
Salivary glands
Inflammatory
Lymphoepithelial sialadenitis
Author: Kim A. Ely, M.D.
Editorial Board Member: Lisa Rooper, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 4 December 2020
Last staff update: 13 April 2021
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: lymphoepithelial sialadenitis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ely K. Lymphoepithelial sialadenitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandslymphoepithelialsialadenitis.html. Accessed April 3rd, 2025.
Definition / general
- Part of a heterogeneous group of lesions with a prominent lymphoid component that involves the salivary glands (Med Oral Patol Oral Cir Bucal 2007;12:E479)
- May be isolated or associated with Sjögren syndrome
- Histologically characterized by the lymphoepithelial lesion, which is formed by a proliferation of ductal remnants permeated by lymphocytes (Virchows Arch 1999;434:315)
Essential features
- May be isolated or associated with Sjögren syndrome
- Usually occurs in women
- Affects the parotid (90%) and submandibular gland (10 - 15%) with rare involvement of the minor salivary glands
- Histologically characterized by the lymphoepithelial lesion, which is formed by a proliferation of ductal remnants permeated by lymphocytes
- Indolent behavior; however, continued observation is mandatory because of an increased risk for lymphoma development (MALT lymphoma)
Terminology
- Myoepithelial sialadenitis: a misnomer as ultrastructural and immunohistochemical studies showed that the cells involved are not myoepithelial cells but rather basal epithelial cells (Virchows Arch 1999;434:315)
- Autoimmune sialadenitis
- Lymphoepithelial lesion
- Sjögren sialadenitis
ICD coding
- ICD-10: K11.2 - sialoadenitis
Epidemiology
- May be isolated or associated with Sjögren syndrome (Am J Clin Pathol 1999;111:S94)
- Usually affects women
Sites
- Affects the parotid (90%) and submandibular gland (10 - 15%) with rare involvement of the minor salivary glands (Ellis: Tumors of the Salivary Glands, 3rd Series, 1996)
- Commonly bilateral
- If the submandibular gland is affected in patients with Sjögren syndrome, the parotid glands are usually also involved
Etiology
- Cause of lymphoepithelial sialadenitis unassociated with Sjögren syndrome has not been determined (Chin Med J (Engl) 2015;128:493)
- Lymphoepithelial sialadenitis in the setting of Sjögren syndrome is likely multifactorial, with environmental and genetic factors causing an abnormal autoimmune response (Pathol Int 2008;58:465)
Clinical features
- Recurring, firm swelling of the affected glands, which is sometimes associated with discomfort or pain (Med Oral Patol Oral Cir Bucal 2007;12:E479)
Laboratory
- Positive serum anti SSA, anti SSB or a positive rheumatoid factor and antinuclear antibody titer of 1:320 are present when associated with Sjögren syndrome (Med Clin North Am 2014;98:1407)
Prognostic factors
- Indolent behavior; however, continued observation is mandatory due to increased risk for lymphoma development (MALT lymphoma) (Med Oral Patol Oral Cir Bucal 2007;12:E479)
Case reports
- 18 year old woman with linear cutaneous lupus erythematosus and submandibular sialadenitis (Clin Exp Dermatol 2001;26:56)
- 21 year old woman with an infraauricular mass (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:721)
- 4 cases of thymic hyperplasia resembling lymphoepithelial sialadenitis (Am J Clin Pathol 2012;138:816)
Treatment
- Corticosteroids have been used with limited success (Med Clin North Am 2014;98:1407)
Microscopic (histologic) description
- Major salivary gland:
- Early, extent of inflammation varies with collections of small lymphocytes surrounding intralobular ducts, minimal epitheliotropism, plasma cells not prominent (Med Oral Patol Oral Cir Bucal 2007;12:E479)
- Inflammation intensifies, contains lymphoid follicles with germinal center formation and more frequent plasma cells
- As inflammation becomes diffuse, there is partial and then total acinar destruction with the only remaining epithelium being the ducts
- Remnant ducts proliferate and are infiltrated by lymphocytes, forming the lymphoepithelial lesion
- Eosinophilic, hyaline basement membrane-like material may be present among the cells of the lesion (Virchows Arch 2003;443:17)
- Overall lobular architecture is maintained
- Labial salivary gland:
- Adequate biopsy has a glandular area of at least 4 mm², optimally 10 mm² (Arthritis Rheum 2011;63:2021)
- Germinal centers and lymphoepithelial lesions are less common in lip biopsies
Microscopic (histologic) images
Contributed by James S. Lewis, M.D.
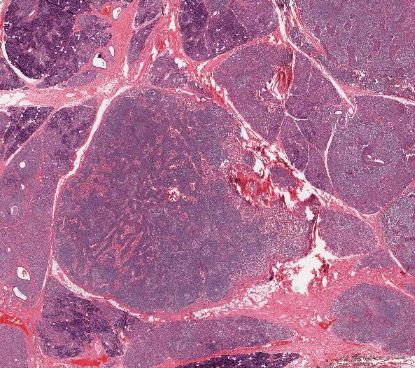
Maintenance of lobular architecture
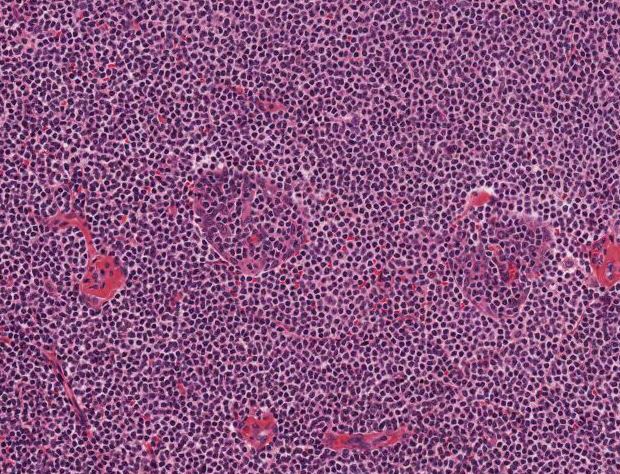
Intense chronic inflammation
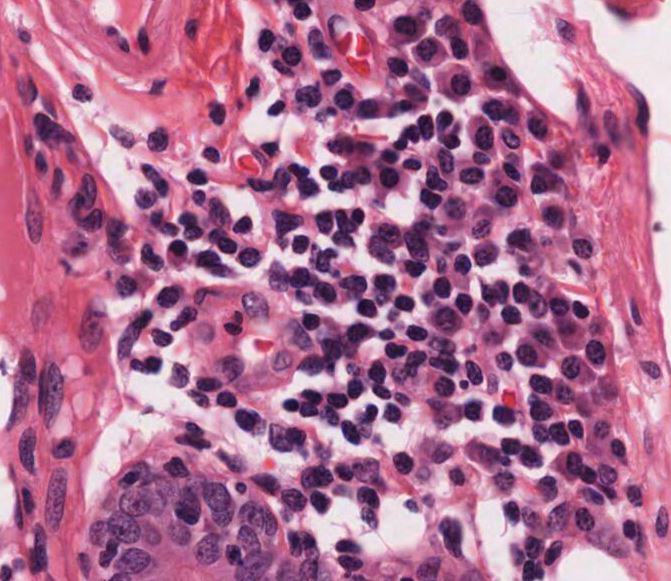
Plasma cells
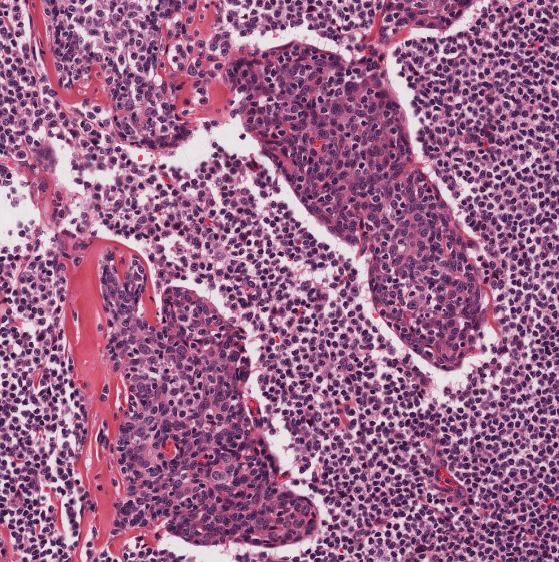
Lymphoepithelial lesion
Positive stains
- Cytokeratin, AE1 / AE3 stains lymphoepithelial lesion
Negative stains
- SMA negative within lymphoepithelial lesion
Sample pathology report
- Parotid, left, excision:
- Lymphoepithelial sialadenitis (see comment)
- Comment: There is extensive chronic inflammation with plasma cells and lymphocytes containing follicles with germinal centers. The infiltrate effaces the parenchyma, resulting in acinar loss. Residual ducts show hyperplasia of their lining as well as permeation by lymphocytes. These glandular complexes represent the lymphoepithelial lesion.
Differential diagnosis
- Extranodal marginal zone B cell lymphoma:
- May be difficult to differentiate
- Clonal monocytoid B cells both within and encircling the lymphoepithelial lesions to form halos and anastomosing cords, which can interconnect the lymphoepithelial lesions (Med Oral Patol Oral Cir Bucal 2007;12:E479)
- Sheets of plasma cells
- Monoclonality by IHC or flow cytometry (Mod Pathol 2002;15:255)
- Extension beyond capsule into adjacent tissues
- Loss of lobular architecture
- IgG4 related sialadenitis:
- Slight male predilection
- Typically submandibular gland
- Dense chronic inflammatory infiltrate rich in plasma cells with an IgG4/IgG ratio > 40%
- Fibrosis, focally storiform
- Obliterative phlebitis (Head Neck Pathol 2016;10:530)
- Absence of lymphoepithelial lesions
- Lymphoepithelial cyst:
- Well defined, unilocular cyst
- Has features of a lymph node or associated with a lymph node (Hum Pathol 2009;40:683)
- Absence of lymphoepithelial lesions
- Lymphadenoma:
- Well circumscribed (Virchows Arch 2012;460:467)
- Even distribution of uniformly sized and shaped epithelial components within lymphoid stroma
- Absence of lymphoepithelial lesions
- Chronic sialadenitis:
- Fibrosis
- Associated with sialolithiasis
- Absence of lymphoepithelial lesions
- Tumor associated lymphoid proliferation (TALP):
- Salivary gland tumor surrounded by a dense infiltrate of lymphocytes (Curr Opin Oncol 1996;8:232)
- Absence of lymphoepithelial lesions
Board review style question #1
- A 40 year old woman complaining of xerostomia, dry eyes and bilateral salivary gland enlargement undergoes excision of her parotid. After receipt of the pathologic diagnosis, her clinician tells her that she is at increased risk for which of the following?
- Burkitt lymphoma
- Hodgkin lymphoma
- Extranodal marginal zone B cell lymphoma
- Anaplastic large cell lymphoma
Board review style answer #1
C. Extranodal marginal zone B cell lymphoma. The patient has lymphoepithelial sialadenitis.
Comment Here
Reference: Lymphoepithelial sialadenitis
Comment Here
Reference: Lymphoepithelial sialadenitis
Board review style question #2
- Which of the following is true about lymphoepithelial sialadenitis?
- It is composed of myoepithelial cells, hence the name myoepithelial sialadenitis is an appropriate alternative term for this lesion
- It may be isolated or associated with Sjögren syndrome
- It affects women and men equally
- It involves the submandibular gland most commonly, followed by the minor salivary glands
Board review style answer #2
B. It may be isolated or associated with Sjögren syndrome
Comment Here
Reference: Lymphoepithelial sialadenitis
Comment Here
Reference: Lymphoepithelial sialadenitis
