
Skin nonmelanocytic tumor
Benign (nonmelanocytic) epidermal tumors or tumor-like lesions
Inflammatory linear verrucous epidermal nevus (ILVEN)
Author: Gauri Panse, M.D.
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.

Last author update: 9 October 2024
Last staff update: 9 October 2024
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Inflammatory linear verrucous epidermal nevus (ILVEN)

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Panse G. Inflammatory linear verrucous epidermal nevus (ILVEN). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticILVEN.html. Accessed April 3rd, 2025.
Definition / general
- Inflammatory linear verrucous epidermal nevus (ILVEN) is a variant of epidermal nevus that most commonly occurs during childhood
- It is characterized by pruritic, erythematous papules and plaques that occur along the lines of Blaschko
Essential features
- ILVEN is a rare form of epidermal nevus that presents in early childhood
- It is clinically characterized by a mostly unilateral, Blaschko linear, hyperkeratotic, erythematous lesion that is intensely pruritic
- Histopathologically, the lesion shows acanthosis, hyperkeratosis and a variable inflammatory infiltrate
- ILVEN is typically resistant to treatment
Terminology
- Verrucous epidermal nevus
ICD coding
Epidemiology
- ILVEN usually presents in childhood, typically within the first 6 months of life; however, onset in adulthood has also been reported (Australas J Dermatol 2001;42:252, J Cutan Pathol 2021;48:140)
Sites
- Most commonly occurs on lower extremities and buttocks but other body sites can also be involved
- ILVEN is usually unilateral as it occurs along the lines of Blaschko
Pathophysiology
- Blaschko linear distribution suggests that ILVEN may arise due to somatic mutations in keratinocyte precursor cells during embryogenesis (Pediatr Dermatol 2022;39:903)
Etiology
- ILVEN is thought to be a variant of epidermal nevus; some experts believe ILVEN to be a form of mosaic inflammatory disorder (Pediatr Dermatol 2022;39:903)
Clinical features
- ILVEN presents as a pruritic erythematous plaque along the lines of Blaschko (Australas J Dermatol 2001;42:252)
- Often present unilaterally (Pediatr Dermatol 1985;3:15)
- Lower extremities are more commonly affected (Australas J Dermatol 2001;42:252)
Diagnosis
- Diagnosis is typically made by clinical findings, with histopathological examination for confirmation
Prognostic factors
- Smaller lesions show favorable prognosis and are amenable to surgical excision
- Larger lesions involving significant body surface areas are less likely to respond to treatment
Case reports
- 5 year old boy with Blaschko linear erythematous papules on bilateral lower extremities (Pediatr Dermatol 2019;36:404)
- 13 year old girl with unilateral Blaschkoid psoriasiform plaques (Pediatr Dermatol 2022;39:757)
- 49 year old woman with linear scaly papules and plaques unilaterally on the lower extremity (J Cutan Pathol 2021;48:140)
Treatment
- Surgical excision for smaller lesions (Ann Plast Surg 2001;47:285)
- Cryotherapy (Dermatology 2013;226:342)
- Laser ablation (Open Access Maced J Med Sci 2017;5:454)
- Topical therapies such as retinoids, corticosteroids or calcipotriol (Clin Exp Dermatol 2021;46:940)
Clinical images
Contributed by Christine Ko, M.D.

Linear hyperkeratotic plaque
Gross description
- Raised hyperkeratotic plaque
Microscopic (histologic) description
- Skin biopsy shows psoriasiform epidermal hyperplasia with papillomatosis and hyperorthokeratosis alternating with parakeratosis (Pediatr Dermatol 1985;3:15)
- Hypergranulosis is seen in areas of hyperorthokeratois; granular layer may be diminished in the areas of parakeratosis (Pediatr Dermatol 1985;3:15)
- Variable inflammatory infiltrate may be seen (Pediatr Dermatol 1985;3:15)
- Cases with spongiotic changes have been described in ILVEN (Dermatology 2006;212:103)
Microscopic (histologic) images
Contributed by Gauri Panse, M.D.

Acanthosis and hyperkeratosis

Alternating
hyperorthokeratosis
and
parakeratosis
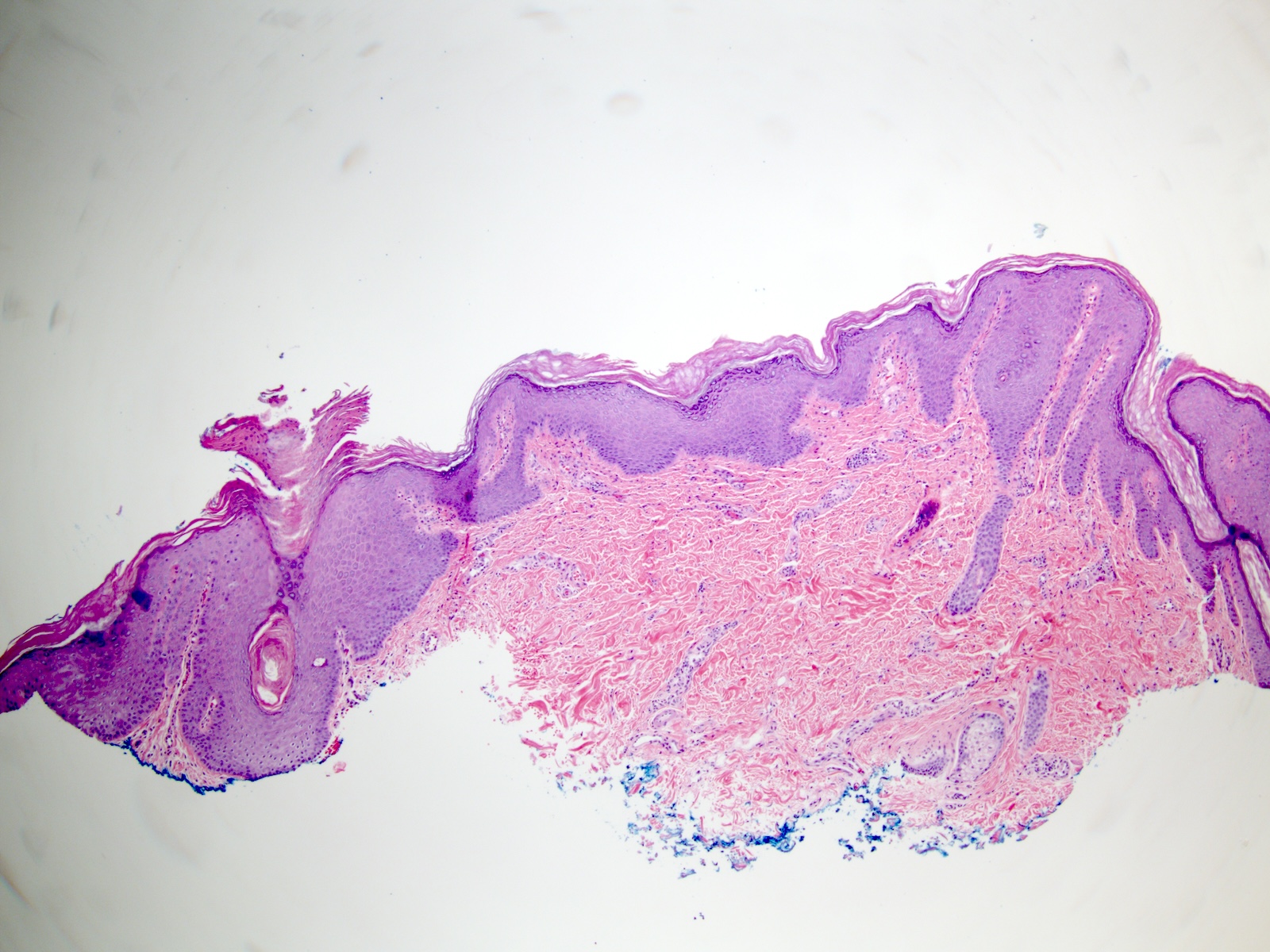
Epidermal hyperplasia

Mild dermal inflammation

Papillomatosis
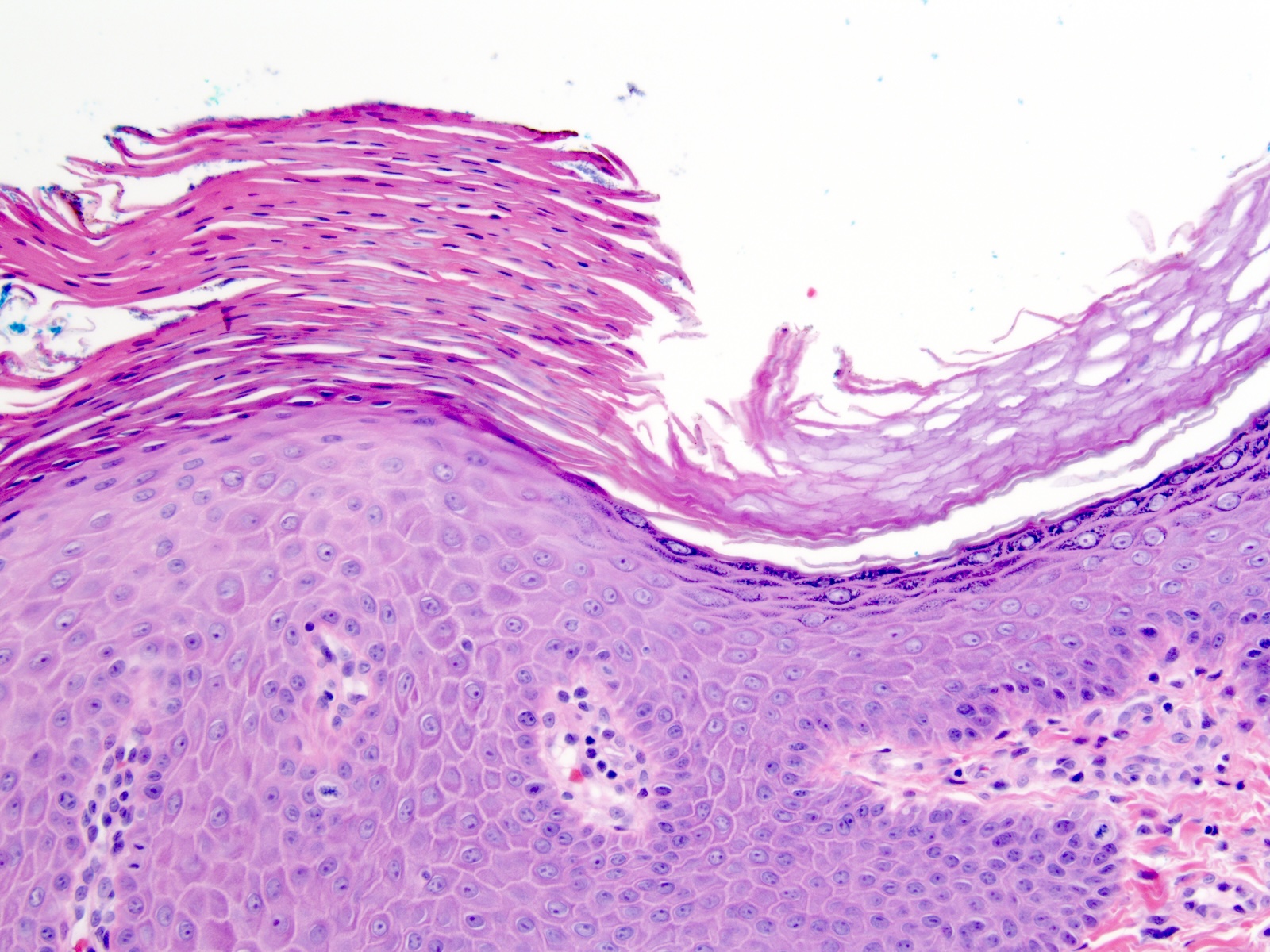
Focal hypogranulosis
Molecular / cytogenetics description
- Single case of ILVEN with GJA1 mutation has been reported (J Invest Dermatol 2017;137:967)
- CARD14 mutations have been also been reported in a small number of cases of ILVEN (J Invest Dermatol 2021;141:2979, Pediatr Dermatol 2022;39:903)
Sample pathology report
- Skin, biopsy:
- Inflammatory linear verrucous epidermal nevus (see comment)
- Comment: The lesion shows psoriasiform epidermal hyperplasia with alternating compact hyperorthokeratosis overlying hypergranulosis and parakeratosis overlying hypogranulosis. These histopathological changes are typical of ILVEN, which typically occurs in childhood and is distributed linearly along the lines of Blaschko. Clinical correlation is recommended
Differential diagnosis
- Seborrheic keratosis:
- Acanthosis with mostly orthohyperkeratosis
- Papillomatosis with horn pseudocysts
- Granular layer is intact
- Typically seen in older individuals
- Linear psoriasis:
- Acanthosis with dry parakeratosis containing neutrophils
- Diffuse hypogranulosis
- Prominent blood vessels in the papillary dermis
- Lichen striatus:
- Interface dermatitis
- Spongiosis may be present
- Superficial and deep perivascular and perieccrine inflammation
- Linear porokeratosis:
- Characterized by presence of cornoid lamellae (tiered parakeratosis, with underlying focal hypogranulosis and necrotic keratinocytes)
- Incontinentia pigmenti:
- Spongiotic microvesicles, apoptotic keratinocytes and intraepidermal eosinophils in vesicular stage
- Acanthosis, papillomatosis, hyperkeratosis and apoptotic keratinocytes in verrucous stage
- Pigment incontinence without significant epidermal hyperplasia in hyperpigmented stage
- Epidermal atrophy in atrophic / hypopigmented stage
Board review style question #1
The lesion shown above is seen unilaterally on the skin of the left thigh of a 3 month old boy. What is the diagnosis?
- Actinic keratosis
- Impetigo
- Inflammatory linear verrucous epidermal nevus (ILVEN)
- Psoriasis
- Seborrheic keratosis
Board review style answer #1
C. Inflammatory linear verrucous epidermal nevus (ILVEN). The shave biopsy of skin shows acanthosis, mature keratinocytes and overlying alternating orthokeratosis and parakeratosis. These findings and the clinical presentation are characteristic of ILVEN. Answer A is incorrect because actinic keratosis shows atypia of the basal keratinocytes and is typically seen in sun damaged skin of older individuals. The basilar keratinocytes are mature in the skin of this 3 month old child and the clinical presentation and pathological findings are not typical of actinic keratosis. Answer B is incorrect because skin biopsies in impetigo show a subcorneal separation with acantholysis and clusters of bacterial organisms. The findings seen here are not those of impetigo. Answer D is incorrect because psoriasis typically shows loss of granular cell layer with overlying dry parakeratosis containing neutrophils. Changes of psoriasis are not seen in this case. Answer E is incorrect because, while the histopathological changes seen here may be compatible with seborrheic keratosis, the clinical presentation is not consistent with this diagnosis. Seborrheic keratosis is seen in older individuals. A seborrheic keratosis-like lesion presenting in childhood is likely to be an epidermal nevus.
Comment Here
Reference: ILVEN
Comment Here
Reference: ILVEN
Board review style question #2
Which of the following is a characteristic histopathological finding in inflammatory linear verrucous epidermal nevus (ILVEN)?
- Acanthosis with alternating orthokeratosis and parakeratosis
- Cornoid lamellae
- Interface dermatitis with perieccrine lymphocytic infiltrate
- Intraepidermal collections of neutrophils
- Spongiotic microvesicles, apoptotic keratinocytes and intraepidermal eosinophils
Board review style answer #2
A. Acanthosis with alternating orthokeratosis and parakeratosis. These histopathological findings are typical of ILVEN. Answer B is incorrect because cornoid lamellae are associated with porokeratosis and not seen in ILVEN. Answer C is incorrect because lichen striatus typically presents with interface dermatitis with perieccrine lymphocytic infiltrate. Answer D is incorrect because psoriasis usually presents with intraepidermal collections of neutrophils. Answer E is incorrect because spongiotic microvesicles, apoptotic keratinocytes and intraepidermal eosinophils may be seen in the vesicular stage of incontinentia pigmenti.
Comment Here
Reference: ILVEN
Comment Here
Reference: ILVEN
