
Skin nontumor
Infectious disorders
Syphilis
Author: Silvija P. Gottesman, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 24 March 2020
Last staff update: 5 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Syphilis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gottesman SP. Syphilis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorsyphilis.html. Accessed April 3rd, 2025.
Definition / general
- Syphilis is primarily a sexually transmitted disease
- Clinically, in the secondary stage, presents with a papulosquamous eruption and has many histologic mimickers, including psoriasis
Essential features
- Lichenoid superficial and deep perivascular and periadnexal lymphohistiocytic inflammation with admixed plasma cells
- Up to 33% of biopsies may lack plasma cells
- Immunohistochemistry is more sensitive than silver stains
Terminology
- Lues venerea, Cupid's disease
ICD coding
- ICD-10: A51.39 - other secondary syphilis of the skin
Epidemiology
- Transmitted via sexual contact
- Can also be transmitted congenitally and rarely via blood products
- More prevalent in men than in women, especially ages 20 - 29
- Higher incidence in gay and bisexual men (MMWR Morb Mortal Wkly Rep 2014;63:402)
Sites
- Skin, mucosal surfaces, eyes, brain / nerves, blood vessels, bones, joints and liver (CDC: Syphilis [Accessed 11 December 2019])
Pathophysiology
- On skin to skin contact, it enters via areas of microtrauma, multiplies locally and disseminates systemically within 24 hours (Infect Dis Clin North Am 2013;27:705)
Etiology
- Treponema pallidum, highly motile coiled spirochete
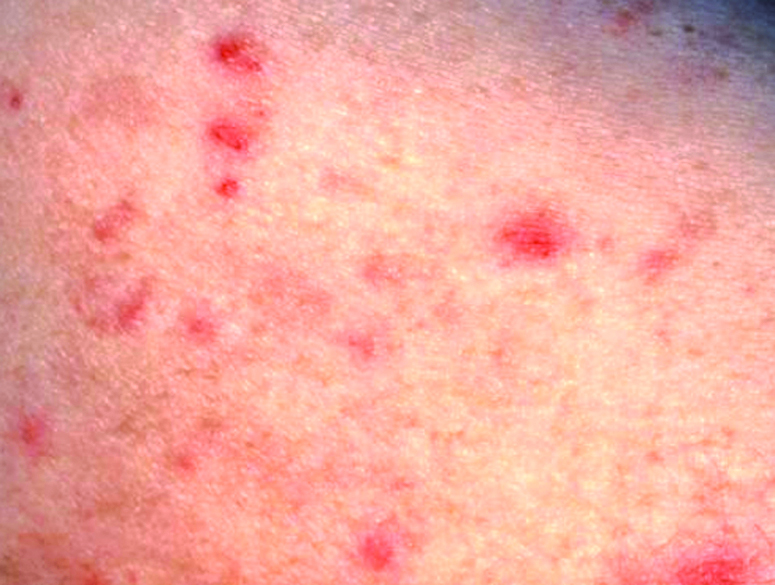
Clinical features
- Primary syphilis: painless chancre with nontender lymphadenopathy 1 - 3 weeks after exposure
- Secondary syphilis:
- Papulosquamous thin papules on the trunk and extremities, palms and soles, fever and adenopathy
- Rash may resemble a drug eruption, pityriasis rosea and psoriasis
- May present as moth eaten alopecia on the scalp, mucous patches on tongue
- Tertiary syphilis: may present with gummatous lesions, neurologic or cardiovascular symptoms (Infect Dis Clin North Am 2013;27:705)
- Lymph node: solitary inguinal lymphadenopathy associated with syphilitic chancre
Diagnosis
- T. pallidum can be visualized using darkfield microscopy
- Blood and cerebrospinal fluid (CSF) analysis
- Skin biopsy for H&E, special stain and immunohistochemical analysis (Infect Dis Clin North Am 2013;27:705)
Laboratory
- Nontreponemal and treponemal tests are performed on blood serum
- Nontreponemal tests: rapid plasma reagin (RPR) test or venereal disease research laboratory (VDRL) test
- Treponemal tests: Treponema pallidum particle agglutination assay (TPPA) or fluorescent treponemal antibody absorption (FTA-ABS) test
- Cerebrospinal fluid (CSF) analysis
- Lymphocytic pleocytosis and elevated cerebrospinal fluid total protein
- Cerebrospinal fluid venereal disease research laboratory test confirms diagnosis of neurosyphilis
- Of note, cerebrospinal fluid fluorescent treponemal antibody absorption test has a high false positive rate but is more sensitive than cerebrospinal fluid venereal disease research laboratory test
Prognostic factors
- Favorable with early treatment
Case reports
- 27 year old man presents with recurrent oral ulcers (J Indian Acad Oral Med Radiol 2014;26:436)
- Man in his late 20s presented with a rash and multiple lytic lesions of the bones (BMJ Case Rep 2014 Sep 19;2014)
- 36 year old man with progressive vision loss (Case Rep Infect Dis 2014;2014:352047)
- 39 year old man presents with generalized weakness, joint aches (Cleve Clin J Med 2017;84:510)
- 59 year old man presents with ulcer of the hard palate (J Med Case Rep 2019;13:227)
Treatment
- Penicillin is the main drug of choice
- If a pregnant patient with syphilis is allergic to penicillin, an attempt should be made on penicillin desensitization with an allergist
- Other medications for nonpregnant adults are doxycycline, tetracycline and ceftriaxone (Infect Dis Clin North Am 2013;27:705, CDC: Syphilis [Accessed 11 December 2019])
Clinical images
Contributed by Mark R. Wick, M.D.
Secondary

Gumma
Microscopic (histologic) description
- Primary syphilis: ulcer with lymphoplasmacytic inflammation
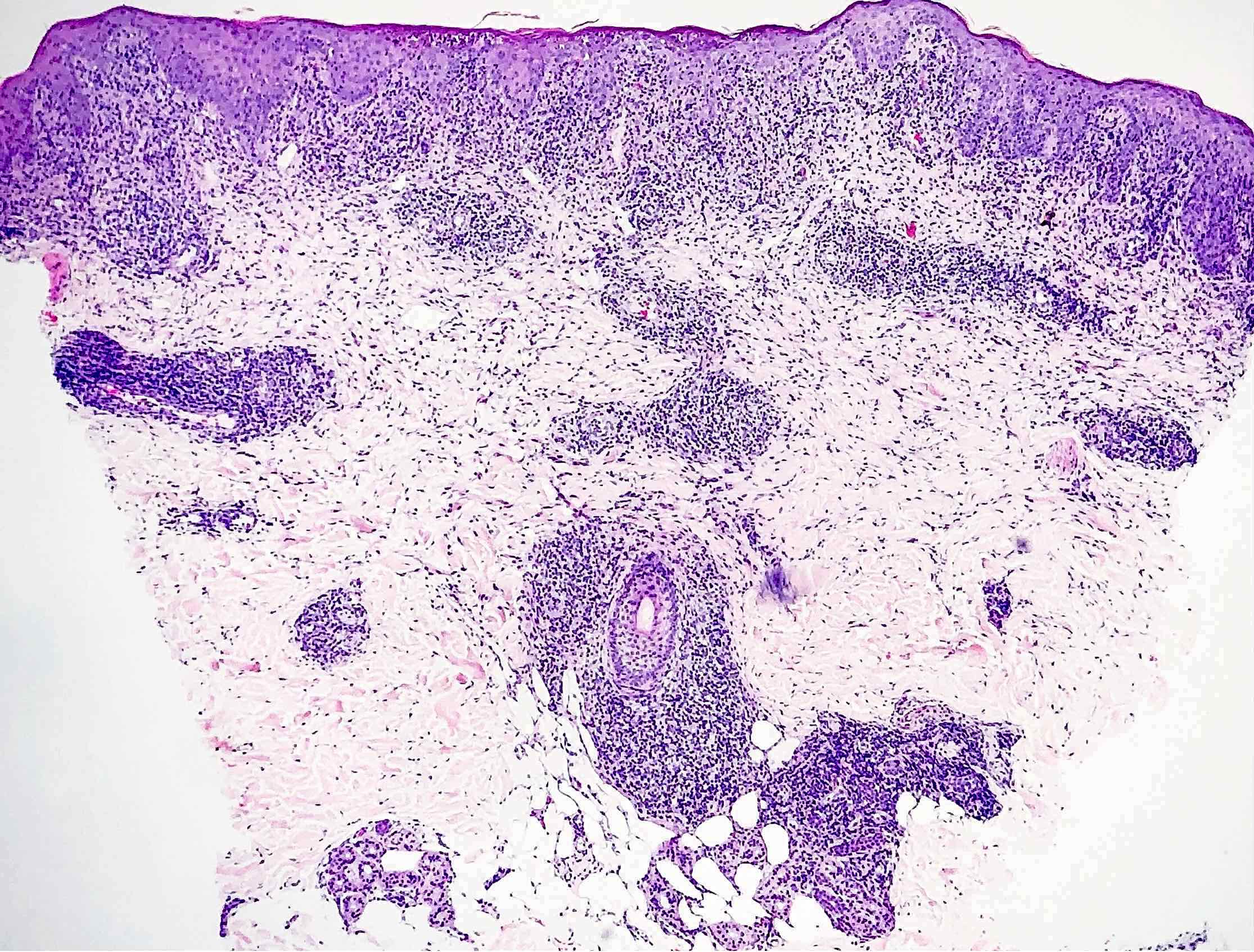
- Secondary syphilis:
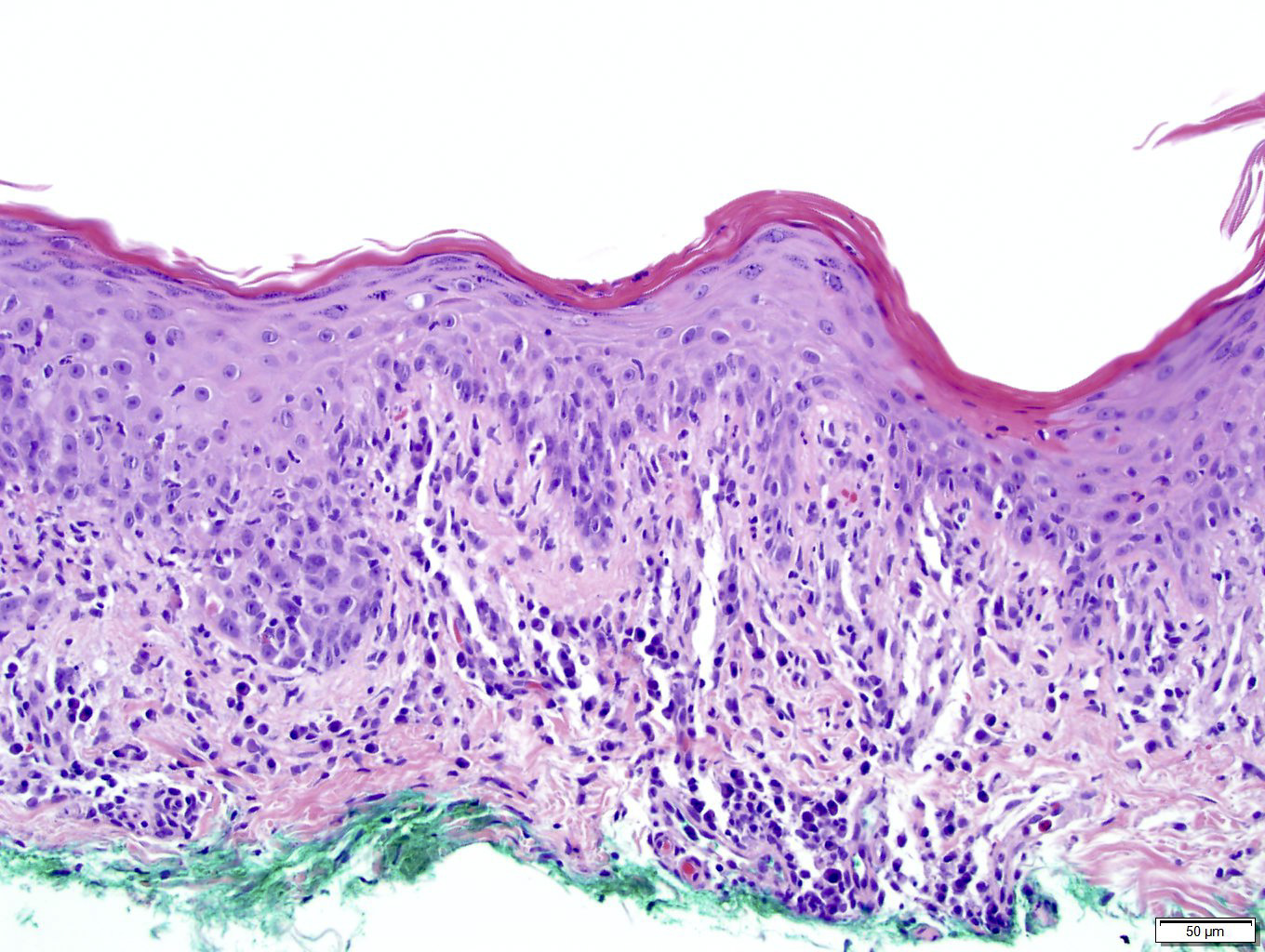
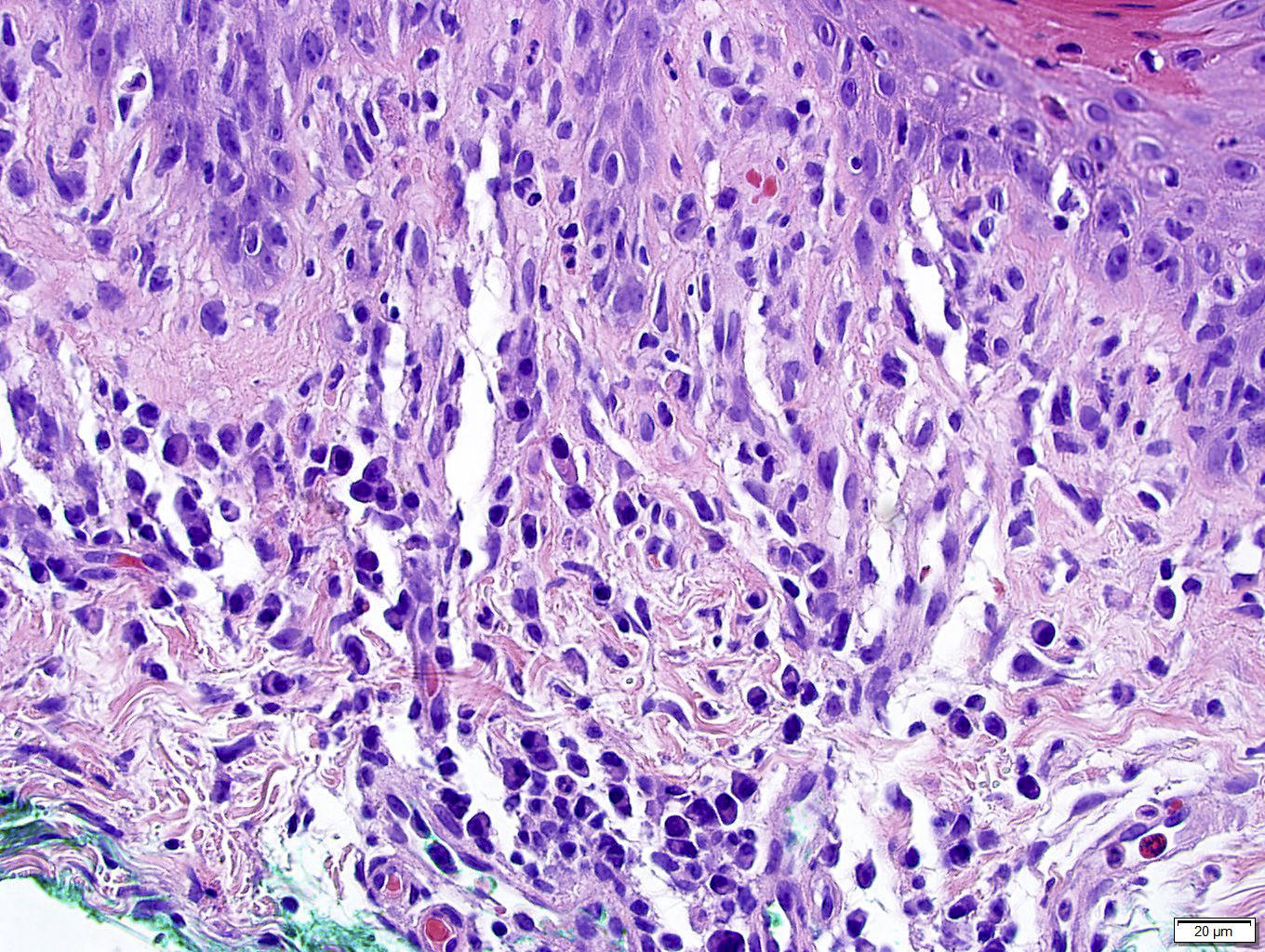
- Lichenoid superficial and deep perivascular and periadnexal lymphohistiocytic inflammation with admixed plasma cells
- Plasma cells may be absent in 33% of biopsies
- Eosinophils can be present
- Marked endothelial swelling and proliferation of blood vessels can be seen
- Commonly identified are vacuolar interface change, acanthosis or lymphocyte exocytosis
- In late secondary syphilis, granulomatous inflammation may be present
- Microabscess formation of the hair follicle has also been seen
- Condyloma lata (lesions on genital skin) show marked epidermal hyperplasia and inflammatory infiltrate akin to secondary syphilis
- Tertiary syphilis: large areas of necrosis with peripheral mixed inflammatory infiltrate and Langhans giant cells
- Lymph node:
- Primary syphilis:
- Capsular and pericapsular fibrosis, follicular hyperplasia, diffuse interfollicular plasma cells, prominent endarteritis outside the capsule
- Noncaseating granulomas and abscesses are rare
- Spirochetes easiest to identify within blood vessel walls
- Secondary / tertiary syphilis: follicular hyperplasia
- Primary syphilis:
- References: J Cutan Pathol 2004;31:595, J Am Acad Dermatol 2015;73:1025, J Am Acad Dermatol 2020;82:156
Microscopic (histologic) images
Contributed by Silvija P. Gottesman, M.D., Hillary Rose Elwood, M.D., Mark R. Wick, M.D. and AFIP images
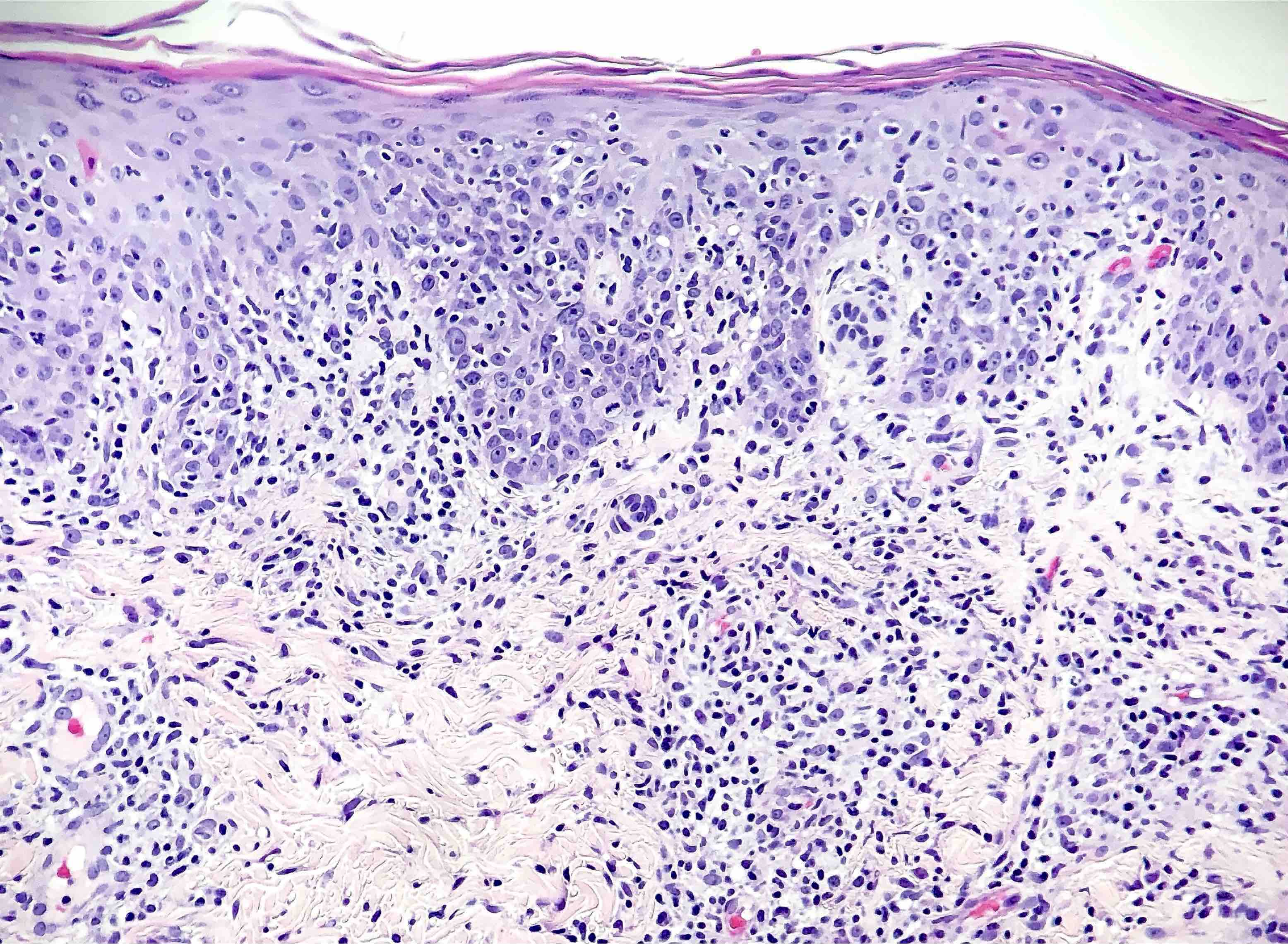
Dense lymphohistiocytic inflammation

Plasma cells
Psoriasiform hyperplasia
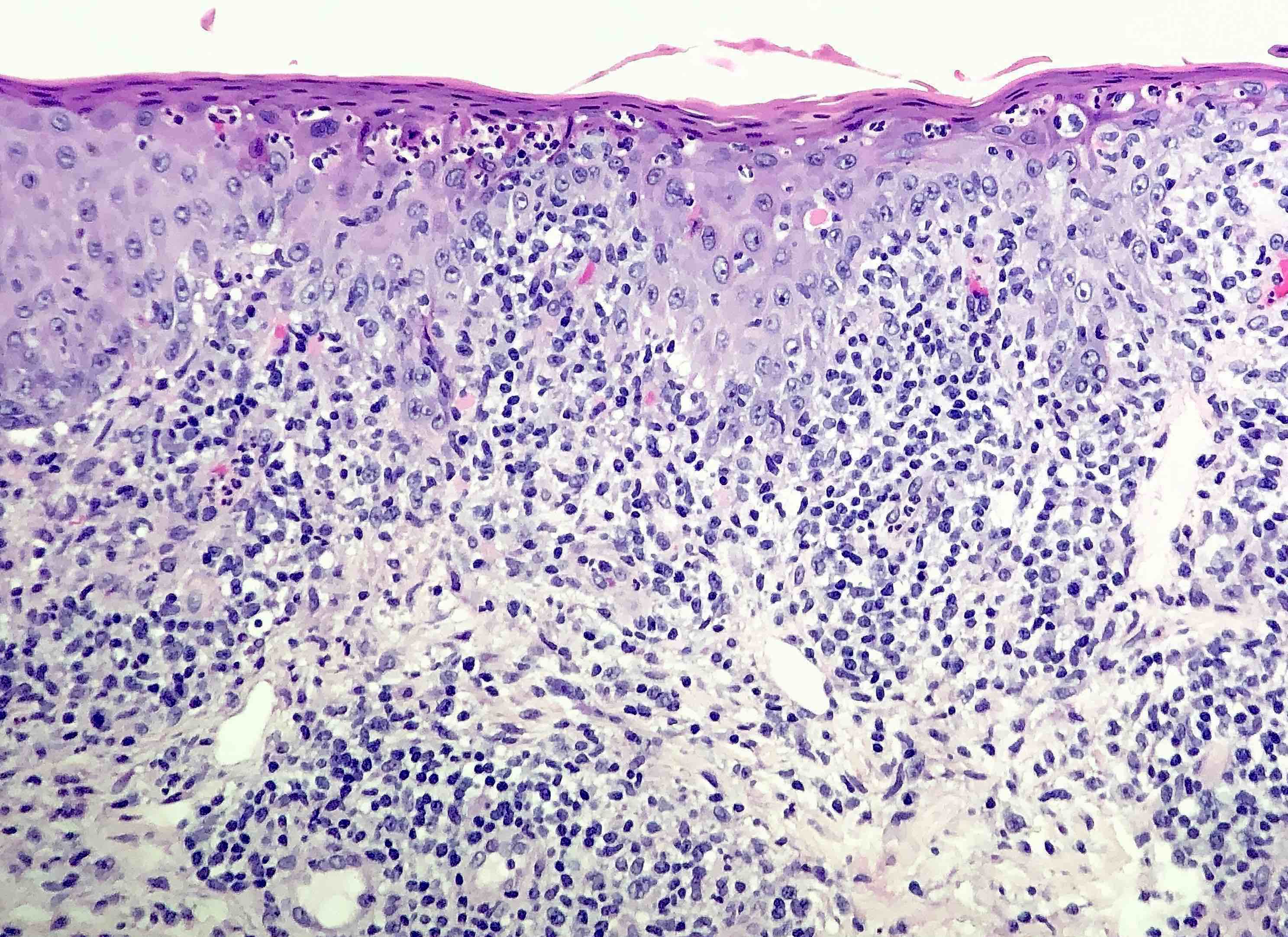
Secondary syphilis
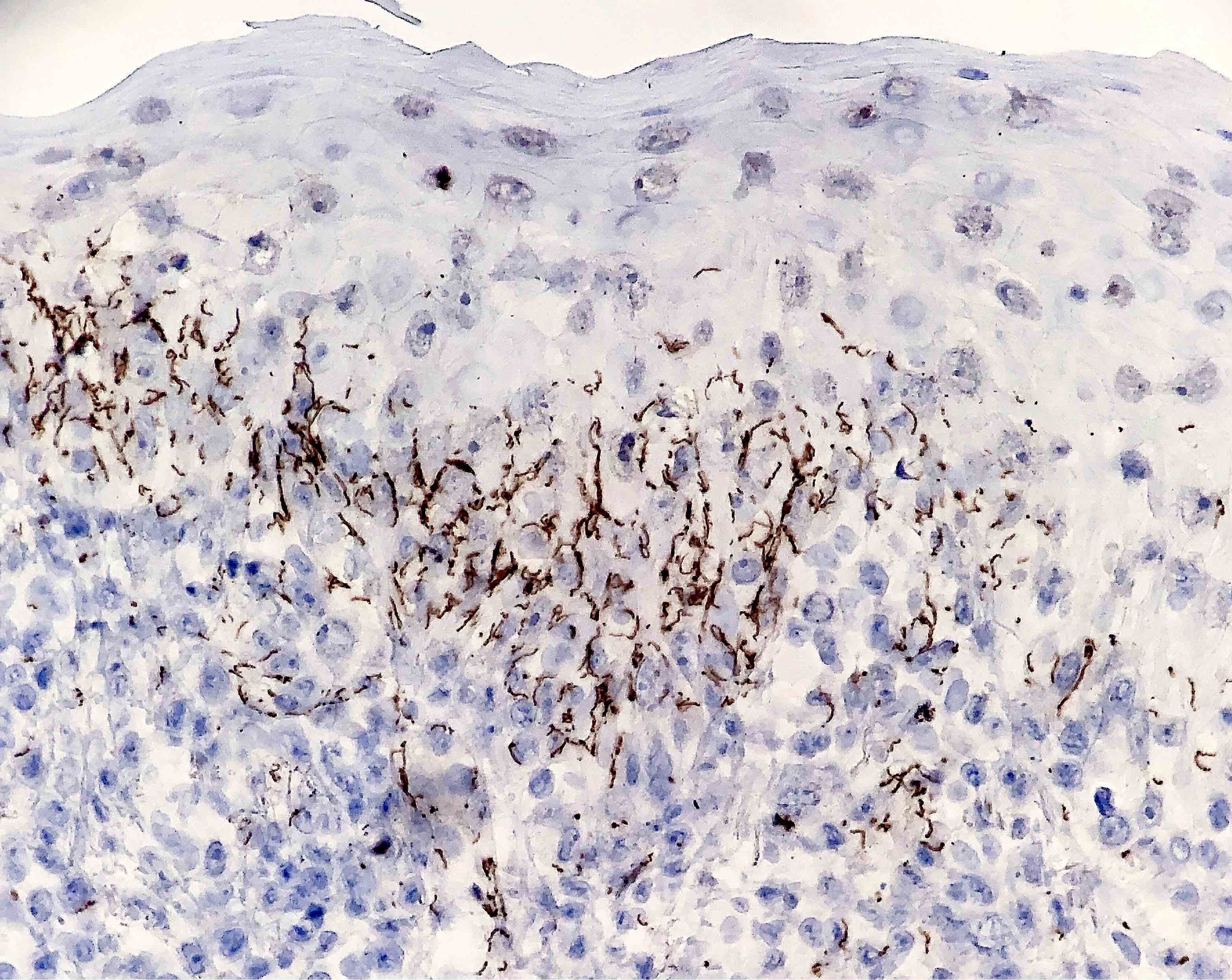
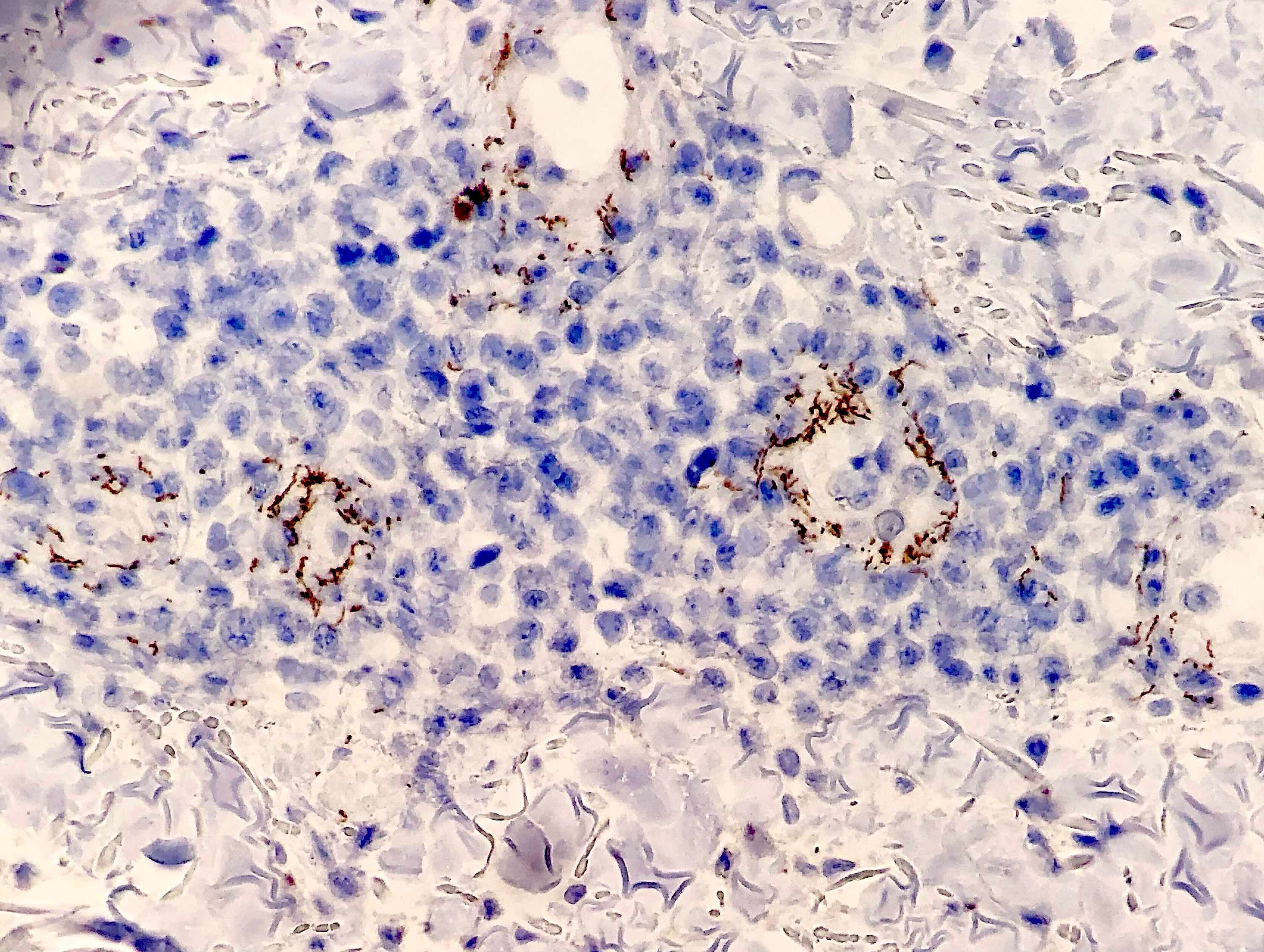
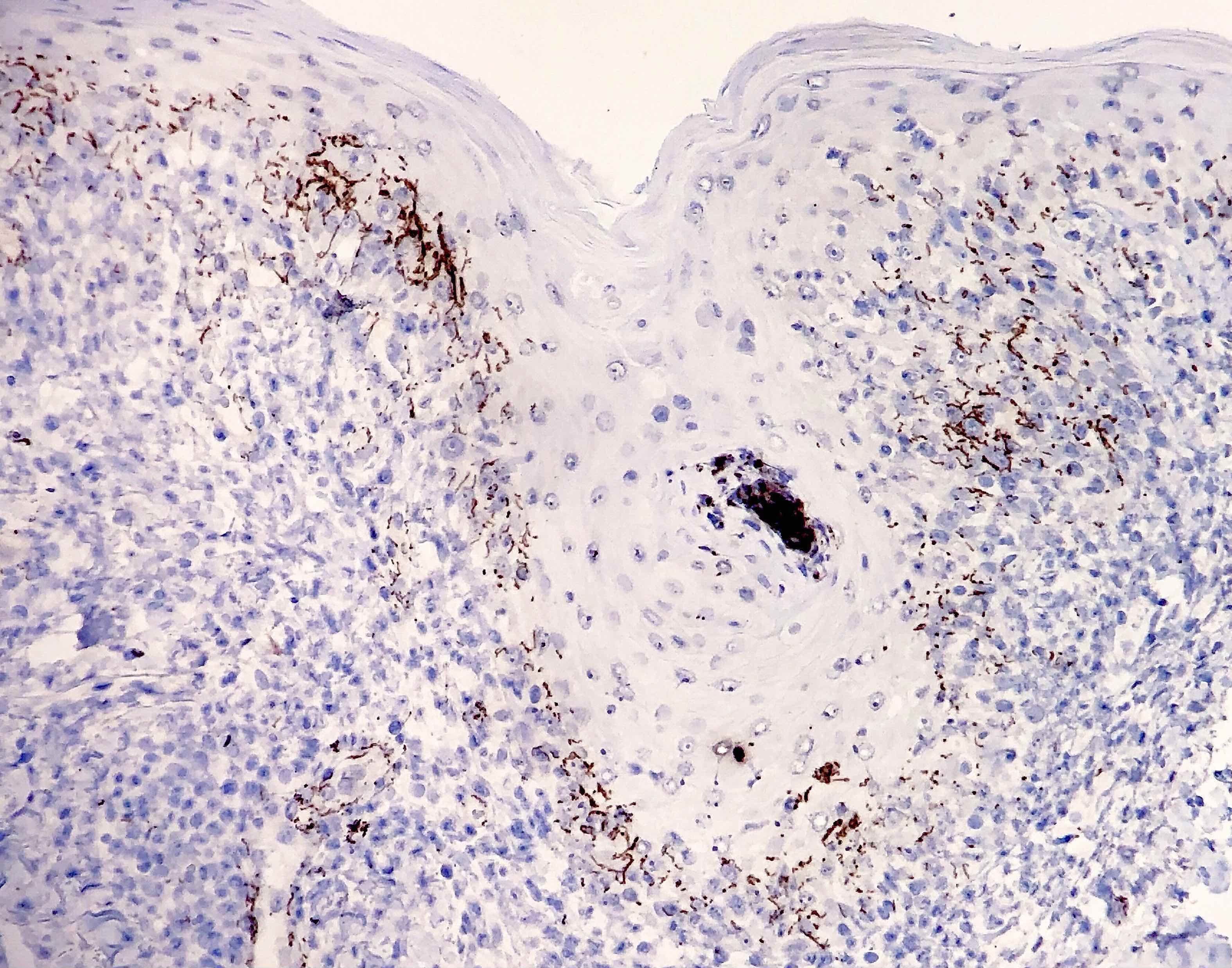
Treponemal spirochetes
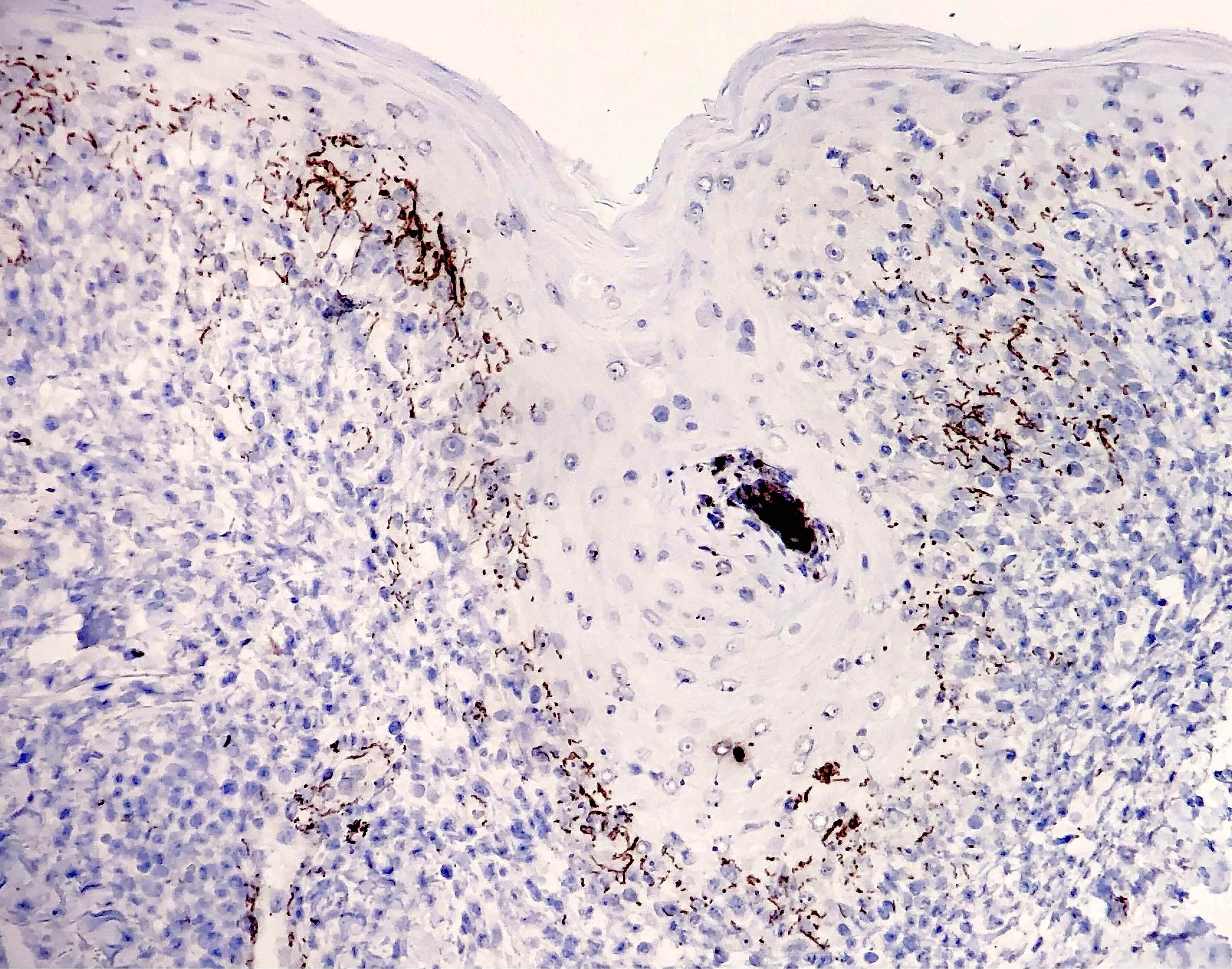
Numerous spirochetes
Dense plasma cell infiltrate
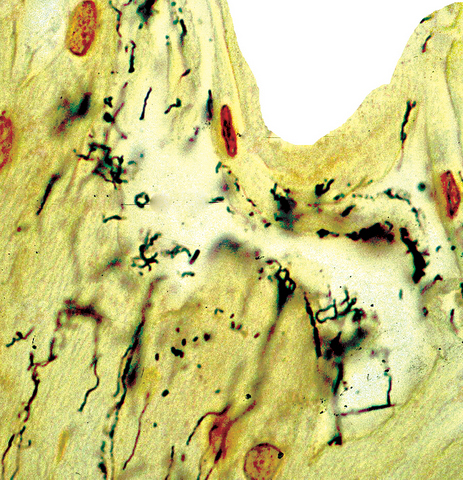
Steiner stain, secondary
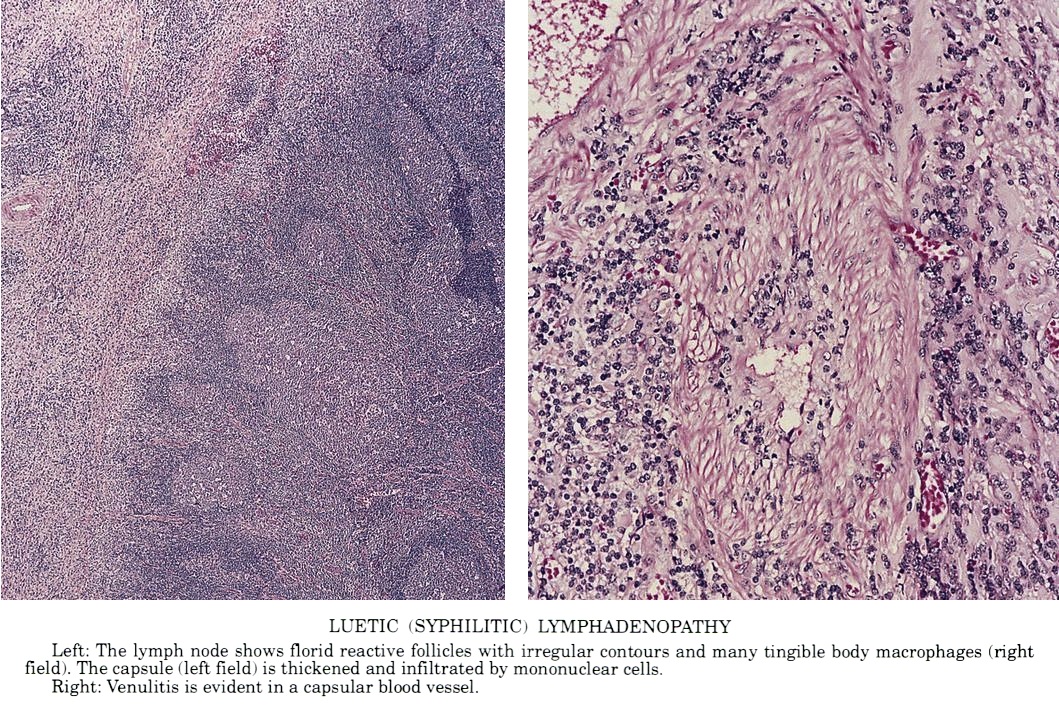
Luetic (syphilitic) lymphadenopathy
Positive stains
- Silver stains: Warthin-Starry or Steiner stain (41% sensitive) (J Cutan Pathol 2004;31:595)
- Immunohistochemical stain: treponema (71% sensitive) (J Cutan Pathol 2004;31:595)
Negative stains
- Not relevant to the diagnosis
Molecular / cytogenetics description
- PCR based techniques can be used on tissue
Sample pathology report
- Skin, punch biopsy:
- Psoriasiform lymphohistiocytic inflammation with plasma cells (see comment)
- Comment: There is psoriasiform epidermal hyperplasia with superficial and deep perivascular lymphohistiocytic infiltrate. Admixed plasma cells are also noted. The infiltrate forms a band beneath the hyperplastic epidermis and envelopes some of the adnexal structures. Endothelial swelling of the superficial vascular plexus is present. A treponemal immunohistochemical stain shows numerous coiled spirochetes in the lower half of the epidermis. These findings are diagnostic of syphilis.
Differential diagnosis
- Pityriasis lichenoides et varioliformis acuta:
- Differentiation on histologic grounds is difficult as some cases may also have plasma cells
- Treponema-, silver-
- Pityriasis rosea:
- Similar clinically
- Basilar spongiosis and extravasated red blood cells are more likely
- Neutrophils in the stratum corneum are less common
- Mycosis fungoides:
- Papillary dermal fibrosis and complete vacuolar changes are more often seen
- While late lesions may have plasma cells, they are rarely seen in early lesions
- Alopecia areata:
- Also can show peribulbar lymphocytic inflammation
- Peribulbar plasma cells will not be present
Board review style question #1
A 28 year old man presents with fever, sore throat, lymphadenopathy and a skin rash. Which of the following is the most important cutaneous finding that should prompt suspicion of syphilis?
- Erythematous scaly papules on the palms and soles
- Genital mucocutaneous ulceration
- Maculopapular eruption on the trunk and extremities
- Mucosal patches on the bilateral oral commissures
Board review style answer #1
Board review style question #2
A punch biopsy specimen from a 26 year old woman with a rash shows superficial and deep perivascular and periadnexal lymphocytic inflammation. The presence of which of the following should prompt the pathologist to order treponemal immunohistochemical stain?
- Histiocytes
- Mucin
- Neutrophils
- Plasma cells
Board review style answer #2
