
Skin nontumor
Vesiculobullous and acantholytic reaction patterns
Linear IgA bullous dermatosis
Last author update: 1 July 2011
Last staff update: 28 February 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Linear IgA disease


Table of Contents
Definition / general | Sites | Etiology | Clinical features | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Differential diagnosisCite this page: Hamodat M. Linear IgA bullous dermatosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorlineariga.html. Accessed April 2nd, 2025.
Definition / general
- Children or adults with acquired (drug induced or idiopathic) autoimmune disorder of pruritic subepidermal bullae or vesicles with linear deposits of IgA along the basement membrane
Sites
- Thighs, buttocks, lower trunk, genital area, scalp, perioral face
- Mucous membrane involvement is importance because of associated scarring
Etiology
- Unclear, appears to be immune mediated
- Target antigen of IgA autoantibodies is 120 kd secretory portion of BP180 antigen, but other antigens have also been reported
- Often occurs after administration of antibiotics, predominantly vancomycin or penicillin, rarely after amoxicillin-clavulanic acid (Pediatr Dermatol 2007;24:E40)
- Also after administration of nonsteroidal anti-inflammatory agents, diuretics, rarely interferon alpha-2A
- Not associated with HLA DR3, B8 (Clin Exp Dermatol 2009;34:e123)
Clinical features
- Small tense blisters or annular bullous plaques ("cluster of jewels" or "string of beads") with erosions and crusting
- Vancomycin associated cases may present with morbilliform (resembling measles) eruption without blistering (Arch Dermatol 2008;144:774)
- In Tunisia, is most frequent childhood bullous dermatosis; usually spares mucosa; responds rapidly to dapsone with long stabilization; erythromycin and oxacillin may be alternative therapy (Pediatr Dermatol 2009;26:28)
- Healing may be associated with hyper or hypopigmentation
- Childhood cases are usually self healing; symptoms may last over 5 years, and occasionally extend into adult life
- Adult cases follow a more prolonged course and rarely are refractory
- Associated with internal malignancy, including lymphoma and bladder carcinoma
Case reports
- 5 year old girl with lesions developing after an insect bite (Minerva Pediatr 2008;60:351)
- 16 year old girl with IgA nephropathy 6 years after skin disease (Pediatr Dermatol 2008;25:339)
- 73 year old man with vesicles after vancomycin therapy (Dermatol Online J 2006;12:12)
Treatment
- Withdrawal of offending drug, if applicable
- Dapsone or dapsone plus corticosteroids (eMedicine: Linear IgA Dermatosis [Accessed 28 August 2018])
- Dexamethasone, 2 mg/day, in one report (J Dermatol 2008;35:737)
- Possibly enteric coated mycophenolate sodium for refractory cases (J Dermatolog Treat 2008;19:364)
Clinical images
Images hosted on other servers:


Annular bullous plaques ("cluster of jewels") with erosions and crusting, pre and posttherapy
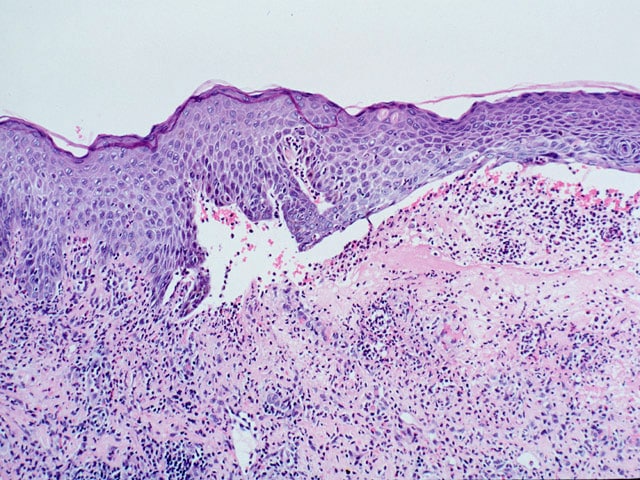
Microscopic (histologic) description
- Subepidermal blisters with neutrophilic infiltration
- Identical to dermatitis herpetiformis
Microscopic (histologic) images
Images hosted on other servers:

Subepidermal blisters with neutrophils
Neutrophilic microabscess


(B) and (C), respectively: vancomycin associated cases

Linear IgA basement membrane staining
Positive stains
- Linear deposition of IgA along the basement membrane zone of epidermis
- IgA band is linear, at basement membrane, compared to dermatitis herpetiformis, which has granular band at dermal papillae
- IgG in 25% of cases (Br J Dermatol 1997;116:293)
- IgM and C3 are occasionally present (Int J Dermatol 1985;24:569)
Differential diagnosis
- Dermatitis herpetiformis: similar morphology but IgA band is usually granular; band is at dermal papillae; serum has anti-endomysial or anti-tissue transglutaminase IgA antibodies, symptoms improve on gluten-free diet (Dermatol Online J 2008;14:21)
- Bullous lupus erythematosus: systemic symptoms; papillary dermal microabscesses, mucin in reticular dermis
