

Salivary glands
Primary salivary gland neoplasms
Malignant
Carcinosarcoma


Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Carcinosarcoma

- First described by Kirklin in 1951 (Surg Gynecol Obstet 1951;92:721)
- Characterized by a variable combination of malignant epithelial and sarcomatous tumor components
- High grade, aggressive salivary gland malignancy
- Combined salivary tumor with malignant epithelial and mesenchymal component
- May arise from pre-existing pleomorphic adenoma (PA)
- Necrosis and hemorrhage are frequently seen
- Poor prognosis
- Also known as true mixed malignant tumor
- Sometimes named carcinosarcoma ex pleomorphic adenoma when tumor arises from longstanding or recurrent pleomorphic adenoma
- ICD-O: 8980/3 - carcinosarcoma, NOS
- ICD-11
- 2B67.Y & XH2W45 - other specified malignant neoplasms of parotid gland & carcinosarcoma, NOS
- 2B68.2 & XH2W45 - other specified malignant neoplasms of submandibular or sublingual glands & carcinosarcoma, NOS
- Patients are usually in their sixth to seventh decade of life
- Mean age: 60.1 years (Histopathology 2023;82:576)
- Range: 10 - 86 years (Histopathology 2023;82:576)
- M:F = ~3:2 (Histopathology 2023;82:576)
- Represents ~0.4% of all salivary gland malignancies (Pathol Annu 1993;28:279)
- Cases of salivary carcinosarcoma ex pleomorphic adenoma (SCS ex PA) represent 3 - 6% in large carcinoma ex pleomorphic adenoma (CA ex PA) series (Histopathology 2023;82:576, Virchows Arch 2017;470:601)
- Most commonly affects the parotid glands (70.3%), followed by submandibular gland (18.9%)
- Rarely affects the minor salivary glands (11.8%), with palate most commonly involved (Histopathology 2023;82:576)
- Molecular mutations are heterogeneous
- Clonal relationship between carcinomatous and sarcomatous components (Am J Surg Pathol 1996;20:277, Oral Oncol 2009;45:259)
- Derivation of the sarcomatous component has been postulated from myoepithelial cells of pleomorphic adenoma and primary carcinomatous components (Histopathology 2023;82:576)
- Recently proposed to arise with a complex multistep adenoma - carcinoma - sarcoma progression developing from a pleomorphic adenoma (Histopathology 2023;82:576, Virchows Arch 2017;470:601)
- Tumor conventionally thought to develop from a pre-existent pleomorphic adenoma for half of the cases and de novo for the rest (Oral Surg Oral Med Oral Pathol 1986;61:597, Kurume Med J 2000;47:307)
- Recent molecular studies suggest that tumor almost always develops from pleomorphic adenoma (Histopathology 2023;82:576)
- Few cases occurred after radiotherapy (Virchows Arch A Pathol Anat Histopathol 1986;409:93, J Laryngol Otol 1994;108:443, B-ENT 2016;12:339)
- Large, rapidly growing infiltrative mass
- May have a longstanding mass or history of recurrent mass that represents a pleomorphic adenoma (Laryngoscope 2020;130:E335)
- Facial pain and paresis (facial nerve palsy)
- Otalgia
- Dysphagia
- Skin ulceration
- May have a history of radiation therapy for pleomorphic adenoma
- Advanced stage of presentation with lymph node metastasis and distant hematogenous spread (17.2%), mostly to lung and liver; there is a high frequency of local recurrence (Laryngoscope 2020;130:E335, Histopathology 2023;82:576)
- Neck mass that typically leads to imaging studies (computed tomography [CT] / magnetic resonance imaging [MRI]) and fine needle aspiration (FNA)
- Definite diagnosis only rendered after surgical resection
- CT
- Irregular, heterogeneously enhancing lesion
- Peripheral, septal contrast enhancement
- May show cystic necrotic areas and marked restricted diffusion on apparent diffusion coefficient (ADC) maps (Ear Nose Throat J 2022 Sep 28 [Epub ahead of print])
- Calcifications may be present (World J Surg Oncol 2018;16:103)
- MRI
- T1 hypointense and T2 hyperintense heterogenous contrast enhancing lesion on MRI (Ear Nose Throat J 2022 Sep 28 [Epub ahead of print], J Nippon Med Sch 2018;85:51)
- Thick, irregular enhancing rim (Oral Oncol 2006;42:323)
- May be lobulated or multilobed (Case Rep Otolaryngol 2015;2015:694684)
- May show solid cystic or cystic necrotic appearance
Images hosted on other servers:

CT of head and neck

CT showing cystic necrotic areas

MRI of parotid lesion

MRI of heterogeneous mass lesion
- Prognosis is poor
- Mortality of 50% and mean survival of 2.4 - 3.6 years (Oral Surg Oral Med Oral Pathol 1986;61:597, Pathol Annu 1993;28:279, Laryngoscope 2020;130:E335)
- With a median follow up of 36 months, the 3 year overall survival was 57.6% (Otolaryngol Head Neck Surg 2023;168:775)
- 5 year overall survival was 37% and 5 year disease specific survival was 62% (Laryngoscope 2020;130:E335)
- 41 year old woman with dysphagia, facial pain and swelling of left face and 56 year old man with dysphagia and facial pain (Ear Nose Throat J 2022 Sep 28 [Epub ahead of print])
- 50 year old man with longstanding right submandibular swelling (Indian J Surg Oncol 2019;10:61)
- 67 year old man with right floor of mouth ulcer (Cureus 2023;15:e37206)
- 72 year old man with rapidly enlarged parotid mass (World J Surg Oncol 2018;16:103)
- 75 year old man with longstanding right parotid swelling (J Surg Case Rep 2021;2021:rjab361)
- Typically, surgical resection followed by adjuvant radiotherapy or chemotherapy
Images hosted on other servers:

Swelling of right parotid
- Often large (> 6 cm, mean size: 4 cm; range: 2 - 9 cm), infiltrating tumor (Laryngoscope 2020;130:E335)
- Noncapsulated to poorly circumscribed
- Can be a solid or solid cystic lesion
- Gray-white to yellow appearance in solid area
- Necrosis and hemorrhage are frequently seen
- Calcifications may be seen (World J Surg Oncol 2018;16:103)
- Smaller, often sclerotic nodule may be present that represents a pre-existing pleomorphic adenoma (Histopathology 2023;82:576)
Contributed by Alexander Tang, M.B.B.S.

Cut section of tan, fleshy carcinosarcoma
- Diagnosis of high grade carcinoma or raising a possibility of sarcoma component is required from a representative section of the tumor for appropriate surgical management, including defining the extent of resection and the levels of neck dissection required
- Variable combination of malignant epithelial and sarcomatous tumor components
- There may be more than 1 type of carcinoma or sarcoma
- Carcinomatous component commonly an adenocarcinoma (43%), salivary duct carcinoma (29.1%), undifferentiated carcinoma (26.7%), squamous cell carcinoma (18.6%) or myoepithelial carcinoma (2.3%) (Histopathology 2023;82:576)
- Recent case series showed higher frequency of myoepithelial carcinoma (31.3%) (Histopathology 2023;82:576)
- Other rare carcinomatous components include epithelial myoepithelial carcinoma, papillary cystadenocarcinoma, mucoepidermoid carcinoma, large cell neuroendocrine carcinoma (Mod Pathol 2006;19:350, Case Rep Otolaryngol 2015;2015:694684, Head Neck Pathol 2013;7:163)
- Sarcomatous component most commonly a chondrosarcoma (51.2%), osteosarcoma (29.1%), spindle cell sarcoma (27.9%), pleomorphic sarcoma (8.1%), rhabdomyosarcoma (7%)
- Heterologous component seen in 75.6% (Histopathology 2023;82:576)
- Uncommon / rare sarcoma types reported include leiomyosarcoma, liposarcoma and malignant giant cell tumor (Arch Pathol Lab Med 2001;125:812, Arch Pathol Lab Med 1995;119:69, Histopathology 1993;23:594, Arch Pathol Lab Med 1998;122:743, Oral Surg Oral Med Oral Pathol 1986;61:597, Ann Maxillofac Surg 2015;5:240)
- Intraductal pathway of tumorigenesis displays intraductal neoplasia, combined with dominant undifferentiated or salivary duct type carcinoma as an epithelial component and with pleomorphic or osteo / chondrosarcoma as a mesenchymal component
- Myoepithelial pathway of tumorigenesis displays an absence of intraductal neoplasia and almost obligate combination of myoepithelial carcinoma and chondrosarcomatous differentiation
- Sarcomatous components frequently dominate
- High grade cytomorphology; mitotic figures and necrosis are frequently seen
- Pre-existing PA may be seen and may be suggested by the presence of extensive hyalinized stroma (Head Neck Pathol 2013;7:163, Histopathology 2023;82:576)
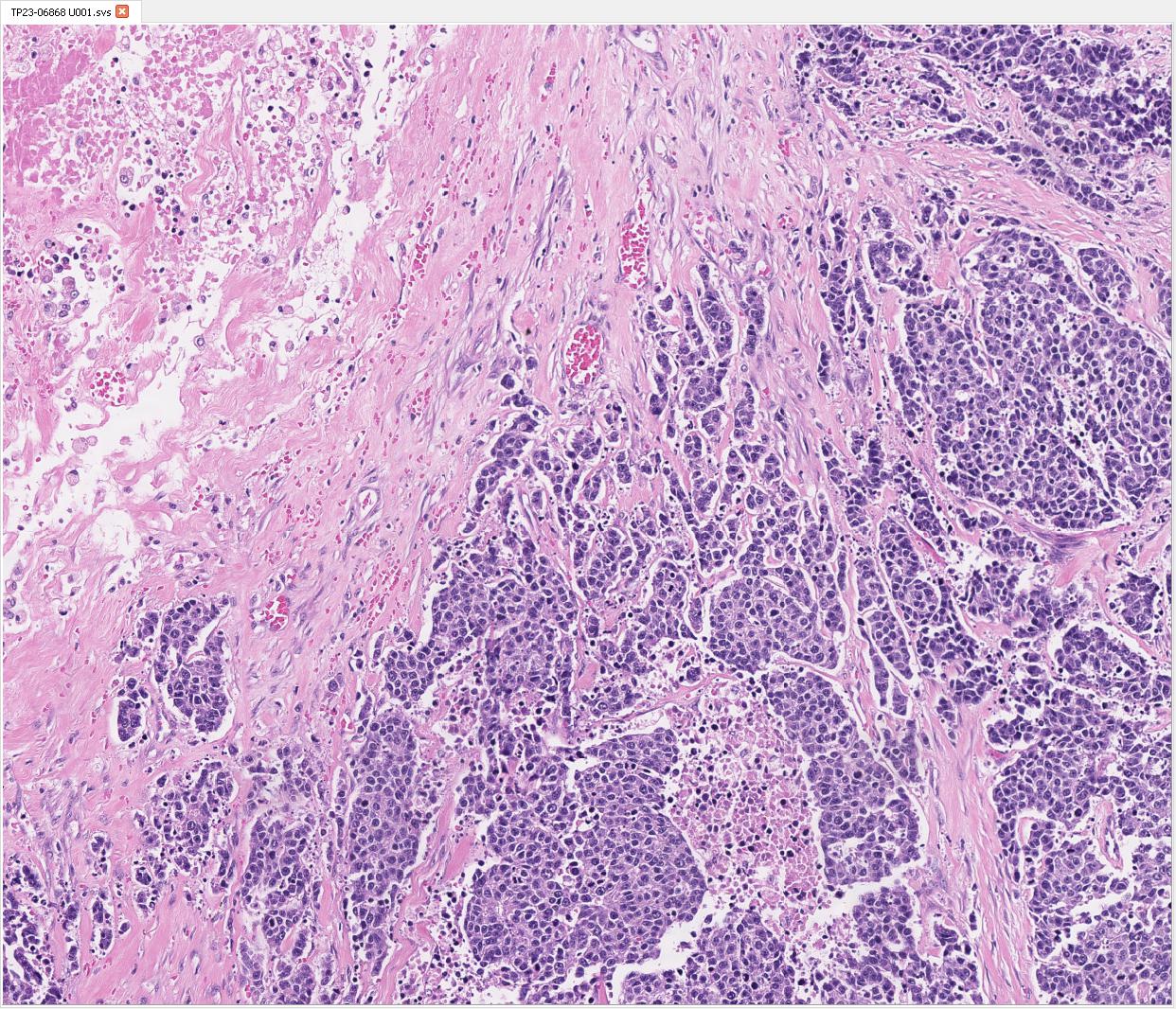
Contributed by Manish Mahadeorao Bundele, M.B.B.S., M.D.
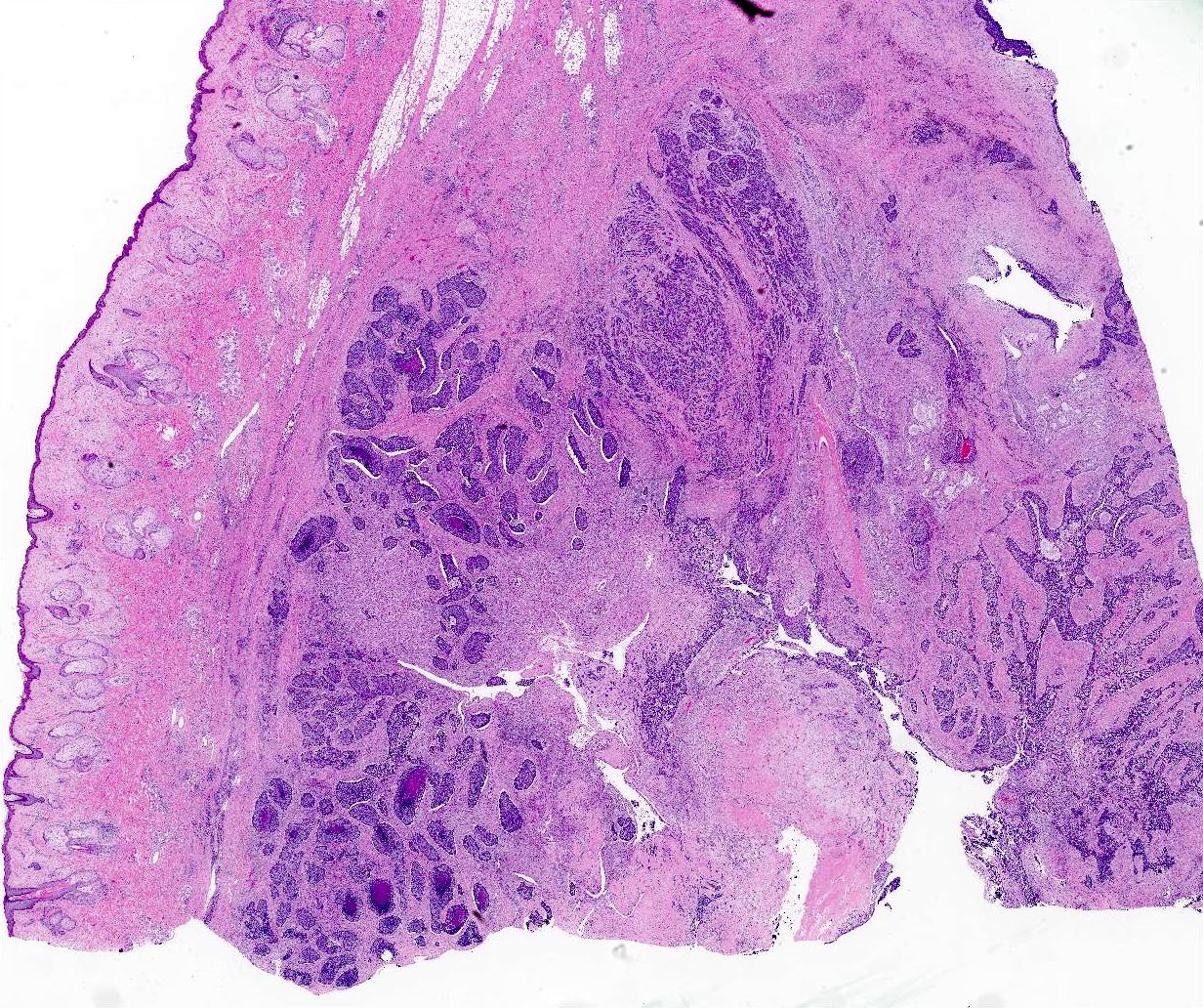
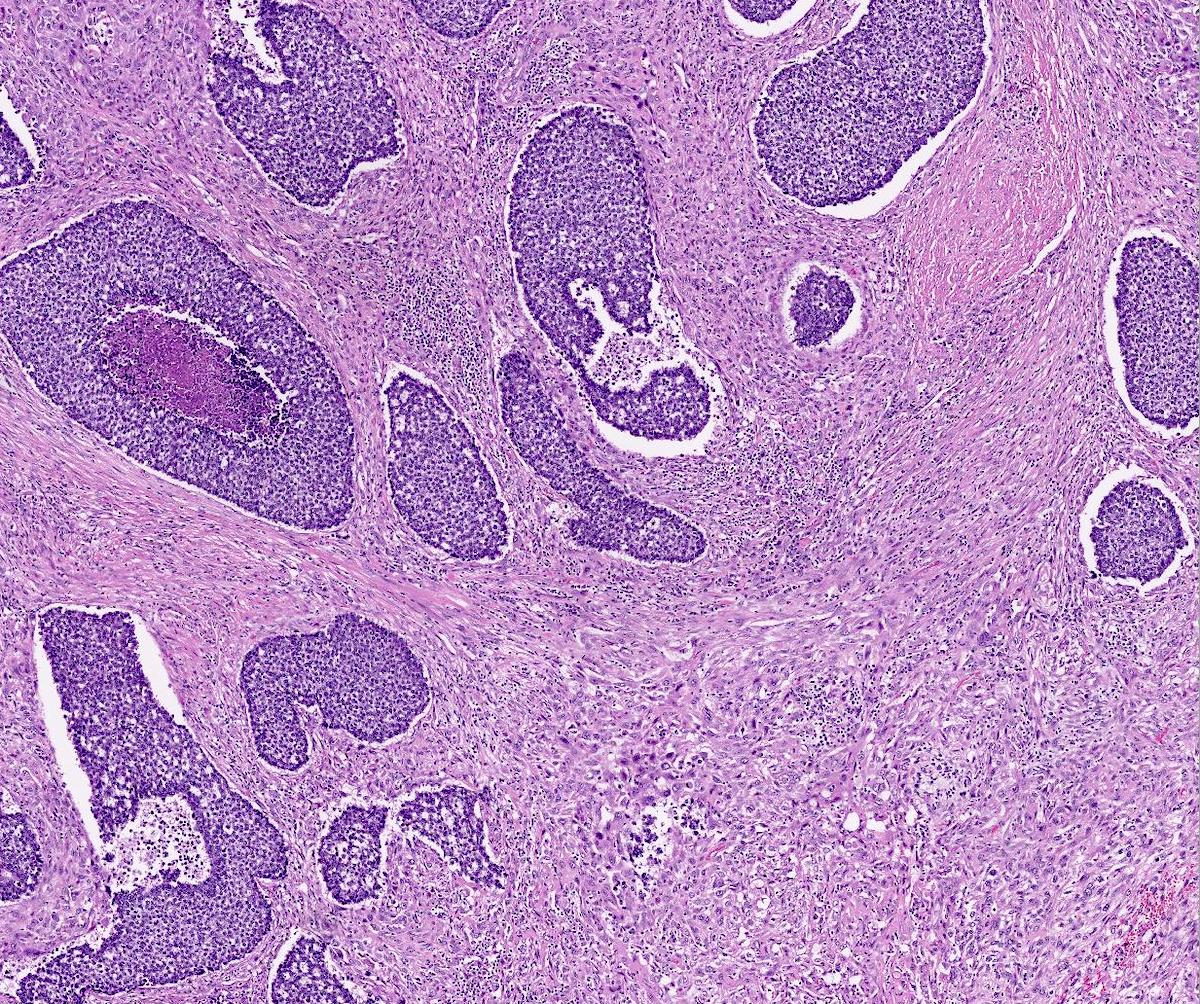
Carcinomatous and intervening sarcomatous components

Carcinosarcoma with residual PA

Sarcomatoid component with storiform pattern
Undifferentiated carcinoma with necrosis

Undifferentiated carcinoma / pleomorphic sarcoma

Focal squamoid component

Focal squamoid component

p40+ / SOX10- squamoid component

p40+ squamoid component
Focal SOX10 staining

Nonspecific CD117 staining

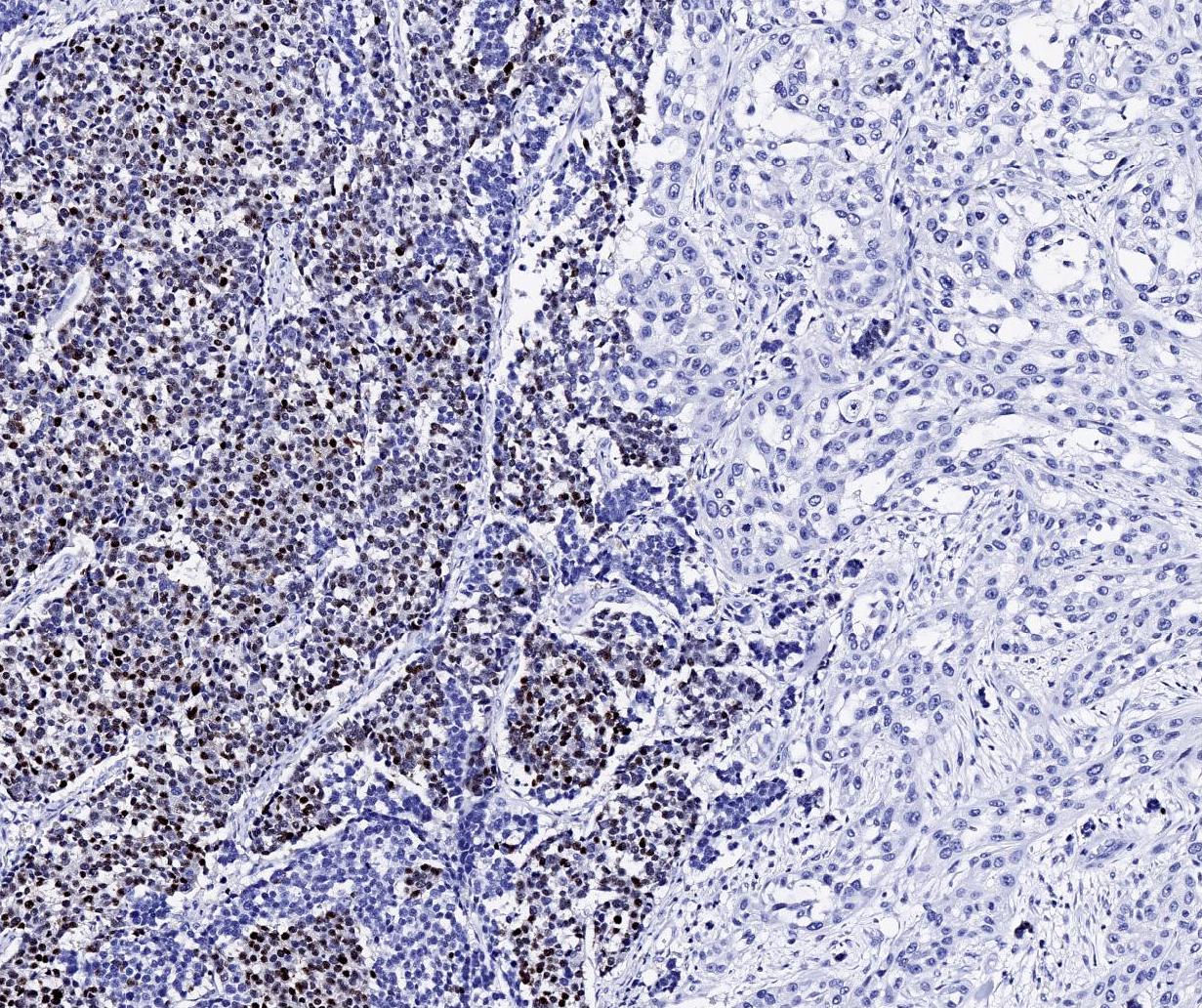
High proliferative index

Diffuse positive p53

AE1 / AE3 + sarcomatoid component
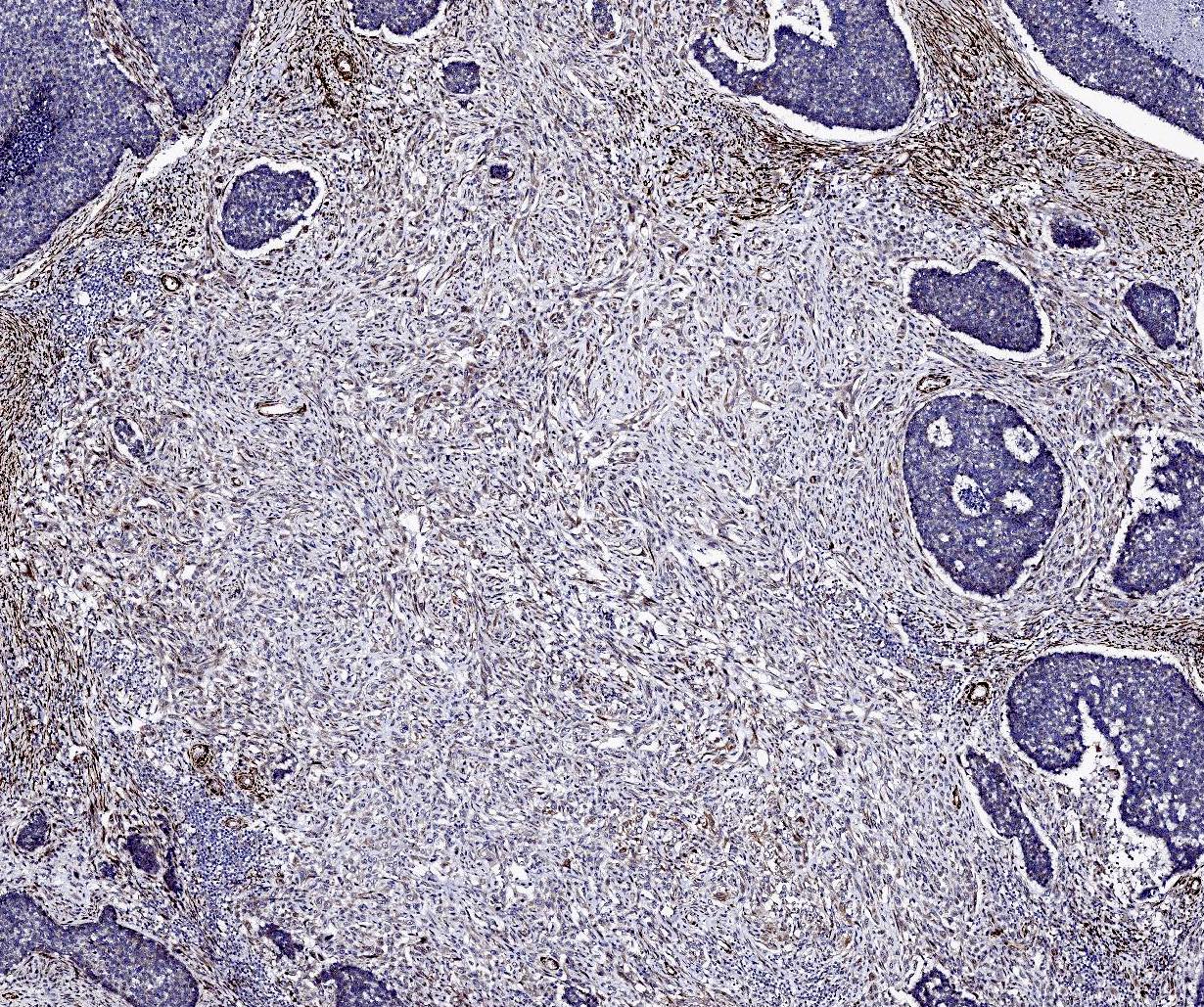
Calponin weak positive

Variably increased p53 staining

Myoepithelial cells in PA
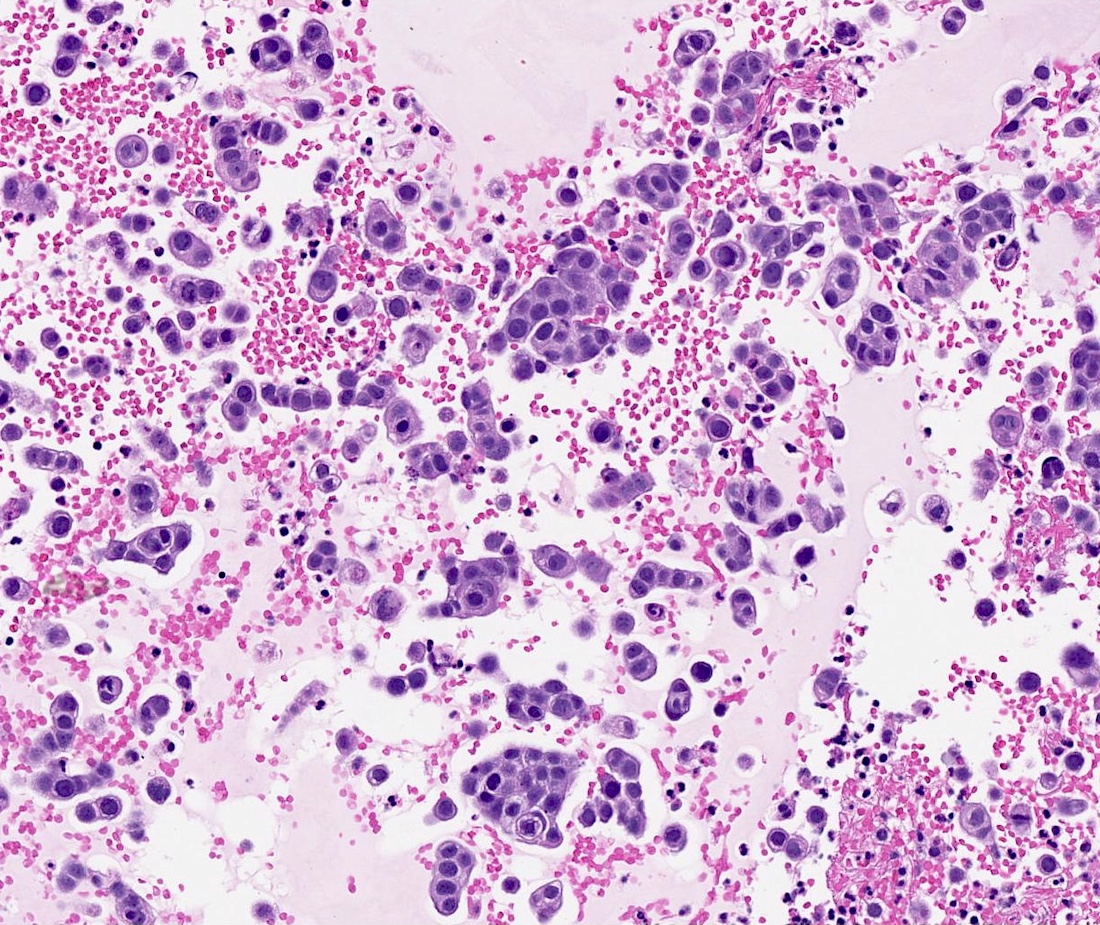
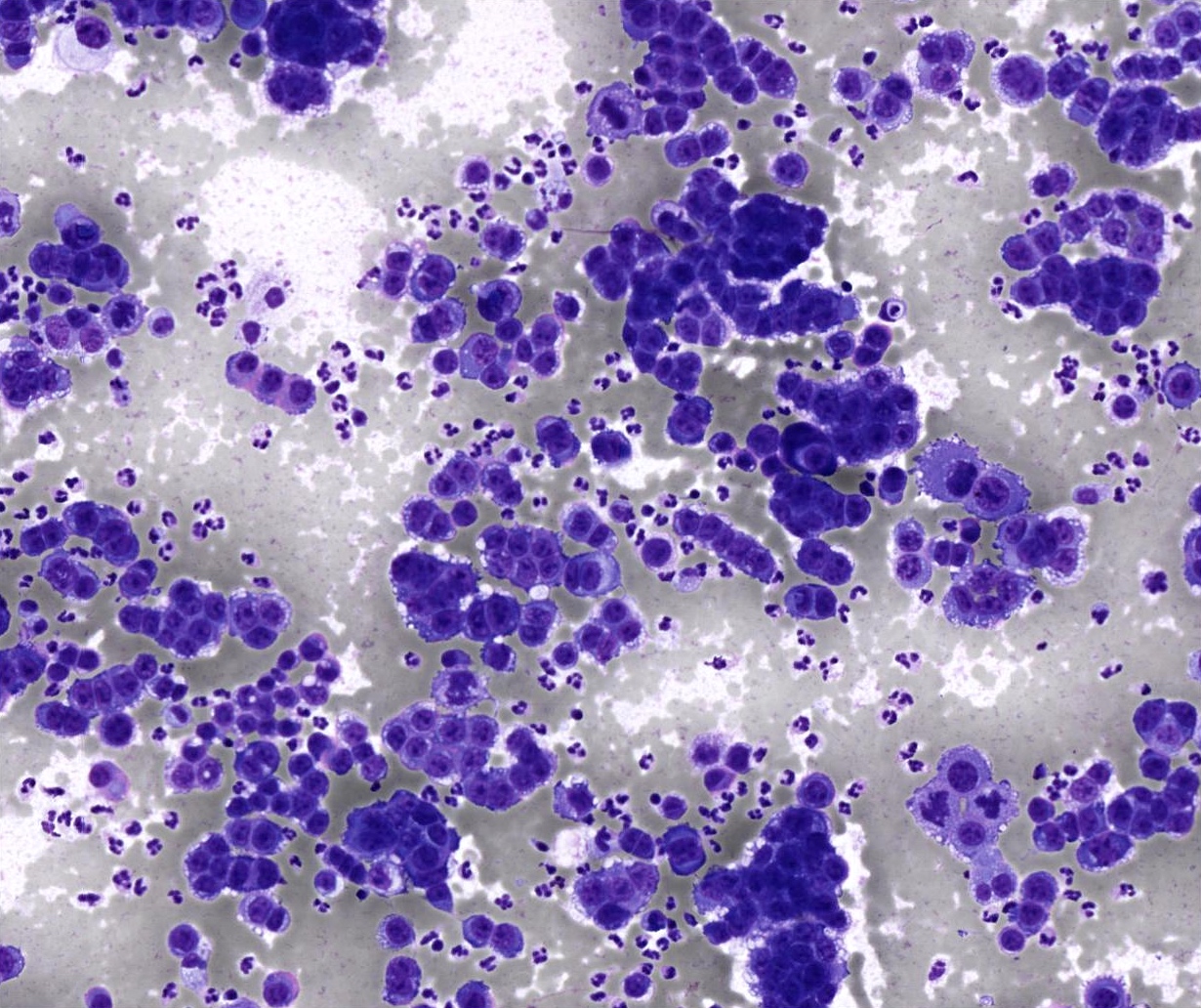
- Scattered fragments of large epithelial cells
- Epithelial cells have abundant cytoplasm; enlarged, pleomorphic, hyperchromatic nuclei and prominent nucleoli
- Epithelial component can show squamoid features
- Epithelial cells arranged in pseudoacinar pattern entrapped in myxoid materials have been reported (Diagn Cytopathol 2009;37:680)
- Often show features of a high grade carcinoma without sarcomatous component
- When sarcomatous component is present, it may appear as spindle cells showing atypical nuclei and giant cells in a background of necrosis (J Pathol Transl Med 2018;52:136, Acta Cytol 1998;42:1027)
Contributed by Manish Mahadeorao Bundele, M.B.B.S., M.D.

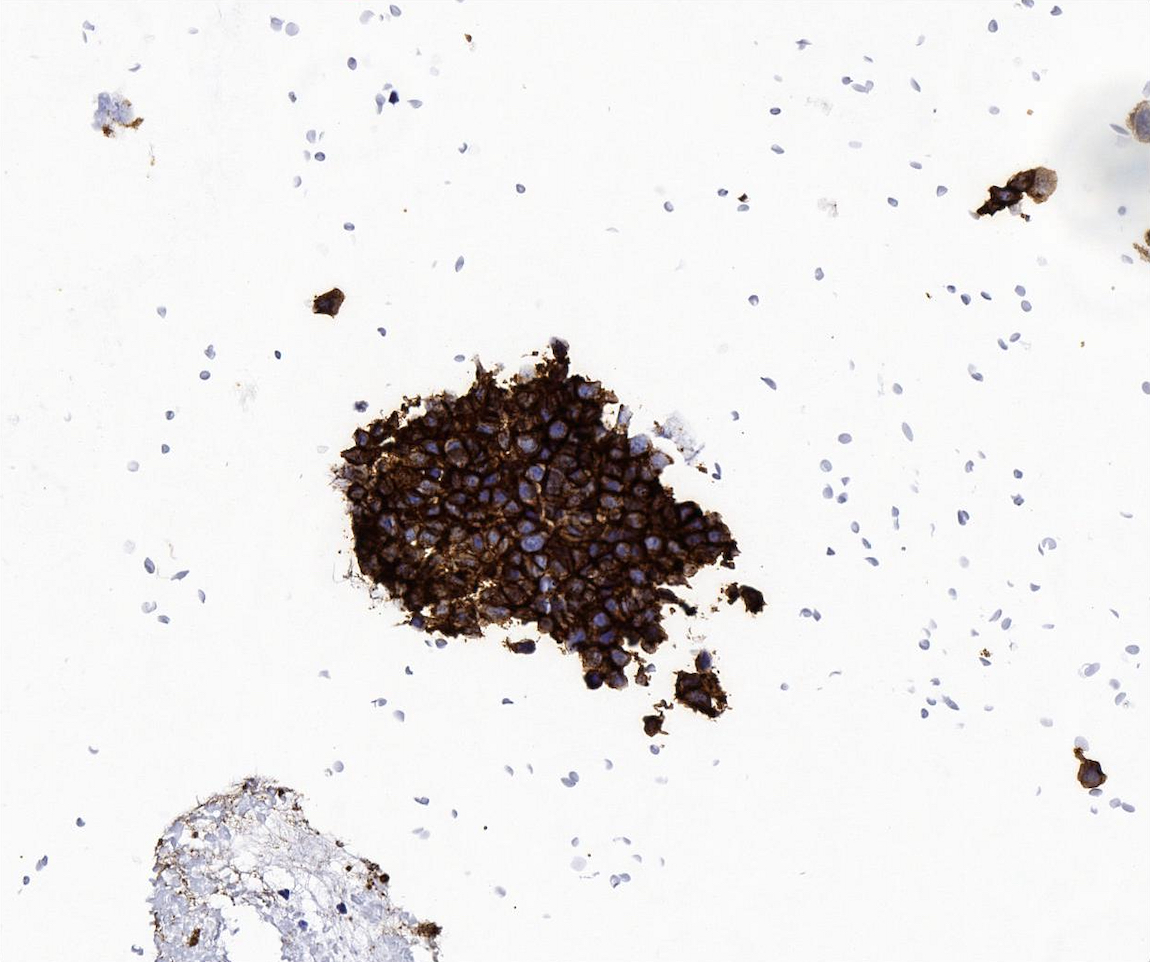
Cell block showing sheets of carcinoma cells
Cell block

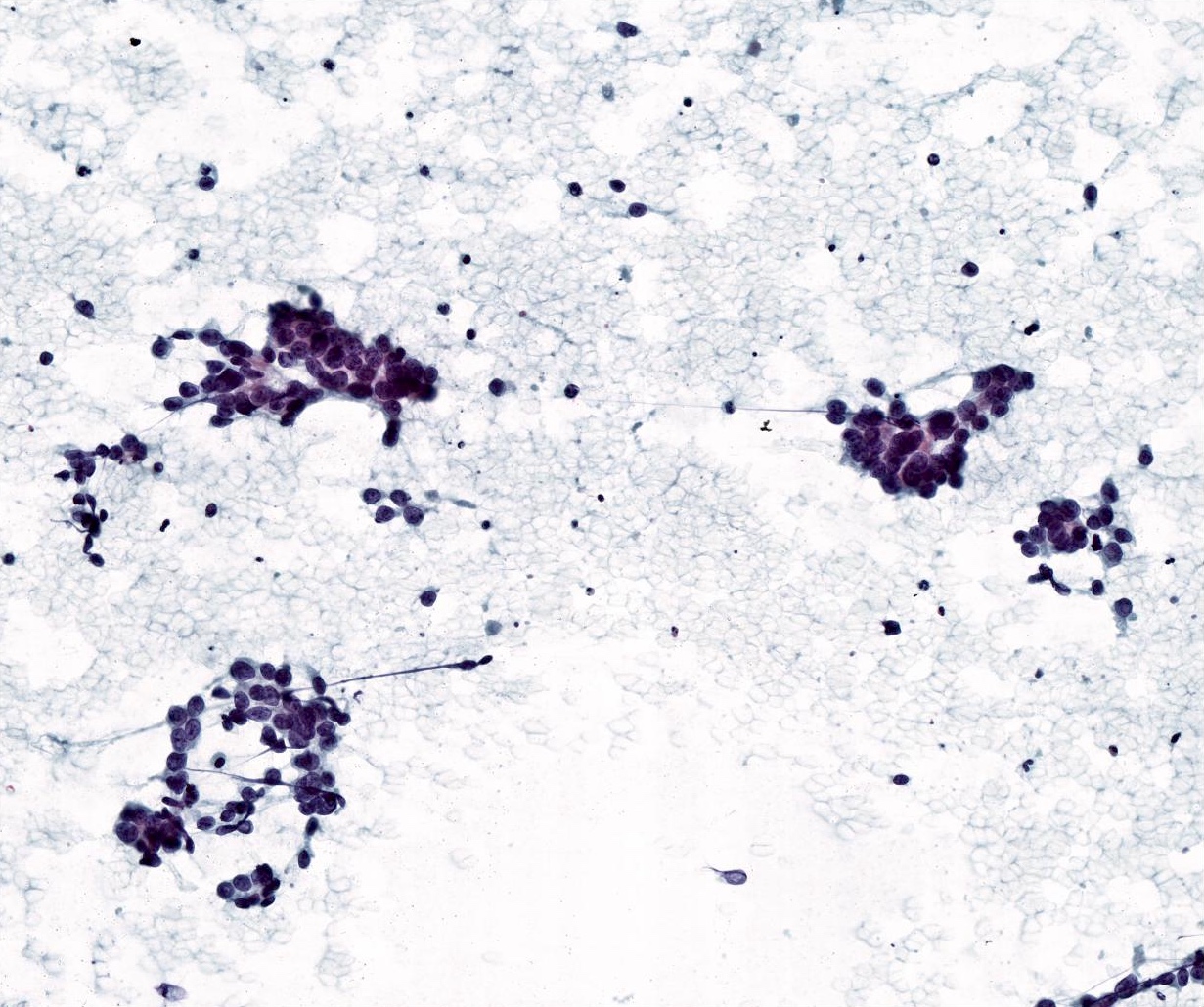
Parotid FNA (high grade carcinoma)


Parotid FNA (high grade carcinoma)

Pleural fluid metastasis
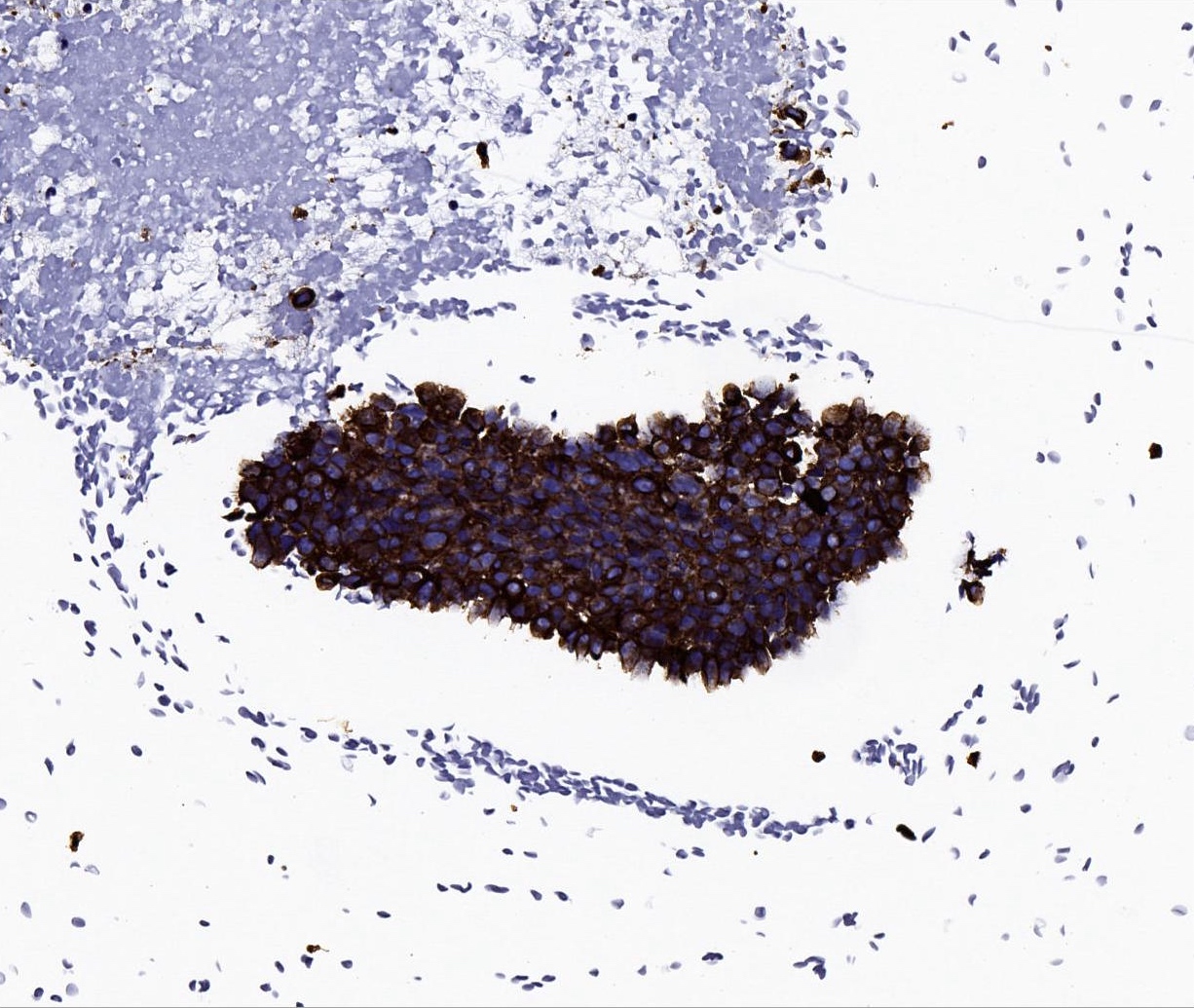
Cytokeratin positive
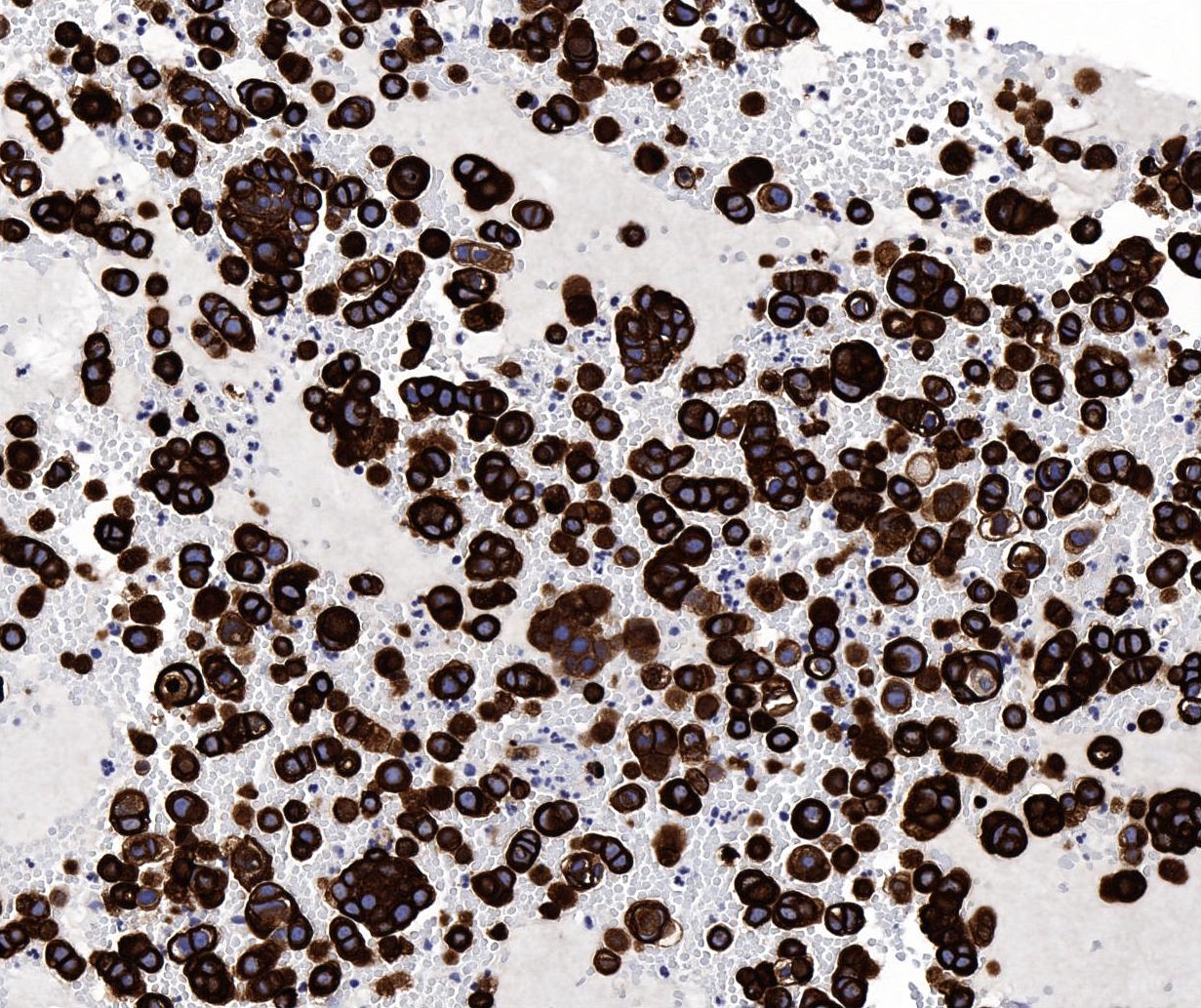
CK7

Nonspecific CD117 positive
- Immunohistochemistry depends on the classification of the malignant components
- Carcinomatous component
- Cytokeratin AE1 / AE3, CK7 positive
- Salivary duct carcinoma: AR, GATA3 and HER2 positive
- Myoepithelial carcinoma: myoepithelial markers positive such as smooth muscle actin, calponin, S100 / SOX10, p63 / p40, glial fibrillary acidic protein, vimentin
- Squamous cell carcinoma: p40 and CK5/6 positive
- Adenocarcinoma, NOS: SOX10 positive; indicates intercalated duct phenotype
- Sarcomatous component
- May have strong aberrant nuclear p53 expression in both carcinomatous and sarcomatous components (Head Neck Pathol 2013;7:163, Histopathology 2023;82:576)
- Often high Ki67 proliferation index
- Pleomorphic adenoma component: CAM5.2 in luminal component and myoepithelial cell markers p63 / p40, S100 / SOX10, smooth muscle actin, calponin, glial fibrillary acidic protein, vimentin in abluminal component
- PLAG1::CTNNB1, PLAG1::FGFR1, PLAG1::HNRNPA2B1 and HMGA2::WIF1 fusions have been reported (Histopathology 2023;82:576)
- Left parotid, parotidectomy:
- Carcinosarcoma (see comment)
- Comment: The biphasic tumor features both malignant epithelial (undifferentiated carcinoma) and sarcomatous (chondrosarcoma) components. Focally, there is a sclerotic area with myoepithelial cells, which could be suggestive of residual pleomorphic adenoma component.
- Carcinoma ex pleomorphic adenoma:
- Absence of sarcomatous component
- Rarely > 60 mm (Histopathology 2023;82:576)
- Intraductal intracapsular carcinoma can be seen
- Pleomorphic adenoma:
- Lack of invasive features, completely encapsulated
- Absence of carcinomatous and sarcomatous areas
- Salivary carcinoma with sarcomatoid differentiation:
- Generally smaller in size (< 30 mm) (Histopathology 2023;82:576)
- Very rare heterologous differentiation
- No pleomorphic adenoma component
- Spindle cell squamous cell carcinoma:
- Absence of heterologous differentiation
- Absence of residual / sclerotic pleomorphic adenoma
- Biphasic synovial sarcoma:
- Most cases in adolescents and young adults
- Monomorphic blue spindle cell sarcoma showing variable epithelial differentiation
- Diffuse and strong nuclear immunostaining for TLE1
- Demonstration of specific SS18::SSX1 / SS18::SSX2 / SS18::SSX4 gene fusion
- Sarcoma, primary or metastatic:
- Absence of carcinomatous and pleomorphic adenoma component
- Clinicopathological correlation
A 68 year old man who has a history of longstanding right parotid mass presented with a rapidly enlarging mass of the right parotid. A radical resection is performed. What is the diagnosis?
- Carcinoma ex pleomorphic adenoma
- Carcinosarcoma
- Pleomorphic adenoma
- Spindle cell squamous carcinoma
Comment Here
Reference: Carcinosarcoma
- It is a low grade indolent salivary gland malignancy
- Most common sarcomatous component is chondrosarcoma
- No necrosis and hemorrhage is seen
- There is no association with pleomorphic adenoma
Comment Here
Reference: Carcinosarcoma

