
Prostate gland & seminal vesicles
Squamous carcinomas
Squamous cell carcinoma
Authors: Kenneth A. Iczkowski, M.D., Komal Arora, M.D.
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 18 February 2019
Last staff update: 5 April 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma


Table of Contents
Definition / general | Essential features | Epidemiology | Pathophysiology | Clinical features | Adenosquamous carcinoma | Laboratory | Radiology images | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Iczkowski KA. Squamous cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostatesquamous.html. Accessed April 2nd, 2025.
Definition / general
- Extremely rare; incidence is < 0.6% of all prostate cancers with ~70 cases reported (Rare Tumors 2010;2:e47, Am J Surg Pathol 2004;28:651)
- Most are accompanied by concomitant adenocarcinoma (adenosquamous), generally high grade; some are purely squamous (Am J Surg Pathol 2004;28:651, Case Reports in Clinical Pathology 2016;3:60)
Essential features
- Criteria for diagnosis of pure primary squamous cell carcinoma of the prostate:
- Unequivocal features of malignancy
- Definitive squamous differentiation
- Lack of admixed conventional carcinoma component (would be adenosquamous) (Rare Tumors 2010;2:e47)
- No squamous cell carcinoma elsewhere (Mod Pathol 2004;17:316)
Epidemiology
- Most over age 70 (Cent European J Urol 2014;67:26, Rare Tumors 2010;2:e47, Am J Surg Pathol 2004;28:651)
- In 35/66 cases (over 50%) it arises in the settings of previous radiation or hormonal treatment for prostatic adenocarcinoma (Diagn Pathol 2011;6:46)
Pathophysiology
- Possible origin (J Clin Pathol 1988;41:1288):
- Purely prostatic with transformation of adenocarcinoma
- Collision tumor
- Derived from pluripotent stem cells
- Clonal evolution of adenocarcinoma under pressure from therapy
- After estrogen therapy, glutamine therapy, radiation seed implantation (Prostate Cancer and Prostatic Diseases 2000;3:53)
- Squamous differentiation of a prostatic urethral primary tumor
Clinical features
- Early metastasis to liver, bone and lungs (Rare Tumors 2010;2:e47)
- Does not respond to hormone therapy (Radiat Oncol 2007;2:15)
- Median survival 14 months (Cent European J Urol 2014;67:26)
Adenosquamous carcinoma
- Incidence is < 0.6% of all prostate cancers
- Have normal serum PSA and PSAP levels
- Originates from the periurethral glands or prostatic acinar basal cells
- Either de novo or postradiation or hormonal therapy for ordinary adenocarcinoma
- Micro description: both glandular (acinar) and squamous components
- Negative stains: PSA / PAP
- References: Am J Surg Pathol 1987;11:403, Hum Pathol 1995;26:123, Hum Pathol 1984;15:87BJU Int 2008;102:1369
Laboratory
- Can have normal serum PSA and PSAP (Clin Genitourin Cancer 2014;12:e29)
Radiology images
Contributed by Kenneth A. Iczkowski, M.D.

T2 weighted MRI
Case reports
- 55 year old man adenosquamous carcinoma of the prostate (Urology 1999;53:832)
- 57 years old primary squamous cell carcinoma of the prostate (Future Sci OA 2015;1:FSO18)
- 62 year old man with mixed adenocarcinoma, sarcomatoid carcinoma and adenosquamous carcinoma of the prostate (Oncol Lett. 2014 Nov;8(5):2325)
- 65 year old man with squamous cell carcinoma of the prostate following treatment with an LHRH agonist (Cent European J Urol 2014;67:26)
- 67 year old man concomitant adenocarcinoma in the absence of prior androgen deprivation therapy (Case Reports in Clinical Pathology 2016;3:60)
- 73 year old man in which docetaxel therapy was effective (Hinyokika Kiyo 2016;62:259)
- 77 year old man with pure squamous cell carcinoma involving the prostate and urinary bladder (Diagn Pathol 2011;6:46)
- Primary adenosquamous carcinoma of the prostate (Clin Genitourin Cancer 2014;12:e29)
- Long term survival after combined chemoradiation (Radiat Oncol 2007;2:15)
Treatment
- Long term survival has been reported after combined chemoradiation (Cent European J Urol 2014;67:26)
Gross description
- Tends to occur more in transition zone / periurethral (Rare Tumors 2010;2:e47)
Microscopic (histologic) description
- Pure tumors exhibit infiltrating nests, strands and sheets of polygonal cells with nuclear atypia
- Squamous differentiation is manifested as individual cell keratinization, intercellular bridges or keratin pearl formation
Microscopic (histologic) images
Contributed by Kenneth A. Iczkowski, M.D.
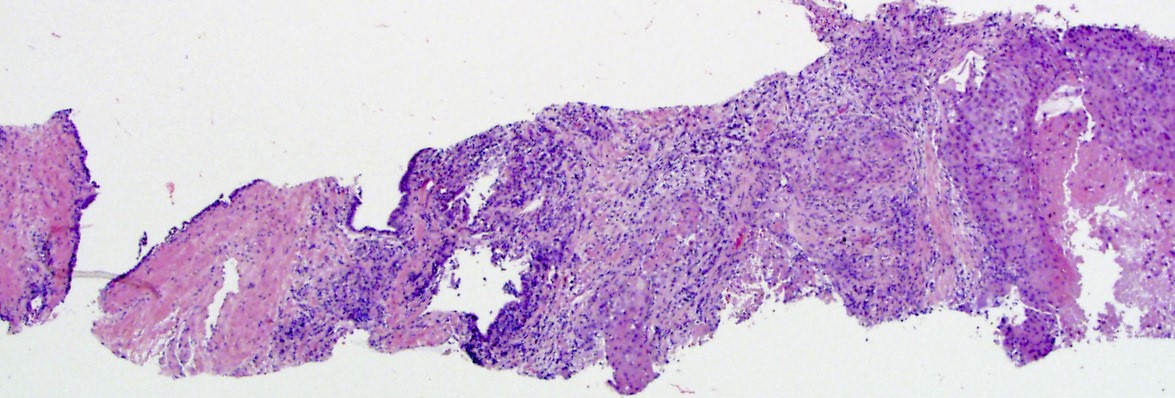
Needle biopsy
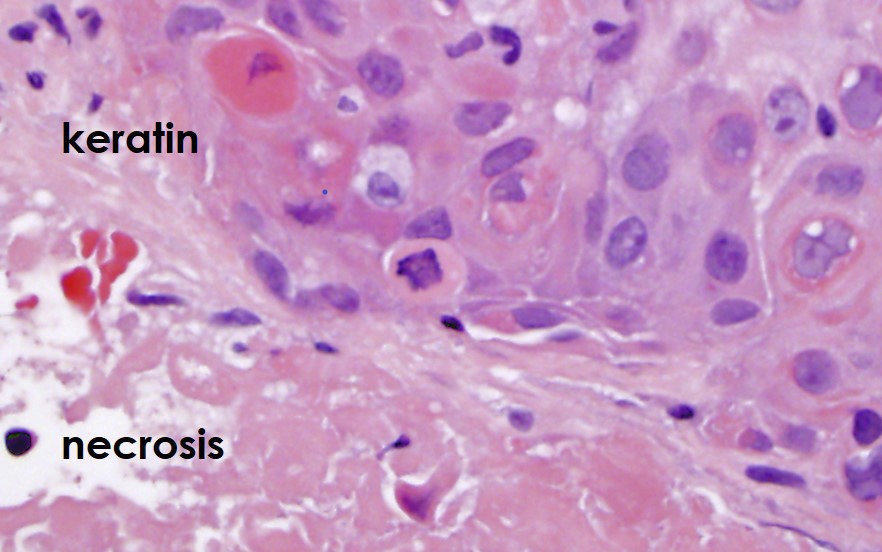
Keratinization with necrosis
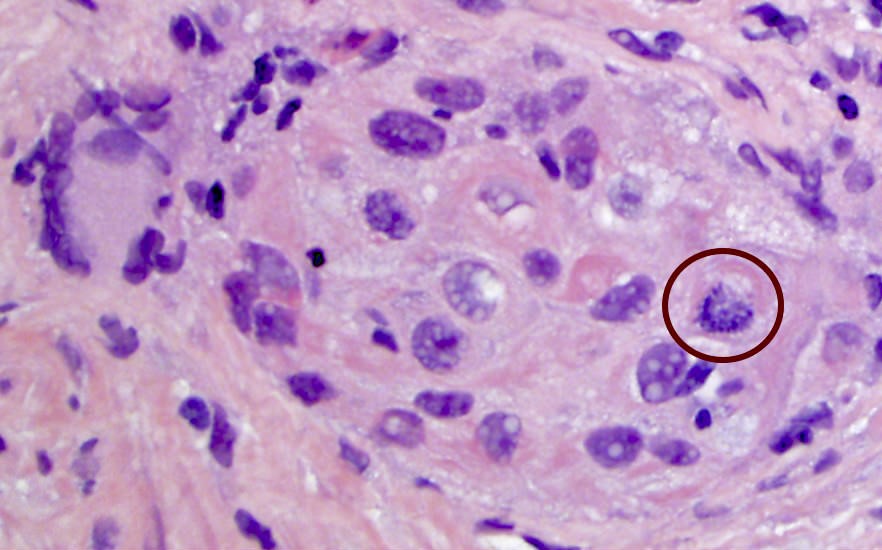
Multinucleation
Images hosted on other servers:


Squamous cell carcinoma
Positive stains
- Cytokeratin 34βE12, AE3 (Am J Surg Pathol 2004;28:651, Prostate Cancer and Prostatic Diseases 2000;3:53, Clin Genitourin Cancer 2014;12:e29)
- p53 strong positive consistent with mutation (Oncol Lett 2014;8:2325)
- AMACR may be expressed in adenosquamous areas (maintains an immunohistochemical profile similar to adenocarcinoma) (Diagn Pathol 2011;6:46, Urology 1999;53:832)
Negative stains
- Prostate specific antigen and prostatic acid phosphatase, P501S
- Cytokeratin CAM5.2 (low molecular weight)
- Uroplakin II, S100 protein, CDX2
Differential diagnosis
- Urothelial carcinoma
- Urothelial carcinoma with squamous differentiation
- May be difficult to impossible to differentiate
- Will not have adenosquamous areas
- Squamous carcinoma of other origins such as penis, bladder or anorectal
- Requires clinical and radiologic correlation
- Will not have adenosquamous areas
- Squamous metaplasia
- Can be seen around infarcts within the prostate
- Lacks overt pleomorphism and atypical mitotic figures; does not form a mass
Board review style question #1
What is a finding that may rule out primary pure squamous cell carcinoma of the prostate?
- Negative for low molecular weight cytokeratin
- Negative for prostate specific antigen
- Presence of keratin
- Presence of squamous cell carcinoma elsewhere
Board review style answer #1
Board review style question #2
Which of the following is true about squamous cell carcinoma of the prostate?
- Does not originate adjacent to coexisting squamous metaplasia
- More likely to occur as a focus separate from adenocarcinoma, rather than intermixed and merging with adenocarcinoma
- More often occurs following radiotherapy or antiandrogen therapy than in the absence of those prior therapies
- Serum PSA elevation is useful for diagnosis of the pure form of squamous cell carcinoma
Board review style answer #2
C. More often occurs following radiotherapy or antiandrogen therapy than in the absence of those prior therapies
Comment Here
Reference: Squamous cell carcinoma
Comment Here
Reference: Squamous cell carcinoma
