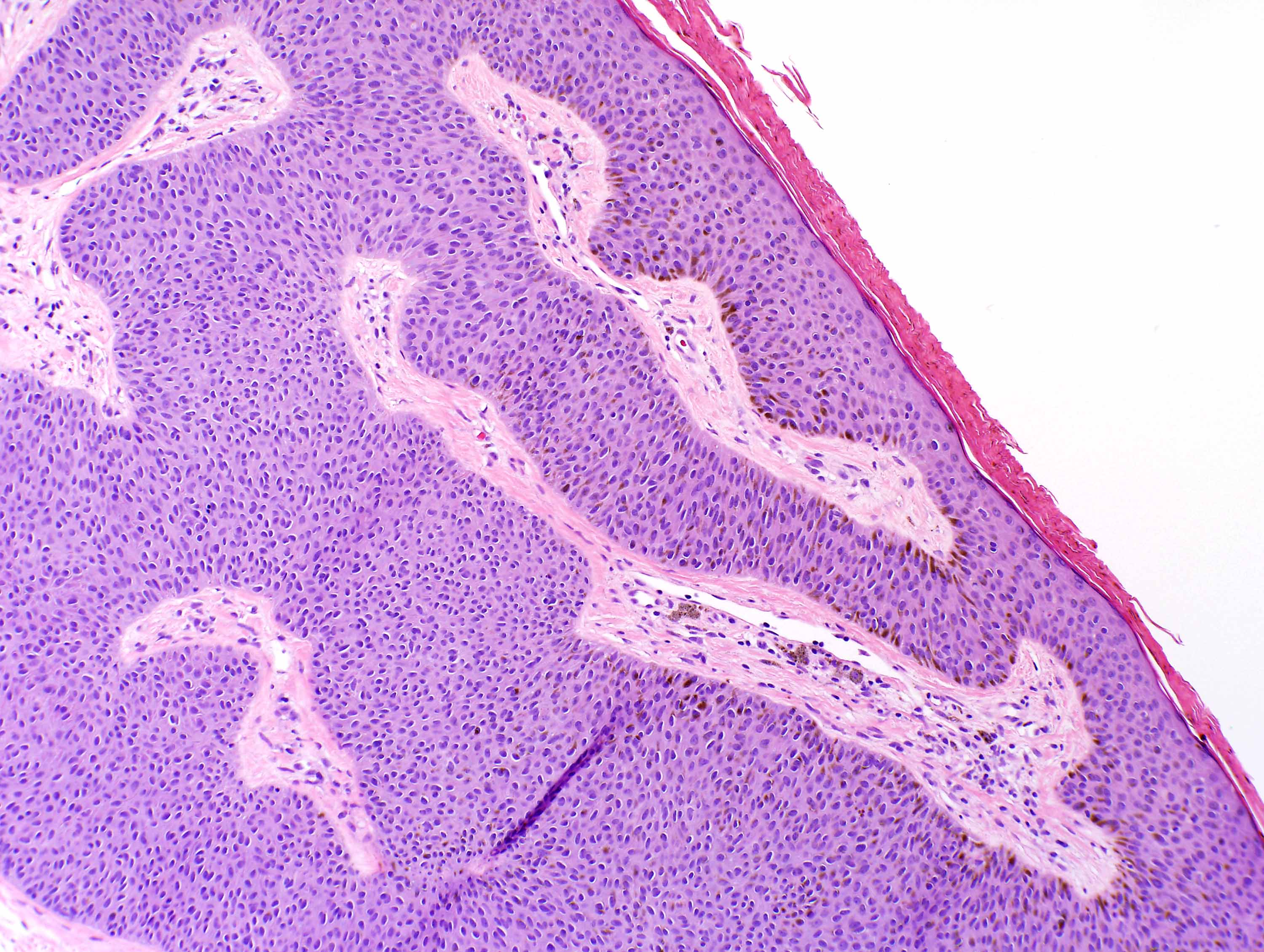
- Acanthotic type:
- Most common (Ann Dermatol 2016;28:152)
- Epidermis expanded by wide bands of keratinocytes
- Keratotic (papillomatous) type (Indian J Sex Transm Dis AIDS 2017;38:176):
- Marked hyperorthokeratosis and papillomatosis
- Can form a cutaneous horn
- Reticulated (adenoid) type:
- Thin, anastomosing strands of basaloid cells
- Small horn cysts
- May have increased pigment
- Clonal type (Dermatol Pract Concept 2015;5:5, Pan Afr Med J 2019;34:54):
- Pale basaloid keratinocytes in nests (Borst-Jadassohn phenomenon)
- Horn pseudocysts may be absent
- Irritated type (Arch Plast Surg 2017;44:570, Dermatol Online J 2019;25:13030):
- Squamous metaplasia and whorled squamous eddies
- Reactive squamous atypia
- Scattered keratinocyte apoptosis and dyskeratosis
- Spongiosis
- Scale crust and parakeratosis in the stratum corneum
- Lichenoid infiltrate in the superficial dermis (variable)
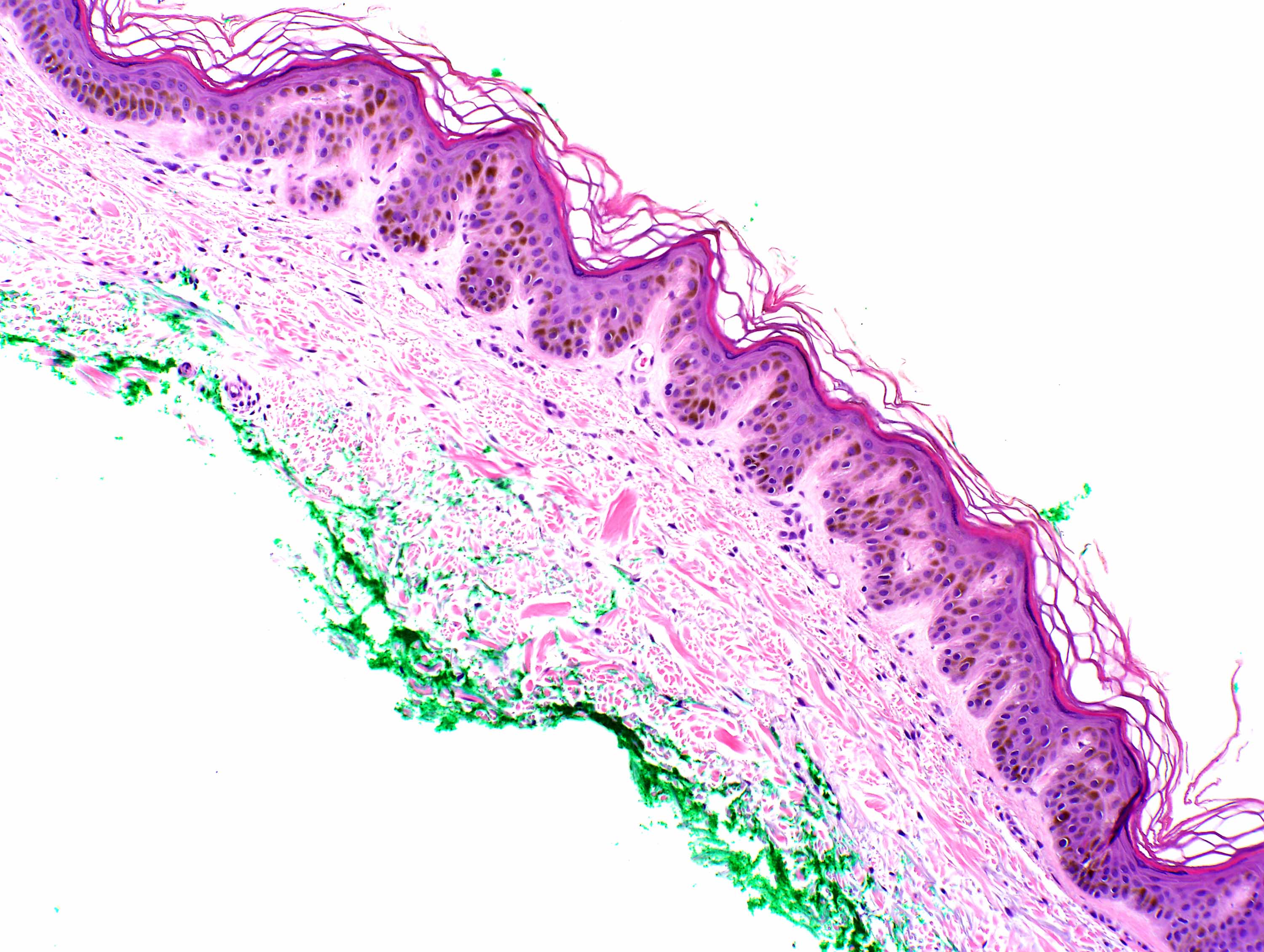
- Pigmented:
- Increased melanin pigmentation in the keratinocytes
- Increased melanophages, mostly in the basal layer
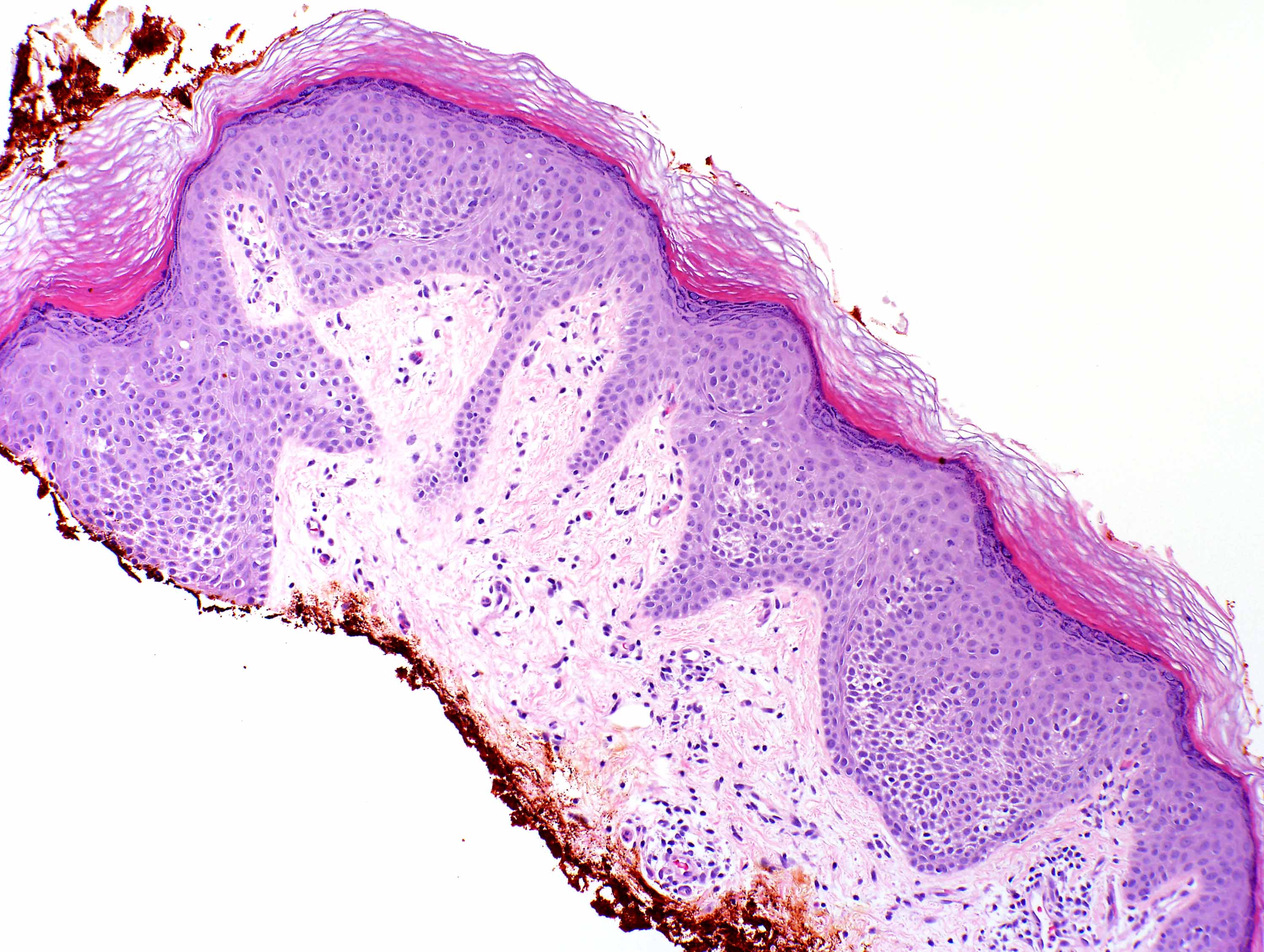
- Macular:
- Minimal / mild acanthosis
- Absent horn pseudocysts
- Usually basal pigmentation increased
Microscopic (histologic) images
Contributed by Sara Shalin, M.D., Ph.D. and Caroline I. Mullins, M.D.
Acanthotic (regular)
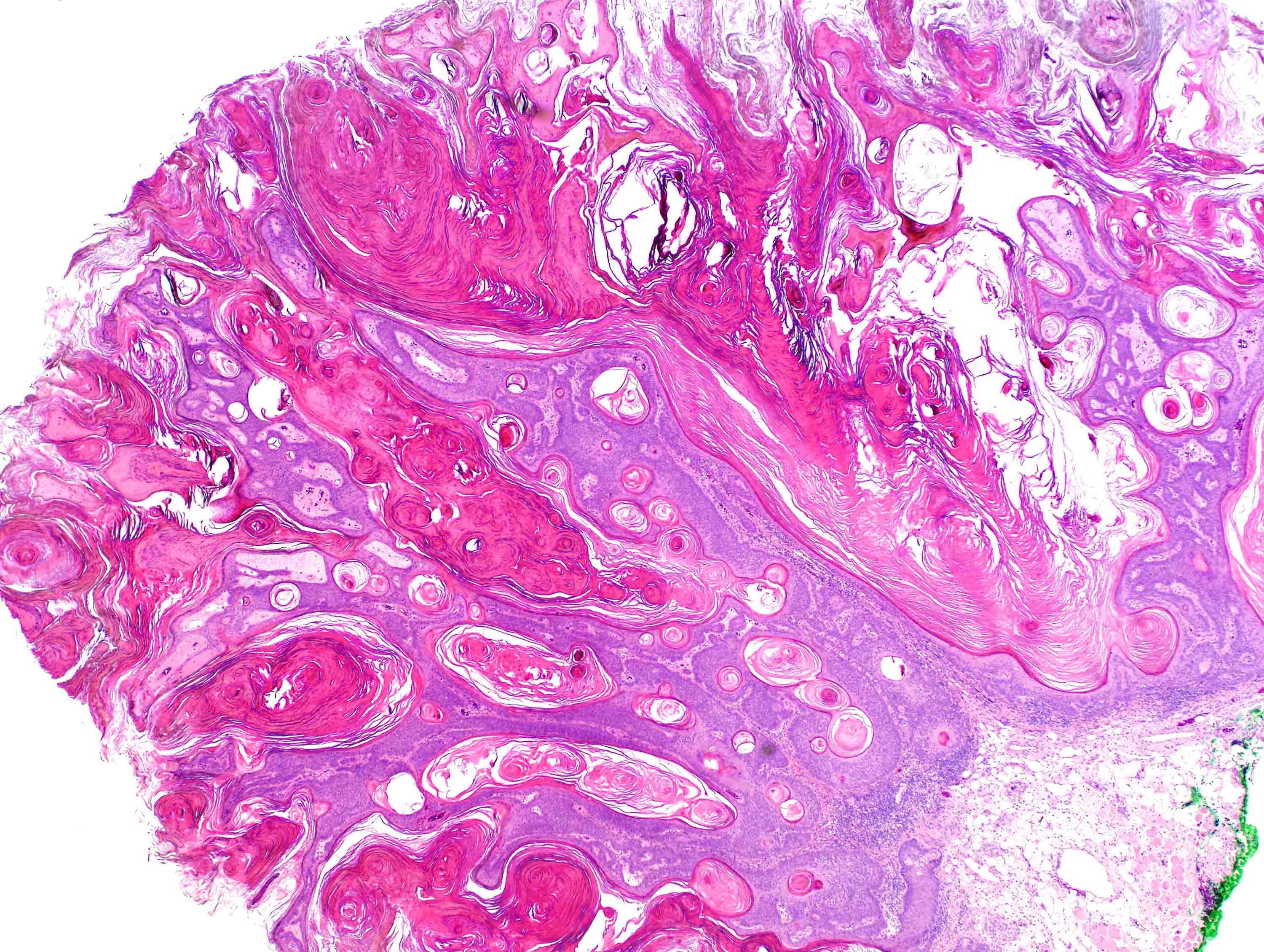
Hyperkeratosis

Papillomatosis without atypia
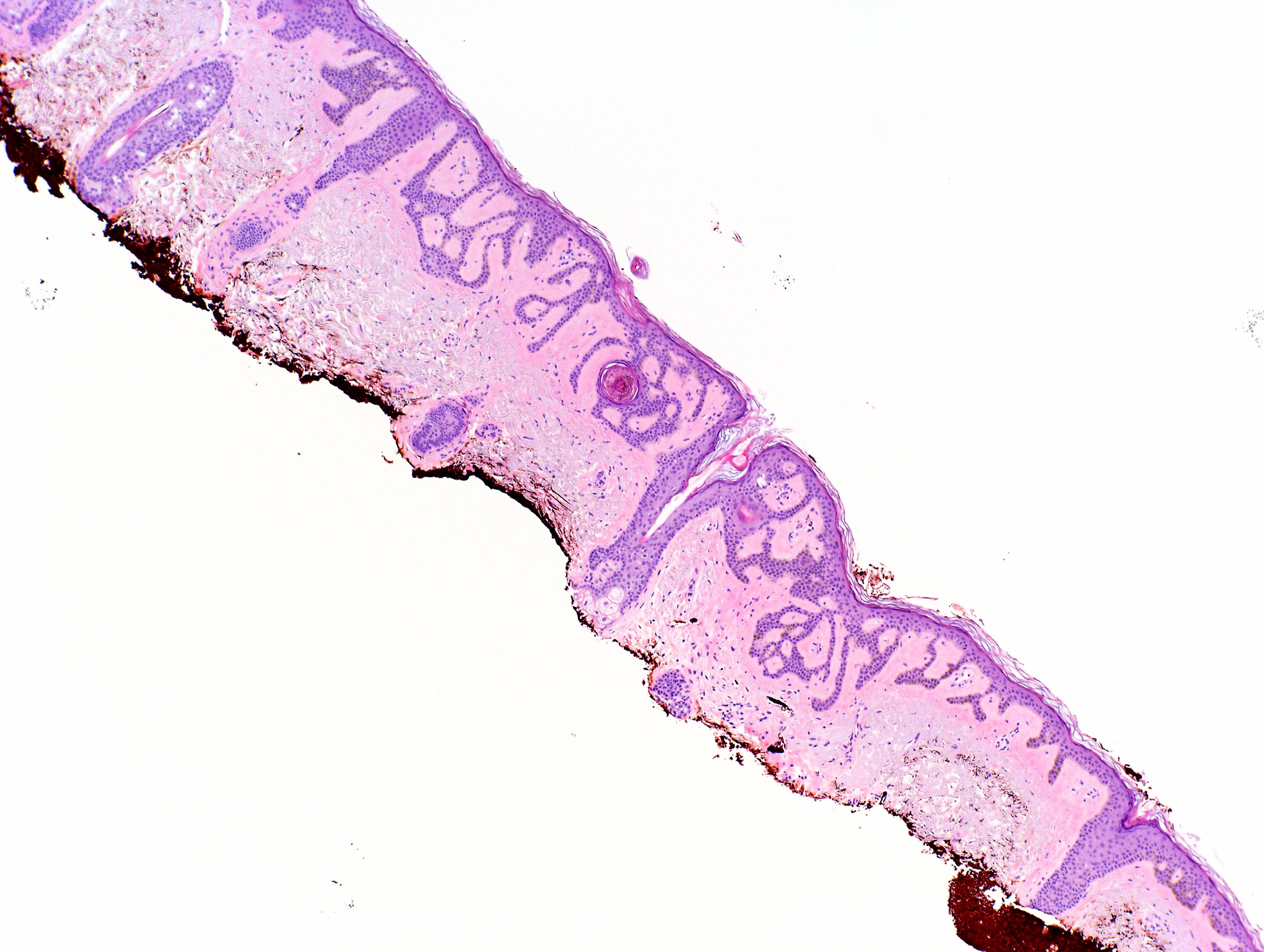
Reticulated pattern
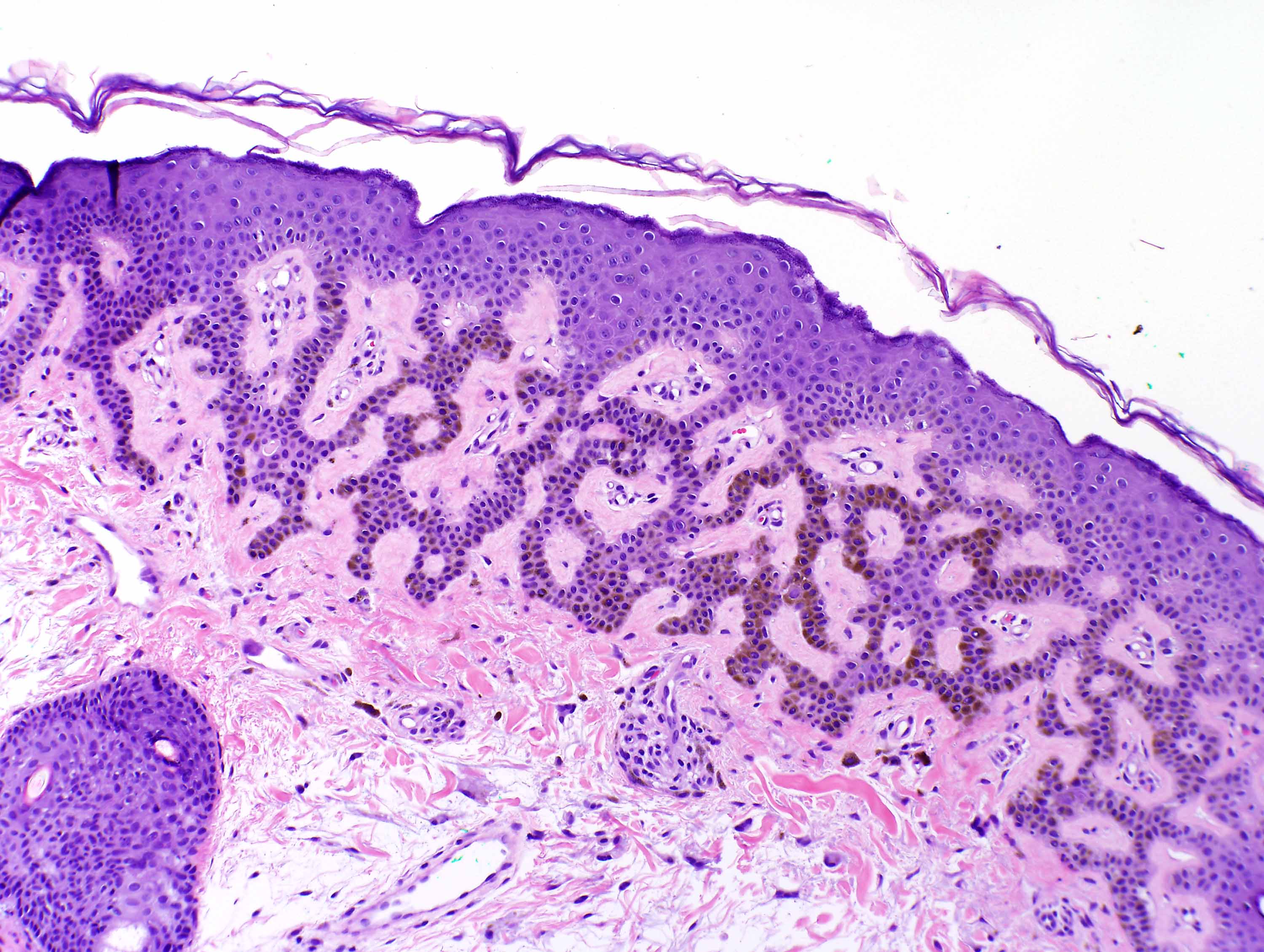
Adenoid with increased pigment
Clonal nests
Pale keratinocytes
Clonal nests and horn pseudocyts
Irritated
Increased pigmentation
Minimal acanthosis
Negative stains
- CK10 sparing of suprabasal nests in clonal seborrheic keratosis may help differentiate this lesion from Bowenoid squamous cell carcinoma (J Cutan Pathol 2012;39:225, Am J Dermatopathol 2017;39:433)
Videos
Seborrheic keratosis overview
Seborrheic keratosis and variants
Sample pathology report
- Left chest, shave of skin:
- Seborrheic keratosis
Differential diagnosis
- Melanocytic nevus:
- Nests of melanocytes in dermis or at dermal epidermal junction
- Also present in younger patients
- Solar lentigo:
- Similar to reticulated seborrheic keratosis
- Lentigo has pigmented, nonanastomotic, bulbous rete and no horn cysts
- Malignant melanoma:
- Malignant melanocytes with invasion into the dermis
- Pigmented basal cell carcinoma:
- Clefting, peripheral palisading, mucin, apoptosis and mitosis
- Condyloma acuminatum:
- Koilocytes
- Dysplastic changes
- Clinical findings (genital areas) and HPV positivity helpful in distinguishing
- Verruca vulgaris:
- Hypergranulosis, tiers of parakeratosis, dilated papillary blood vessels, intracorneal hemorrhage
- Clinical features (present on hands and feet) and HPV positivity helpful in distinguishing
- Actinic keratosis:
- Atypia of basal keratinocytes
- Squamous cell carcinoma:
- Full thickness squamous atypia
- Increased, often atypical mitoses
- Melanoacanthoma:
- Numerous dendritic melanocytes
- Regarded by some as a variant of seborrheic keratosis
- Clear cell acanthoma:
- Clear keratinocytes (glycogenated)
- No horn cysts
- Achrochordon:
- Usually in flexural areas
- More polypoid clinically
- Histologically normal skin lacking adnexal structures
- Inverted follicular keratosis:
- May have filiform growth
- Endophytic growth
- BCL2 upregulation in dendritic cells
Board review style question #1
Which feature helps distinguish the above lesion from squamous cell carcinoma?
- Acanathosis and papillomatosis
- Atypical mitotic figures
- Lack of atypia
- Molecular testing for FGFR3
Board review style answer #1
C. Lack of atypia. Seborrheic keratosis is a benign keratinocyte proliferation that lacks atypia and dysplasia. Acanthosis and papillomatosis (A) are features of seborrheic keratosis but can also be seen in squamous cell carcinoma. Atypical mitotic figures (B) are a feature of squamous cell carcinoma. Many seborrheic keratoses have mutations in FGFR3 (D) but it is not diagnostic or ubiquitous.
Comment Here
Reference: Seborrheic keratosis
Comment Here
Reference: Seborrheic keratosis
Board review style question #2
Sudden eruption of seborrheic keratosis on the trunk should prompt which clinical response?
- Evaluation for underlying colonic carcinoma
- Full body skin exam for atypical nevi
- Immediate treatment with cryotherapy
- No further workup is necessary
Board review style answer #2
A. Evaluation for underlying colonic carcinoma. Sudden eruption of multiple seborrheic keratoses, the Leser-Trélat sign, is a paraneoplastic phenomenon. It is associated with underlying malignancy, most often colonic adenocarcinoma and should prompt a clinical workup to evaluate (D). The Leser-Trélat sign is not associated with increased risk for atypical nevi or melanoma (B). While seborrheic keratoses can be treated with cryotherapy (C), they are benign and treatment is not necessary.
Comment Here
Reference: Seborrheic keratosis
Comment Here
Reference: Seborrheic keratosis
