
Pleura & peritoneum
Pleura other tumors
Metastases
Author: Vaidehi Avadhani, M.D.

Last author update: 1 April 2014
Last staff update: 11 January 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Metastases pleura[TI]


Table of Contents
Definition / general | Sites | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology images | Case reports | Microscopic (histologic) images | Cytology description | Cytology images | Positive stainsCite this page: Avadhani V. Metastases. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pleurametastases.html. Accessed April 1st, 2025.
Definition / general
- Metastases to pleura are more common than primary tumors of pleura
Sites
- Most common primary pleural neoplasms originate from chest wall, mediastinum, lungs
- Lung cancer: most common type in pleural fluid is adenocarcinoma, followed by small cell neuroendocrine carcinoma; squamous cell carcinoma is rare
- Extrathoracic malignancy: most common primary carcinomas are breast, gastrointestinal tract and ovary
- Metastases: lung is most common primary site in men, breast in women (see table below)
- For lung, breast and ovarian metastases, 92% of pleural effusions are ipsilateral to primary lesion
Pathophysiology
- Adenocarcinoma of lung spreads to parietal pleura from visceral pleura along adhesions
- Pleural metastases from extrathoracic sites occur via hematogenous or lymphatic spread
- Malignant pleural effusions from breast occur via chest wall lymphatics or hepatic metastases, resulting in contralateral or bilateral effusions
Diagrams / tables
Images hosted on other servers:
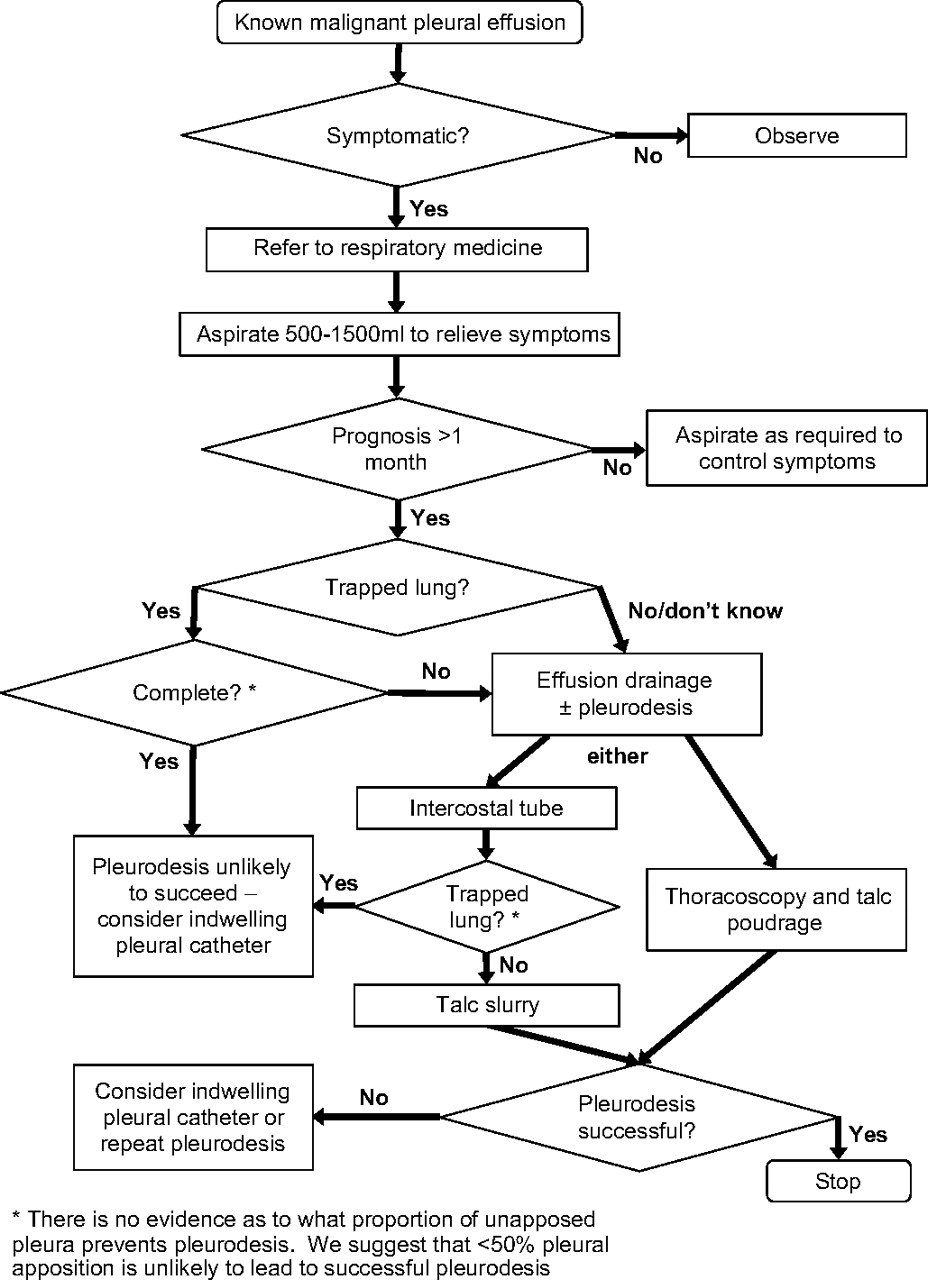
Management
algorithm for
malignant
pleural effusion

Primary tumor
site in patients
with malignant
pleural effusion

Diagnostically
useful pleural fluid
characteristics
Clinical features
- Most malignant effusions are symptomatic; dyspnea is most common symptom and may be associated with chest pain and cough
Diagnosis
- Cytologic examination of pleural fluid leads to diagnosis in 2/3 of malignant pleural effusions
- Three specimen are recommended if clinical suspicion of metastases is high
- Note: British Thoracic Society guidelines do not recommend more than 2 specimens (British Thoracic Society: BTS Pleural Disease Guideline 2010 [Accessed 11 January 2021])
Laboratory
- Recommended tests for all sampled pleural effusions:
- Biochemistry: LDH and protein (send pleural fluid and blood simultaneously so that Light's criteria can be applied, Thorax 2010;65:ii4)
- Microscopy and culture
- Cytological examination
- Differential count
Radiology images
Images hosted on other servers:

PET: pancreatic metastases

EUS view
Case reports
- 64 year old man with late multiple pleural metastases of renal cell carcinoma (Intern Med 2013;52:2475)
- 76 year old woman with early gastric cancer with solitary metastasis to pleura (Clin Endosc 2013;46:666)
- 78 year old man with pleural metastases from papillary thyroid carcinoma mimicking mesothelioma (Intern Med 2014;53:163)
Microscopic (histologic) images
Images hosted on other servers:

Metastatic breast carcinoma to pleura
Cytology description
- Cytology helpful since associated pleural effusion contains tumor cells
Cytology images
Images hosted on other servers:

Diff-Quik
Positive stains
- Commonly used IHC markers: CK AE1 / AE3, CK7, CK20, mCEA, BerEP4, calretinin, PAX2, PAX8 (depending on history and differential diagnosis)
- Cytochemical stains can also be used: mucicarmine, PAS, D-PAS, Alcian blue
