
Skin nontumor
Keratinization disorders
Epidermolytic hyperkeratosis
Last author update: 1 December 2014
Last staff update: 11 November 2020
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Epidermolytic hyperkeratosis



Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Carlquist EM, Stuart LN. Epidermolytic hyperkeratosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorepidermolytichyperkeratosis.html. Accessed April 1st, 2025.
Definition / general
- Keratinization disorder which presents at birth with generalized erythema, widespread bullae and desquamation resulting in denuded skin
- Form of ichthyosis, an abnormality of epidermal maturation resulting in skin fragility
- "Epidermolytic hyperkeratosis" is a descriptive term which refers to specific microscopic features (i.e. vacuolar degeneration of the spinous layer, keratin filament clumping and hyperkeratosis), but these findings may be seen in various entities, not just this disease (Int J Dermatol 2005;44:1):
- Generalized: bullous ichthyosis
- Systematized or linear: epidermal nevus variant
- Palmoplantar: palmoplantar keratoderma variant (Vorner type)
- Solitary: epidermolytic acanthoma
- Multiple discrete: disseminated epidermolytic acanthoma
- Incidental: focal epidermolytic hyperkeratosis
- Solar keratosis related: a rare variant of solar keratosis
- Follicular: nevoid follicular epidermolytic hyperkeratosis
- Mucosal: epidermolytic leukoplakia
Terminology
- Other names:
- Epidermolytic ichthyosis
- Bullous congenital ichthyosiform erythroderma
- Bullous ichthysosis
- Bullous erythroderma ichthyosiformis congenita of Brocq
- Disorder of cornification type 3
- Vorner's syndrome
Epidemiology
- Rare, 1 of every 100,000 - 300,000 live births (Int J Dermatol 2005;44:1)
- Inherited autosomal dominant disease but 50% are sporadic due to spontaneous mutations (Int J Dermatol 2005;44:1)
- Mosaic form can occur due to a postzygotic mutation (An Bras Dermatol 2013;88:116)
- A recessive and fatal form has been described (Dermatol Online J 2014;20:21248)
- No male or female predilection (Int J Dermatol 2005;44:1)
Sites
- Widespread hyperkeratosis is most prominent over joints (Int J Dermatol 2005;44:1) and flexural surfaces
- Hyperkeratosis is also seen on scalp, neck and infragluteal folds (Dermatol Online J 2014;20:21248)
Pathophysiology
- Defects in keratin genes (KRT1 and KRT10) cause excessive and abnormal keratinization
- Mutations occur in carboxy-terminal of rod domain of keratin 1 (K1) and in amino-terminal of rod domain of keratin 10 (K10)
Clinical features
- Presents at birth with generalized erythema, followed by development of thick verrucous scaling on flexor surfaces
- Distinct foul odor due to secondary bacterial colonization of thickened skin (Dermatol Online J 2014;20:21248)
- Complications include infection, sepsis, dehydration and electrolyte imbalances due to compromised skin barrier (Dermatol Online J 2014;20:21248)
- Palmar and plantar involvement occurs in 60% of patients, most commonly in those with K1 mutations (Dermatol Online J 2014;20:21248)
- Linear epidermolytic hyperkeratosis is associated with genetic mosaicism (Dermatol Online J 2014;20:21248)
- Linear hyperkeratosis in streaks along Blaschko lines
- Unilateral or bilateral, localized or generalized
- Absence of blistering (unlike classical epidermolytic hyperkeratosis)
Diagnosis
- Characteristic histological and ultrastructural findings (see below)
- Immunofluorescence to determine which keratin type is involved (Hum Mol Genet 2006;15:1133)
Case reports
- 5 year old boy with systematized linear epidermolytic hyperkeratosis (Dermatol Online J 2014;20:21248)
- 13 year old boy with epidermolytic hyperkeratosis (Dermatol Online J 2006;12:6)
- 37 year old woman with mosaic epidermolytic ichthyosis (An Bras Dermatol 2013;88:116)
Treatment
- Symptom management only (Int J Dermatol 2005;44:1):
- Daily bathing and moisturizing twice daily
- Alpha hydroxy acids to reduce xerosis
- Antibiotic ointment applied to fissures
- Retinoids in severe cases, but use with caution as may exacerbate blistering (An Bras Dermatol 2011;86:S72)
Clinical images
Images hosted on other servers:

Corrugated cardboard-like

Palms

Anterior ankles

Close up of ankle

Presenting as erythroderma and blistering

Hyperkeratotic papules

Papules in proximal thigh

Left palmar hyperkeratosis

Plantar hyperkeratosis

Thickened red hyperkeratotic corrugated plaques

Plaques distributed over neck, back and flexural surfaces
Gross description
- Varies based on age
- Infants have generalized erythema accompanied by erosions and bullae
- In a few years, lesions evolve into verrucous plaques and scales
Microscopic (histologic) description
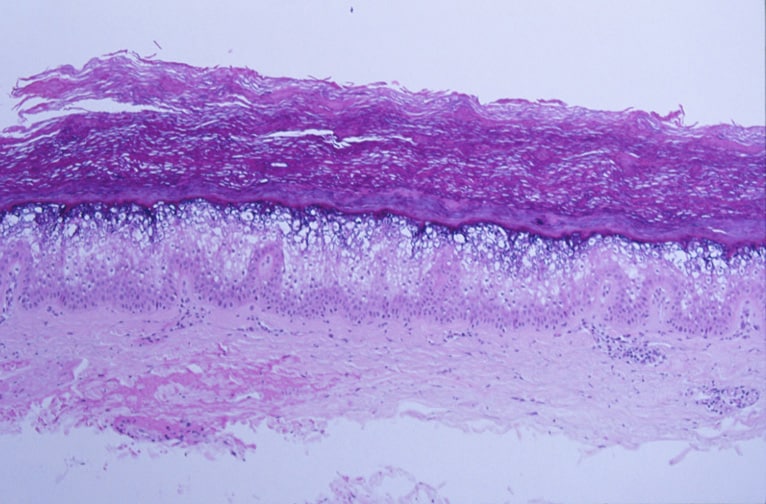
- Epidermolytic hyperkeratosis (characteristic feature disease is named for), also called granular degeneration, is seen in upper epidermis
- Granular and vacuolar degeneration of spinous and granular cell layers
- Microscopically this appears as cleared spaces of variable size around nuclei in upper layers of nucleated epidermis
- Granular layer contains an increased number of irregularly shaped keratohyaline granules
- Overlying hyperkeratosis
- Bullae form due to separation of edematous keratinocytes; keratinocytes fall apart (epidermolysis) due to lack of normal cytoplasmic keratin filament infrastructure that normally gives keratinocytes their strength
- Mild lymphocytic inflammatory infiltrate in upper epidermis
- Many more mitoses are present than in normal epidermis
Microscopic (histologic) images
Images hosted on other servers:

Focal epidermolytic hyperkeratosis

Continuous epidermolytic hyperkeratosis

Mosaic
Epidermolytic ichthyosis

Parakeratosis, hypergranulosis
and vacuolar degeneration of
granular and spinous layer
Positive stains
- Suprabasal epithelium shows increased expression of keratin 14
Electron microscopy description
- Increase and clumping of tonofilaments
- Increased and premature formation of keratohyaline granules of variable size
- At periphery of cells are numerous keratohyaline granules embedded in thick shells of irregularly-clumped tonofilaments
- Desmosome attachment to keratinocytes is abnormal due to disturbed desmosome-tonofilament associations, which leads to blister formation
Differential diagnosis
- Arsenicism: pigmented or erythematous patches primarily involving palms and soles
- Congenital ichthyosiform erythroderma: autosomal recessive; collodion baby with fine white scales and erythroderma
- Epidermolytic palmoplantar keratoderma: defect in keratin 9; primarily involving palms and soles (histology is essentially identical to EHK)
- Ichthyosis bullosa of Siemens: defect of keratin 2e; mild hyperkeratosis of extremities and easily sloughed skin
- Ichthyosis hystrix, Curth-Macklin type: defect in keratin 1; perinuclear tonofibrillar shells on histologic examination of biopsy specimen
- Ichthyosis vulgaris: abnormal desmosomes; fine white scales mainly affecting extensor surfaces
- Lamellar ichthyosis: defect in transglutaminase; collodion baby with rippled, thick, plate-like, dark scales
- X linked ichthyosis: steroid sulfatase defect; thick brown scales over extremities
Additional references
