

Table of Contents
Definition / general | Terminology | Sites | Etiology | Clinical features | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosisCite this page: Do HK. Folliculitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorfolliculitis.html. Accessed April 1st, 2025.
Definition / general
- Primary inflammation of a hair follicle, either infectious or noninfectious
Terminology
- Perifolliculitis: presence of inflammatory cells in the perifollicular tissues that may involve the adjacent reticular dermis; either primarily lymphocytic (lichen planopilaris, pityriasis rubra pilaris) or granulomatous (perioral dermatitis, rosacea)
- Pseudolymphomatous folliculitis: facial lesion with dense, polymorphic, mixed lymphocytes around hair follicles and infiltrating follicular epithelium
Sites
- Common sites are the face, scalp, thighs, axilla and inguinal area
Etiology
- Caused by infection, friction and other causes of follicular trauma, excessive perspiration and occlusion
- Infectious cases are either superficial (fungi, bacteria, syphilis, viral) or deep (usually granulomatous and due to either fungi or bacteria)
- Fungal forms may be endothrix (spores are within hair shaft) or ectothrix (spores are on outer surface of hair shaft)
- Noninfectious cases are either superficial / suppurative (acne vulgaris, rosacea, follicular mucinosis, steroid induced), deep / granulomatous (acne vulgaris-conglobate and keloidal forms or perforating) or spongiotic (Fox-Fordyce disease, atopic dermatitis, pruritic folliculitis of pregnancy)
- Epidermal growth factor receptor (EGFR) inhibitors appear to be relevant in folliculitis by causing abnormal epidermal differentiation that leads to follicular obstruction and subsequent inflammation (Br J Dermatol 2001;144:1169)
Clinical features
- Superficial folliculitis is more common but is often self-limited
- Patients with recurrent or persistent superficial folliculitis or with deep folliculitis are more likely to seek medical care
- In recalcitrant folliculitis that failed standard therapy, consider cultures for sensitivity, Gram stain, potassium chloride (KOH) preparation to rule out fungal folliculitis
- Clinical presentation of superficial folliculitis is acute onset of mildy tender papules and pustules
- Deep folliculitis is usually associated with more pain and may have suppurative drainage; may cause scarring and permanent hair loss
Treatment
- For uncomplicated superficial folliculitis, use antibacterial soaps, good handwashing
- For recurrent and deep lesions, treat empirically with topical antibiotics
- Antiobiotics should kill Staphylococcus aureus, the most common pathogen; recommended to use dicloxacillin and cephalosporins (eMedicine)
- For MRSA, use clindamycin, bactrim, minocycline or linezolid
- For Staphylococcus aureus carriers, treat patient and family with mupirocin ointment BID x 5 days or rifampin 600 mg/day x 10 days
Clinical images
Images hosted on other servers:

Folliculitis
Microscopic (histologic) description
- Superficial folliculitis has moderate inflammatory cells in the follicular ostium and upper regions of the follicle
- Infiltrate initially consists of neutrophils, later becomes more mixed with lymphocytes and macrophages
Microscopic (histologic) images
Images hosted on other servers:
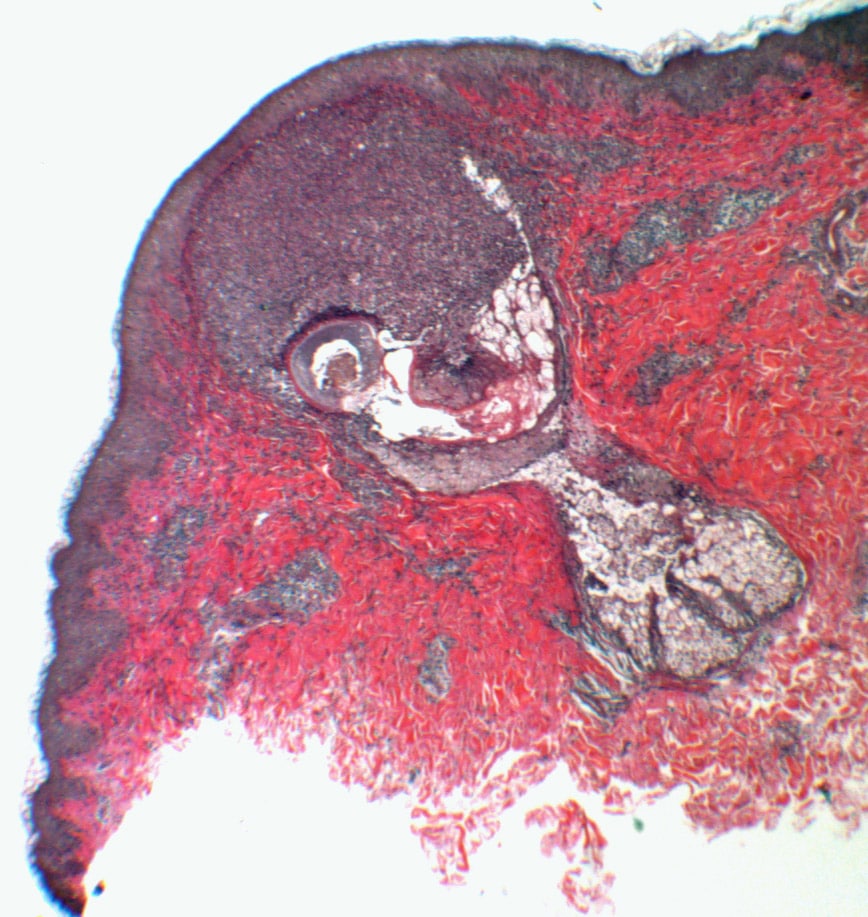
Micro image of folliculitis
Differential diagnosis
- Acne vulgaris
- Acneiform eruptions
- Arthropod bites
- Cutaneous candidacies
- Coccidiomycosis
- Ermatologic manifestations of renal disease
- Erythema toxic neonatorum
- Fox-Fordyce disease
- Graham-Little-Piccardi-Lasseur syndrome
- Id-reaction (autoeczematization)
- Impetigo
- Irritant contact dermatitis
- Milia
- Perioral dermatitis
- Papular urticaria
- Pruritic papular eruption of HIV disease (Indian J Sex Transm Dis AIDS 2018;39:44)
- Rosacea
- Seabathers eruption
- Subcorneal pustular dermatosis
