
Skin nontumor
Infectious disorders
Dermatophytes / tinea
Editorial Board Member: Bethany R. Rohr, M.D.

Last author update: 2 January 2025
Last staff update: 2 January 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Dermatophytes / tinea

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gustafson DM, Chung CG. Dermatophytes / tinea. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorfungisuperficialinfections.html. Accessed April 2nd, 2025.
Definition / general
- Superficial cutaneous mycoses classified by location of infection
- Common genera involved (Trichophyton, Epidermophyton, Microsporum and others) (J Fungi (Basel) 2023;9:669)
- Dermatophytes typically reside in keratinized tissue (i.e., the stratum corneum, nails and hair shaft) and rarely show invasion (Mycoses 2021;64:340)
Essential features
- Tinea is diagnosed by identification of fungal organisms consistent with dermatophytes by microscopic examination of skin scrapings with KOH or by skin biopsy; periodic acid-Schiff (PAS) or Grocott-Gomori silver (GMS) special stains may be used on skin biopsies to help identify organisms
- Diagnosis classified by body site of infection
Terminology
- Classified by primary site of infection (Am Fam Physician 2014;90:702, JAAD Int 2023;13:104, Mycopathologia 2010;170:143)
- Majocchi granuloma: dermatophytosis of hair follicles outside of the scalp and beard area
- Tinea barbae: dermatophytosis of the beard area, characteristically involving hair follicles
- Tinea capitis: dermatophytosis of the scalp, characteristically involving hair follicles
- Tinea corporis: dermatophytosis involving the trunk, neck, arms and legs
- Tinea cruris: dermatophytosis of the groin
- Tinea faciei: dermatophytosis of the face
- Tinea favosa: variant of tinea capitis; due to T. schoenleinii
- Tinea incognito: variant of tinea exacerbated by administration of topical / systemic corticosteroids
- Tinea manuum: dermatophytosis of the hands
- Tinea pedis: dermatophytosis of the feet
- Tinea unguium (onychomycosis): dermatophytosis of the nails
- Kerion: profound scalp inflammatory reaction associated with tinea capitis, especially by Microsporum canis infection
ICD coding
- ICD-10
- ICD-11
Epidemiology
- Affects 20 - 25% of the population worldwide (J Fungi (Basel) 2023;9:669)
- More common in subtropical regions (J Fungi (Basel) 2021;8:39)
- Most common organisms found in humans are Trichophyton, Microsporum, Epidermophyton and Nannizzia (J Fungi (Basel) 2023;9:669)
- Tinea capitis is more common in children
- Afro-Caribbean and Afro-American children in the United States have higher rates of infection; however, a host of epidemiologic factors can affect transmission (Am J Clin Dermatol 2005;6:203)
- Immunocompromised patients may have extensive / recurrent disease (J Fungi (Basel) 2021;8:39)
- Tinea favosa is endemic in Nigeria, Ethiopia, Western China, Iran and some regions in India (StatPearls: Favus [Accessed 26 September 2024)
- Trichophyton indotineae is an emerging dermatophyte that is sexually transmitted and extremely recalcitrant to therapy (J Am Acad Dermatol 2024;91:315, J Clin Med 2024;13:3558)
Sites
- See Terminology
Pathophysiology
- Fungal cell wall adhesins aid in inoculation and proteases digest host keratin (J Fungi (Basel) 2021;8:39)
- Host immune responses include innate, humoral and cell mediated (J Fungi (Basel) 2021;8:39)
Etiology
- Involves a group of closely related fungi that infect keratinized tissues such as the skin, hair and nails
- Spreads via direct contact with infected individuals, animals or contaminated surfaces
Clinical features
- Scaly, erythematous patches / plaques, often with an annular morphology (J Fungi (Basel) 2023;9:669)
- May present with pustules / vesicles (J Fungi (Basel) 2023;9:669)
- Onychomycosis may affect 1 or more nails and is characterized by onycholysis, hyperkeratosis, accumulation of subungual debris and nail discoloration (J Fungi (Basel) 2023;9:669)
Diagnosis
- Common methodologies
- Wood lamp fluorescence (Pathogens 2022;11:957)
- Potassium hydroxide (KOH) preparation
- Skin biopsy
- Other methodologies
- Culture on dermatophyte test medium and Sabouraud dextrose agar (SDA)
- Various other media can be used to differentiate Trichophyton species (Pathogens 2022;11:957)
- Polymerase chain reaction may be used for diagnosis (Pathogens 2022;11:957)
Prognostic factors
- Most localized infections are treated effectively with topical or oral antifungal medications (J Am Acad Dermatol 2000;43:S104)
- Half of patients with invasive dermatophytosis are immunosuppressed (Mycoses 2021;64:340)
- Overall mortality rate is ~8% in invasive dermatophytosis and is higher in disseminated infection (Mycoses 2021;64:340)
Case reports
- 8 year old boy with tinea capitis and alopecia (CMAJ 2024;196:E526)
- 18 year old man with tattoo associated tinea corporis (Cureus 2022;14:e21210)
- 23 year old woman with ulcerative tinea manuum caused by N. gypsea (Cureus 2024;16:e55576)
- 27 year old man with T. indotineae (Med Mycol Case Rep 2022;36:37)
- 28 and 47 year old woman with T. indotineae, first reported U.S. cases (MMWR Morb Mortal Wkly Rep 2023;72:536)
- 57 year old man with tinea incognito (J Fungi (Basel) 2022;8:312)
- 78 year old woman with tinea capitis due to T. rubrum (Actas Dermosifiliogr (Engl Ed) 2021 Apr 24 [Epub ahead of print])
Treatment
- Topical antifungal therapy for most localized infections (J Fungi (Basel) 2021;8:39)
- Oral antifungal medications may be required for more extensive infections, including (J Fungi (Basel) 2021;8:39, Indian Dermatol Online J 2016;7:77)
- Large body surface area of involvement or overlapping body regions (e.g., tinea cruris, tinea corporis and tinea pedis)
- Infection failing to respond to repeated and different topical agents
- Tinea capitis
- Tinea affecting the nails
- Tinea pedis with extensive sole, heel or dorsal involvement or blistering
Clinical images
Contributed by David M. Gustafson, M.D. and Catherine G. Chung, M.D.

Tinea capitis

Tinea corporis
Images hosted on other servers:


Kerion celsi, Majocchi granuloma and tinea capitis

Tinea corporis: well demarcated margins and diffuse erythema
Microscopic (histologic) description
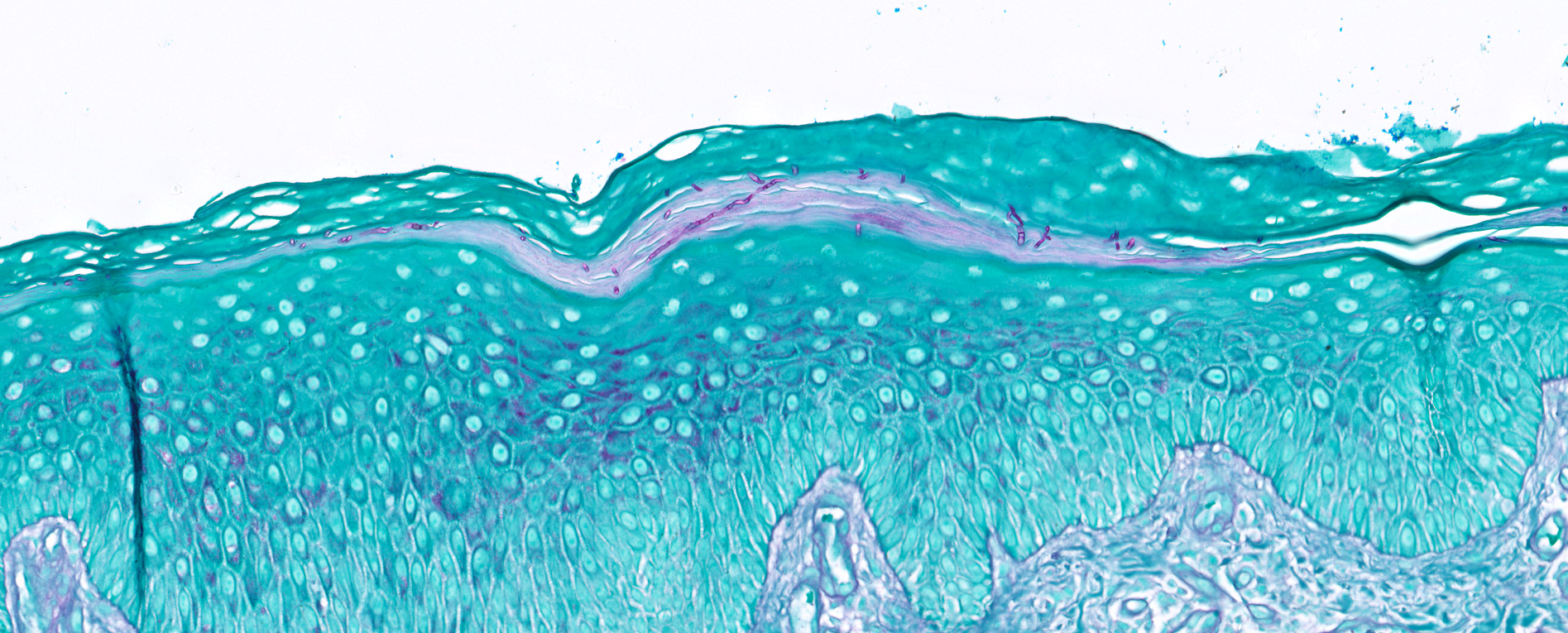
- Fungal hyphae and spores (1 - 2 microns in size) within the stratum corneum or within follicles
- In tinea capitis
- Endothrix: fungi invade the hair shaft and grow within it
- Ectothrix: hyphae do not invade the hair shaft but degrade the cuticle and grow on the surface of the hair
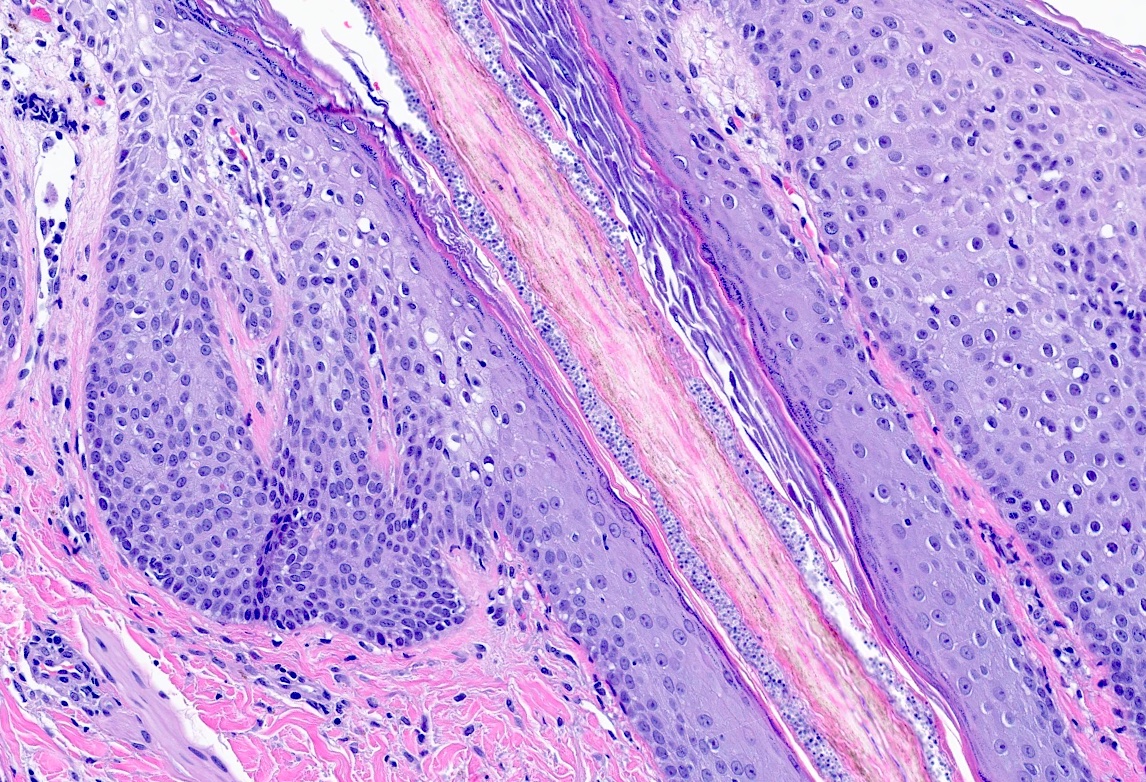
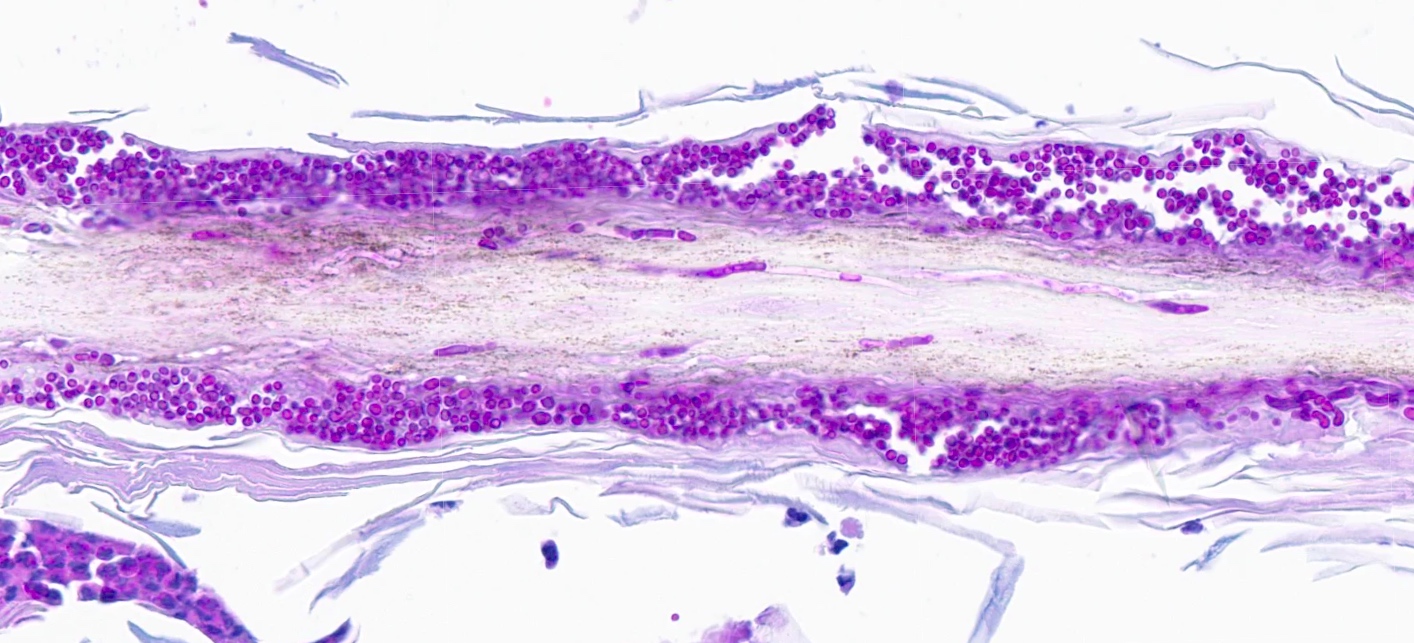
- Soft clues (Ann Dermatol 2014;26:286)
- Neutrophils within the stratum corneum and epidermis with parakeratosis
- Compact orthokeratosis
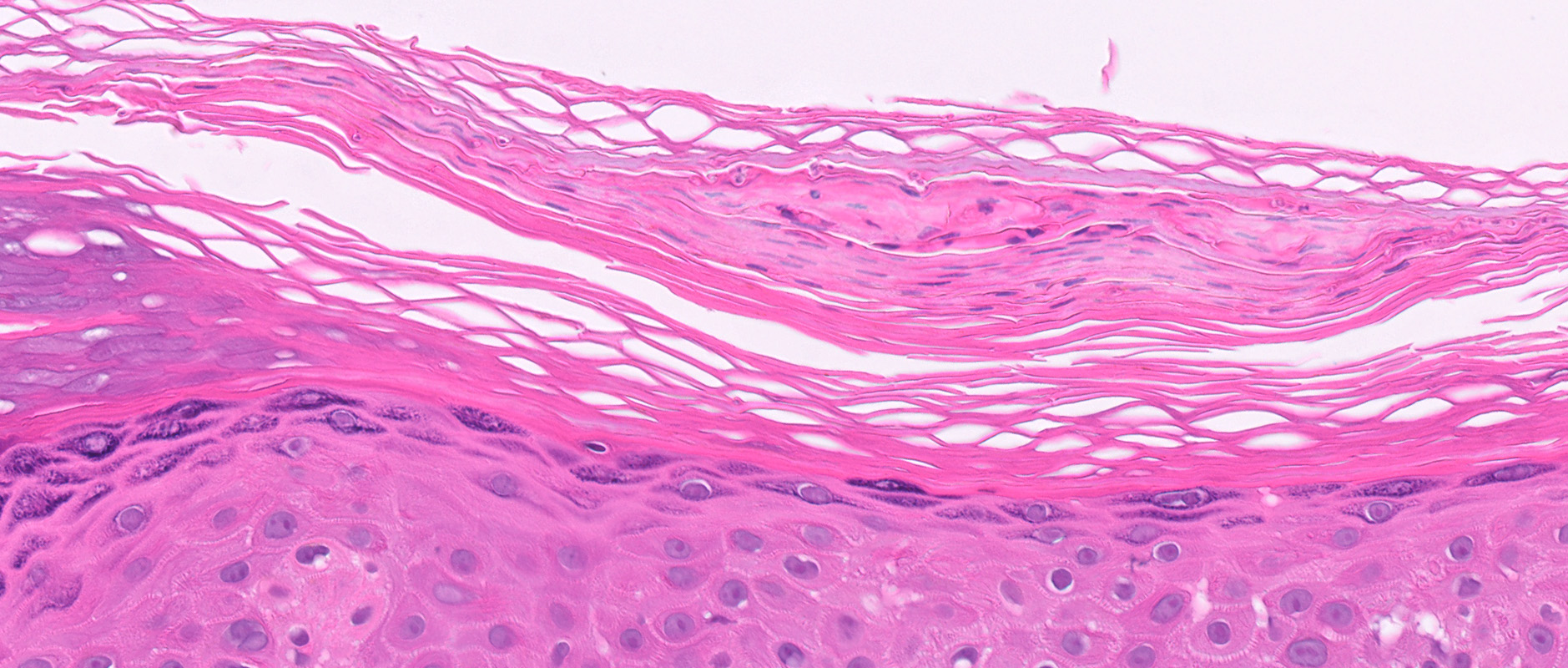
- Sandwich sign: orthokeratosis or parakeratosis alternating in layers with basketweave stratum corneum
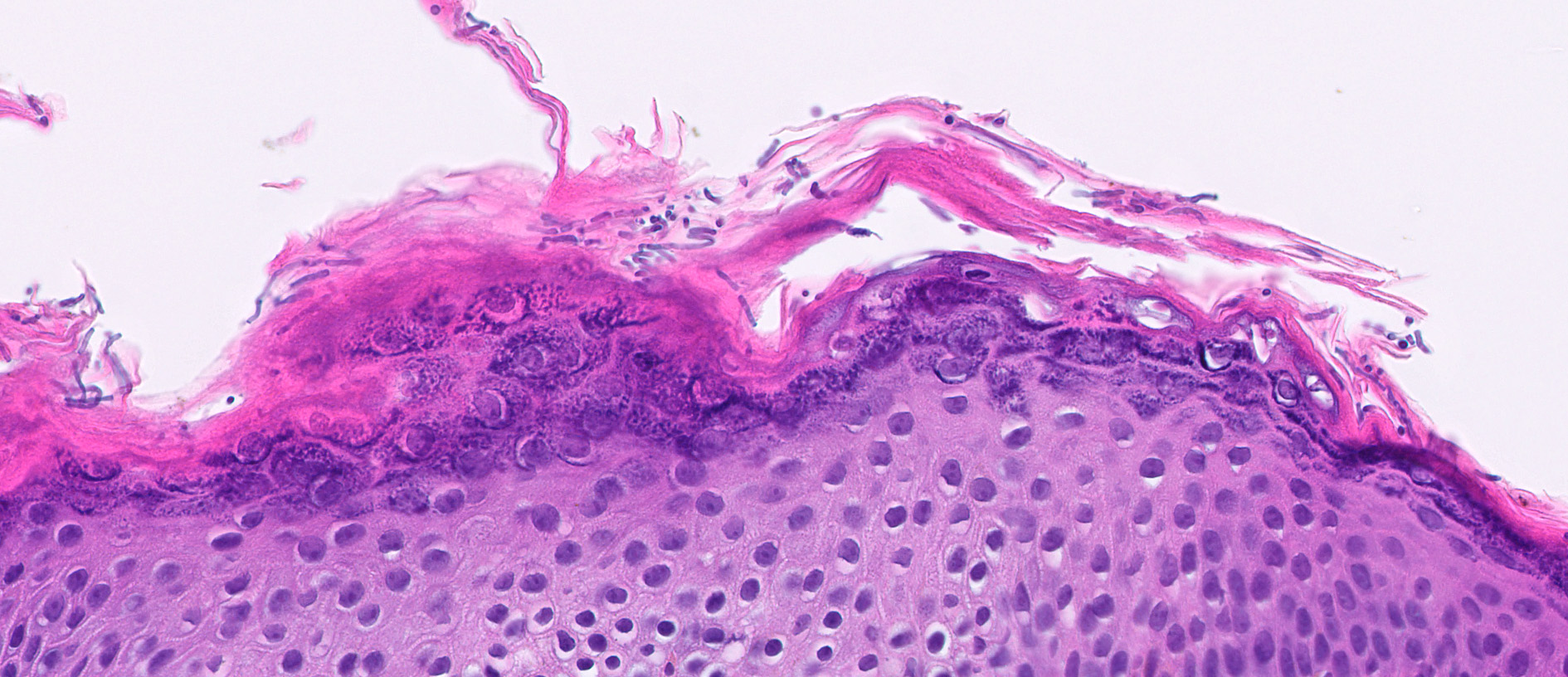
- Epidermal spongiosis
- Variable inflammatory response (lymphocytic, neutrophilic, histiocytic)
Microscopic (histologic) images
Contributed by David M. Gustafson, M.D., Catherine G. Chung, M.D. and Mona Deerwester, M.D., M.Sc.
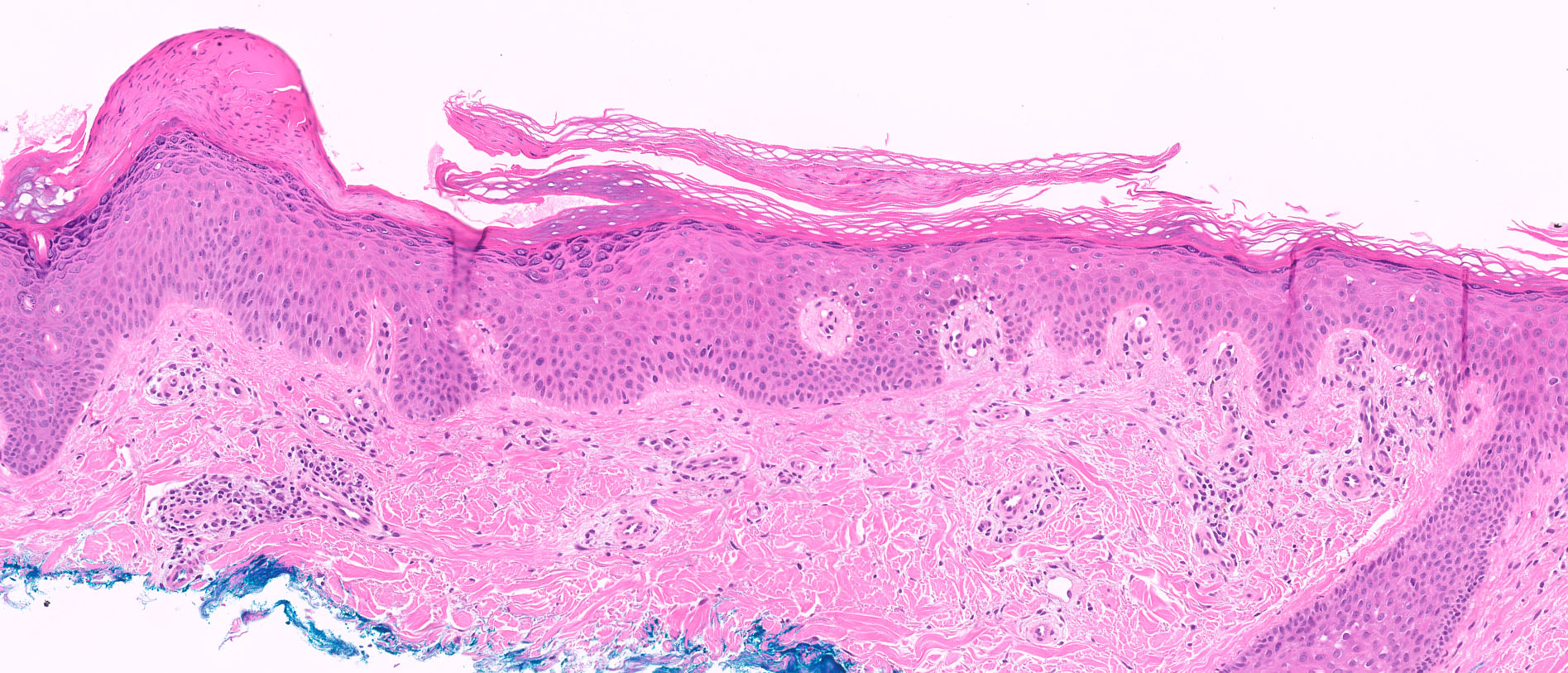
Sandwich sign
Spongiosis and refractile figures
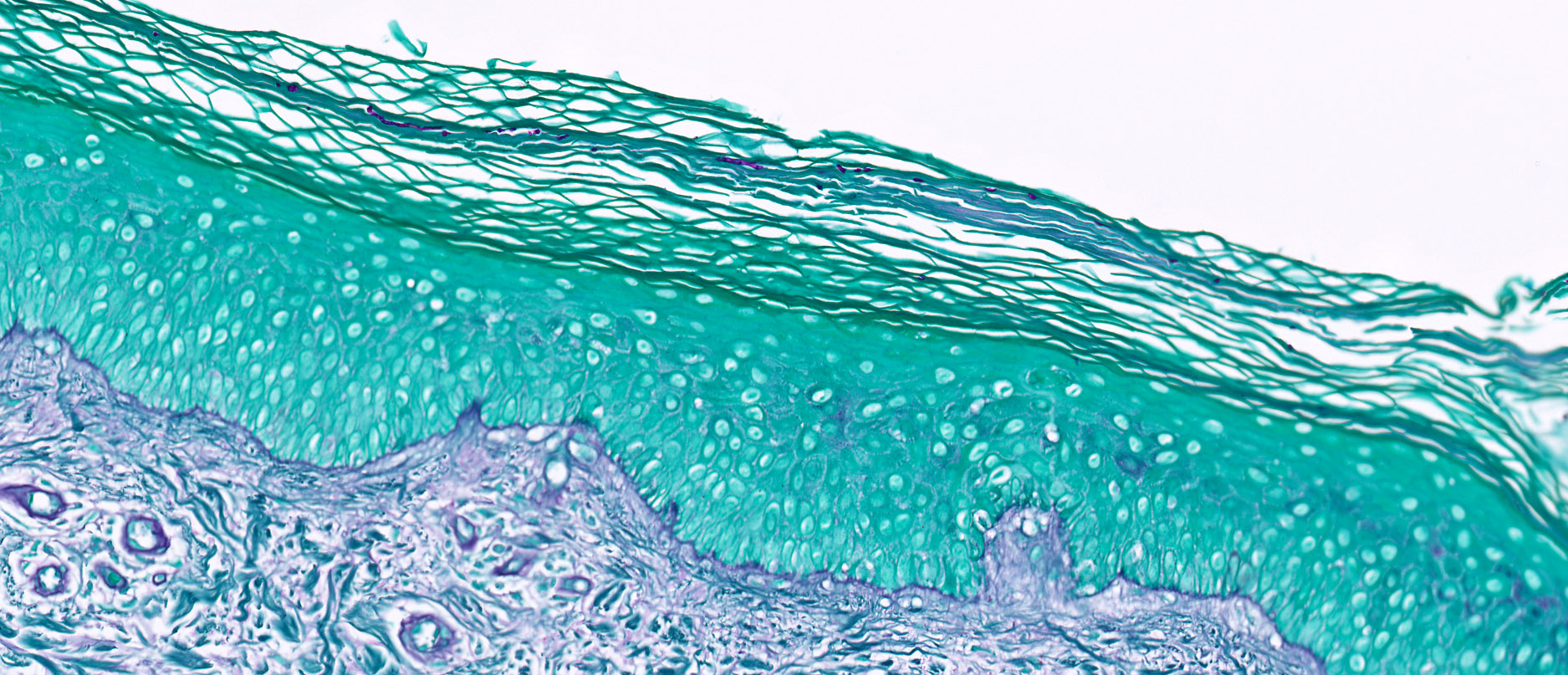
PAS positive organisms
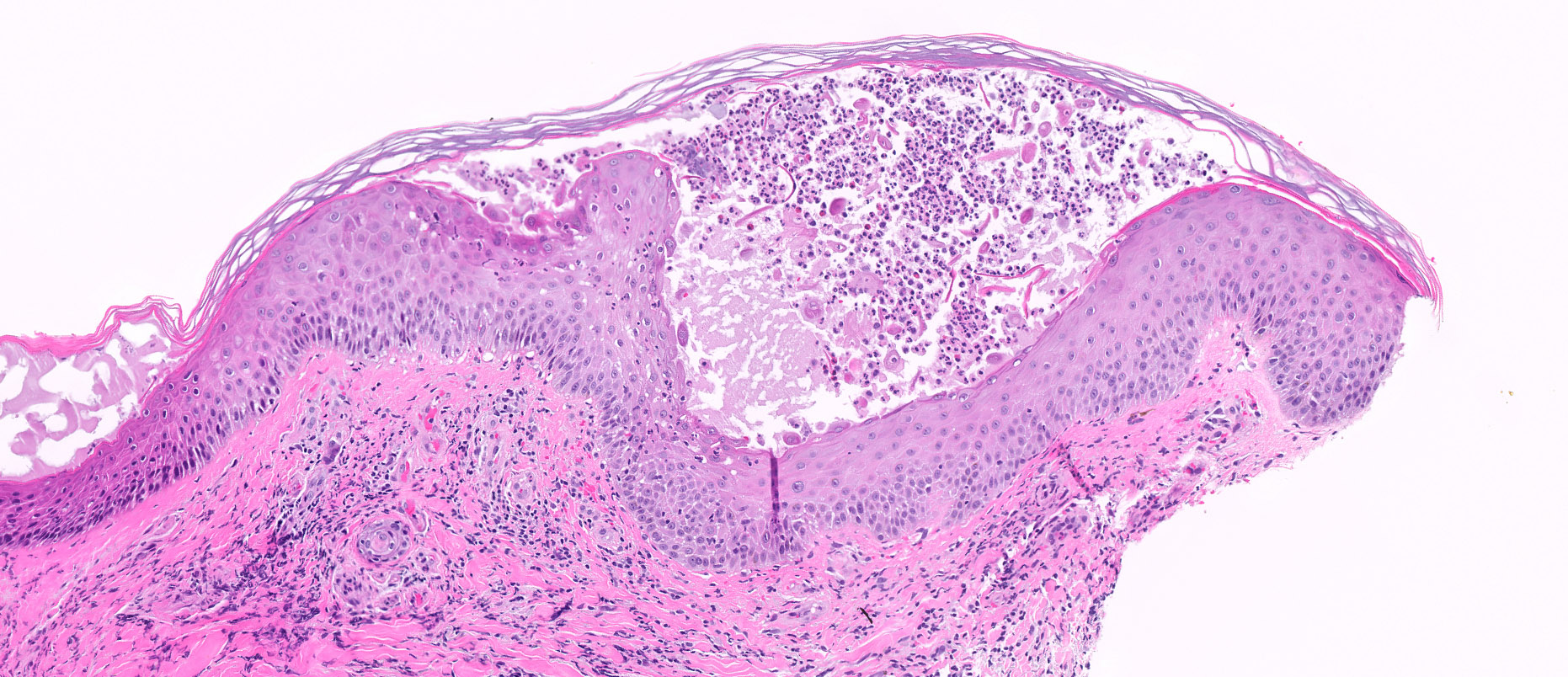
Pustular dermatophytosis
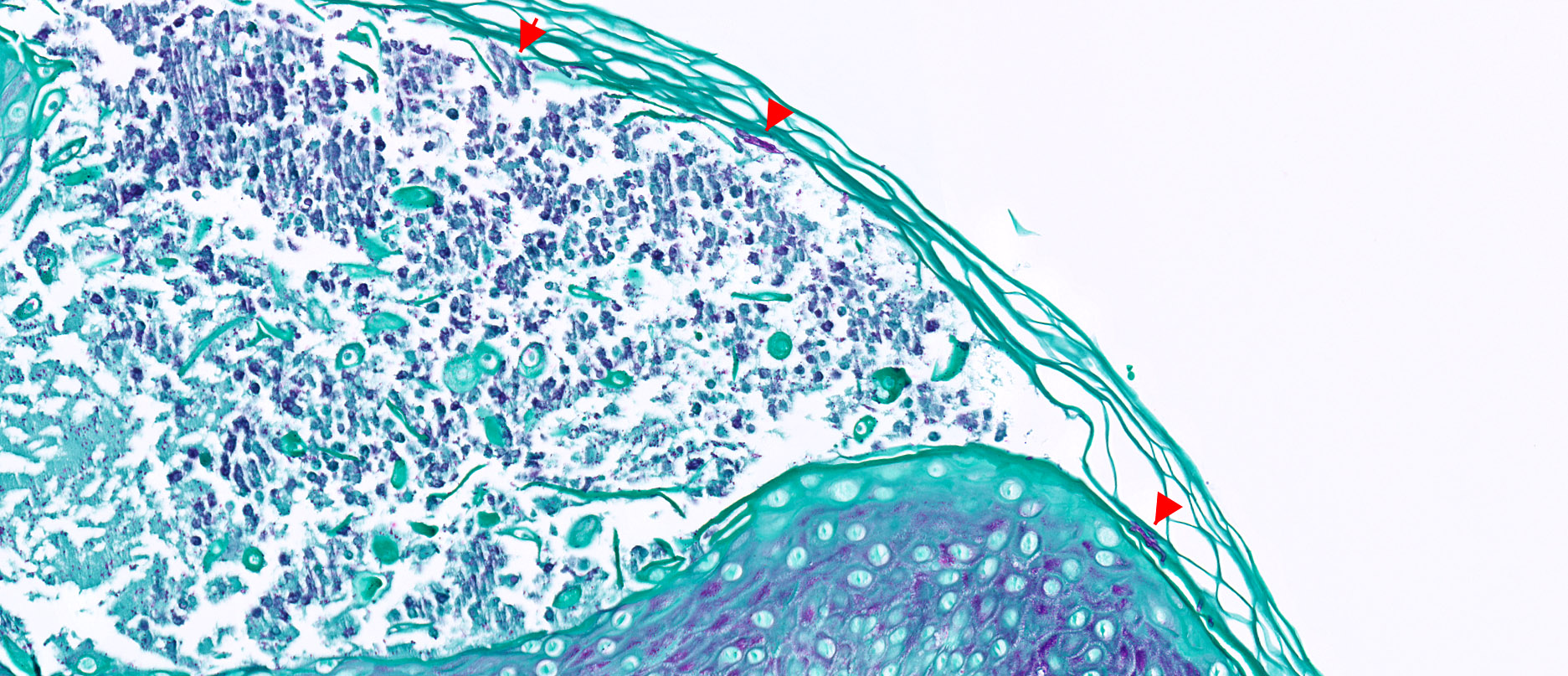
PAS of pustular dermatophytosis
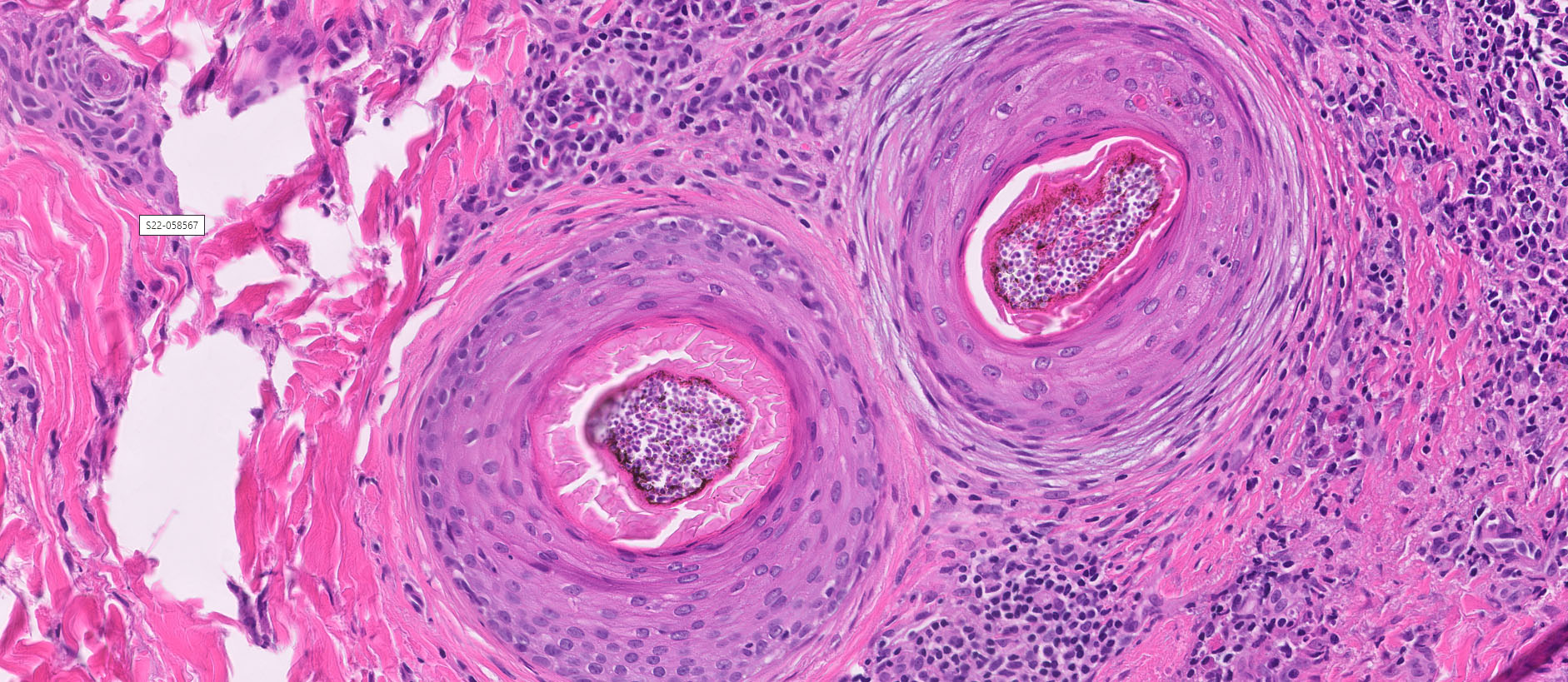
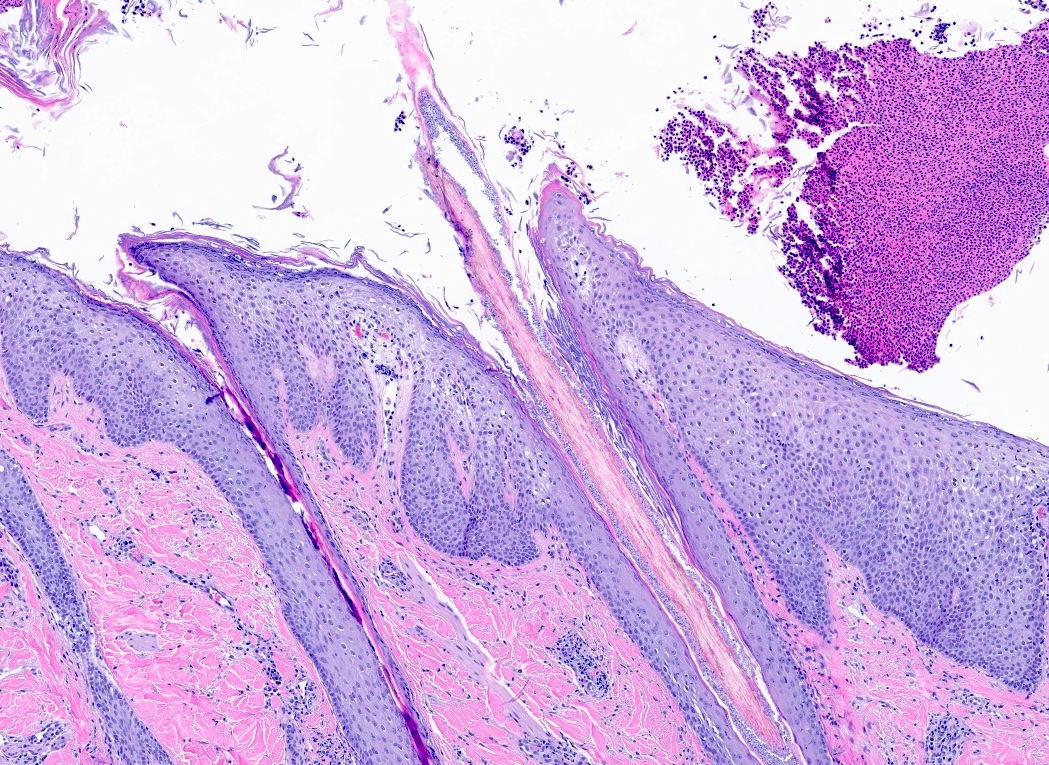
Tinea capitis
Endothrix dermatophytosis
Endothrix (PAS)
Cytology description
- Potassium hydroxide preparation of skin scrapings may show hyphae and spores (Am Fam Physician 2014;90:702)
Cytology images
Images hosted on other servers:

KOH preparation
Positive stains
- Special stains: period acid-Schiff (PAS), Grocott-Gomori methenamine silver (GMS)
Sample pathology report
- Skin, biopsy:
- Dermatophytosis (tinea) (see comment)
- Comment: The sections show a biopsy of skin with spongiosis and a superficial perivascular lymphocytic infiltrate. Special stains (PAS) highlight fungal organisms in the stratum corneum.
Differential diagnosis
- Clinical differential will vary widely depending on location and will include other annular and scaly eruptions (Am Fam Physician 2014;90:702)
- Atopic dermatitis, nummular dermatitis, allergic contact dermatitis:
- Spongiosis, superficial perivascular lymphocytic infiltrate; may have eosinophils
- Negative fungal special stains
- Psoriasis:
- Psoriasiform hyperplasia, confluent parakeratosis, diminished granular layer and collections of neutrophils in the stratum corneum
- Negative fungal special stains
- Pityriasis rosea:
- Spongiotic dermatitis with superficial perivascular lymphocytic infiltrate
- Few extravasated red blood cells
- Negative fungal special stains
- Granuloma annulare:
- Palisading granulomas in the dermis surrounding degenerated collagen and central mucin deposition
- Mild perivascular lymphocytic infiltrate
- Annular / gyrate erythemas:
- Superficial and deep perivascular dermatitis with a coat sleeve appearance of lymphocytes hugging vessels
- Negative fungal special stains
- Syphilis:
- Psoriasiform and lichenoid dermatitis with increased collections of plasma cells
- Positive treponema immunohistochemical stain or Warthin-Starry silver stain
- If pustular, one may consider the following
- Impetigo:
- Subcorneal neutrophils
- May have acantholysis
- Gram stain may show bacterial organisms
- Pustular psoriasis:
- Subcorneal neutrophils, in addition to the features of psoriasis
- Arthropod bites:
- Superficial and deep, wedge shaped mixed inflammatory infiltrate (lymphocytes, histiocytes, and eosinophils)
- Candidiasis:
- See below
- Impetigo:
- Atopic dermatitis, nummular dermatitis, allergic contact dermatitis:
- In cases where fungal organisms are identified, the differential diagnosis includes
- Pityrosporum (tinea) versicolor:
- Organisms present in basketweave stratum corneum usually without inflammatory reaction and will have shorter hyphae with numerous yeast forms that are readily identifiable on routine H&E slides
- Candidiasis:
- Nonseptate pseudohyphae
- Infection often in intertriginous areas or mucous membranes
- Pityrosporum (tinea) versicolor:
Board review style question #1
A patient presents with multiple pruritic, scaly patches on the back. A skin biopsy was performed and a PAS special stain is shown above. What is the best diagnosis?
- Candidiasis
- Tinea corporis
- Tinea cruris
- Tinea versicolor
Board review style answer #1
B. Tinea corporis. The sections show PAS positive hyphae in the stratum corneum, without yeast. Answer A is incorrect because candidiasis will have nonseptate pseudohyphae. Answer C is incorrect because while the etiology / morphology of organisms is the same, tinea cruris is classified as a superficial infection involving the groin. Answer D is incorrect because tinea versicolor is a superficial mycosis due to Malessezia spp. and morphologically will have short hyphae and yeast organisms.
Comment Here
Reference: Dermatophytes / tinea
Comment Here
Reference: Dermatophytes / tinea
Board review style question #2
Which of the following is true regarding dermatophyte infections?
- Candida is most frequently identified in cases of tinea cruris
- Invasive spread of organisms is impossible due to the superficial nature of cutaneous dermatophyte infections
- Morphologic features include abundant budding yeast
- Most commonly due to Trichophyton, Epidermophyton, Microsporum and Nannizzia organisms
Board review style answer #2
D. Most commonly due to Trichophyton, Epidermophyton, Microsporum and Nannizzia organisms. These are the most common organisms to cause dermatophytosis. Answer A is incorrect because Candida is not a dermatophyte. Answer B is incorrect because invasive dermatophytosis has been reported in immunosuppressed patients. Answer C is incorrect because tinea is not characterized by budding yeast.
Comment Here
Reference: Dermatophytes / tinea
Comment Here
Reference: Dermatophytes / tinea
