

Skin nontumor
Alopecia
Androgenic alopecia
Editorial Board Member: Robert E. LeBlanc, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 6 May 2021
Last staff update: 26 April 2023
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Androgenic alopecia [title] pathology

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Saleh J, Speiser J. Androgenic alopecia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumoralopeciaandrogenic.html. Accessed December 29th, 2024.
Definition / general
- Nonscarring, patterned alopecia caused by androgen mediated follicular miniaturization (An Bras Dermatol 2015;90:529)
Essential features
- Most commonly affects Caucasians, followed by Asians, African Americans and Native Americans (StatPearls: Androgenetic Alopecia [Accessed 8 July 2020])
- Androgen sensitive hair follicles miniaturize due to accumulation of dihydrotestosterone, resulting in hair thinning and eventually hair loss (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020], Plast Reconstr Surg Glob Open 2013;1:e64)
- Polygenetic condition with varying severity, rate of progression, age of onset and affected scalp sites (BMJ 1998;317:865)
- Progressive miniaturization with varying size of hair follicles and decrease in size of dermal papilla, bulb size and hair shaft diameter (Histopathology 2010;56:24)
Terminology
- Also known as androgenetic alopecia, pattern baldness, male pattern baldness, male pattern alopecia and female pattern baldness (An Bras Dermatol 2015;90:529, Endocrine 2017;57:9)
Epidemiology
- Onset in males typically between 20 and 25 years (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
- 30% of men affected by age 30, 50% by age 50 and 80% by age 70 (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020], BMJ 1998;317:865)
- Up to 13% of premenopausal women are reported to have androgenetic alopecia (J Am Acad Dermatol 1988;18:1073)
- Incidence in women increases following menopause and affects at least 41% of women over the age of 65 (StatPearls: Androgenetic Alopecia [Accessed 8 July 2020], Int J Womens Dermatol 2018;4:203)
- Most commonly affects Caucasians, followed by Asians, African Americans and Native Americans (StatPearls: Androgenetic Alopecia [Accessed 8 July 2020])
Sites
- Scalp
Pathophysiology
- Increased androgen receptors and increased 5-alpha reductase leads to increased testosterone conversion in hair follicle to dihydrotestosterone (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020], Plast Reconstr Surg Glob Open 2013;1:e64)
- Dihydrotestosterone accumulates in the hair follicles (Plast Reconstr Surg Glob Open 2013;1:e64)
- Androgen sensitive hair follicles miniaturize, resulting in hair thinning and eventually hair loss (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020], Plast Reconstr Surg Glob Open 2013;1:e64)
- Role of androgens in female androgenetic alopecia is not fully established and is probably a multifactorial, genetically determined trait with both androgen dependent and androgen independent mechanisms contributing to the phenotype (Int J Womens Health 2013;5:541, Int J Womens Dermatol 2018;4:203)
Clinical features
- Polygenetic condition with varying severity, rate of progression, age of onset and affected scalp sites (BMJ 1998;317:865)
- Men: hair loss typically involves the temporal and vertex region while sparing the occipital region; the hairline also recedes to form a characteristic “M” shape (BMJ 1998;317:865)
- Women: diffuse thinning of the frontal / parietal scalp with retention of the frontal hairline (Int J Womens Dermatol 2018;4:203)
- Has been associated with several other medical conditions:
- Men: coronary heart disease, prostate cancer, diabetes, obesity and hypertension (StatPearls: Androgenetic Alopecia [Accessed 8 July 2020])
- Women: polycystic ovary syndrome (Int J Womens Dermatol 2018;4:203)
- Hair pull test is normal (Int J Womens Health 2013;5:541)
- Male pattern baldness (Norwood-Hamilton classification) (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
- Type I: minimal bitemporal recession of hair
- Type II: extension of type I
- Type III: hair loss in tonsure area and recession of hair from the forehead
- Type IV - VI: extension of type III
- Type VII: most severe pattern of hair loss, with a confluence of the balding areas; hair preserved only around the back and the sides of the head
- Female pattern baldness (Ludwig classification) (Int J Womens Dermatol 2018;4:203)
- Type I: mild (hair loss on the front and top of the scalp with relative preservation of the frontal hairline)
- Type II: moderate
- Type III: severe
Diagnosis
- Scalp biopsy
Case reports
- Man in the fourth decade of life with new onset androgenic alopecia following hCG diet and implantation of testosterone pellets (Int J Trichology 2018;10:284)
- 44 year old woman with female androgenic alopecia (Cutis 2012;90:73)
- 73 year old woman with androgenic alopecia and hirsutism (Gynecol Endocrinol 2009;25:324t)
Treatment
- Topical minoxidil and oral finasteride (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
- Dutasteride (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
- Oral antiandrogens (i.e. spironolactone, cyproterone acetate) (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
- Hair transplant surgery (Endotext: Male Androgenetic Alopecia [Accessed 8 July 2020])
Clinical images
Images hosted on other servers:

Hair shaft diameter variability
Microscopic (histologic) description
- Unchanged total number of hair follicles (Histopathology 2010;56:24)
- Progressive miniaturization with varying size of hair follicles and decrease in size of dermal papilla, bulb size and hair shaft diameter (Histopathology 2010;56:24)
- Increased number of vellus and telogen hairs (Histopathology 2010;56:24)
- Ratio of anagen to telogen is reduced from 12:1 to less than 5:1 (BMJ 1998;317:865)
- Reduced terminal to vellus ratio of 4:1 or less (normal scalp = 7:1) (Histopathology 2010;56:24)
- Decreased number of terminal hair follicles and increased stellae in the subcutaneous fat (Histopathology 2010;56:24)
- Increased fibrous tracts (Histopathology 2010;56:24)
- Mild peri-infundibular lymphocytic cell infiltrate and perifollicular collagen deposition present in 40% of cases
Microscopic (histologic) images
Contributed by Jodi Speiser, M.D.
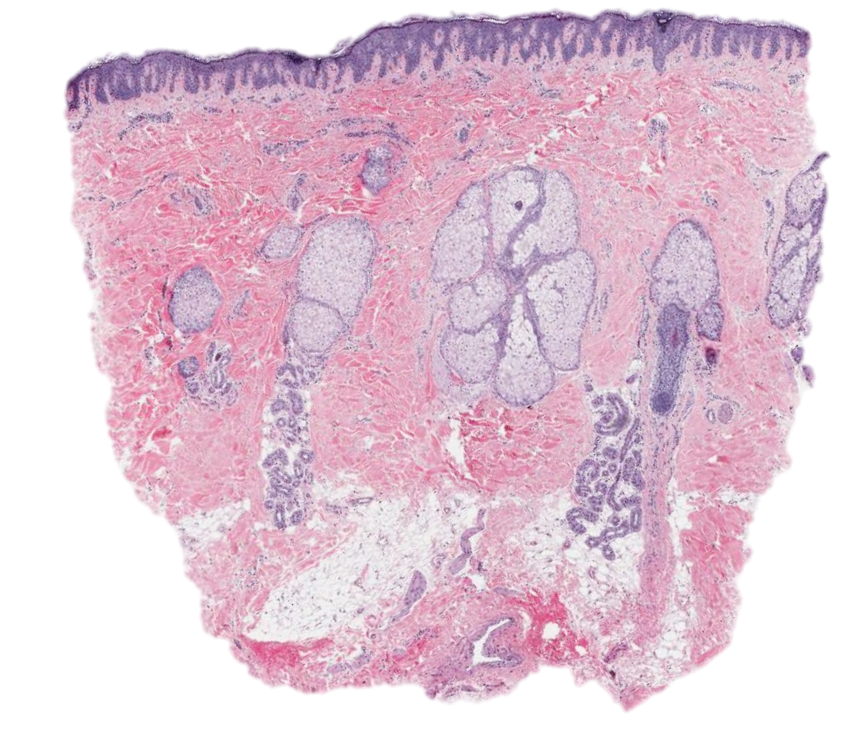
Vertical section of scalp biopsy
Positive stains
- Elastic Verhoeff-van Gieson stain typically shows delicate and thin elastic fiber network without loss, clumping, thickening or recoil (Am J Dermatopathol 2018;40:254, Am J Dermatopathol 2017;39:556)
- Periodic acid-Schiff stain shows normal basement membrane thickness
Sample pathology report
- Skin, left scalp, punch biopsy:
- Nonscarring alopecia (see comment)
- Comment: Histological sections show a decrease in hair follicles with a mild periadnexal lymphocytic infiltrate around the upper third of the hair follicle. No peribulbar inflammation is present in the sections examined. There are increased vellus hairs present. Some sections show prominent sebaceous glands. PAS stain shows normal basement membrane thickness and EVG stain shows preservation of elastic fibers. These findings are consistent with androgenic alopecia.
Differential diagnosis
- Telogen effluvium:
- Increased telogen hairs without follicular miniaturization
- Alopecia areata:
- Uniformly miniaturized follicles with less variation in hair size
- Lower terminal to vellus and anagen to catagen ratios compared to androgenic alopecia
- Peribulbar lymphocytic infiltrate
- Traumatic alopecia (traction alopecia / trichotillomania):
- Melanin pigment casts and trichomalacia with increased catagen hairs and no follicular miniaturization
- Cicatricial alopecia:
- Follicular scars with absent elastic fibers
- Fibrosing alopecia in a pattern distribution:
- Lichenoid inflammatory infiltrate in the upper follicle region, peripilar casts and loss of follicular openings
- Syphilis:
- Superficial and deep perivascular and perifollicular lymphoplasmacytic infiltrate and sometimes necrotizing pustular folliculitis
Board review style question #1
Which of the following is true about androgenic alopecia?
- No association with several other medical conditions
- Positive hair pull test
- Progressive miniaturization with varying size of the hair follicles
- Scarring alopecia
Board review style answer #1
C. Progressive miniaturization with varying size of the hair follicles
Comment Here
Reference: Androgenic alopecia
Comment Here
Reference: Androgenic alopecia
Board review style question #2
Which of the following features is observed in androgenic alopecia?
- Increased number of terminal hair follicles
- No fibrous tracts
- No hair miniaturization
- Reduced terminal to vellus ratio of 4:1 or less
Board review style answer #2

