
Skin melanocytic tumor
Melanoma
Melanomas with unusual features (balloon cell, verrucous, signet ring cell, small cell, etc.)
Editorial Board Member: Bethany R. Rohr, M.D.


Last author update: 29 February 2024
Last staff update: 29 February 2024
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Melanomas with unusual features

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Clinical features | Diagnosis | Case reports | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Capuzzolo M, Cazzato G. Melanomas with unusual features (balloon cell, verrucous, signet ring cell, small cell, etc.). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumormelanocyticmelanomaunusual.html. Accessed April 1st, 2025.
Definition / general
- Rare forms of melanoma that account for < 1% of cases (Curr Opin Oncol 1993;5:364)
Essential features
- Melanoma can present with rare and unusual histomorphological forms (variants) that account for < 1% of cases
- Morphological peculiarities do not always translate to a worsening prognosis
- Appropriate histological description and immunohistochemical markers allow us to reach a precise and detailed diagnosis of unusual forms of melanoma
- It is essential to consider the differential diagnoses of particular forms of melanoma
Terminology
- Balloon cell melanoma (Dermatopathology (Basel) 2022;9:100)
- Rhabdoid melanoma (Int J Clin Exp Pathol 2014;7:840)
- Verrucous melanoma (Open Access Maced J Med Sci 2017;5:547)
- Signet ring cell melanoma (Pathol Int 2015;65:383)
- Small cell melanoma (Dermatopathology (Basel) 2019;6:231)
- Myxoid melanoma (Clin Exp Dermatol 2013;38:559)
- Osteogenic melanoma (Skeletal Radiol 2018;47:711)
- Dedifferentiated / undifferentiated melanoma (Dermatopathology (Basel) 2021;8:494)
ICD coding
Epidemiology
- Middle aged to elderly persons
- No sex predilection (Int J Clin Exp Pathol 2014;7:840)
Sites
- Balloon cell: choroid (14%) and other locations
- Melanoma with rhabdomyosarcomatous differentiation: metastatic setting (lymph nodes, soft tissue, liver) more common than primary cutaneous (scalp, trunk, extremities) (Int J Clin Exp Pathol 2014;7:840)
- Verrucous: more common in face and limbs
- Signet ring cell: metastatic setting more common than primitive
- Small cell, 2 forms
- Develops in large congenital nevus
- Develops in children, de novo, on the scalp
- Myxoid: metastatic more common than primary mucocutaneous (skin, nasal sinuses, conjunctiva, gastrointestinal system)
- Osteogenic: more common on acral skin and nail bed; occasional mucosal involvement
Clinical features
- Balloon cell (Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014)
- Usually pigmented lesion on the extremities
- Clinical features not different from common melanoma
- Nodular, polypoid, papillated lesions
- Clinical appearance not influenced by cytological alterations
- Rhabdoid
- No distinctive clinical features for either primary cutaneous or metastatic lesions
- Verrucous (Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014)
- Resembles a keratotic epidermal tumor such as squamous cell carcinoma (SCC), seborrheic keratosis (SK), keratoacanthoma (KA) or others
- Signet ring cell
- More frequent in metastatic setting
- No distinctive clinical findings
- Usually very thick (Pathol Int 2015;65:383)
- Small cell (Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014)
- First form: core of a large congenital nevus
- Second form: de novo, children, on the scalp, rapidly fatal
- Possible metastatic setting
- Myxoid (Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014)
- Myxoid variant of melanoma is more likely to be metastastic than primitive, although usually primitive melanoma is common
- Primitive forms are very rare
- Osteogenic
- Some cases related to potential trauma (Mod Pathol 2006;19:S41)
- Dedifferentiated / undifferentiated
- Nonspecific
Diagnosis
- Excisional biopsy
- Incisional biopsy
- Shave or punch biopsy with adequate breadth and depth
Case reports
- 28 year old man with asymptomatic pink lesion on his arm (Dermatol Pract Concept 2017;7:59)
- 32 year old woman with a lesion in the left lumbar region (Case Rep Oncol 2016;9:262)
- 32 year old man with a right thumb lesion (Skeletal Radiol 2018;47:711)
- 57 year old man with enlarging nodule arising from a congenital nevus on the right flank (Pathol Int 2015;65:383)
- 64 year old man with metastatic rhabdoid melanoma (Indian J Cancer 2020;57:473)
- 79 year old woman with a pigmented, raised lesion (Dermatopathology (Basel) 2021;8:494)
- Woman with a verrucous keratotic lesion on the right thigh (Open Access Maced J Med Sci 2017;5:547)
Microscopic (histologic) description
- Balloon cell
- Melanocytes with abundant and finely vacuolated cytoplasm, scattered dusty melanin granules (Dermatopathology (Basel) 2022;9:100)
- Nuclei are pleomorphic with occasional prominent nucleoli
- Mitoses are rare, something found only in hot areas
- Frequent involvement of the dermis and subcutis
- Rhabdoid
- Rhabdoid cells have plasmacytoid appearance, round to oval contour and large amounts of cytoplasm with refractive, deeply eosinophilic material (Int J Clin Exp Pathol 2014;7:840)
- Nuclei are crescent or round shaped, disposed polar to the cytoplasm against the cellular membrane
- Hyperchromatism, pleomorphism, high mitotic rate and single cell necrosis are frequent
- Verrucous
- Striking epidermal and adnexal hyperplasia with thickened epidermis, dyskeratotic cells, squamous eddies and keratotic cysts (Cureus 2022;14:e29098)
- Strikingly atypical proliferation of melanocytes at the junction and in the dermis
- Rare pagetoid spread
- Signet ring
- Large cells containing a big roundish cytoplasmic vacuole (Am J Dermatopathol 2014;36:985)
- Nuclei seem to be pushed against the cell membrane, with a crescent shaped silhouette
- Small cell
- 2 variants: small cells, so called non-Merkel tumor-like cell variant and large cells, Merkel cell tumor-like variant (Dermatopathology (Basel) 2019;6:231)
- Small or barely visible cytoplasm with hyperchromatic nucleus with coarse chromatin
- Cells are atypical and mitoses are easily found
- No maturation as the lesion goes deeper
- Monotonous cells
- Pigment is usually rare and focal
- Myxoid
- Dendritic or stellate melanocytes scattered in abundant mucinous material
- Large nuclei and irregularly clumped nuclear chromatin (J Am Acad Dermatol 2002;46:264)
- Rare mitoses in myxoid background
- Scarce melanin
- Osteogenic (osseocartilaginous differentiation)
- Atypical melanocytes with chondroid or osteoid metaplasia (J Am Acad Dermatol 2002;46:264)
- Dedifferentiated / undifferentiated
- Pleomorphic, atypical cells, with numerous mitotic figures; nuclei with thinned chromatin and numerous central and peripheral nucleoli (Am J Surg Pathol 2021;45:240)
Microscopic (histologic) images
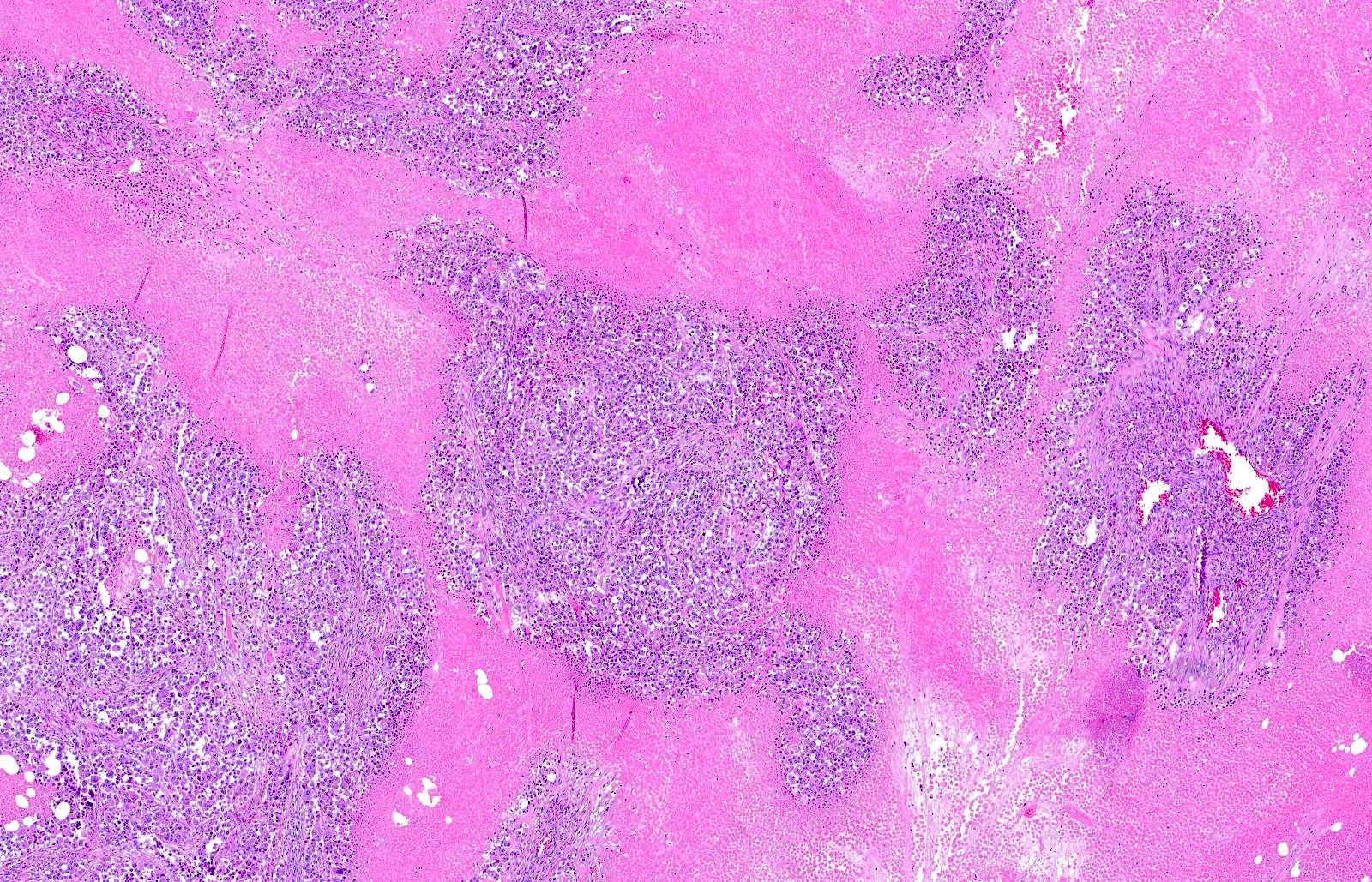
Contributed by Gerardo Cazzato, M.D., Ph.D.
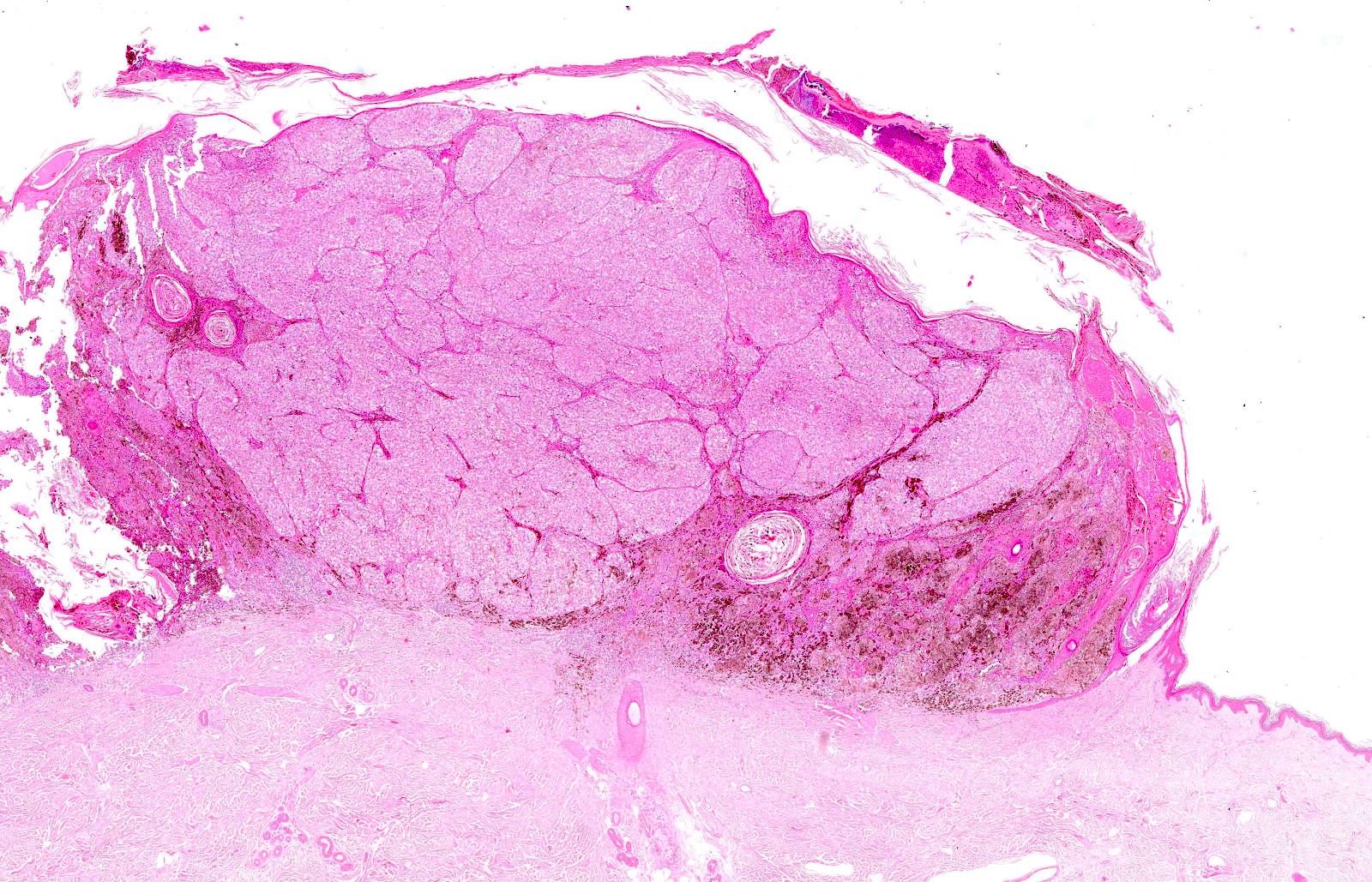
Melanocytes with clear / balloon cytoplasm
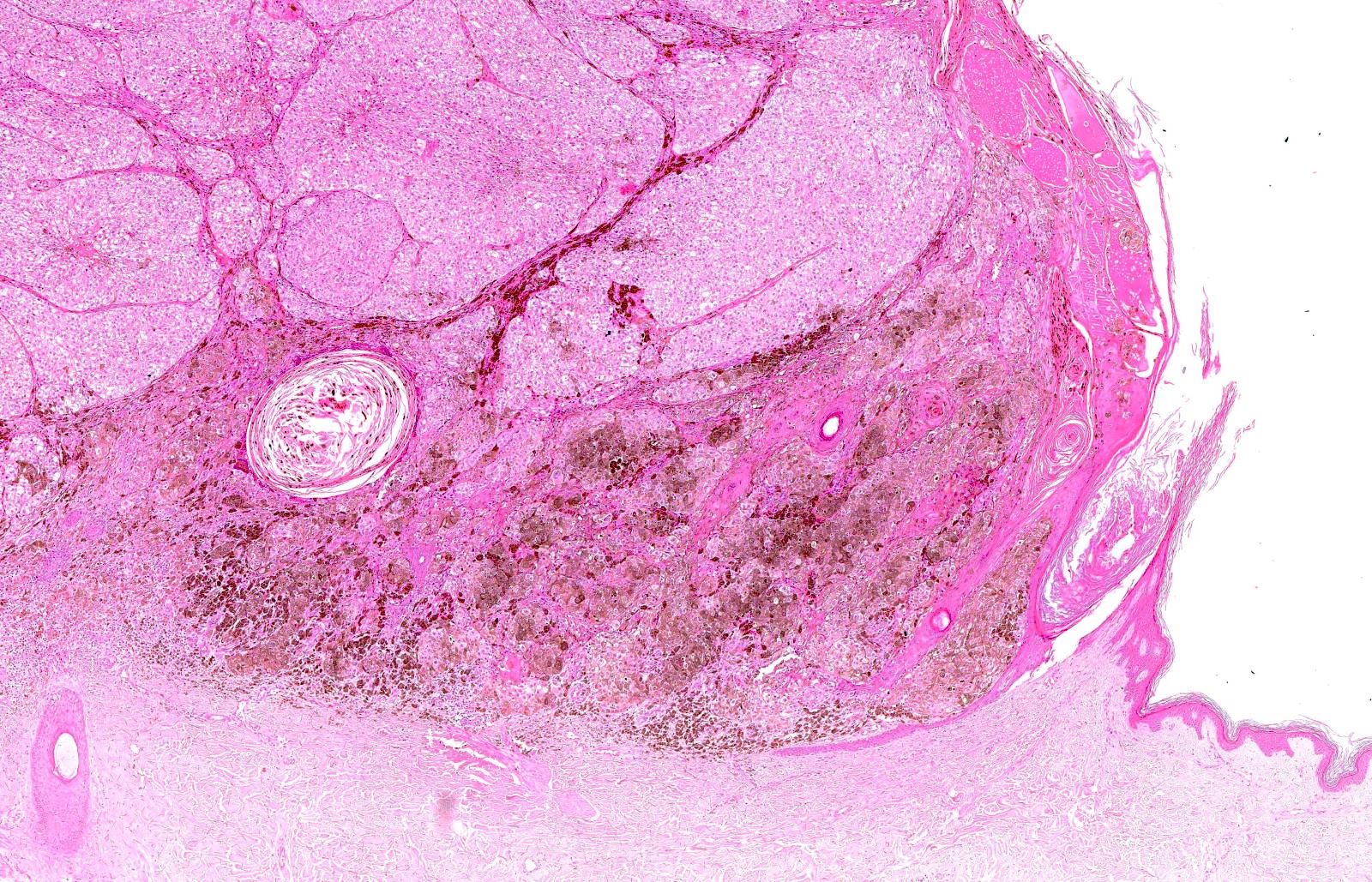
Balloon cell with atypia
Rhabdoid melanocytes within necrosis
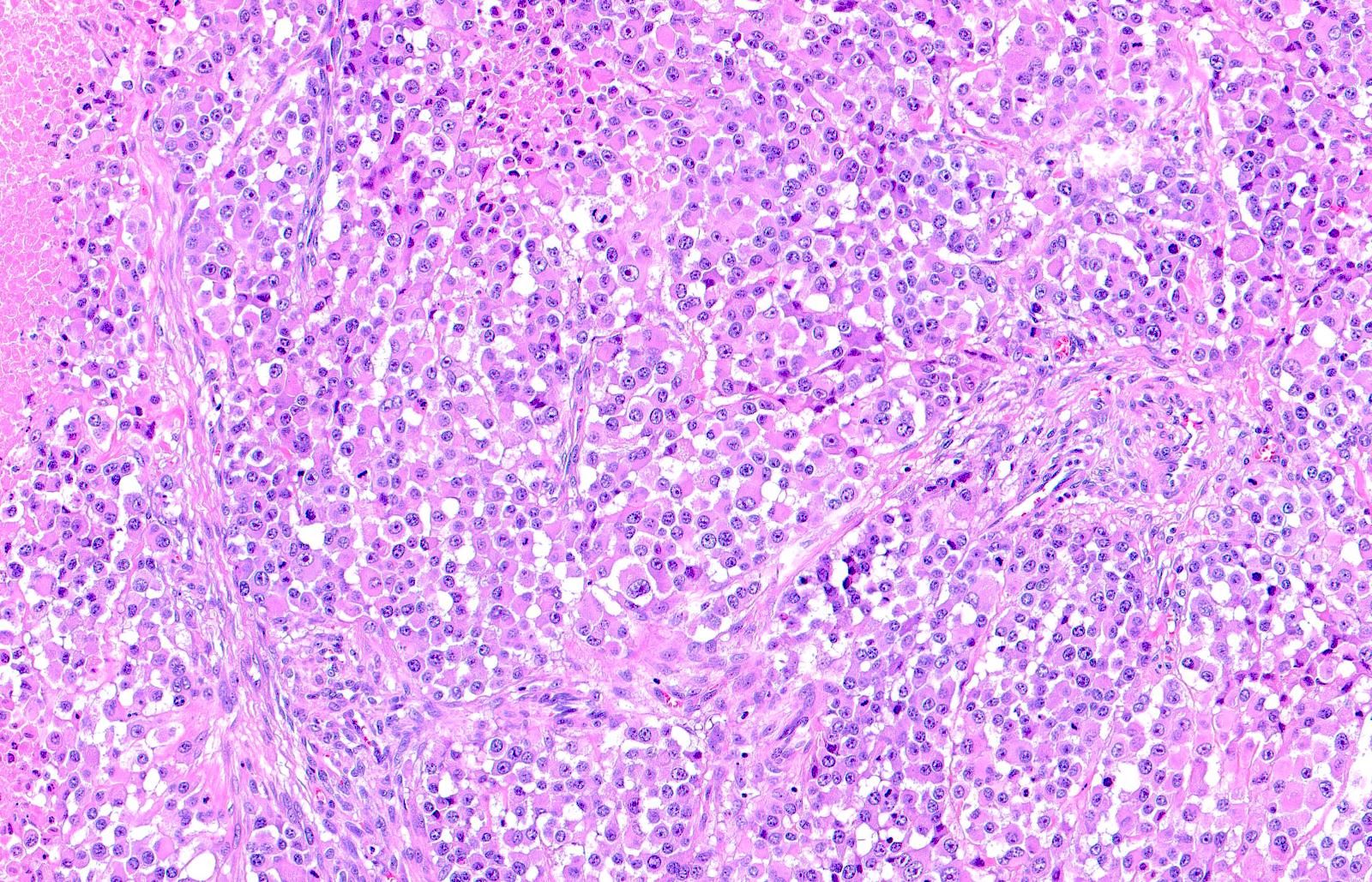
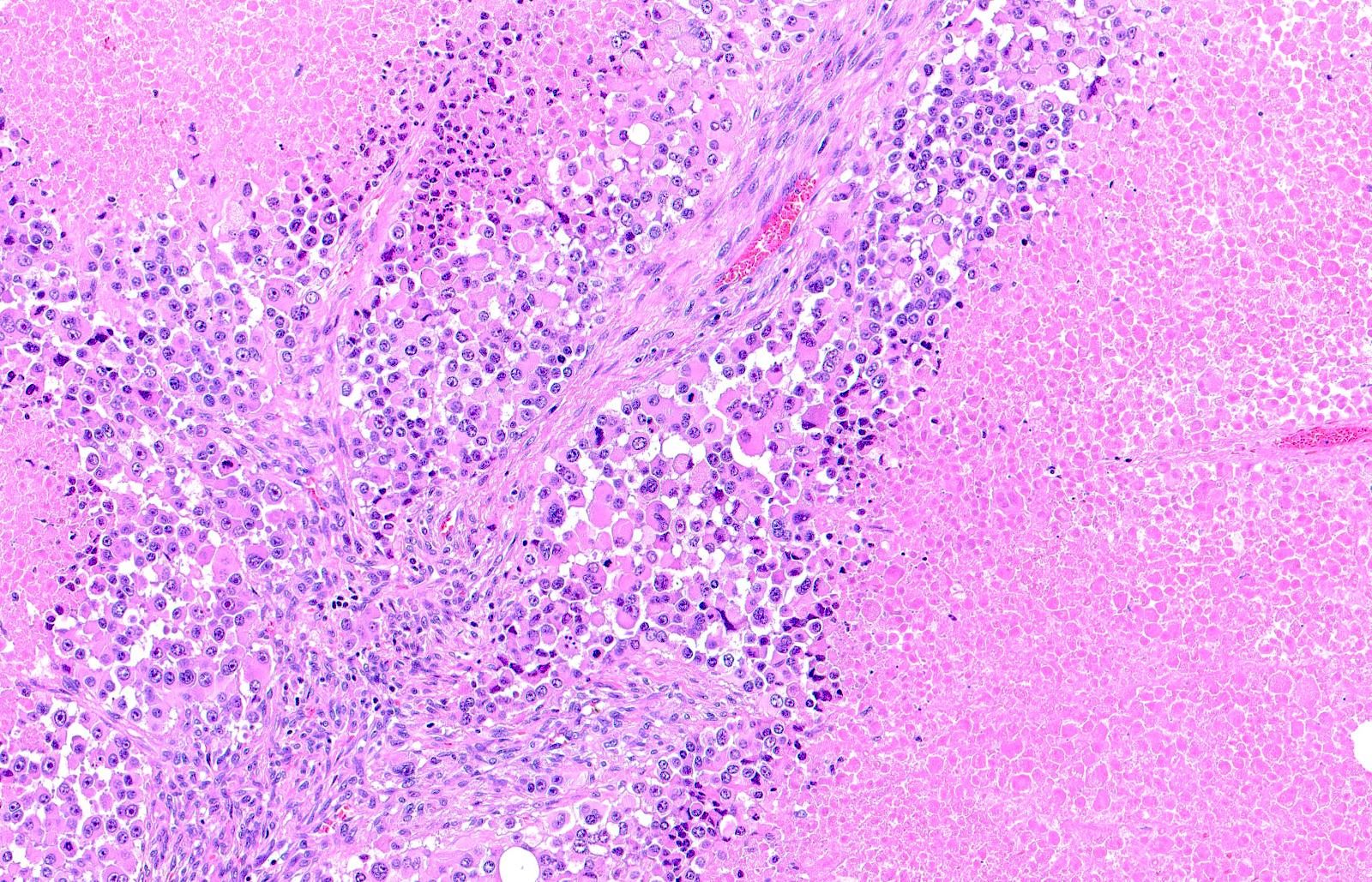
Rhabdoid melanocytes with mitoses
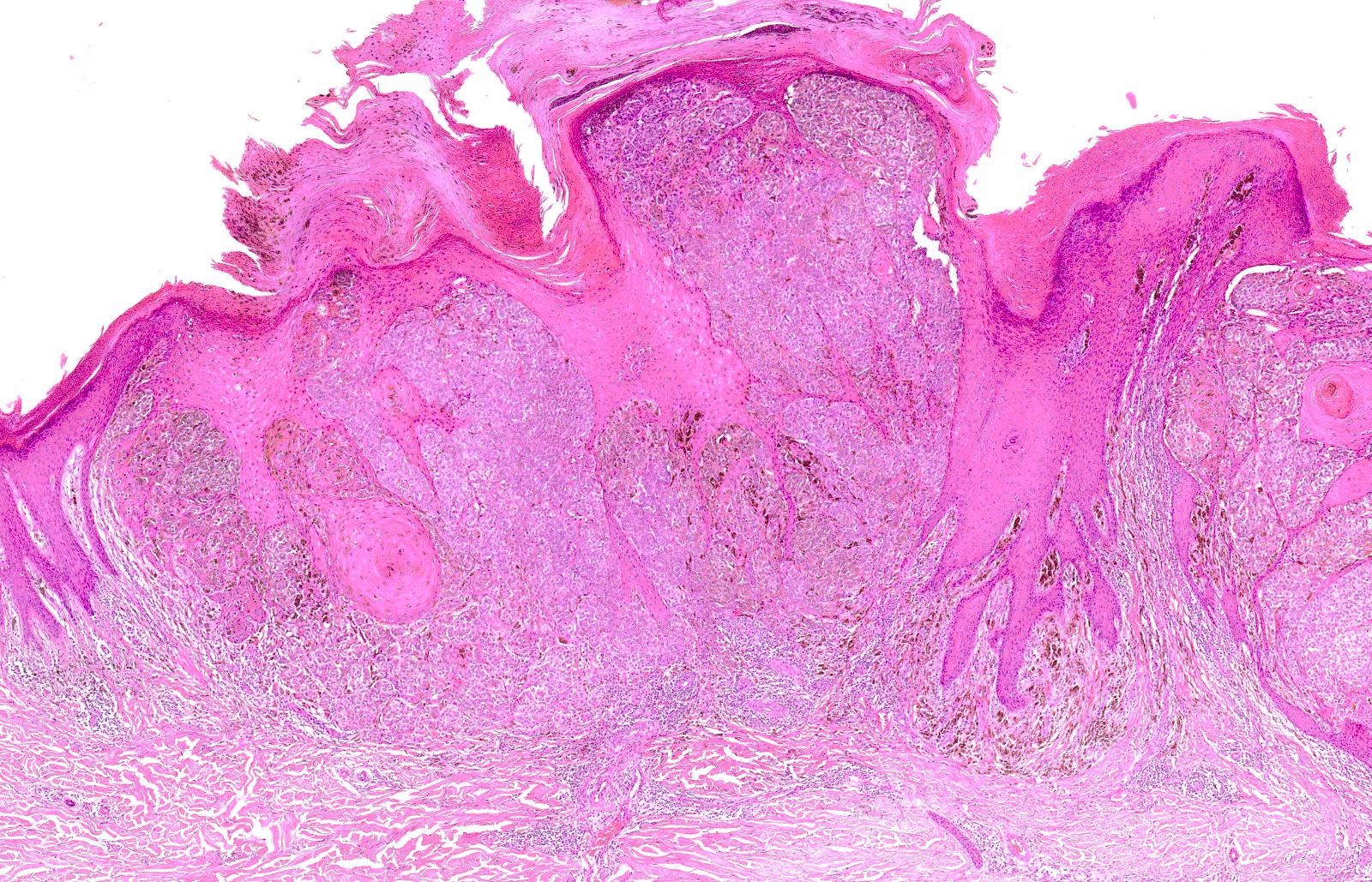
Striking atypical melanocytic proliferation
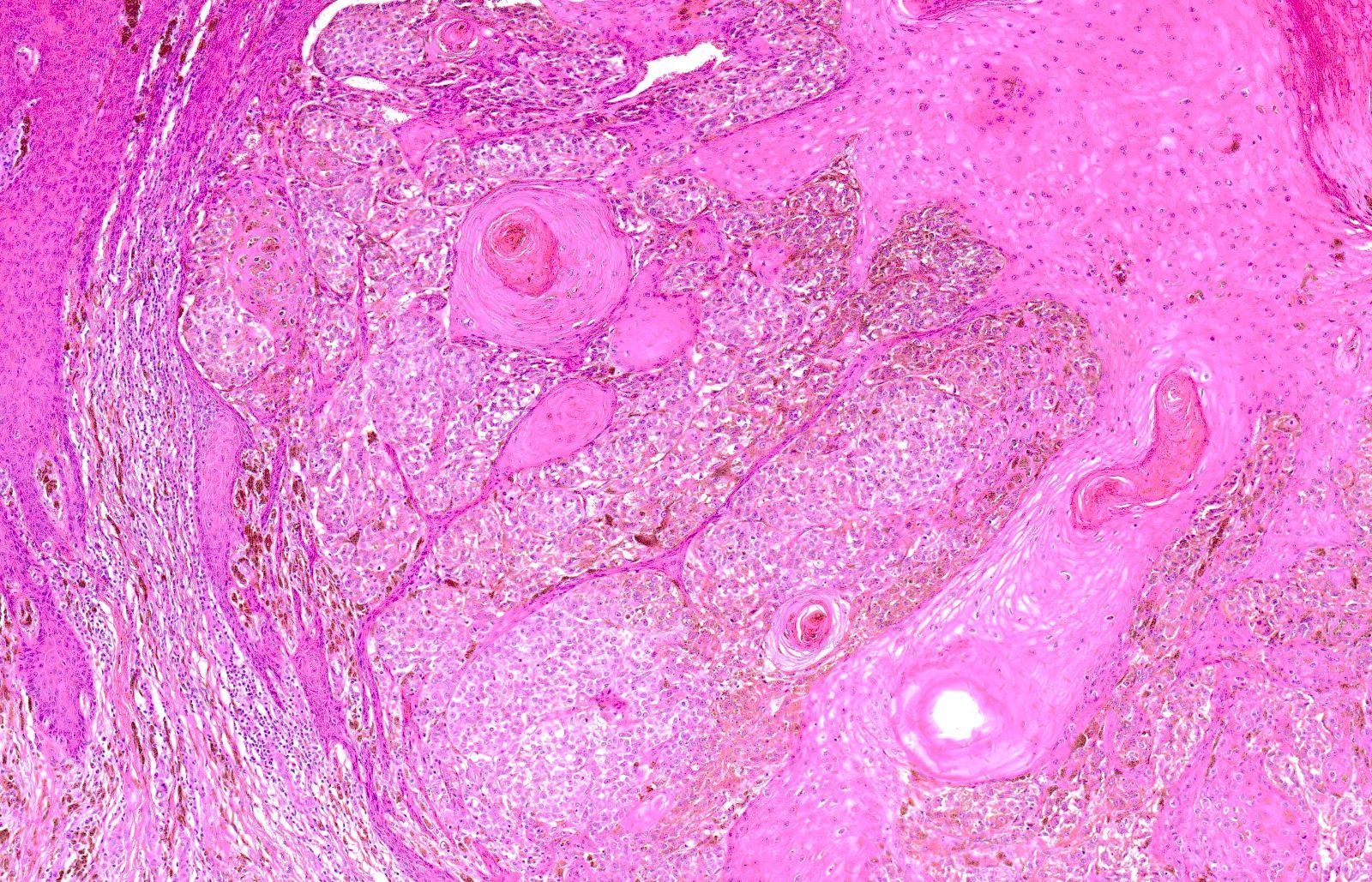
Melanoma with pseudo-epitheliomatous hyperplasia
Images hosted on other servers:

Signet ring cell melanoma

Small cell melanoma

Myxoid melanoma
Positive stains
- Balloon cell
- S100, HMB45: diffusely and strongly positive but also MelanA and SOX10 (Dermatopathology (Basel) 2022;9:100)
- MITF usually positive, also PRAME (Diagn Cytopathol 2017;45:828)
- Rhabdoid
- S100, HMB45: diffusely and strongly positive (rare cases negative for both); consistent expression of vimentin and sometimes, desmin
- Sometimes aberrant expression of cytokeratin (CK), SMA and synaptophysin
- SOX10
- PRAME usually positive (Dermatopathology (Basel) 2022;9:148)
- Verrucous
- Usually same as conventional melanoma
- SOX10
- Usually MITF and PRAME positive
- Signet ring cell
- Small cell
- Usually same as conventional melanoma
- SOX10
- Myxoid
- Osteogenic
Negative stains
- Rhabdoid
- Dedifferentiated / undifferentiated
- Almost all negative (Am J Surg Pathol 2021;45:240)
- Usually MITF and PRAME negative
Molecular / cytogenetics description
- Dedifferentiated / undifferentiated: detection of a melanoma compatible gene mutation, such as BRAF or NRAS, aids in diagnosis (Am J Surg Pathol 2021;45:240)
Videos
Rhabdoid melanoma
Small cell melanoma
Sample pathology report
- Limb skin, excisional biopsy:
- Melanoma with rhabdoid cell features (see comment)
- Comment: Sections of skin and subcutis including a proliferation of cells with a plasmacytoid appearance, characterized by round / oval outlines and large amounts of cytoplasm containing eosinophilic material with a glassy hyaline but sometimes filamentous appearance. The cell nuclei (hyperchromatic, pleomorphic) are crescent shaped or round and arranged polar to the cytoplasm against the cellular membrane.
Differential diagnosis
- Balloon cell
- Balloon cell nevus:
- Symmetrical, usually papillated, small, round melanocytes and roundish, small, monomorphous nuclei
- No mitosis, atypia
- Renal cell carcinoma (RCC):
- Clear cells arranged in solid sheets with a delicate branching vasculature
- Carbonic anhydrase IX, CD10 positive
- Clear cell sarcoma:
- Much deeper and balloon cells are without the vacuoles
- S100 positive such as balloon cell melanoma
- Xanthoma:
- No atypia, histiocytes
- Liposarcoma:
- Lipoblasts
- Eccrine acrospiroma:
- Different cellular components
- Atypical fibroxanthoma (AFX):
- Pleomorphic cells, negative for melanocytic markers
- Granular cell tumor (GCT)
- Cells with abundant, granular cytoplasm with occasional neurotropism
- Balloon cell nevus:
- Rhabdoid
- Rhabdomyosarcoma:
- Cells with rhabdoid morphology, usually positive for skeletal muscle markers
- Rhabdoid renal tumor metastatic to the skin
- Rhabdoid ovarian tumor metastatic to the skin
- Malignant peripheral nerve sheath tumor (MPNST), epithelioid variant:
- Positive for EMA and synaptophysin
- Different clinical setting
- S100 and vimentin can be positive
- Malignant form of primitive neuroectodermal tumor (PNET):
- Rhabdoid appearance of carcinoma:
- CK strongly expressed
- Rhabdomyosarcoma:
- Verrucous
- Carcinoma or other epithelial neoplasms:
- Different immunohistochemistry
- Spitz nevus with pseudocarcinomatous hyperplasia:
- More nests of melanocytes than sheets
- No atypia
- No mitotic figures
- Carcinoma or other epithelial neoplasms:
- Signet ring cell
- Primitive cutaneous or metastatic signet ring carcinoma
- Liposarcoma:
- Lipoblasts; absence of real signet ring cell
- Lymphoma:
- Lymphoid cells, positive for CD45 LC and other lymphocytic markers
- Squamous cell carcinoma
- Basal cell carcinoma
- Epithelioid hemangioma
- Hemangioendothelioma
- Small cell
- Lymphoma:
- Lymphoid cells, positive for CD45 LC and other lymphocytic markers
- Merkel cell carcinoma
- MPNST
- Small cell metastatic carcinoma
- PNET
- Neuroblastoma
- Proliferative nodule in children
- Lymphoma:
- Myxoid
- Malignant
- Benign
- Mucinosis:
- Different background; no cells
- Melanocytic nevi with mucinous change
- Myxoid schwannoma
- Neurofibroma
- Chondroid syringoma
- Mucinosis:
- Osteogenic
- Nevi with metaplastic changes
- MPNST with osteochondroid metaplasia
- Dedifferentiated / undifferentiated
- Carcinomas:
- Different lineage of cells; variable positivity for epithelial markers
- High grade sarcomas:
- Different lineage of cells; molecular biology necessary
- Carcinomas:
- Reference: Massi: Histological Diagnosis of Nevi and Melanoma, 2nd Edition, 2014
Board review style question #1
A 61 year old man with a history of melanoma of the right preauricular region presents with right lateral cervical swelling. Which of the following statements is true regarding this entity?
- Clinical features are pathognomonic
- S100 and HMB45 are almost always positive
- S100 is usually negative
- This lesion is usually primary cutaneous
Board review style answer #1
B. S100 and HMB45 are almost always positive. Despite the morphological peculiarities of rhabdoid melanoma, immunohistochemical investigations for neuroectodermal markers, such as S100 protein and HMB45, are almost always invariably positive and help the pathologist in the correct differential diagnosis with other entities of striated muscle lineage. Rhabdoid melanoma can present with widespread and strong positivity for vimentin and sometimes for desmin, while usually MelanA is negative. Answer A is incorrect because rhabdoid melanoma doesn't have any clinical pathognomonic features. Answer C is incorrect because S100 is usually positive, not negative. Answer D is incorrect because the metastatic setting is more common than primary cutaneous setting in case of rhabdoid melanoma.
Comment Here
Reference: Melanomas with unusual features
Comment Here
Reference: Melanomas with unusual features
Board review style question #2
What are the characteristics that allow a differential diagnosis between balloon cell melanoma and balloon cell nevus?
- Melanin
- Mitoses, large nuclei, distinct and large nucleoli, architecture of the neoplasm and intraepidermal pagetoid scatter of balloon cells
- Percentage of balloon cell component
- Positivity for MelanA
Board review style answer #2
B. Mitoses, large nuclei, distinct and large nucleoli, architecture of the neoplasm and intraepidermal pagetoid scatter of balloon cells. It is important to remember that the parameters used in the differential diagnosis of common forms of melanoma are the same as with unusual and rare forms of melanoma; therefore, in differentiating a balloon cell melanoma from a balloon cell nevus, it is essential to rely on the criteria we know. Answer D is incorrect because positivity for MelanA is not useful for a differential diagnosis. Answer A is incorrect because presence of melanin is not a criterion. Answer C is incorrect because the percentage of melanocytes with balloon cell appearance is useful for the diagnosis of a balloon cell lesion but not in distinguishing a nevus from a melanoma.
Comment Here
Reference: Melanomas with unusual features
Comment Here
Reference: Melanomas with unusual features
