
Salivary glands
Inflammatory
Sjögren syndrome
Editorial Board Member: Lisa Rooper, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 19 December 2023
Last staff update: 19 December 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Sjögren syndrome

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ormandy A, Balgobind S. Sjögren syndrome. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandssjogren.html. Accessed April 3rd, 2025.
Definition / general
- Chronic autoimmune disorder of the salivary and lacrimal exocrine glands
- Primary etiological events remain unknown (CMAJ 2014;186:E579)
- Characterized by lymphocytic infiltrates of the affected glands with subsequent dysfunction of these glands and the clinical picture of sicca syndrome
- Considered primary if not associated with other systemic disease or secondary if it occurs in association with another underlying autoimmune condition (Clin Exp Med 2022;22:9)
Essential features
- Chronic autoimmune disorder of uncertain etiology
- Characterized by focal lymphocytic sialadenitis with subsequent clinical sequela including keratoconjunctivitis sicca (dry eyes) and xerostomia (dry mouth)
- Diagnosed using a combination of subjective and objective measures as determined by the 2016 American College of Rheumatology / European League Against Rheumatism (ACR / EULAR) classification
- Salivary gland biopsy findings consistent with diagnosis are focal lymphocytic sialadenitis with a focus score (FS) ≥ 1
Terminology
- Not recommended: Mikulicz disease (Lancet 2005;366:321)
Epidemiology
- One of the 3 most common autoimmune disorders (Lancet 2005;366:321)
- F:M = 9:1 (Clin Exp Med 2022;22:9)
- Bimodal distribution
- Third and fourth decade
- Sixth decade (Lancet 2005;366:321)
- Incidence of 6.92 per 100,000 person-years (person-years is defined as the estimate of the actual time at risk in years that all persons contributed to a study) (95% confidence interval, 4.98 - 8.86)
- Prevalence of 60.82 cases per 100,000 inhabitants (Europe, South America, Asia) (95% confidence interval, 43.69 - 77.94) (Ann Rheum Dis 2015;74:1983)
Sites
- Exocrine glands
- Notably lacrimal and salivary glands (Eur J Oral Sci 2018;126:37)
Pathophysiology
- Pathological basis of the disease remains unknown
- Numerous theories have been proposed; however, a consensus has not been established (Immunol Lett 2011;141:1)
Etiology
- Etiology is unknown
- Likely multifactorial with potential genetic, environmental and hormonal factors suggested; however, no causal associations have been demonstrated (Clin Exp Rheumatol 2022;40:2211)
- Primary Sjögren syndrome
- 90% of patients with high anti-Ro and anti-La antibody titers are HLA DR3 positive (Clin Med (Lond) 2007;7:53)
- Secondary Sjögren syndrome
- Sjögren syndrome associated with rheumatoid arthritis has a different genetic background (HLA DR4) (Lancet 2005;366:321)
Diagrams / tables
Images hosted on other servers:

ACR / EULAR
classification criteria
for primary Sjögren
syndrome
Clinical features
- Keratoconjunctivitis sicca (dry eyes)
- Xerostomia (dry mouth)
- Enlarged salivary glands
- Extraglandular manifestations include
- Musculoskeletal
- Myalgia, arthralgia and morning stiffness
- Dermatological
- Xerosis
- Respiratory tract
- Rhinosinusitis
- Vocal hoarseness
- Chronic cough (Clin Exp Med 2022;22:9)
- Musculoskeletal
Diagnosis
- 2016 ACR / EULAR classification system
- Score ≥ 4 is compatible with a diagnosis of primary Sjögren syndrome in patients experiencing ocular or oral dryness or with clinical suspicion due to systemic features (Arthritis Rheumatol 2017;69:35)
- Factors assessed include
- Labial salivary gland biopsy with lymphocytic sialadenitis and focus score ≥ 1 (3 points)
- Anti-SSA (Ro) positive serology (3 points)
- Ocular staining score ≥ 5 (1 point)
- Schirmer test ≤ 5 mm / 5 min (1 point)
- Unstimulated whole saliva flow rate ≤ 1 mL/min (1 point)
- Exclusion criteria
- History of head and neck radiation treatment
- Active hepatitis C infection
- Sarcoidosis, amyloidosis
- IgG4 related disease
- Graft versus host disease
- Acquired immunodeficiency syndrome (Arthritis Rheumatol 2017;69:35)
Laboratory
- Positive anti-SSA (Ro) antibodies and anti-SSB (La) antibodies
- Emerging potential biomarkers: muscarinic type 3 receptor (M3R), salivary calprotectin and carbamylated proteins (homocitrulline) (Eur J Oral Sci 2018;126:37)
Radiology description
- Sialography
- Serial Xray projections taken following injection of contrast medium
- Imaging with computed tomography (CT) and magnetic resonance imaging (MRI) has also been developed producing 3 dimensional images of the ductal system
- Dilatation of ducts and punctate collections of contrast medium (sialectasis)
- Sparsity of ductal branching
- Less commonly used (J Clin Med 2020;9:2492)
- Serial Xray projections taken following injection of contrast medium
- MRI
- Heterogeneous signal intensity distribution on T1 and T2 weighted images conveying a salt and pepper appearance
- Cystic changes in advanced disease (J Clin Med 2020;9:2492)
- Ultrasound
- Hypoechogenic areas, hyperechogenic reflections and poorly defined salivary gland borders (J Clin Med 2020;9:2492)
- Ultrasound findings may be incorporated in the diagnostic features in the future; however, these require further validation (Clin Exp Rheumatol 2018;36:159)
Radiology images
Images hosted on other servers:

Sialography findings: normal versus Sjögren

Ultrasound findings
suggestive of
primary Sjögren
syndrome
Prognostic factors
- High focus score predicts greater decline in unstimulated salivary flow over time (Ann Rheum Dis 2008;67:949)
- Overall increased risk of lymphoma with an estimated risk of 5 - 15% of patients (Presse Med 2012;41:e511)
- Risk of lymphoma thought to be 40 times greater than the general population (Ann Intern Med 1978;89:888)
- Most commonly low grade non-Hodgkin lymphoma, specifically extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma
- Features thought to be associated with increased risk of transformation to lymphoma include
- High focus score
- Particularly focus score ≥ 3 has a positive predictive value of 16% and negative predictive value of 98% for non-Hodgkin lymphoma (Ann Rheum Dis 2014;73:1537)
- Detection of ectopic germinal centers, although some studies did not find these a predictive factor for MALT lymphoma (Rheumatology (Oxford) 2013;52:276)
- Usually correlate with a higher focus score (Ann Rheum Dis 2014;73:1537)
- High focus score
Case reports
- 22 year old woman with a diagnosis of ranula preceding a diagnosis of primary Sjögren syndrome (World J Clin Cases 2021;9:5701)
- 41 year old woman with a varied clinical presentation of primary Sjögren syndrome (BMJ Case Rep 2019;12:e231802)
- 55 year old woman with bilateral parotid gland enlargement and Sjögren syndrome (J Int Oral Health 2015;7:72)
- 60 year old woman with cutaneous mucosa associated lymphoid tissue lymphoma complicating Sjögren syndrome (World J Clin Cases 2022;10:4509)
Treatment
- Primarily symptomatic treatment, including
- Artificial tears
- Saliva replacement
- NSAIDs for musculoskeletal symptoms (Clin Med (Lond) 2007;7:53)
Clinical images
Images hosted on other servers:


Bilateral parotid gland enlargement
Microscopic (histologic) description
- Historically minor salivary gland biopsy has been assessed
- In a limited study, parotid gland biopsy was shown to have similar diagnostic sensitivity and specificity (Rheumatology (Oxford) 2007;46:335)
- Focal lymphocytic sialadenitis is the histological hallmark
- 1 or more dense aggregates with 50 or more lymphocytes
- Usually in perivascular or periductal areas
- Cannot be attributed if dominated by features of nonspecific chronic sialadenitis or chronic sclerosing sialadenitis (Reumatismo 2018;70:146)
- Other features are nonspecific and include
- Nonspecific chronic sialadenitis and chronic sclerosing sialadenitis
- Mild to diffuse lymphocytic infiltrates
- Progressive atrophy of normal salivary gland acini
- Duct dilatation
- Variable parenchymal fibrosis
- Lymphoepithelial lesions (seen in ~50% of patients with primary Sjögren syndrome) (Clin Exp Rheumatol 2022;40:2434)
- Lymphocytic infiltrate of ducts and basal cell hyperplasia
- Ectopic germinal centers
- Recommended that these always be reported if present (Ann Rheum Dis 2017;76:1161)
- Granulomatous inflammation
- Adiposis (Autoimmun Rev 2020;19:102690, Reumatismo 2018;70:146)
- Nonspecific chronic sialadenitis and chronic sclerosing sialadenitis
- ACR / EULAR classification criteria for labial salivary gland biopsy
- Focal lymphocytic sialadenitis
- If identified, a focus score should be recorded, with a focus score ≥ 1 suggestive of Sjögren syndrome (Arthritis Rheumatol 2017;69:35)
- Focus score 1 = 1 focus of 50 lymphocytes per 4 mm2 (Arthritis Rheum 2011;63:2021)
- Recommended at least 4 labial salivary glands with a surface area of at least 8 mm2 to allow for adequate assessment and focus scoring (Ann Rheum Dis 2017;76:1161)
- Focal lymphocytic sialadenitis
Microscopic (histologic) images
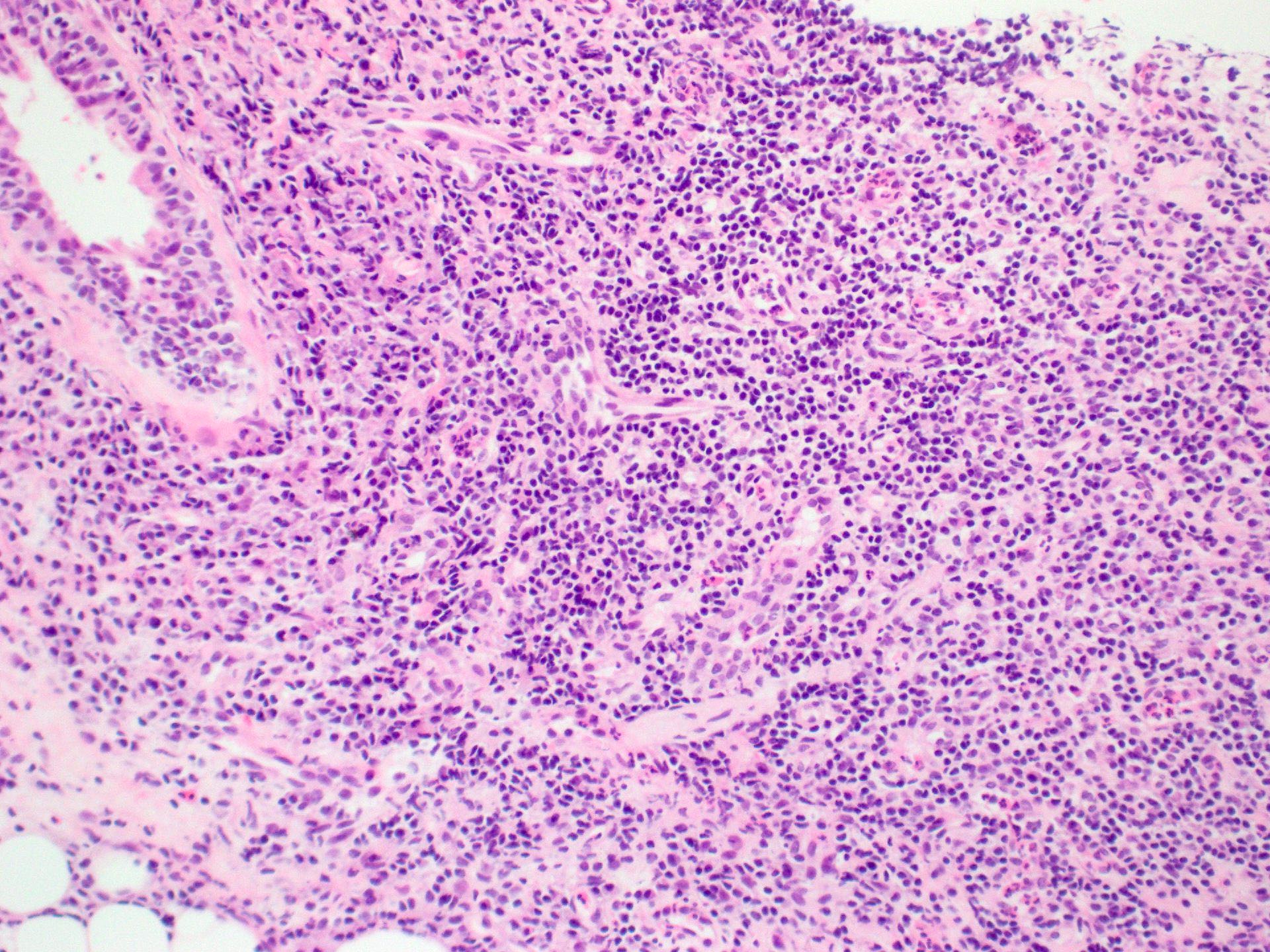
Contributed by Alice Ormandy, M.B.B.S., M.P.H. and Salman Marvi, M.D.
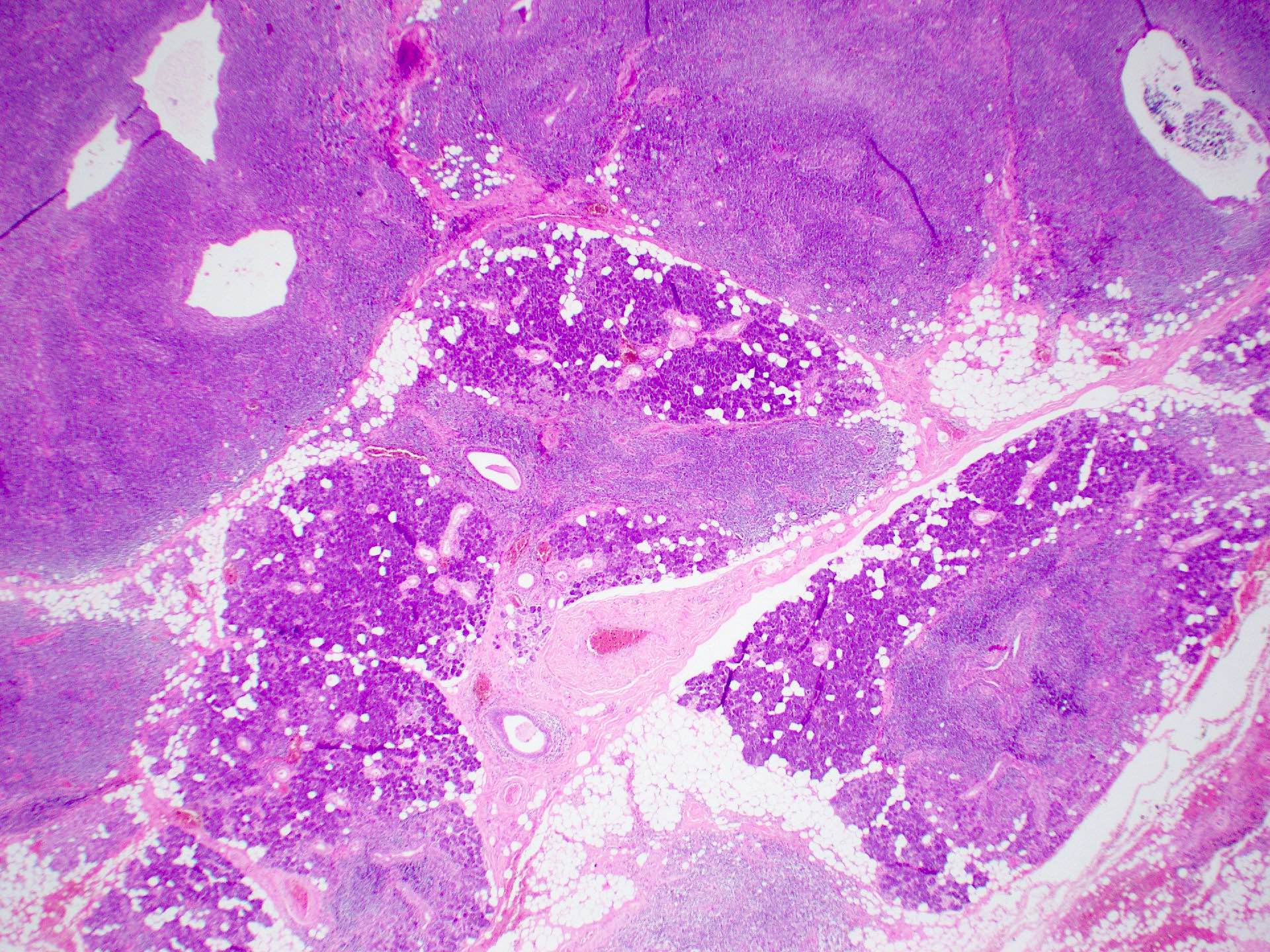
Multiple nodular lymphocytic aggregates

Lymphocytic aggregates with germinal centers

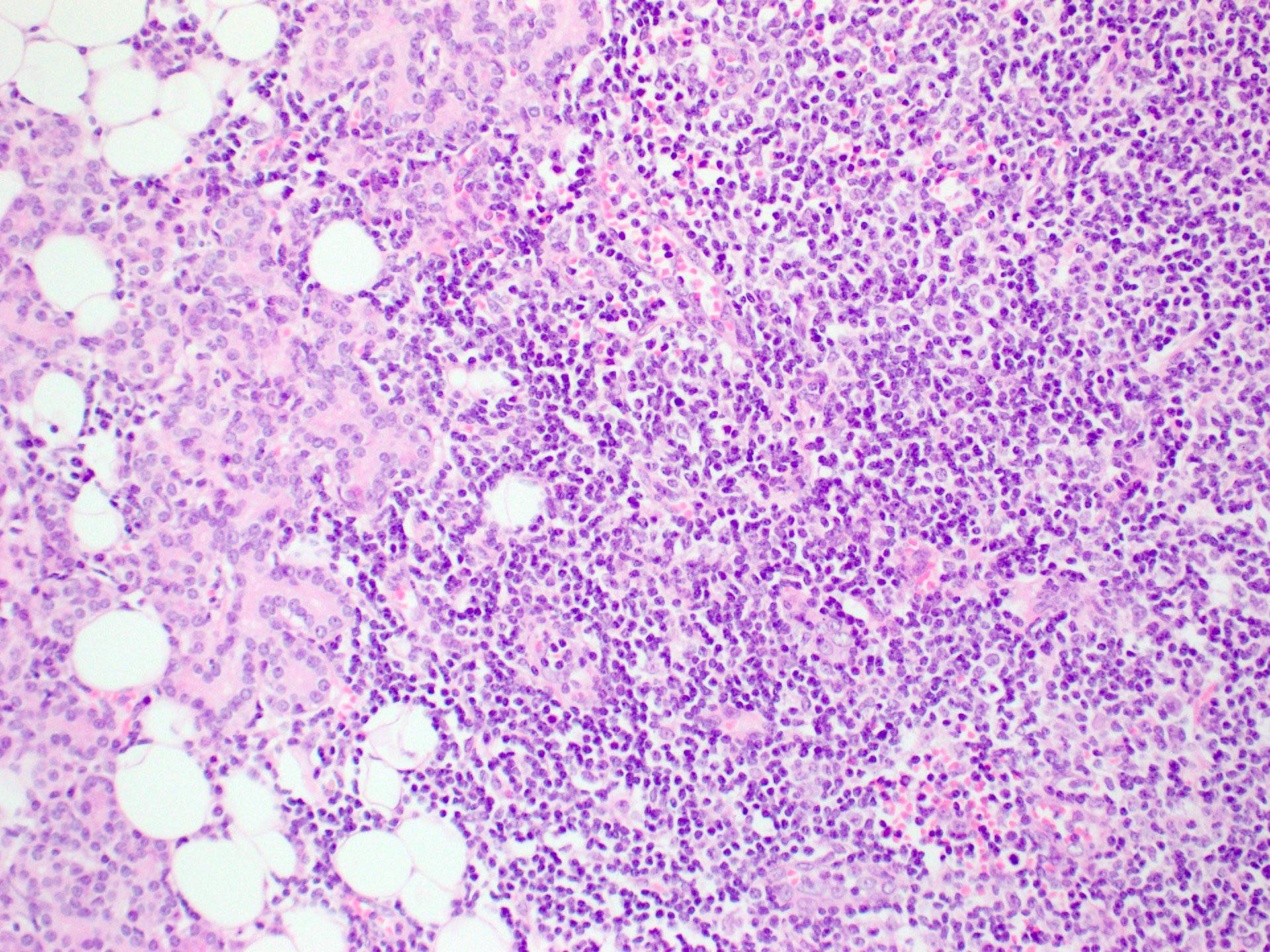
Nodular lymphocytic aggregate

Core biopsy parotid

Germinal center



Submandibular gland lymphoid aggregates

Submandibular gland germinal centre
Cytology description
- Nonspecific findings
- May find benign myoepithelial and ductal epithelial cells interspersed with a lymphocytic infiltrate
- There may be macrophages in the background (Prog Health Sci 2013;3:178)
Cytology images
Contributed by Alice Ormandy, M.B.B.S., M.P.H.

Lymphoid clusters

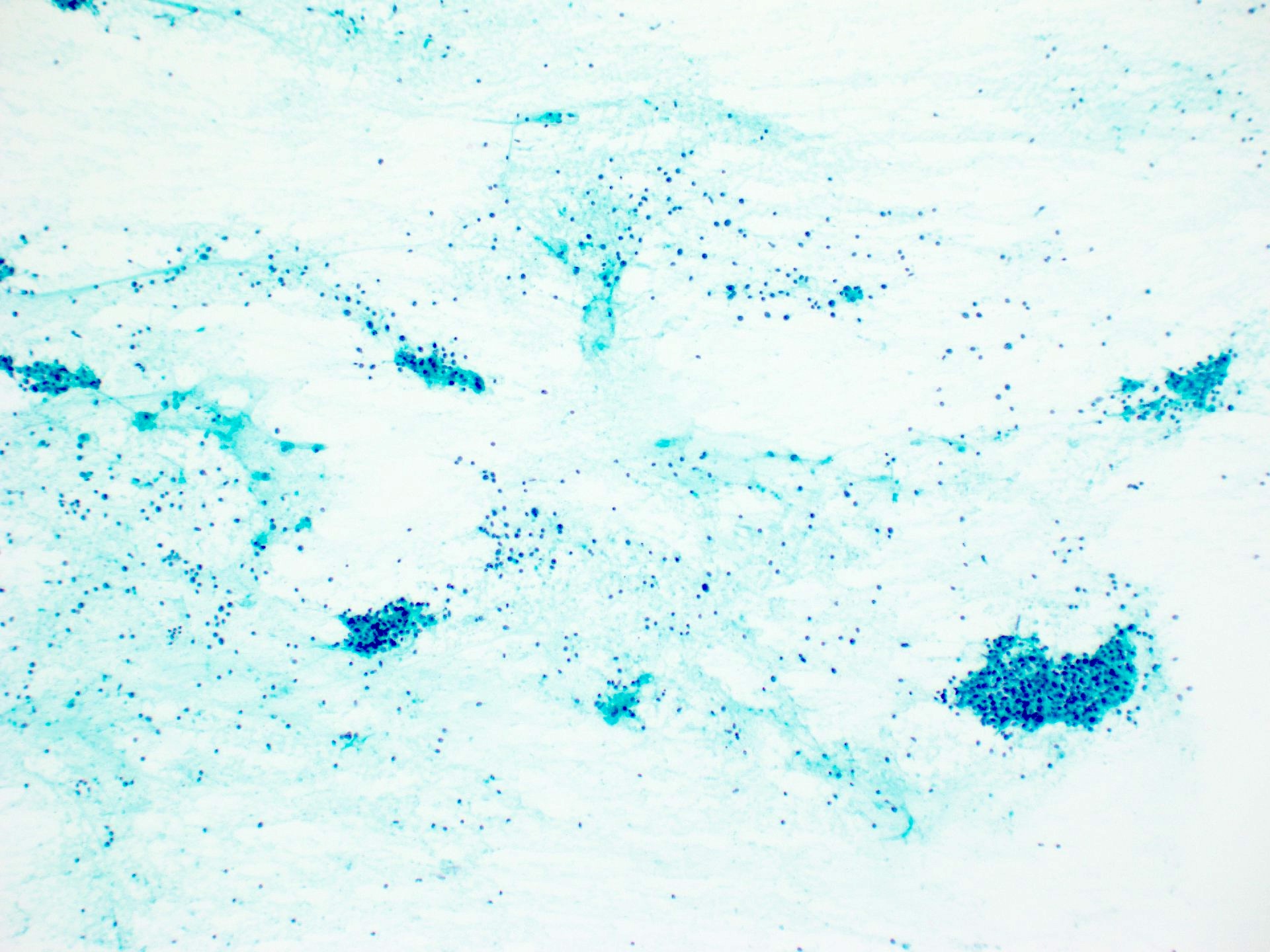
Lymphocytic infiltrate
Positive stains
- BCL6 highlight germinal center B cells
- CD21 / CD23 can highlight follicular dendritic cells in germinal centers (Reumatismo 2018;70:146)
Sample pathology report
- Salivary gland, biopsy
- Focal lymphocytic sialadenitis with associated mild atrophy of the salivary acini (see comment)
- Comment: There is a single nodular lymphocytic aggregate (1 cluster of > 50 lymphocytes per 4 mm2, focus score = 1). There is no germinal center formation and no features to suggest malignancy. The finding of focal chronic sialadenitis with a focus score of 1 is compatible with the diagnosis of Sjögren syndrome in the correct clinical context. Correlation with clinical history, radiology, serology and flow cytometry is recommended.
Differential diagnosis
- Nonspecific chronic sialadenitis:
- Clinical pathological correlation required
- IgG4 disease:
- Plasma cell rich inflammatory infiltrate
- Increased ratio of IgG4 to IgG plasma cells
Board review style question #1

What features on the salivary gland biopsy shown from a patient with Sjögren syndrome are associated with an increased risk of lymphoma?
- Atrophy
- Fat infiltration
- Fibrosis
- Focus score ≥ 3
Board review style answer #1
D. Focus score ≥ 3. A high focus score, particularly ≥ 3, has a positive predictive value of 16% and negative predictive value of 98% for non-Hodgkin lymphoma (Ann Rheum Dis 2014;73:1537). Answers A, B and C are incorrect because fat infiltration and fibrosis are all features that can be present in salivary gland biopsies of patients with Sjögren syndrome; however, they have not been associated with increased risk of lymphoma in these patients.
Comment Here
Reference: Sjögren syndrome
Comment Here
Reference: Sjögren syndrome
Board review style question #2
What is the most common salivary gland lymphoma occurring in patients with primary Sjögren syndrome?
- Diffuse large B cell lymphoma
- Extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma
- Follicular lymphoma
- Hodgkin lymphoma
Board review style answer #2
B. Extranodal marginal zone of mucosa associated lymphoid tissue (MALT) lymphoma. Answers A and C are incorrect because diffuse large B cell lymphoma and follicular lymphoma have been reported in salivary glands; however, they are not the most common lymphoma in this site. Answer D is incorrect because Hodgkin lymphoma is rare in salivary glands (Rheumatology (Oxford) 2022;61:3818).
Comment Here
Reference: Sjögren syndrome
Comment Here
Reference: Sjögren syndrome
