
Skin melanocytic tumor
Lentigines, melanotic macules and melanocytic hyperplasia
Lentigo
Authors: Megan V. Ha, M.D., Bethany R. Rohr, M.D.
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 10 December 2024
Last staff update: 10 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Lentigo

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ha MV, Rohr BR. Lentigo. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumormelanocyticsolarlentigo.html. Accessed March 31st, 2025.
Definition / general
- Lentigines are pigmented macules that occur primarily on sun exposed sites in older adults and are characterized histologically by elongation of pigmented and bulbous rete (Pigment Cell Melanoma Res 2014;27:339)
Essential features
- Clinically present as tan to dark brown macules on sun exposed areas (J Cutan Pathol 2004;31:441)
- Associated with ultraviolet (UV) exposure (Br J Dermatol 2007;156:1214, Exp Dermatol 2016;25:174)
- Characterized histologically by elongation of pigmented and bulbous rete (J Cutan Pathol 2022;49:1074, Pigment Cell Melanoma Res 2014;27:339)
Terminology
- Solar lentigo, senile lentigo, lentigo senilis, actinic lentigo, sunburn freckle, freckle in adulthood, aging spot, liver spot, sun spot (Pigment Cell Melanoma Res 2014;27:339)
- Lentigo simplex, simple lentigo and juvenile lentigo represent a different entity of lentigo that may be precursor lesions to nevi (J Invest Dermatol 2009;129:2730, Am Fam Physician 2017;96:797)
ICD coding
Epidemiology
- Found in at least 90% of fair skinned people over the age of 60 years (Br J Dermatol 2006;154:438)
- Also prevalent in Asian populations (J Dermatol 2012;39:829)
- Syndromes with increased lentigines (Fam Cancer 2011;10:481)
- Peutz-Jeghers syndrome (PJS)
- Carney complex (CNC)
- Laugier-Hunziker syndrome (LHS)
- Bannayan-Riley-Ruvalcaba syndrome (BRRS)
- Cowden disease (CD)
- LEOPARD / Noonan syndrome
Sites
- Sun exposed areas of the skin, including the face, scalp, forearms and dorsa of hands (J Cutan Pathol 2004;31:441)
- In familial lentiginosis syndromes, lentigines may appear on all parts of the body but particularly labia majora, palms, soles, conjunctivae and vermillion border of the lips (Fam Cancer 2011;10:481)
Pathophysiology
- Chronic exposure to UV radiation leads to enhancement of melanin production and alteration of cellular proliferation (Br J Dermatol 2007;156:1214, Exp Dermatol 2016;25:174)
- In lentigines that are a part of genetic syndromes, mutations in pathways that regulate protein kinase A (PKA), Ras-MAP kinase and the mammalian target of rapamycin (mTOR) have been identified (J Med Genet 2005;42:801, Fam Cancer 2011;10:481, Front Biosci 2000;5:D353)
Etiology
- Likely combination of genetic variants and environmental factors, especially UV exposure (Pigment Cell Res 2004;17:225, J Invest Dermatol 2024;144:1412)
- Constituents of ambient air pollution have also been associated with solar lentigo development (J Invest Dermatol 2019;139:974)
- Lentigines with other specific etiologies include
- PUVA lentigines (J Am Acad Dermatol 1985;13:761)
- Radiation lentigines (Arch Dermatol 1997;133:209)
- Tanning bed lentigines (J Am Acad Dermatol 1989;21:689)
Clinical features
- Typically tan to dark brown macules with moth eaten borders (Pigment Cell Melanoma Res 2014;27:339)
- Color may range from yellow-brown to black, the latter often leading to a label of ink spot lentigo (Int J Immunopathol Pharmacol 2013;26:953)
- Color is often homogenous but darker lesions frequently have mottled appearance (J Cutan Pathol 2004;31:441)
- Can range from millimeters to centimeters in diameter (Pigment Cell Melanoma Res 2014;27:339)
- Larger lesions tend to be irregular in shape (J Cutan Pathol 2004;31:441)
- Dermoscopy typically shows structureless homogenous pigmentation (ISRN Dermatol 2013;2013:546813)
- There may be areas of delicate light brown pseudonetwork, feathering or parallel fingerprint-like patterns (J Am Acad Dermatol 2024;91:1006)
Diagnosis
- Clinical diagnosis with or without dermoscopy is most common
- Biopsy can confirm diagnosis and rule out a melanocytic neoplasm (J Cutan Pathol 2022;49:1074)
Prognostic factors
- Sun exposure is associated with increasing size and number of lentigines over time (J Am Acad Dermatol 2024;91:1006)
- There may be transformation into lichen planus-like keratoses (also known as benign lichenoid keratoses) (J Invest Dermatol 1975;65:429, Dermatol Pract Concept 2023;13:e2023115)
Case reports
- 39 year old woman with a black macule (Arch Dermatol 1992;128:934)
- 45 year old man with brown macules on the legs (Arch Dermatol 1997;133:209)
- 47 year old woman with an asymptomatic tan-brown macule (J Cutan Pathol 1986;13:308)
- 54, 55 and 64 year old men presented for removal of pigmented lesions (Lasers Surg Med 2012;44:112)
- 65 year old man with multiple pigmented lesions (J Eur Acad Dermatol Venereol 1999;13:193)
- 72 year old woman with a 2 year history of a light brown pigmented lesion (Case Rep Dermatol Med 2019;2019:3907671)
- 5 patients with ink spot lentigo (Int J Immunopathol Pharmacol 2013;26:953)
Treatment
- No treatment is necessary
- Combination based treatments: associated with a higher frequency of complete response (Dermatol Surg 2023;49:17)
- Cosmetic treatment options
- Laser based treatments: the most successful monotherapy (Dermatol Surg 2023;49:17)
- Topical retinoids (Dermatol Surg 2023;49:17)
- Cryotherapy: previously considered first line in treatment of lentigines; however, there are reports that it may have lower response rates compared to other modalities (Dermatol Surg 2023;49:17)
- Chemical peels (Dermatol Surg 2023;49:17)
- Other treatments may include topical hydroquinone, undecylenoyl and cysteamine (J Drugs Dermatol 2021;20:1276, Dermatol Surg 2023;49:17)
Clinical images
Images hosted on other servers:

Well defined, homogenous brown macule

Well defined light brown patch

Irregularly shaped, well defined brown patch

Multiple light brown to dark brown macules

Well defined macule with moth eaten borders

Classic reticular and parallel patterns

Back lesions


Pre and post laser treatment
Microscopic (histologic) description
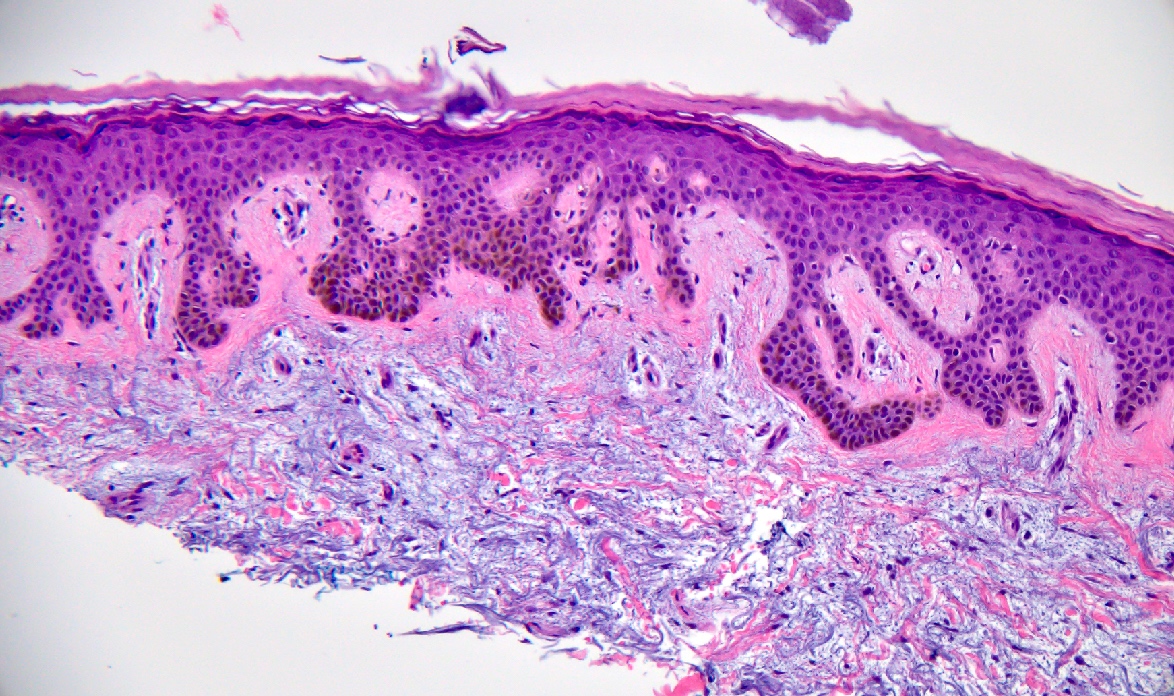
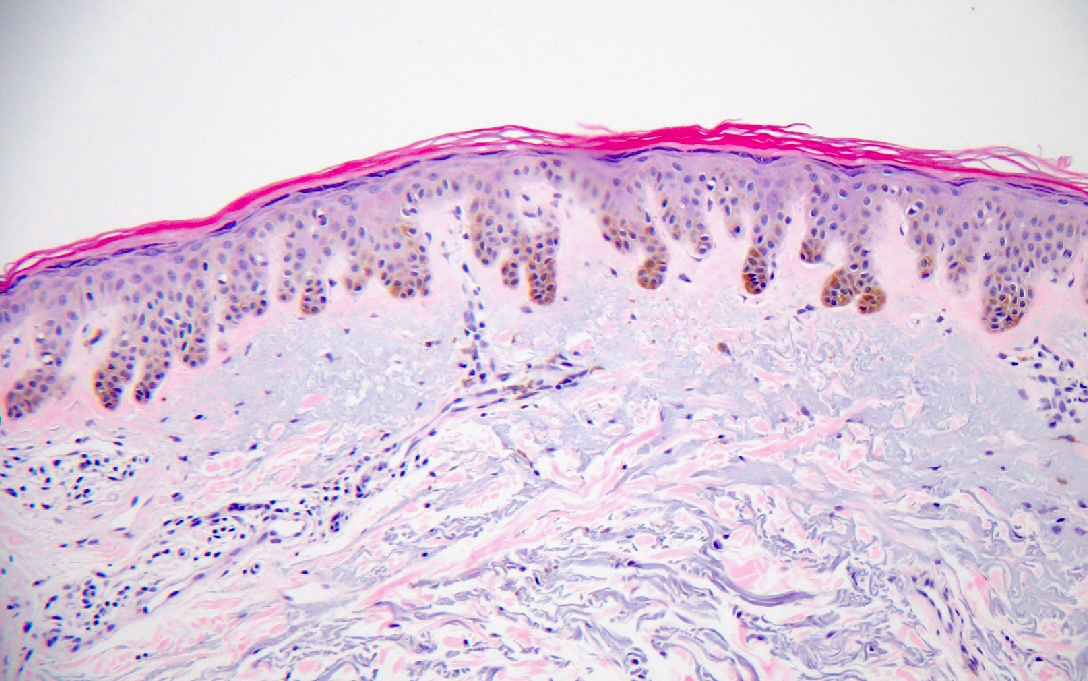
- Characterized by acanthosis composed of elongated, bulbous rete ridges, although this feature is not always observed in lesions on the face (J Cutan Pathol 2022;49:1074, Pigment Cell Melanoma Res 2014;27:339)
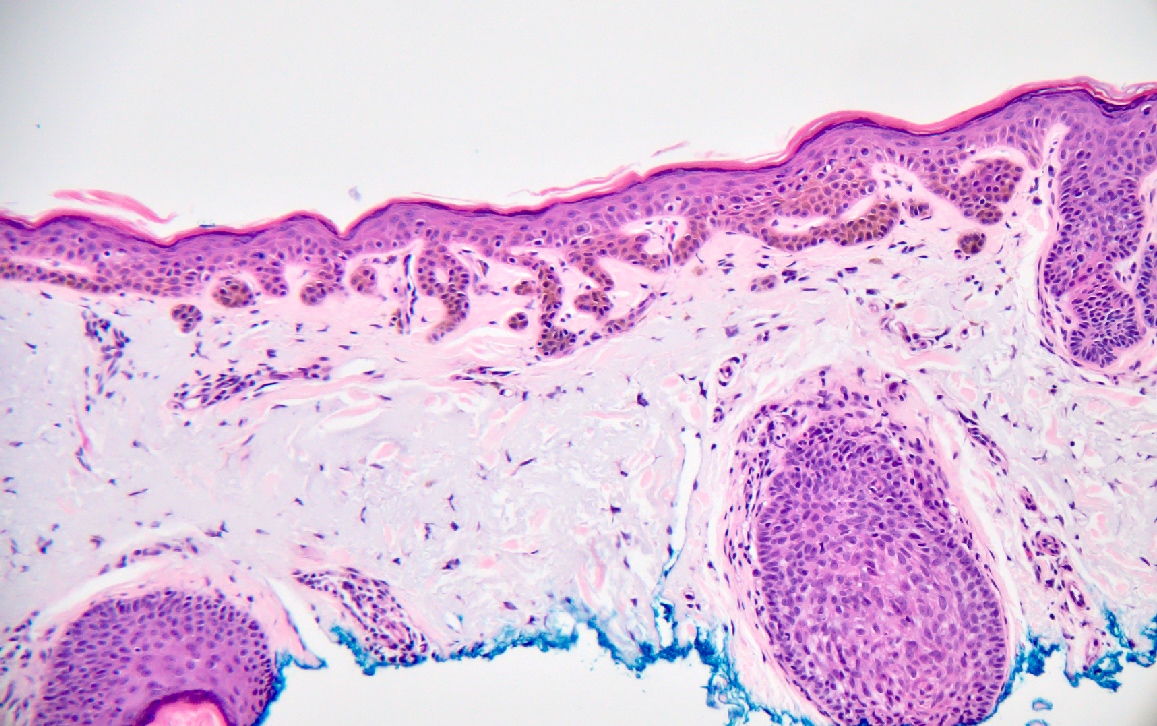
- Lentigines on the face may show flattened epidermis with basal melanosis and typically more severe elastosis (J Cutan Pathol 2022;49:1074, J Dermatol 2012;39:829)
- Hyperpigmented basal layer that is often denser at tips of rete ridges, giving a dirty socks appearance (J Cutan Pathol 2022;49:1074, Pigment Cell Melanoma Res 2014;27:339)
- Typically atrophic epidermis between the rete ridges (J Cutan Pathol 2022;49:1074)
- Normal or slightly increased number of basal layer monomorphic melanocytes that are distributed equidistant from one another and do not form nests (J Cutan Pathol 2022;49:1074)
- Similarly, lentigo simplex is characterized by elongated rete ridges and an increased number of basal layer banal melanocytes; however, it is absent of solar elastosis
Microscopic (histologic) images
Contributed by Megan V. Ha, M.D. and Bethany R. Rohr, M.D.
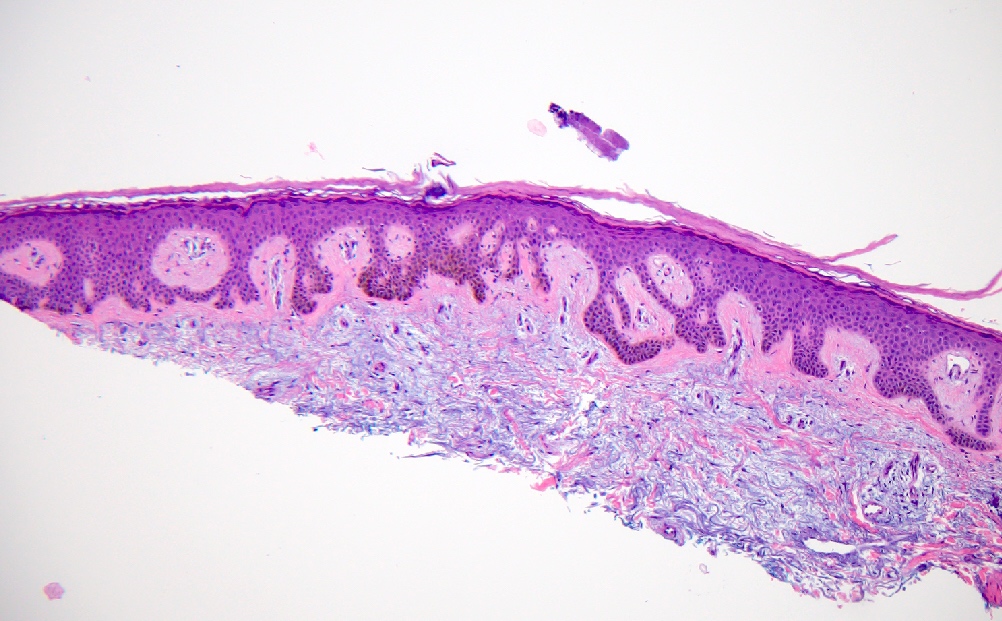
Elongated rete
Underlying solar elastosis
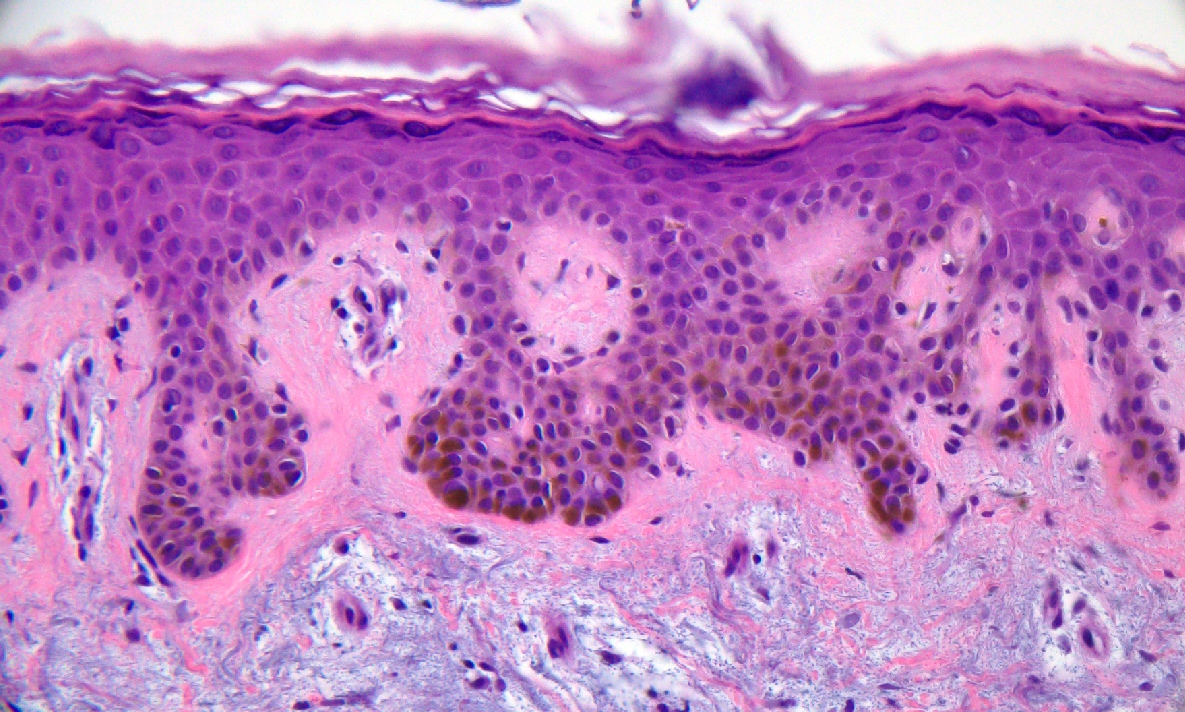
Increased junctional melanocytes

Overlap with seborrheic keratoses
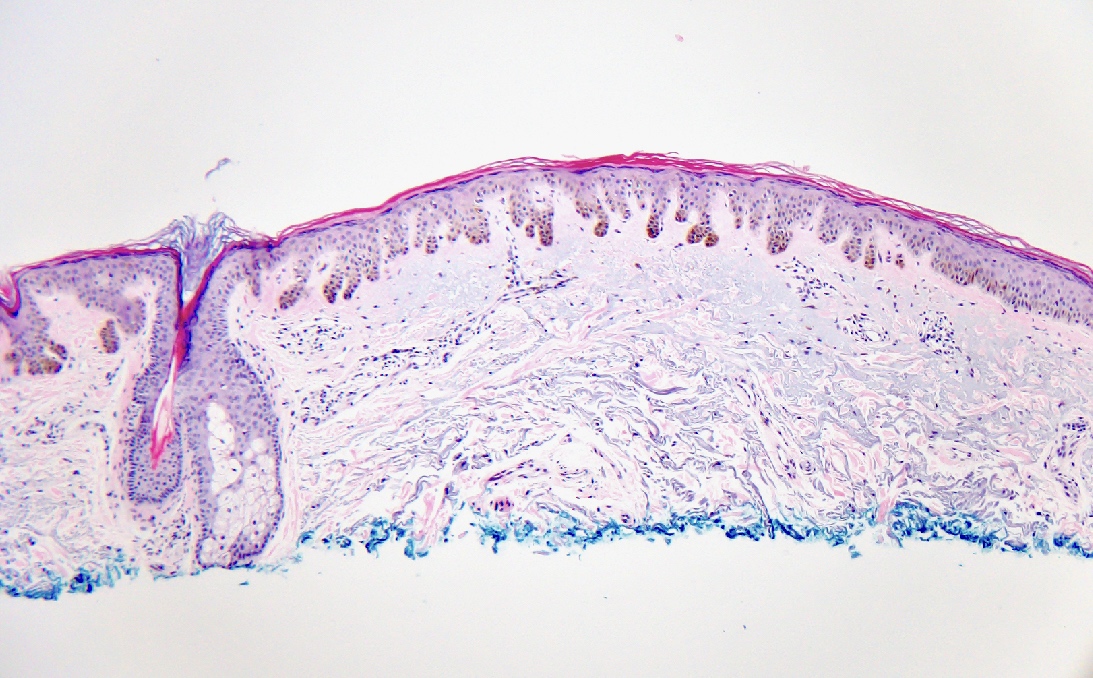
Interrete atrophic epidermis
Dirty socks
Thin rete
Positive stains
- Immunostains are not required for diagnosis
- Melanocyte stains may demonstrate normal to slightly increased number of basal melanocytes without asymmetry, nesting or significant pagetoid spread
- Keratin markers are positive
Videos
Histologic description of solar lentigo
Sample pathology report
- Skin, shave biopsy:
- Solar lentigo (see comment)
- Comment: There are elongated, pigmented and bulbous rete with underlying solar elastosis.
Differential diagnosis
- Lentigo maligna melanoma:
- Atypical melanocytes poorly and irregularly nested along the dermoepidermal junction with scarce pagetoid spread (Dermatol Pract Concept 2022;12:e2022194, J Cutan Pathol 2022;49:1074, JAMA Dermatol 2019;155:782)
- When invasive, atypical melanocytes in single cells and nests within the dermis (Dermatol Pract Concept 2022;12:e2022194, J Cutan Pathol 2022;49:1074)
- Pigmented actinic keratosis:
- Atypical keratinocytes in the lower epidermis with increased melanin pigmentation (Cureus 2019;11:e4721, J Cutan Pathol 2022;49:1074)
- Junctional melanocytic nevus:
- Junctional nests of melanocytes uniform in size, distributed at the tips of rete ridges (Cureus 2022;14:e26127)
- Adenoid / reticulated seborrheic keratosis:
- Thin, typically 2 cell layer rows of reticular acanthosis with hyperkeratosis and papillomatosis; frequently pigmented (Ann Dermatol 2016;28:152)
- Macular or evolving seborrheic keratoses can be clinically difficult to distinguish from solar lentigo
- Ephelides:
- Normal number of melanocytes with pigmentation due to increased melanin in basal keratinocytes (Fam Cancer 2011;10:481)
- May be indistinguishable from lentigo; however, lack of significant solar elastosis and elongation of rete ridges may help to distinguish
Board review style question #1
An 80 year old man with past medical history of multiple nonmelanoma skin cancers presents with a brown patch on his dorsal right arm for the past 10 years. A skin shave biopsy is shown. What is the diagnosis?
- Junctional melanocytic nevus
- Lentigo maligna melanoma in situ
- Pigmented actinic keratosis
- Reticulated seborrheic keratosis
- Solar lentigo
Board review style answer #1
E. Solar lentigo is a hyperpigmented macule commonly found on sun exposed skin in older adults. These lesions are associated with ultraviolet (UV) exposure; sun exposure is also associated with increasing size of lentigines over time. The slide above shows an atrophic interrete epidermis, acanthosis with elongation of rete ridges and solar elastosis. There is basal melanosis, commonly described as dirty socks, and a normal to slight increase in number of junctional melanocytes. Answer B is incorrect because although there will be underlying solar elastosis, lentigo maligna melanoma in situ will show an irregular proliferation of atypical melanocytes. Answer A is incorrect because junctional melanocytic nevi display nests of banal appearing melanocytes at the tips of rete ridges. Answer D is incorrect because although reticulated seborrheic keratoses can display pigmented downward extensions of the epidermis, the strands are usually thin and interlacing. Solar lentigo will have shorter and more bulbous rete. Answer C is incorrect because actinic keratoses are characterized by atypia of basal layer keratinocytes.
Comment Here
Reference: Lentigo
Comment Here
Reference: Lentigo
Board review style question #2

A 65 year old woman with past medical history of lentigo maligna melanoma in situ presents with a brown macule on the cheek of unknown duration. A skin shave biopsy is shown. What is the diagnosis?
- Junctional melanocytic nevus
- Lentigo maligna melanoma in situ
- Pigmented actinic keratosis
- Seborrheic keratosis
- Solar lentigo
Board review style answer #2
E. Solar lentigo. Solar lentigines are hyperpigmented macules on sun exposed skin found in the majority of light skinned older adults. While solar lentigines are typically characterized by acanthosis with elongation of rete ridges, lesions on the face may show a flattened epidermis with basal melanosis and typically more severe solar elastosis. On the slide above, there are both elongated rete ridges as well as portions of flattened epidermis with basal pigmentation. There is also a slightly increased number of basal layer single unit melanocytes. Answer D is incorrect because although reticulated seborrheic keratoses display thin and interlacing pigmented extensions of the epidermis, they are typically longer with more extensive anastomoses. Answer B is incorrect because although there will be underlying solar elastosis, lentigo maligna melanoma in situ will show an irregular proliferation of melanocytes with crowded growth. Answer C is incorrect because actinic keratoses are characterized by atypia of basal layer keratinocytes. Answer A is incorrect because junctional melanocytic nevi display nests of banal appearing melanocytes at the tips of rete ridges.
Comment Here
Reference: Lentigo
Comment Here
Reference: Lentigo
