
Prostate gland & seminal vesicles
Nonneoplastic
Sclerosing adenosis
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.
Last author update: 24 September 2024
Last staff update: 24 September 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Sclerosing adenosis


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: van der Kwast T. Sclerosing adenosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostatesclerosingadenosis.html. Accessed April 1st, 2025.
Definition / general
- Sclerosing adenosis is a circumscribed benign lesion located in the transition zone of the prostate with distinct histopathological and immunostaining features
Essential features
- Uncommon incidental benign finding in the transition zone of the prostate
- Well demarcated unencapsulated proliferation of glandular tissue
- Mixture of variably sized glands and hypercellular spindle cellular stroma with myxoid component
Terminology
- (Pseudo)adenomatoid tumor (not recommended)
- Fibroepithelial nodule (not recommended)
ICD coding
- ICD-10: N40.2 - nodular prostate without lower urinary tract symptoms
Epidemiology
- Incidental finding in transurethral resections for urinary outflow obstruction or in (cysto)prostatectomy specimens of patients with bladder or prostate cancer
- Rarely in prostate biopsies of the transition zone (Arch Pathol Lab Med 2003;127:e14)
- Identified in 2% of a series of 100 whole embedded prostate tissues (Am J Surg Pathol 1992;16:383, Am J Surg Pathol 1991;15:660)
- Multifocal in ~30% of cases (Am J Surg Pathol 1992;16:383)
Sites
- Transition zone of the prostate
Pathophysiology
- Myoepithelial metaplasia of basal cells as witnessed by coexpression of smooth muscle actin and high molecular weight cytokeratin (Am J Surg Pathol 1992;16:383)
Etiology
- Unknown
Diagnosis
- Histologic examination of biopsy or resection specimens
Prognostic factors
- Benign lesion
- No known association with prostate malignancy
Case reports
- 65, 72 and 78 year old men with sclerosing adenosis of the prostate with symptoms of urinary tract obstruction (Histopathology 1992;20:505)
- 66 year old man biopsied for elevated prostate specific antigen (PSA) and 70 year old man with urinary outflow obstruction (Arch Pathol Lab Med 2003;127:e14)
- 83 year old Japanese man with transurethral resection of the prostate showing sclerosing adenosis in combination with basal cell hyperplasia (Med Mol Morphol 2010;43:226)
Treatment
- No treatment required
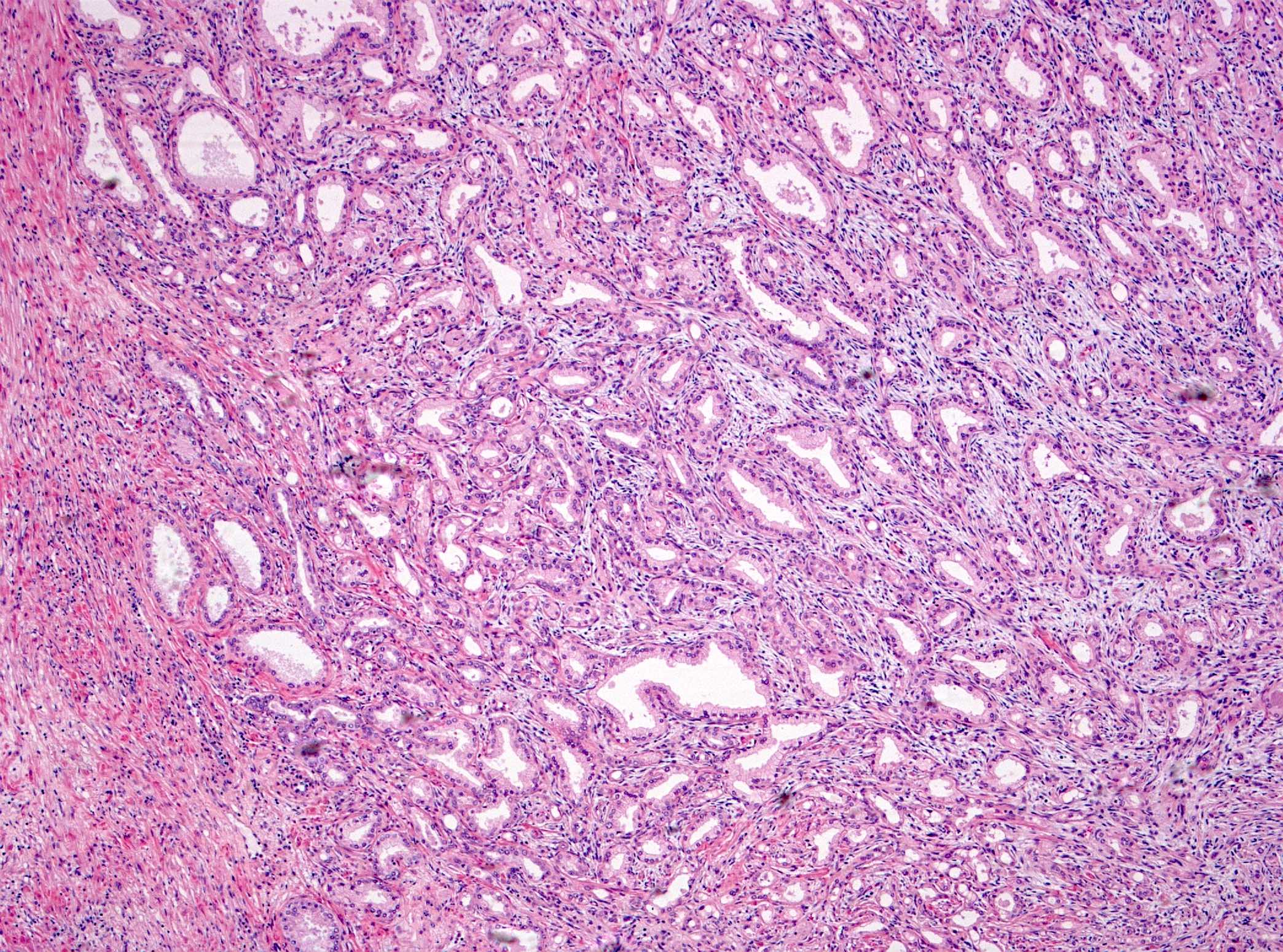
Microscopic (histologic) description
- Nonencapsulated nodular circumscribed lesion with smooth contours; size range: 1.5 - 11.1 mm (Am J Surg Pathol 1992;16:383)
- Lobular small acinar proliferation with clear (pale) to eosinophilic cytoplasm; ranging from well formed acini to poorly formed glands and single cells
- No nuclear pleomorphism
- Areas of prominent spindle cellular and myxoid stroma
- Some acini and epithelial cell nests / clusters surrounded by thickened hyalinized stroma, resembling basement membrane
- Basal cells surrounding the acini may be focally prominent and hyperplastic
- In rare cases, glandular cells may display prominent nucleoli and sporadic mitosis (Histopathology 2010;56:627)
Microscopic (histologic) images
Contributed by Theodorus van der Kwast, M.D., Ph.D. and Liang Cheng, M.D.

Demarcated glandular nodule

Glandular proliferation

Myxoid area

Spindle cellular stroma

Eosinophilic basement membranes

Variably sized glands

Conspicuous nucleoli

Stromogenic glandular lesion

Smooth muscle actin

S100
Positive stains
- Smooth muscle actin in basal cells (Am J Surg Pathol 1992;16:383)
- Calponin in basal cells (World J Clin Cases 2022;10:6009)
- High molecular weight cytokeratin in basal cells (Histopathology 2010;56:627)
- S100, p63 in basal cells
- PSA in acinar luminal cells (Histopathology 2010;56:627)
- Androgen receptor in acinar luminal cells
- AMACR (P504S) in acinar luminal cells (weak to moderate staining in 60% of cases) (World J Clin Cases 2022;10:6009)
Electron microscopy description
- Large aggregates of cytoplasmic microfilaments with multiple dense bodies in the basal cells surrounding the acinar luminal cell (Am J Surg Pathol 1992;16:383, Histopathology 1992;20:505)
Sample pathology report
- Prostate, transurethral resection, weight 25 grams:
- Nodular hyperplasia
- Incidental finding: sclerosing adenosis
Differential diagnosis
- Acinar adenocarcinoma:
- No double layer of basal cells
- Prominent (inclusion-like) nucleoli are commonly present
- Absence of the cellular / myxoid stroma that is characteristic of sclerosing adenosis
- Negative for basal cell or myoepithelial markers such as high molecular weight cytokeratin, S100 or smooth muscle actin
- Adenosis (atypical adenomatous hyperplasia):
- Scattered, not continuous basal cell lining
- Absence of the spindle cellular / myxoid stroma that is characteristic of sclerosing adenosis
- Negative for myoepithelial markers such as S100 or smooth muscle actin
Board review style question #1
What is the most helpful microscopic feature distinguishing sclerosing adenosis from adenocarcinoma in a prostate biopsy?
- Absence of prominent nucleoli
- Multifocality
- Size of the glandular structures
- Spindle cellular stroma with myxoid areas
Board review style answer #1
D. Spindle cellular stroma with myxoid areas. Presence of bland evenly distributed spindle cells and myxoid areas are the distinguishing features most suggestive of sclerosing adenosis. Answer A is incorrect because very conspicuous nucleoli may be seen in atypical sclerosing adenosis. Answer B is incorrect because multifocality can occur both in adenocarcinoma and sclerosing adenosis. Answer C is incorrect because in both sclerosing adenosis and adenocarcinoma, the glandular size may vary considerably.
Comment Here
Reference: Sclerosing adenosis
Comment Here
Reference: Sclerosing adenosis
Board review style question #2
Which pair of immunomarkers are specific for sclerosing adenosis of the prostate?
- AMACR and p63
- Androgen receptor and MIB1
- S100 and calponin
- Smooth muscle actin and high molecular weight keratin
Board review style answer #2
C. S100 and calponin. Myoepithelial metaplasia is characteristic for sclerosing adenosis. Calponin and S100 are myoepithelial markers.
Answer A is incorrect because AMACR is expressed by other prostate lesions as well, such as adenocarcinoma, atrophy and high grade prostatic intraepithelial neoplasia (PIN). p63 is a ubiquitous basal cell marker and is expressed by several benign lesions of the prostate such as benign prostatic hyperplasia (BPH) and adenosis. Answer B is incorrect because androgen receptor is expressed by luminal cells of the prostate, including BPH and adenosis. Answer D is incorrect because although smooth muscle actin expression is specific for sclerosing adenosis, high molecular weight keratin is a ubiquitous basal cell marker, expressed in atrophy, BPH and adenosis.
Comment Here
Reference: Sclerosing adenosis
Comment Here
Reference: Sclerosing adenosis
