
Skin melanocytic tumor
Deep penetrating, BAP1 inactivated & pigmented epithelioid melanocytomas
Pigmented epithelioid melanocytoma
Authors: Elnaz Panah, M.D., Jodi Speiser, M.D.
Editorial Board Member: Viktoryia Kozlouskaya, M.D., Ph.D.

Last author update: 26 June 2023
Last staff update: 26 June 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Pigmented epithelioid melanocytoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Panah E, Speiser J. Pigmented epithelioid melanocytoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumormelanocyticpigmentedepithelioidmelanocytoma.html. Accessed April 1st, 2025.
Definition / general
- Melanocytic tumor with heavily pigmented epithelioid, spindled and dendritic melanocytes (Surg Pathol Clin 2021;14:285)
Essential features
- Composed of pigmented epithelioid, spindled and dendritic melanocytes with large vesicular nuclei
- Associated with Carney complex or can be sporadic
Terminology
- Epithelioid blue nevus (EBN)
- Animal type melanoma (not recommended based on WHO)
- Benign melanocytoma
- Melanocytoma
ICD coding
- ICD-10: C43.9 - malignant melanoma of skin, unspecified
Epidemiology
- Median age of 20 - 27 years (Surg Pathol Clin 2021;14:285)
- Infants and children
- M = F (Am J Clin Dermatol 2018;19:15)
- Affects all racial / ethnic groups
- Associated with Carney complex or can be sporadic
Sites
- Extremities (38.3%), head and neck (30.8%) and trunk (30.8%) (Surg Pathol Clin 2021;14:285)
Pathophysiology
- Hypothesized that reduced expression of glutathione S transferase may play a role
Etiology
- Unknown etiology
Clinical features
- Pigmented epithelioid melanocytoma (PEM) has been divided into 2 general categories (histologically indistinguishable):
- PEM with benign outcome
- PEM associated with Carney complex
- PEM combined with other banal nevi
- PEM with low grade neoplasia
- Sporadic PEM not associated with Carney complex or other banal nevi
- PEM with benign outcome
- Slow growing
- Blue to blue-black papules or nodules (Surg Pathol Clin 2021;14:285)
- Dermoscopy: displays large and centrally homogeneous or structureless blue areas, with the coexistence of black area and crystalline structures
Diagnosis
- Biopsy
Prognostic factors
- Overall, a benign to low grade neoplasm
- Sentinel lymph node involvement (30 - 50% of cases) (Surg Pathol Clin 2021;14:285)
- Rare distant metastasis (Surg Pathol Clin 2021;14:285)
- Clinical meaning of lymph node or rare distant metastases remains uncertain; positive regional nodes in PEM do not imply systemic metastatic disease and death secondary to rare systemic metastases has not been reported
- Does not appear to be related to sun exposure
Case reports
- 4 year old African American girl with an enlarging lesion on her right parietal scalp (J Cutan Pathol 2020;47:70)
- 60 year old Japanese man with a 20 year history of a black dome shaped nodule on the nose (Case Rep Oncol 2018;11:378)
- 63 year old man with a dermal based nodule on the scalp with blue pigmentation (Int J Mol Sci 2017;18:1769)
Treatment
- Complete excision
- As regional lymph nodes do not imply systemic metastatic disease, aggressive therapy is not recommended
Clinical images
Images hosted on other servers:

Pigmented nodule on scalp

Blue-black, dome shaped nodule on nose

Smooth, blue-black papule with protruding hairs

Verrucous lesion with uniform, gray-brown pigment
Gross description
- Domed, papular or nodular lesion with dark blue or purple pigmentation
- May be multifocal
Microscopic (histologic) description
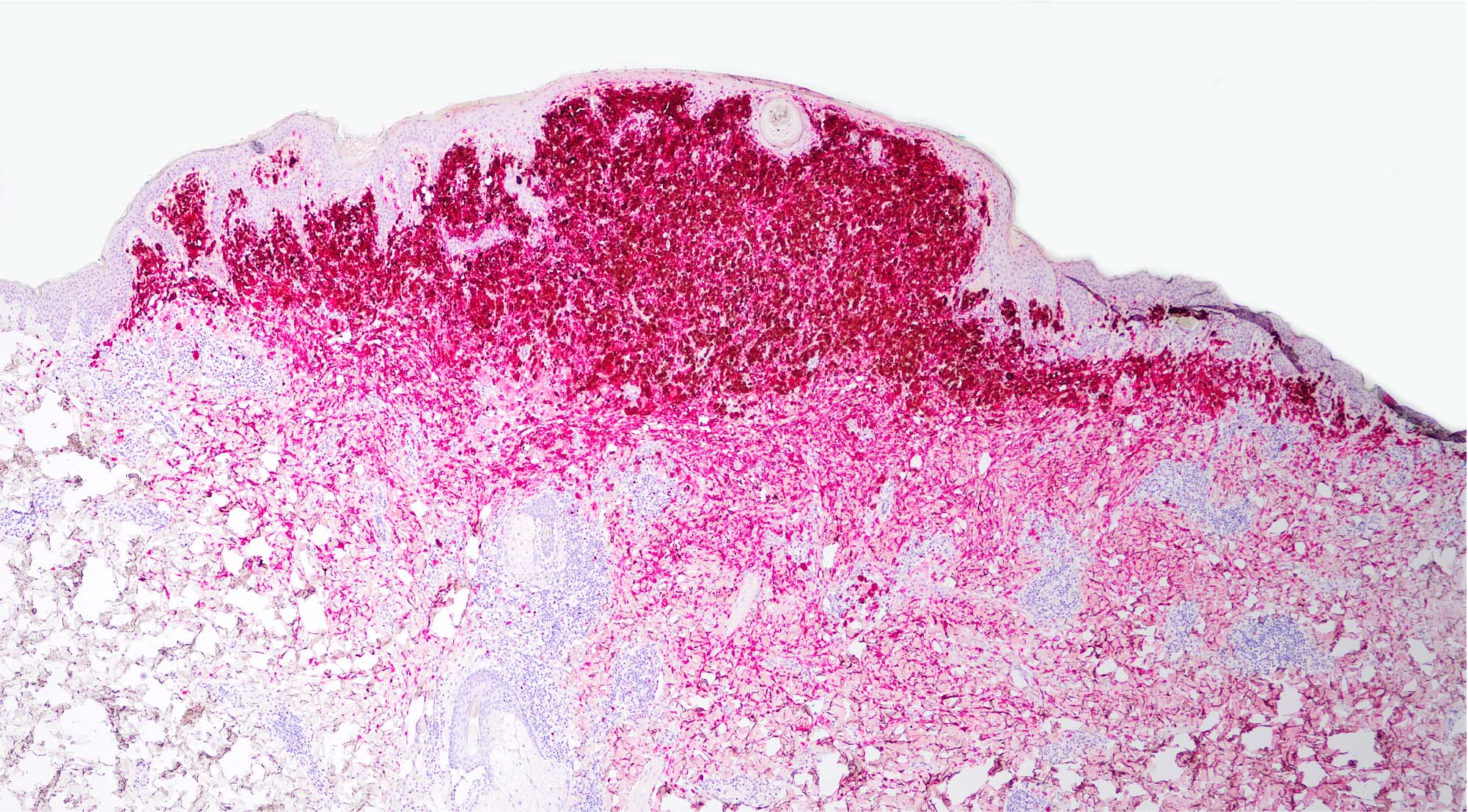
- Wedge shaped and relatively well circumscribed proliferation of melanocytes and melanophages, with the majority having overlying epidermal hyperplasia and dark, evenly distributed pigmentation
- Junctional component generally consists of isolated dendritic melanocytes with upward spread into the spinous layer but some PEM are entirely intradermal or consist of large nests reminiscent of Spitz / spindle cell nevus of Reed
- Dermal component consists of single cell or small nests of melanocytes that do not show maturation but can have periadnexal, perivascular and perineural extension
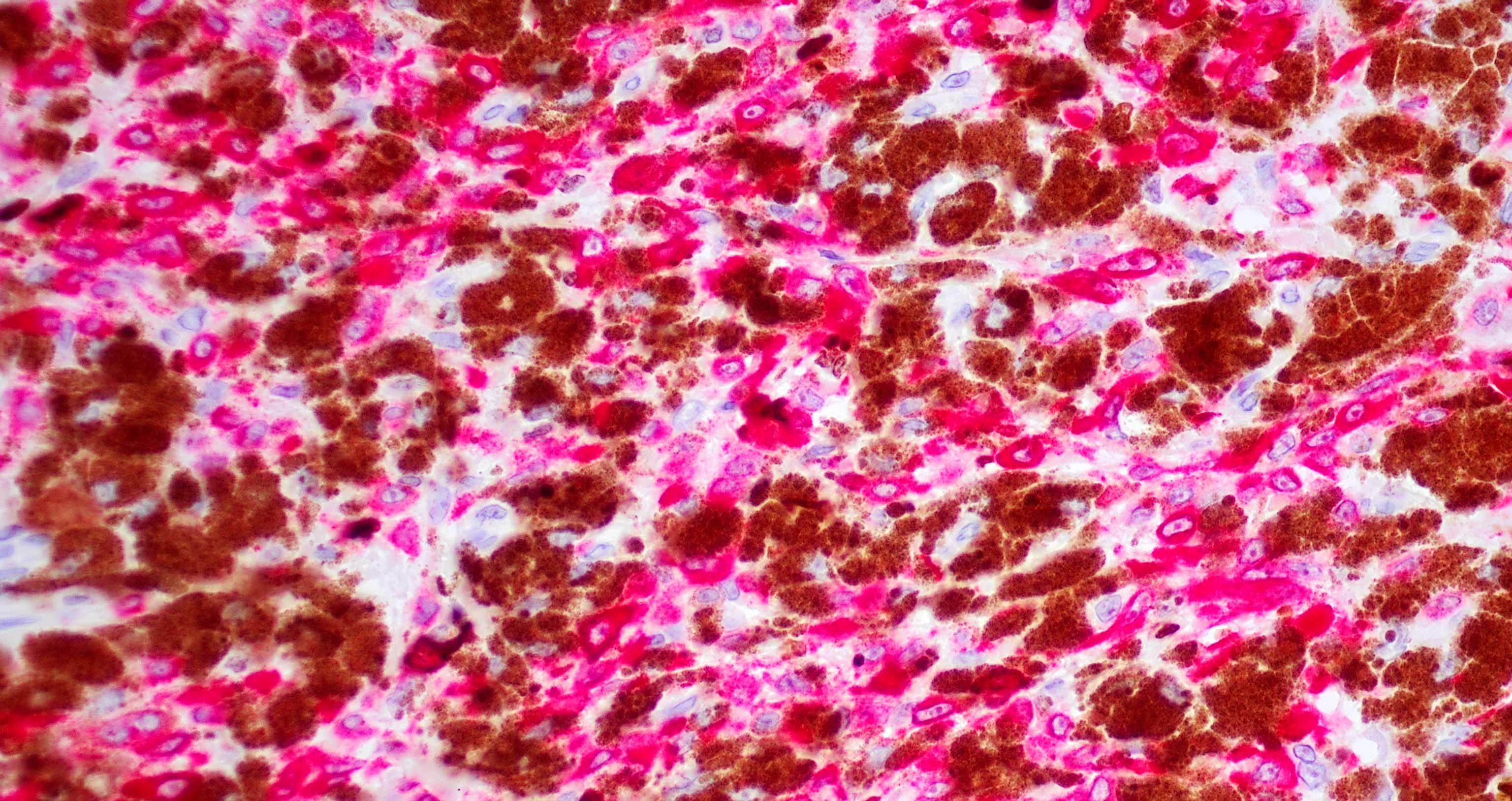
- 4 cell types described (most show mixed cell population):
- Small epithelioid cells
- Large epithelioid cells; can be multinucleated, similar to a Reed-Sternberg cell
- Spindle shaped melanocytes
- Melanophages
- Vesicular nuclei with large, central nucleoli
- Rare or absent mitoses and necrosis
- Histologic features more concerning for PEM with low grade malignancy:
- Large size: extending to subcutis
- Cytologic atypia
- Solid sweeping fascicles with no intervening collagen fibers
- Poor circumscription
- PEM with PRKCA fusion: solid sheets of pigmented epithelioid melanocytes, younger patients
- PEM with PRKAR1A mutation: more cytologic heterogeneity, may have conventional nevus component with smaller nests, separated by fibrous bands of collagen
- References: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019, Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014, Busam: Pathology of Melanocytic Tumors, 1st Edition, 2018
Microscopic (histologic) images
Contributed by Elnaz Panah, M.D. and Jodi Speiser, M.D.
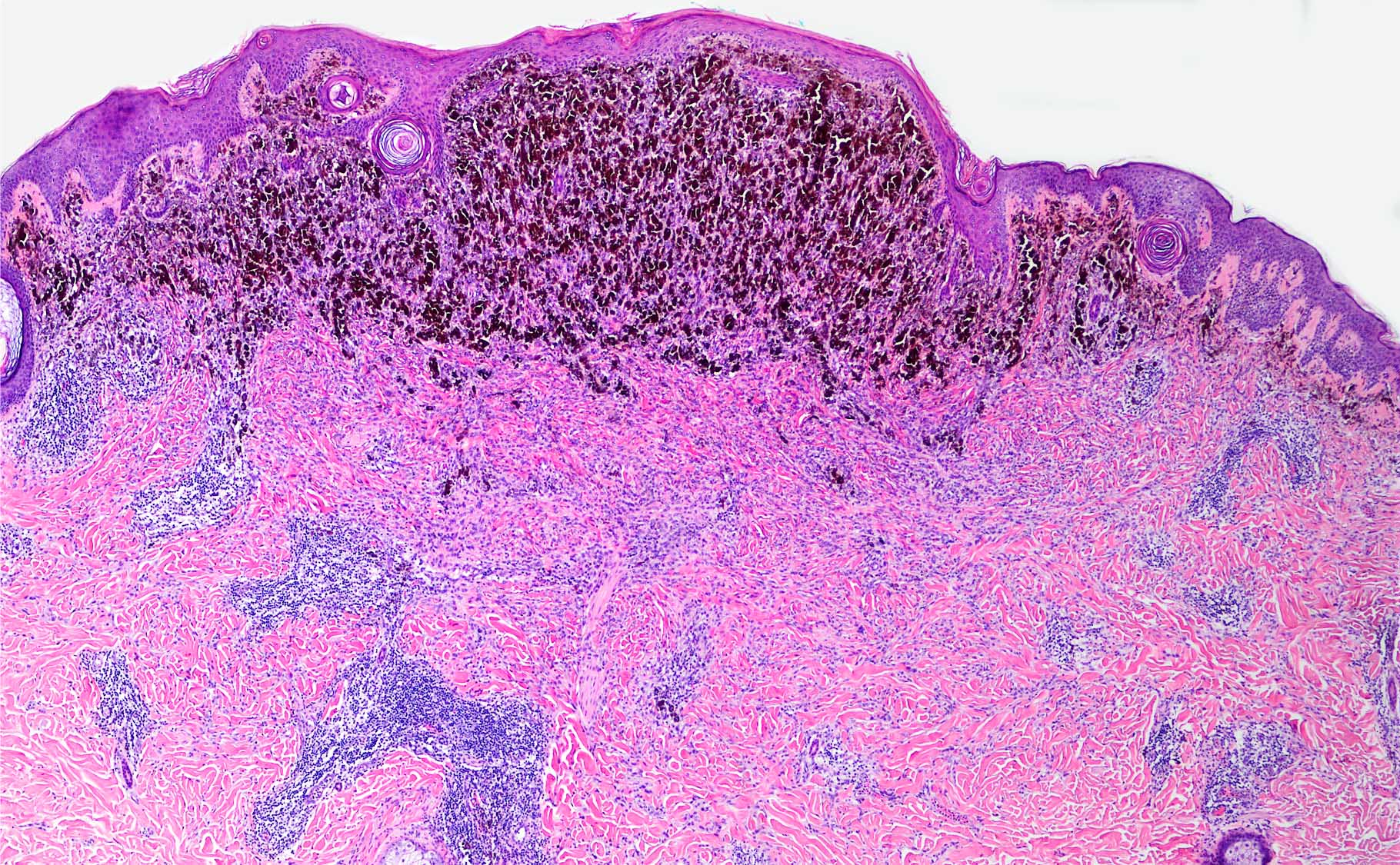
Intradermal melanocytic proliferation
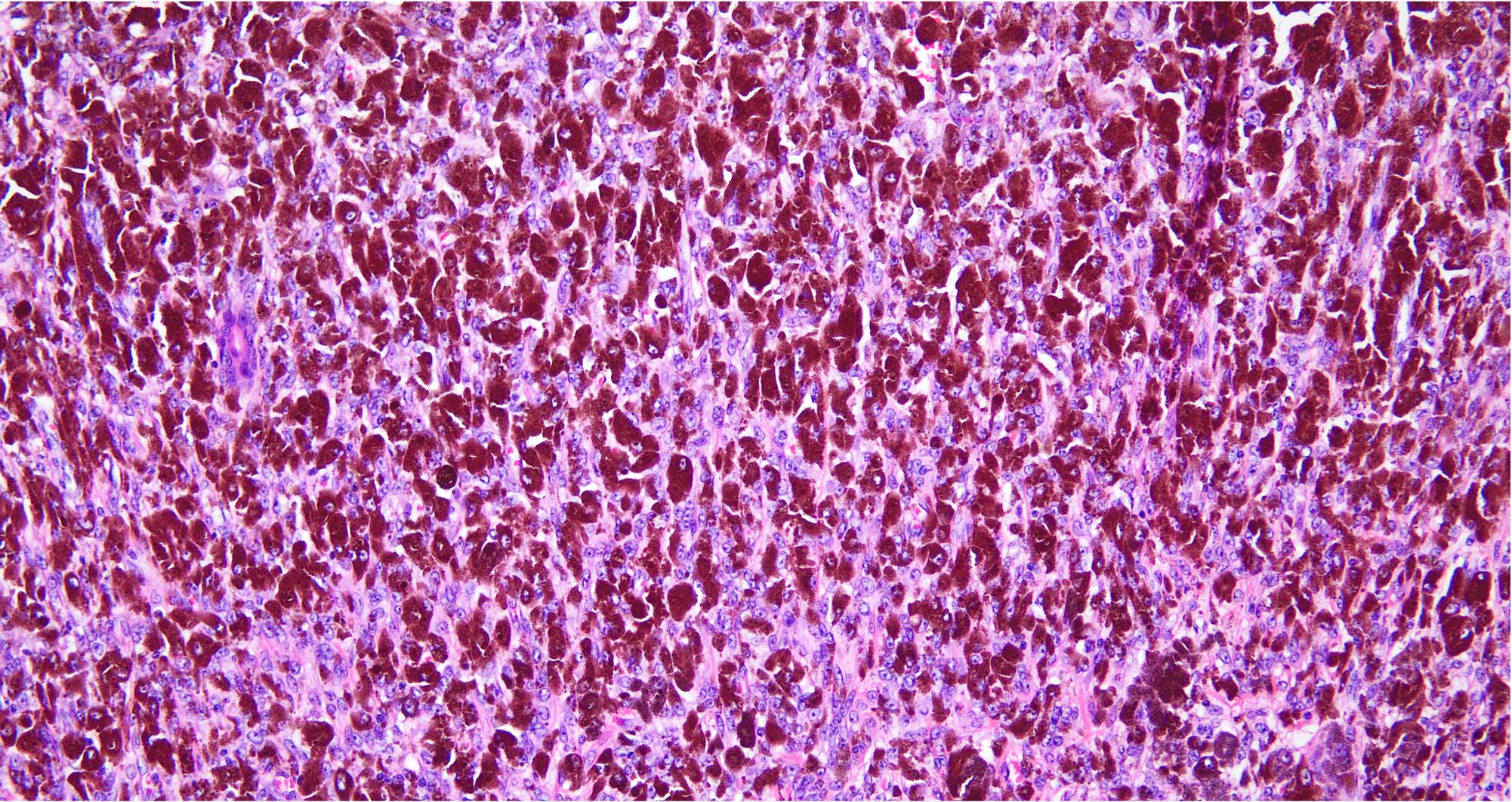
Numerous melanophages
Melanocytes with vesicular nuclei
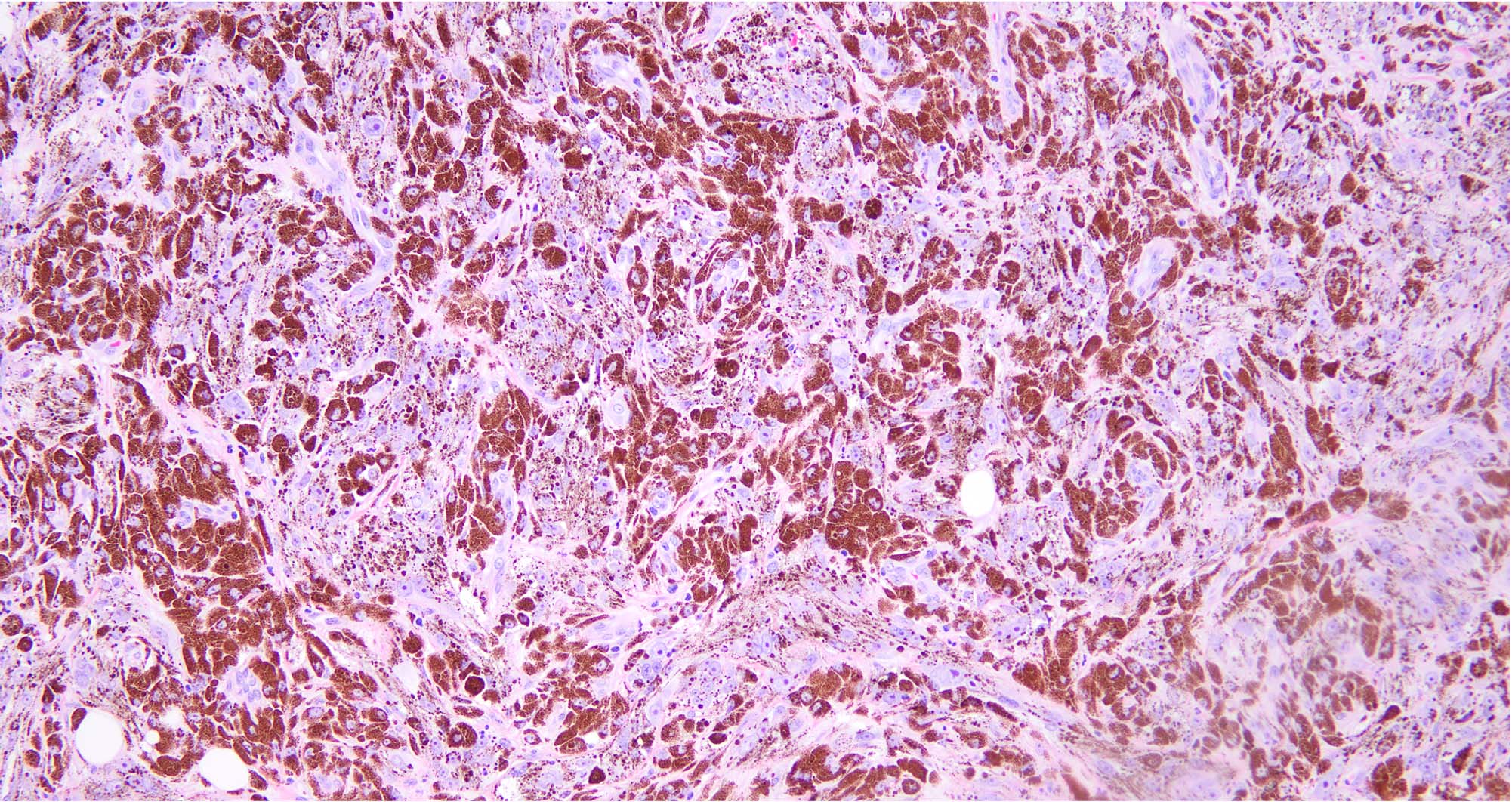
HMB45
MART1 / Ki67
Positive stains
Negative stains
- Loss of cytoplasmic PRKAR1A in combined PEMs and in a subset of pure PEMs but PRKAR1A is retained in PEM associated with PRKCA fusion (Busam: Pathology of Melanocytic Tumors, 1st Edition, 2018)
Electron microscopy description
- Large indented nuclei with abundant cytoplasm
- Numerous single melanosomes varying in size
- Melanosomes seen in the early stage of maturation, a pleomorphic appearance (Arch Dermatol 2009;145:55)
Molecular / cytogenetics description
- Loss of cytoplasmic expression of PRKAR1A
- Inactivating alterations in protein kinase A regulatory subunit R1 alpha gene (PRKAR1A) with a preceding mutation of BRAF (seen in combined PEM) or less frequently, NRAS (J Cutan Pathol 2019;46:878)
- Fusions in protein kinase C alpha fusion (PRKCA) (J Cutan Pathol 2019;46:878)
- Mutations of MAP2K1 associated with loss of expression of PRKAR1A
- Recently, a subset of combined lesions PEM + spitzoid was described (Am J Dermatopathol 2022;44:568)
- CD63::PRKCB fusion was also described (Pediatr Dermatol 2022;39:322)
Sample pathology report
- Skin, biopsy / excision:
- Pigmented epithelioid melanocytoma
- Microscopic description: The sections show a symmetric, compound, wedge shaped mass spanning most of the dermis and comprised of predominantly melanophages and scattered melanocytes. There is epidermal hyperplasia overlying the lesion. The junctional component is relatively inconspicuous and composed of scattered, single dendritic melanocytes. The dermal component is composed of epithelioid and dendritic melanocytes with large, vesicular nuclei and large, central nucleoli.
Differential diagnosis
- Animal type melanoma:
- Controversial diagnosis; some experts use the terms PEM and animal type melanoma interchangeably, some group them into pigment synthesizing melanocytic tumors and some consider them a malignant variant of PEM
- Asymmetric proliferation of deeply pigmented and large epithelioid cells
- Cells obliterate the collagen fibers and can involve the subcutis
- Widespread uniform cellular atypia and mitoses
- Typically all of these entities lack the PRKAR1A changes of PEM (loss of cytoplasmic expression, molecular changes)
- Blue nevus-like melanoma (malignant blue nevus):
- Pigment is irregularity distributed
- Proliferation comprises atypical epithelioid cells
- Lack of benign looking spindle cell component
- Junctional component similar to melanoma in situ
- Blue nevus with epithelioid cells:
- Dermal proliferation of monomorphic epithelioid polygonal cells
- No dendritic cellular component, junctional component
- GNAQ and GNA11 mutations are present
- Deep penetrating nevus:
- Clear cut plexiform architecture (extension of melanocytes along the path of adnexal structures, blood vessels and nerve bundles)
- Less pigmented
- Consists of predominantly larger clear cells
- Common blue nevus:
- No junctional component
- Lack of epithelioid cells
- GNAQ and GNA11 mutations are present
- Blue nevus-like melanoma (malignant blue nevus):
- Pigmented spindle cell nevus of Reed:
- Predominantly epidermal lesion composed of large nests of spindle cells
- Pigment generally most prominent in epidermis, at dermal / epidermal junction and within the papillary dermis
- Nests can coalesce to form a long ribbon with an underlying inferior smooth border
- Nuclei are small, basophilic and inconspicuous
- Psammomatous melanotic schwannoma:
- Asymmetric with variable pigmentation, psammoma bodies, focal nuclear palisading and mild cytologic atypia
- Lacks heterogenous combination of elongated dendritic cells, epithelioid dendritic cells and melanophages
- Melanoma developing in a nevus:
- Asymmetric
- Most commonly has an epidermal component with upward spread
- Lacks heterogenous combination of elongated dendritic cells, epithelioid dendritic cells and melanophages
- Widespread cytologic atypia and frequent mitotic activity
- Pigmented primary nodular melanoma and metastatic melanoma:
- Asymmetric
- Lacks heterogenous combination of elongated dendritic cells, epithelioid dendritic cells and melanophages
- Widespread cytologic atypia, frequent mitotic activity, necrosis
Additional references
Board review style question #1
Based on the pictures shown above, which of the following syndromes can be seen with the diagnosis?
- Carney complex
- Cowden syndrome
- Gorlin syndrome
- Muire-Torre syndrome
Board review style answer #1
Board review style question #2
What are the histologic characteristics of pigmented epithelioid melanocytoma?
- Asymmetric proliferation of deeply pigmented and large epithelioid cells, which obliterate the collagen fibers
- Asymmetric proliferation with variable pigmentation, psammoma bodies, focal nuclear palisading and mild cytologic atypia
- Proliferation comprised of atypical epithelioid cells with irregularly distributed pigmentation
- Proliferation of larger clear cells with plexiform architecture
- Wedge shaped and relatively well circumscribed proliferation of melanocytes and melanophages with the majority having overlying epidermal hyperplasia and dark, evenly distributed pigmentation
Board review style answer #2
E. Wedge shaped and relatively well circumscribed proliferation of melanocytes and melanophages with the majority having overlying epidermal hyperplasia and dark, evenly distributed pigmentation. Pigmented epithelioid, spindled and dendritic melanocytes with large vesicular nuclei.
Comment Here
Reference: Pigmented epithelioid melanocytoma
Comment Here
Reference: Pigmented epithelioid melanocytoma
