
Skin nontumor
Vesiculobullous and acantholytic reaction patterns
Stevens-Johnson syndrome
Last author update: 1 February 2015
Last staff update: 11 November 2020
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Stevens-Johnson syndrome [title] skin "loattrfree full text"[sb]



Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosis | Additional referencesCite this page: Carlquist EM, Stuart LN, Gardner JM. Stevens-Johnson syndrome. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorstevensjohnsonsyndrome.html. Accessed March 31st, 2025.
Definition / general
- Historically there has been controversy as to whether Stevens-Johnson syndrome (SJS) is a distinct entity or at the center of the disease spectrum that includes erythema multiforme (EM) and toxic epidermal necrolysis (TEN)
- Currently, there is an increasing trend for SJS and TEN as representing the ends of a spectrum of severe epidermolytic adverse cutaneous drug reactions (Orphanet J Rare Dis 2010;5:39)
Terminology
- SJS: keratinocyte necrosis; epidermal detachment < 10% body surface area; the beginning of the spectrum (Orphanet J Rare Dis 2010;5:39)
- SJS / TEN: considered point of overlap of two diseases in patients with 10 - 30% body surface area epidermal detachment (N Engl J Med 1994;331:1272)
- TEN: severe disease state and the end of a spectrum of epidermolytic adverse cutaneous drug reactions; full thickness epidermal necrosis; epidermal detachment > 30% body surface area (Orphanet J Rare Dis 2010;5:39)
- Atypical SJS: referred to by some as severe mucositis with Mycoplasma pneumoniae infection but without skin lesions (Pediatrics 2007;119:e1002), while others argue that the classification of SJS requires cutaneous involvement (Pediatr Dermatol 2006;23:546)
Epidemiology
- Incidence: 1.2 - 6 per million persons per year (Allergol Int 2006;55:9)
- Increased incidence with HIV (Orphanet J Rare Dis 2010;5:39)
Sites
- Lesions usually begin on trunk and spread centrifugally
Pathophysiology
- Mechanism unknown but appears to be CD8+ T cell mediated immune reaction (J Allergy Clin Immunol 2011;127:S74)
- Granulysin, a mitochondrial protein, is most important factor in epidermal destruction; is found in blister fluid in increasing concentrations with increased severity of disease (Nat Med 2008;14:1343)
Etiology
- Cases in children are usually associated with infection, especially Mycoplasma pneumonia and herpes simplex virus
- In adults, most cases are due to medications, including:
- Allopurinol (most common cause of SJS and TEN in study of 379 patients in Europe / Israel) (J Am Acad Dermatol 2008;58:25)
- Antibiotics: sulfonamides, cephalosporins, quinolones, aminopenicillins (Orphanet J Rare Dis 2010;5:39)
- Nonsteroidal anti inflammatory drugs (NSAIDs)
- Anticonvulsants: carbamazepine, phenytoin, phenobarbital (Orphanet J Rare Dis 2010;5:39)
- Corticosteroids
- ALDEN (algorithm for assessment of drug causality in SJS and TEN) provides a structured approach to determine the responsible drug (Clin Pharmacol Ther 2010;88:60), although no identifiable cause in some cases (Orphanet J Rare Dis 2010;5:39)
Diagrams / tables
Images hosted on other servers:


SJS vs. SJS / TEN overlap vs. TEN

SCORTEN severity of illness score
Clinical features
- Drug associated cases typically present one to three weeks following initiation of therapy with the offending drug; occurs more rapidly with re-challenge (N Engl J Med 1994;331:1272)
- Fever, malaise, cutaneous and mucosal eruption
- Cutaneous and mucosal lesions are tender
- Nikolsky sign positive for epidermal detachment with application of tangential mechanical pressure (Orphanet J Rare Dis 2010;5:39)
- Eruption consists of either "flat atypical target" lesions or erythematous to purpuric macules, many with central epidermal necrosis or blister formation
- Epidermal detachment < 10% body surface area
- Variable GI and respiratory tract involvement (Orphanet J Rare Dis 2010;5:39)
- Potentially fatal, a medical emergency
Diagnosis
- Based on clinical picture plus confirmatory skin biopsy showing vacuolar interface alteration, often with epidermal necrolysis (Orphanet J Rare Dis 2010;5:39)
Prognostic factors
- Mortality rate 1 - 5%; rises with increasing surface area of epidermal detachment; higher in elderly (Orphanet J Rare Dis 2010;5:39)
- SCORTEN scoring system is used to rapidly evaluate risk and prognosis (J Invest Dermatol 2000;115:149)
- One study of 27 patients suggested Mycoplasma related disease has a less severe course than drug related cases (Mayo Clin Proc 2010;85:131)
Case reports
- 3.5 year old girl with severe gynecologic sequelae of Stevens-Johnson syndrome and toxic epidermal necrolysis (J Reprod Med 2013;58:354)
- 12 year old boy with Mycoplasma pneumoniae induced recurrent Stevens-Johnson syndrome (Pediatr Dermatol 2013;30:624)
- 19 year old woman with photo induced Stevens-Johnson syndrome (J Am Acad Dermatol 2014;71:e82)
- 19 and 36 year old women with Stevens-Johnson syndrome associated with sulfasalazine (J Crohns Colitis 2011;5:457)
- 28 year old man with Stevens-Johnson syndrome associated with furosemide (J Pharm Pract 2010;23:367)
- 49 year old man with doxycycline-induced Stevens-Johnson syndrome (Cornea 2011;30:595)
- 53 year old woman with Stevens-Johnson syndrome associated with adalimumab (Rheumatol Int 2013;33:1351)
- Associated with sorafenib for metastatic renal cell carcinoma (Urol Int 2013;91:482)
- Colonic involvement in Stevens-Johnson syndrome (Dig Endosc 2012;24:382)
- 14 adult cases (Ann Allergy Asthma Immunol 2013;110:207)
Treatment
- Withdrawal of all potential medication triggers, especially medications which have been initiated within the past four weeks (Semin Cutan Med Surg 2014;33:10)
- Primarily supportive and symptom targeted (Semin Cutan Med Surg 2014;33:10)
Clinical images
Images hosted on other servers:


Cutaneous and mucosal lesions

Widespread macules
Gross description
- Cutaneous and mucosal lesions
- Eruption consists of either "flat atypical target" lesions or erythematous to purpuric macules, many with central epidermal necrosis or blister formation
Frozen section description
- Helpful to confirm diagnosis of Stevens-Johnson syndrome
- Patient below had toxic epidermal necrolysis with extensive body surface and mucosal involvement
Frozen section images
Contributed by Hillary Rose Elwood, M.D.
Detached and necrotic epidermis
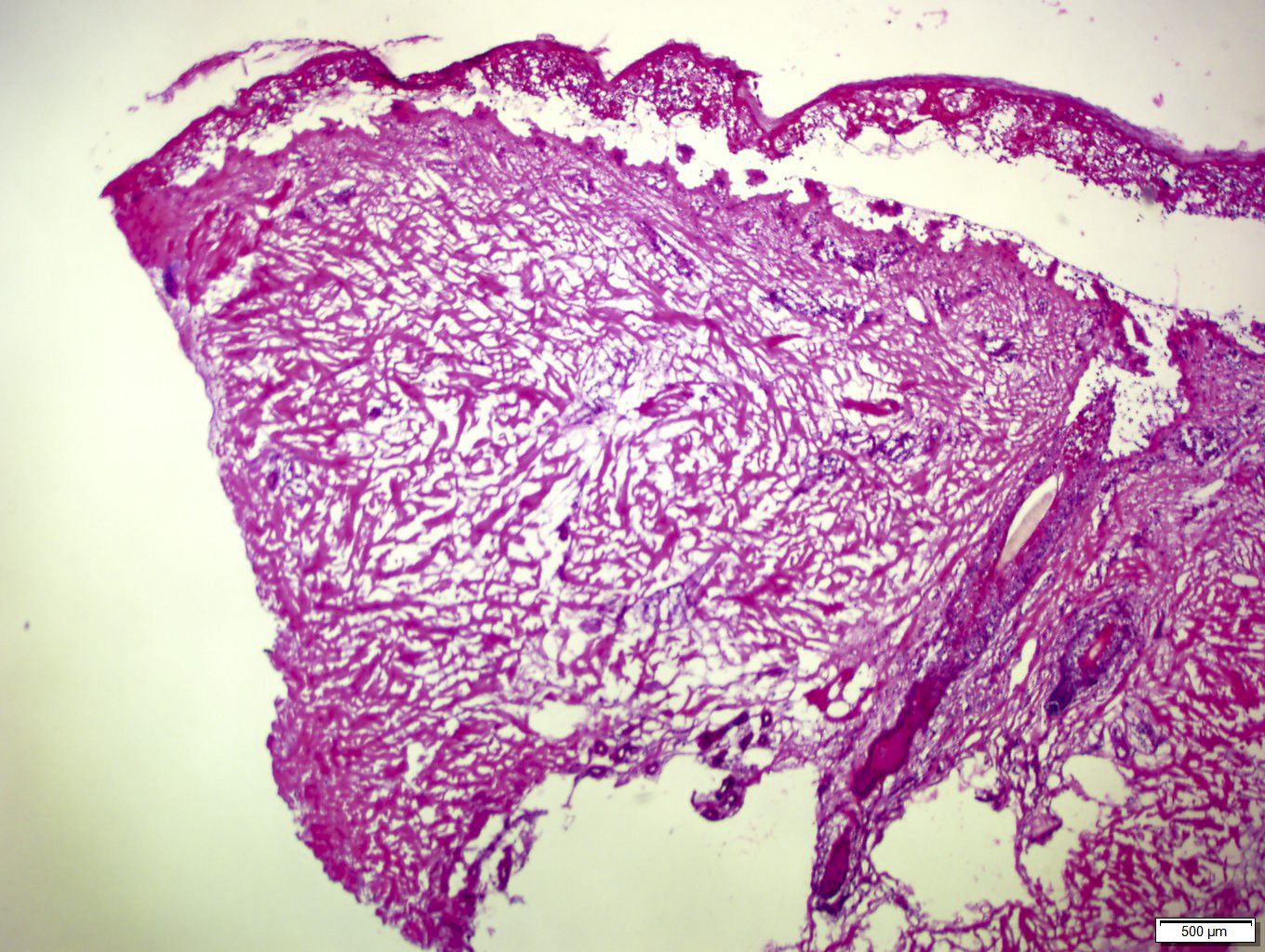
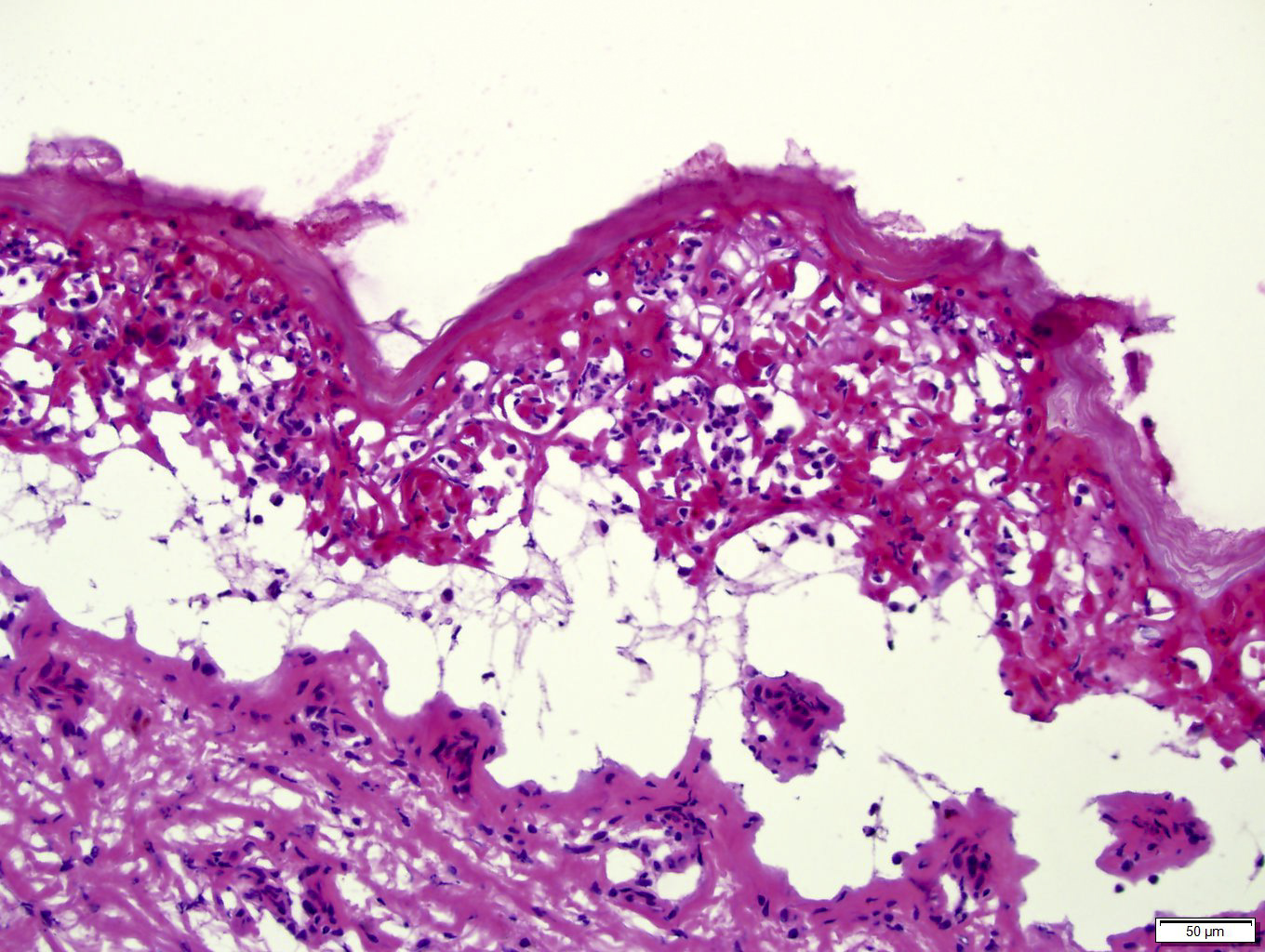
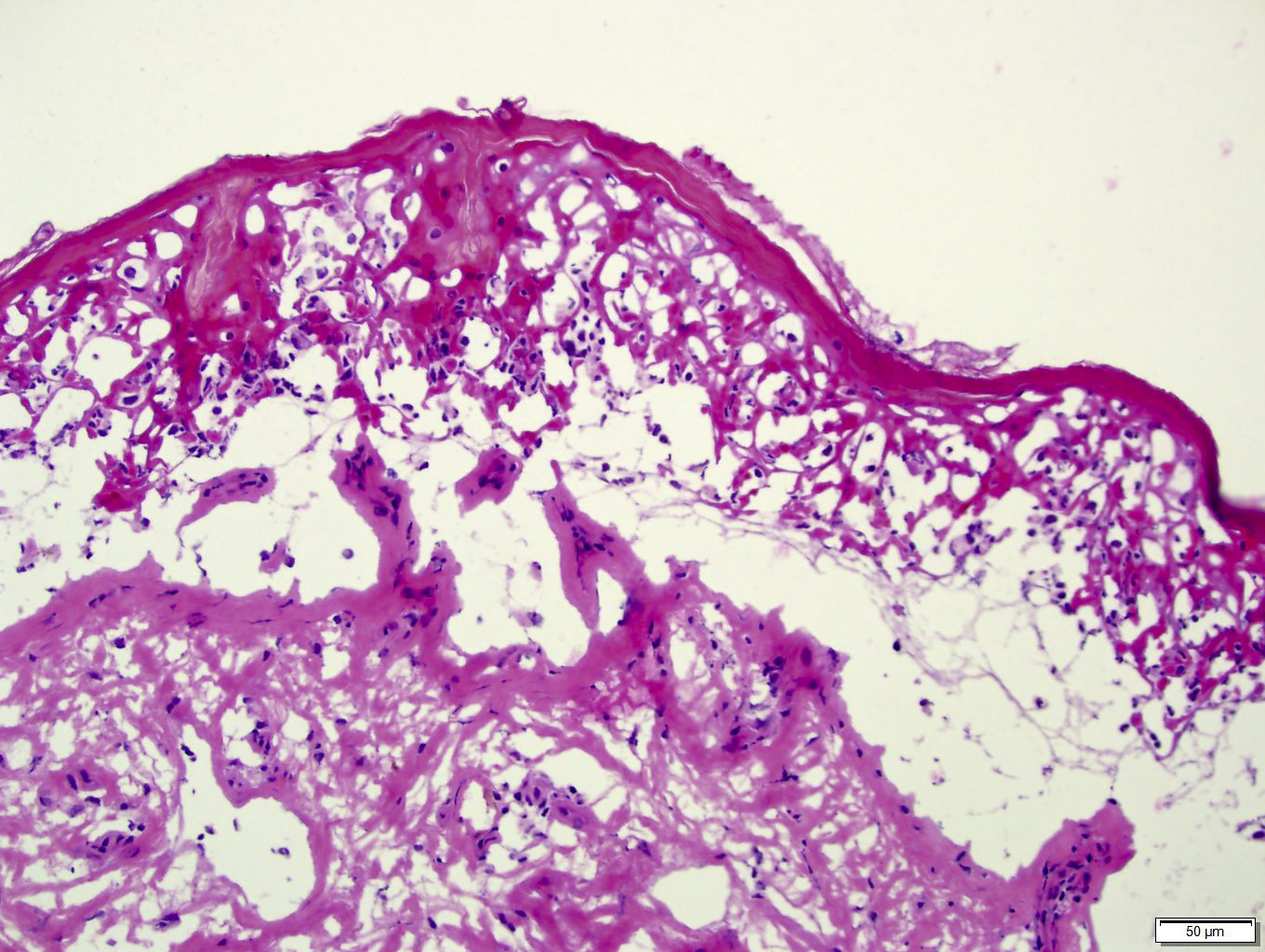
Microscopic (histologic) description
- Early lesions: apoptotic keratinocytes scattered in basal epidermis
- Later lesions: numerous necrotic keratinocytes, full thickness epidermal necrosis and subepidermal bullae
- Epidermal changes are often accompanied by a moderate or dense lymphocyte predominant dermal infiltrate
- Less commonly, neutrophils and eosinophils are present (Mayo Clin Proc 2010;85:131)
- Less common findings are red blood cell extravasation, pigment incontinence, regenerating epidermis, parakeratosis and necrosis of hair follicle (Mayo Clin Proc 2010;85:131)
- Clinical correlation is essential to distinguish erythema multiforme, SJS and TEN, as they may look nearly identical histologically
- Cannot reliably distinguish based on full thickness epidermal necrosis / necrolysis, because EM may have it and SJS / TEN may not, depending on the site of the biopsy
Microscopic (histologic) images
Contributed by Hillary Rose Elwood, M.D.


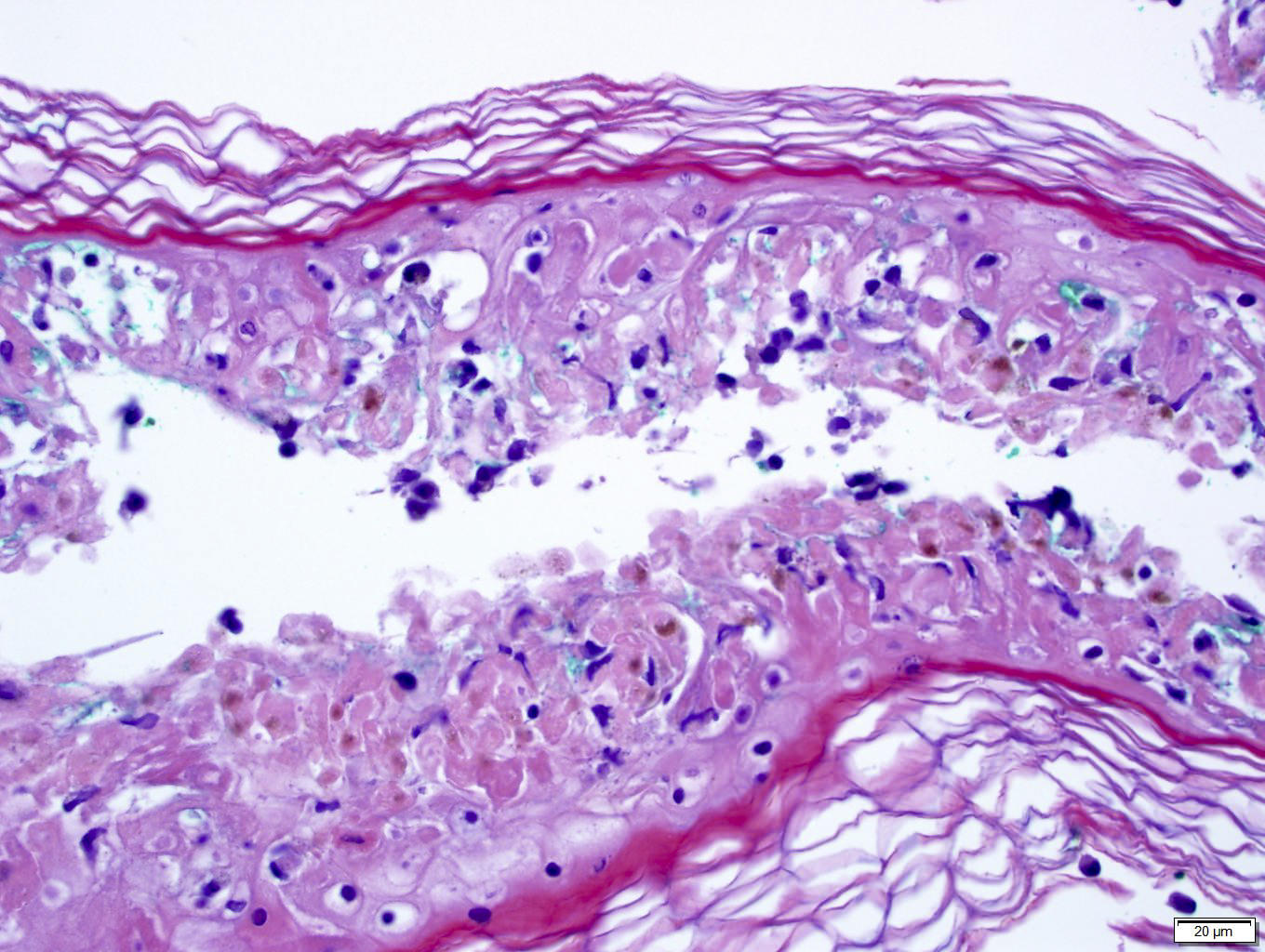
Detached epidermis with full thickness necrosis and dyskeratotic cells
Images hosted on other servers:

Basal cell vacuolar change

Full thickness necrosis of epidermis
Differential diagnosis
- Other entities with vacuolar interface dermatitis (with individual keratinocyte necrosis):
- Acute graft-versus-host disease (GVHD)
- Connective tissue disease (including lupus and dermatomyositis)
- Fixed drug eruption
- Pityriasis lichenoides (PLEVA or PLC)
- Subacute radiation dermatitis
- Viral exanthems
- Other entities with desquamation and epidermal detachment:
- Bullous pemphigoid
- Congenital bullous diseases, such as epidermolysis bullosa
- Other autoimmune blistering diseases
- Pemphigus
- Staphylococcal scalded skin syndrome
- TEN
Additional references
