

Placenta
Nonneoplastic placental conditions and abnormalities
Placental findings in specific conditions
Intrauterine fetal demise
Author: Theonia K. Boyd, M.D.
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.

Last author update: 27 April 2023
Last staff update: 27 April 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Intrauterine fetal demise


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Boyd TK. Intrauterine fetal demise. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/placentafetaldeath.html. Accessed December 26th, 2024.
Definition / general
- Intrauterine fetal demise is the phrase used for fetal death in utero after the twentieth completed week of pregnancy; prior to that, miscarriage or spontaneous abortion is usually applied to circumstances of spontaneous fetal loss
Essential features
- As pregnancy progresses, the causes of intrauterine fetal demise are increasingly likely to be extrinsic to the fetus
- With fetal death, the placental fetal vascular tree begins to involute globally and in a temporally homogeneous manner
- Fetal death due to fetal vascular malperfusion may be difficult to distinguish from passive postmortem fetal vascular involution, as both involve loss of placental fetal vascular integrity
- Scant maternal inflammation within the extraplacental membranes may be due to nonviable antigen exposure rather than antemortem amniotic fluid infection
- Stillbirth changes in umbilical and chorionic vasculature may mimic fetal vasculitis
Terminology
- Before 20 completed gestation weeks: miscarriage, spontaneous abortion
- After 20 completed gestation weeks: fetal death, intrauterine fetal demise (IUFD), stillbirth
Epidemiology
- Intrauterine fetal demise can occur during maternal reproductive years or with assisted reproduction beyond menses
- Stillbirth rates are highest in countries with limited health care resources
- Stillbirth risk increases with advanced maternal age, high body mass index, low socioeconomic status, chronic illness, ingested toxins (smoking, alcohol, illicit substances), multifetal gestations
Sites
- Normal: intrauterine
- Abnormal: tubal, abdominopelvic
Pathophysiology
- Intrauterine demise occurs when fetal cardiac output ceases, regardless of the inciting cause
Etiology
- Sites of origin
- Maternal: systemic disorders - hypertensive, diabetes, auto and other immune mediated, endocrine, hypercoagulability, malignancy
- Uterine: abnormal uterine anatomy, previable delivery
- Placental (not secondary to another primary underlying disorder): fetal vascular malperfusion (e.g., abnormal cord insertion, hypercoiling), fetal maternal hemorrhage, neoplasia (massive chorangioma, placental choriocarcinoma), multifetal complications, amniotic band umbilical cord constriction
- Fetal: cardiac anomalies, multifetal gestation, mass lesions, neoplasia, genetic
- Infectious: ascending, hematogenous, direct inoculation (e.g., amniocentesis)
- Environmental / toxic: mechanical trauma, toxic exposure / ingestion (e.g., illicit drugs)
Clinical features
- Silent stillbirth: maternal decreased fetal movement
- Clinically apparent: uterine rigidity with or without vaginal bleeding due to placental abruption, fever, foul vaginal discharge
Diagnosis
- Maternal: absent fetal heart tones on external fetal monitor, absent Doppler waveforms, absent cardiac activity of ultrasound, previable delivery
- Fetal: previable delivery, Apgar scores 0 / 0 / 0 at delivery
Laboratory
- Fetal maternal hemorrhage: positive Kleihauer-Betke
- Pre and eclampsia: severe maternal hypertension, proteinuria, elevated liver enzymes, seizures, edema, headache, visual disturbances
- Infection: positive cultures (bacterial, fungal), positive serology (viral, parasitic, autoimmune)
Radiology description
- Diagnosis: absent cardiac activity on ultrasound
- Ancillary information: evidence of causative process (e.g., placental abruption)
Prognostic factors
- Recurrence risk is highest for unmodifiable or unmodified maternal diseases, heritable genetic causes, repeated toxic exposure
Treatment
- Maternal
- Treatment of potential sequelae associated with stillbirth (e.g., infection, trauma)
- For potential future reproduction, treat underlying disorder as applicable (e.g., diabetes, hypertension, cervical incompetence)
- Fetal
- Not applicable
Clinical images
Contributed by Theonia K. Boyd, M.D.
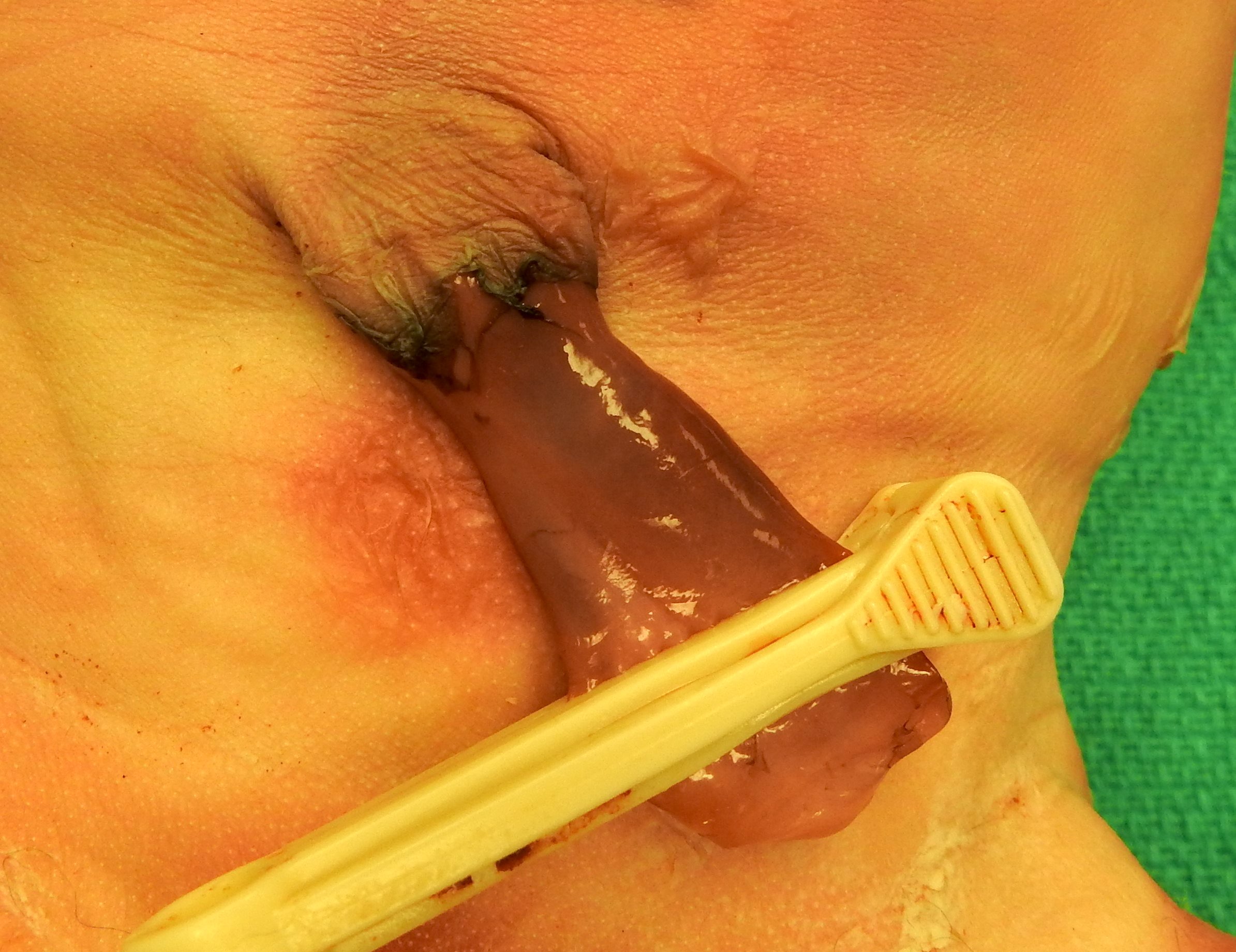
Postmortem umbilical cord discoloration
Gross description
- Nonspecific postmortem placental changes
- Umbilical cord: ruddy brown discoloration
- Extraplacental membranes: variable opacity, tan-brown discoloration
- Fetal surface: variable opacity, tan-brown discoloration
- Maternal surface: variably adherent blood clot without parenchymal compression
- Cut surface: no specific changes
- Selected specific changes
- Umbilical cord
- Ectatic dilated venous thrombosis
- Green / tan meconium discoloration
- Abnormal cord insertion, flat umbilical cord with nuchal / body wrapping
- Extraplacental membranes
- Green / tan meconium discoloration
- Tan-white chorioamnionitis discoloration
- Fetal surface
- Green / tan meconium discoloration
- Tan-white chorioamnionitis discoloration, chorionic vessel hypovolemia with fetal exsanguination
- Ectatic thromboses chorionic vessels with fetal vascular malperfusion
- Maternal surface
- Tightly adherent retroplacental blood with abruption with or without underlying parenchymal compression and with or without infarction
- Cut surface
- Pallor with placental hydrops or fetal exsanguination
- Rounded firm placental infarcts, variably red (recent) to white-tan (remote)
- Umbilical cord
Gross images
Contributed by Theonia K. Boyd, M.D.

Umbilical cord and fetal surface discoloration

Formalin fixed stillbirth cord
Microscopic (histologic) description
- Nonspecific postmortem placental changes
- Umbilical cord: umbilical myocyte elongation and pyknosis
- Extraplacental membranes: bland maternal neutrophil migration with or without karyorrhexis
- Fetal surface: chorionic myocyte elongation and pyknosis
- Maternal surface: necrotizing decidual acute / chronic inflammation, variable retroplacental blood without overlying placental infarction
- Cut surface
- Fetal
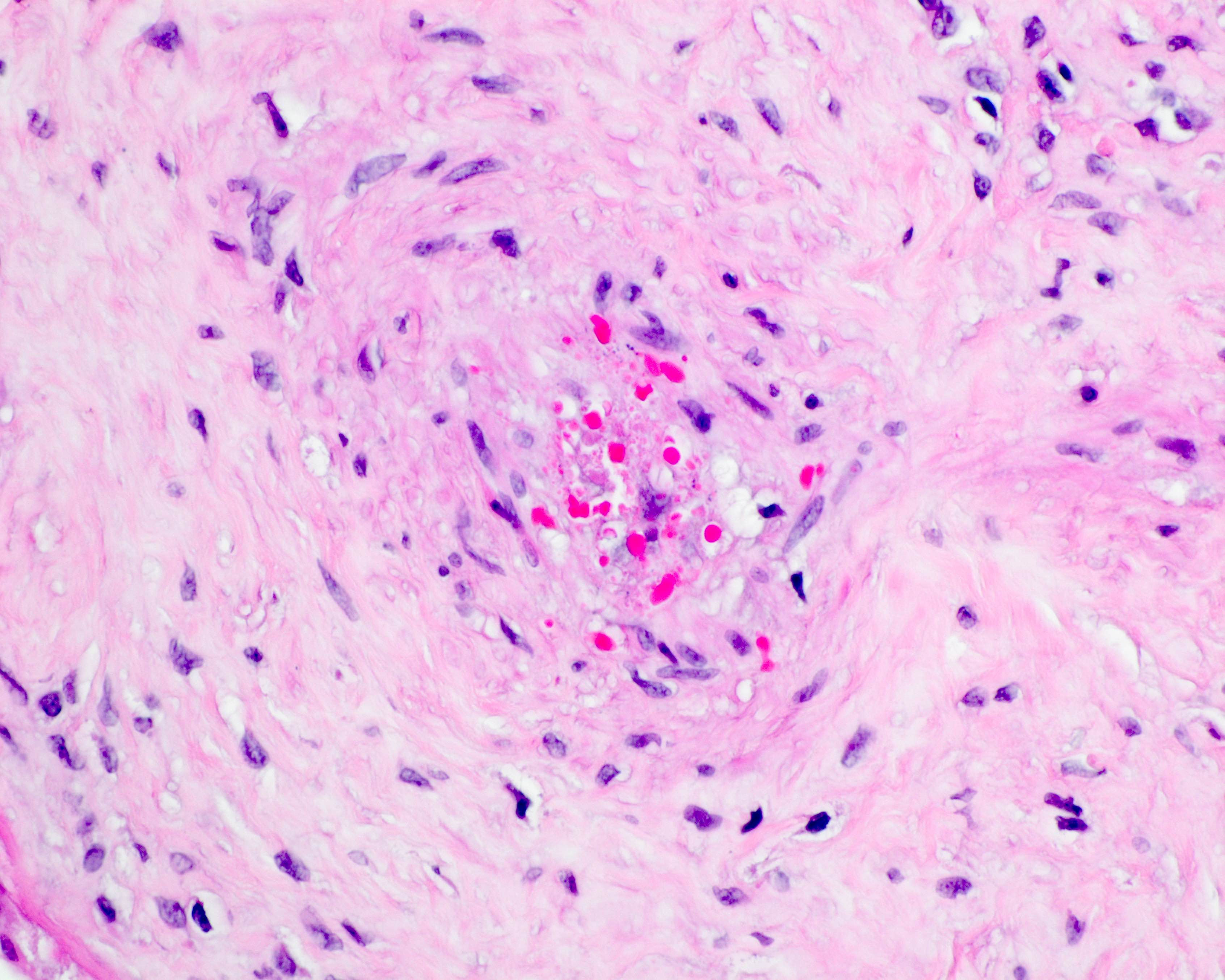
- Passive and global postmortem fetal vascular involution (progressively avascular villi and chorionic / stem vessel obliteration)
- Note: muscular vessels (e.g., umbilical, chorionic, stem) with fibrin thrombi are never postmortem
- Nucleated red blood cells with or without karyorrhexis
- With or without meconium macrophages in extraplacental membranes, chorionic plate, umbilical cord stroma
- Maternal: ischemic parenchymal changes with prolonged demise (increased syncytial knots, intervillous fibrin, parenchymal collapse)
- Fetal
- Selected specific changes
- Umbilical cord
- Vasculitis with or without perivasculitis with intrauterine infection or meconium discharge
- Meconium vascular necrosis with prolonged meconium exposure
- Nucleated fetal red blood cells with infection, hypoxia, diabetes
- Rarely umbilical thrombosis
- Extraplacental membranes
- Acute chorioamnionitis with intrauterine infection (with or without necrosis)
- Meconium macrophages with or without particulate entrapped meconium
- Decidual arteriopathy with hypertensive and autoimmune disorders
- Fetal surface
- Chorionic thrombosis with fetal vascular malperfusion
- Massive subchorionic hematoma, chorionic vasculitis with or without perivasculitis with intrauterine infection
- Chorionic meconium vascular necrosis
- Maternal surface
- Abruption with adherent retroplacental blood with or without overlying infarction, with or without basal intervillous extension and with or without intravillous hemorrhage
- Decidual arteriopathy
- Cut surface
- Fetal vascular malperfusion
- Clustered villous stromal vascular karyorrhesis or avascular villi
- Stem vessel thrombosis orobliteration)
- Maternal vascular malperfusion
- Increased syncytial knots with or without aggregated terminal villi
- Distal villous hypoplasia
- Multifocal and temporally heterogenous infarction
- Immune mediated
- Massive perivillous fibrin
- Noninfectious or infectious chronic villitis
- Fetal hypovolemia and villous edema with anemia and exsanguination
- Viral cytopathic effect, parasitic or spirochetal infection
- Intervillous microabscesses with Listeria
- Fetal intravascular bacteria with sepsis (rare)
- Fetal vascular malperfusion
- Umbilical cord
- Additional microscopic considerations
- Without autopsy: compare microscopic placental changes to estimated time of intrauterine demise as determined clinically
- With autopsy: compare microscopic placental changes by postmortem gross (skin maceration) and microscopic (visceral autolysis) changes to assist indiscriminating ante versus postmortem pathology
Microscopic (histologic) images
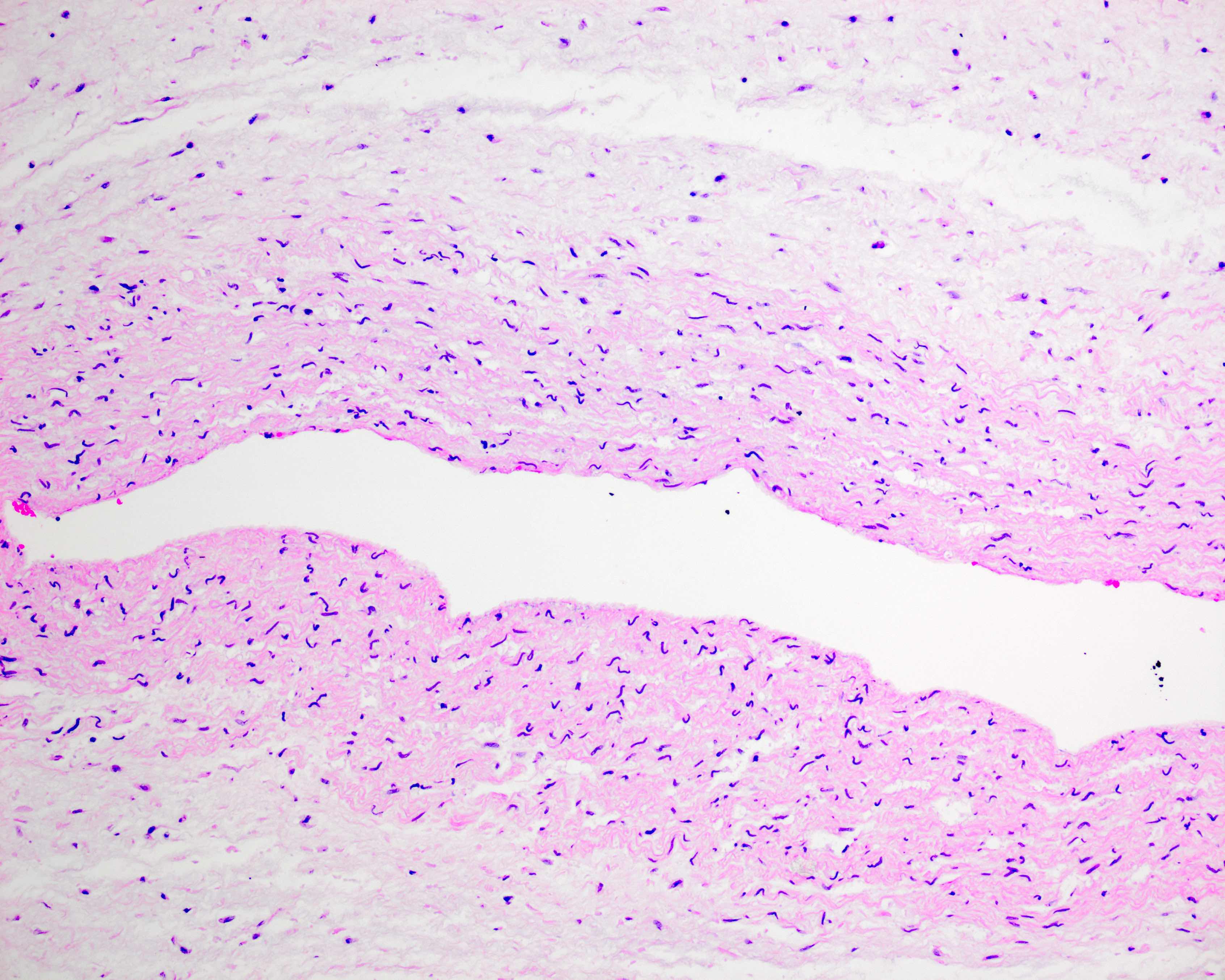
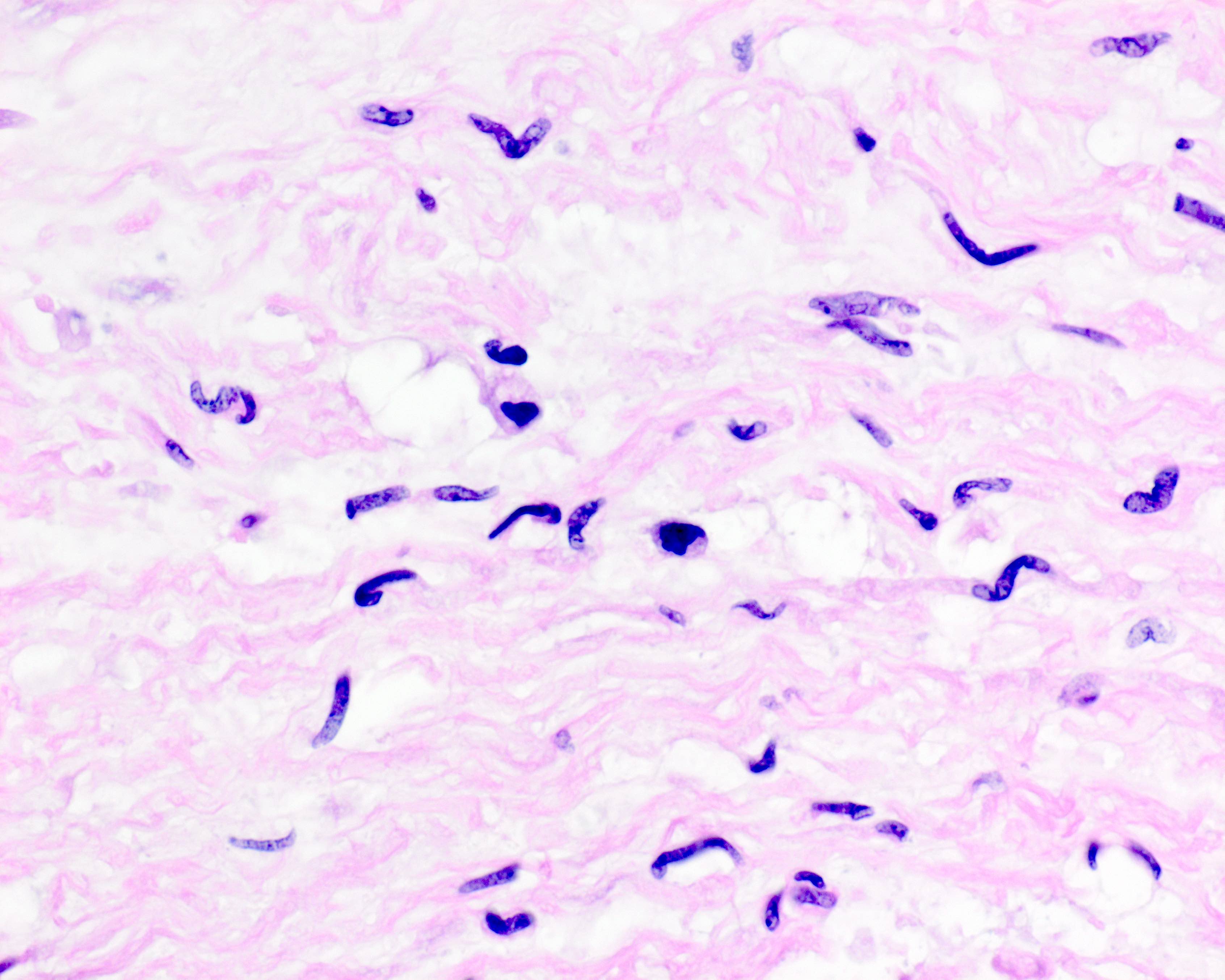
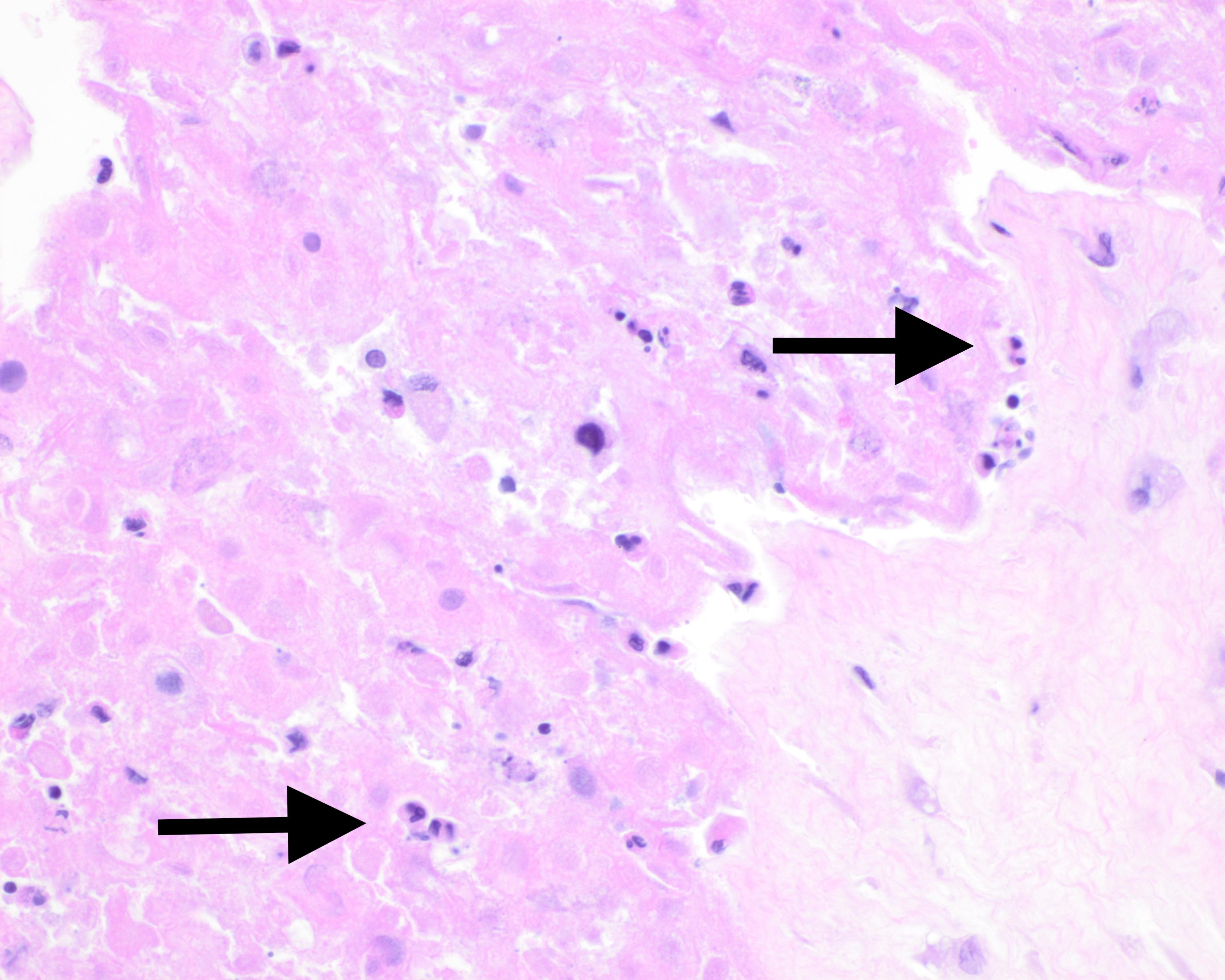
Contributed by Theonia K. Boyd, M.D.
Ischemic umbilical myocyte elongation
Ischemic umbilical myocyte pyknosis
Postmortem chorioamnionitis
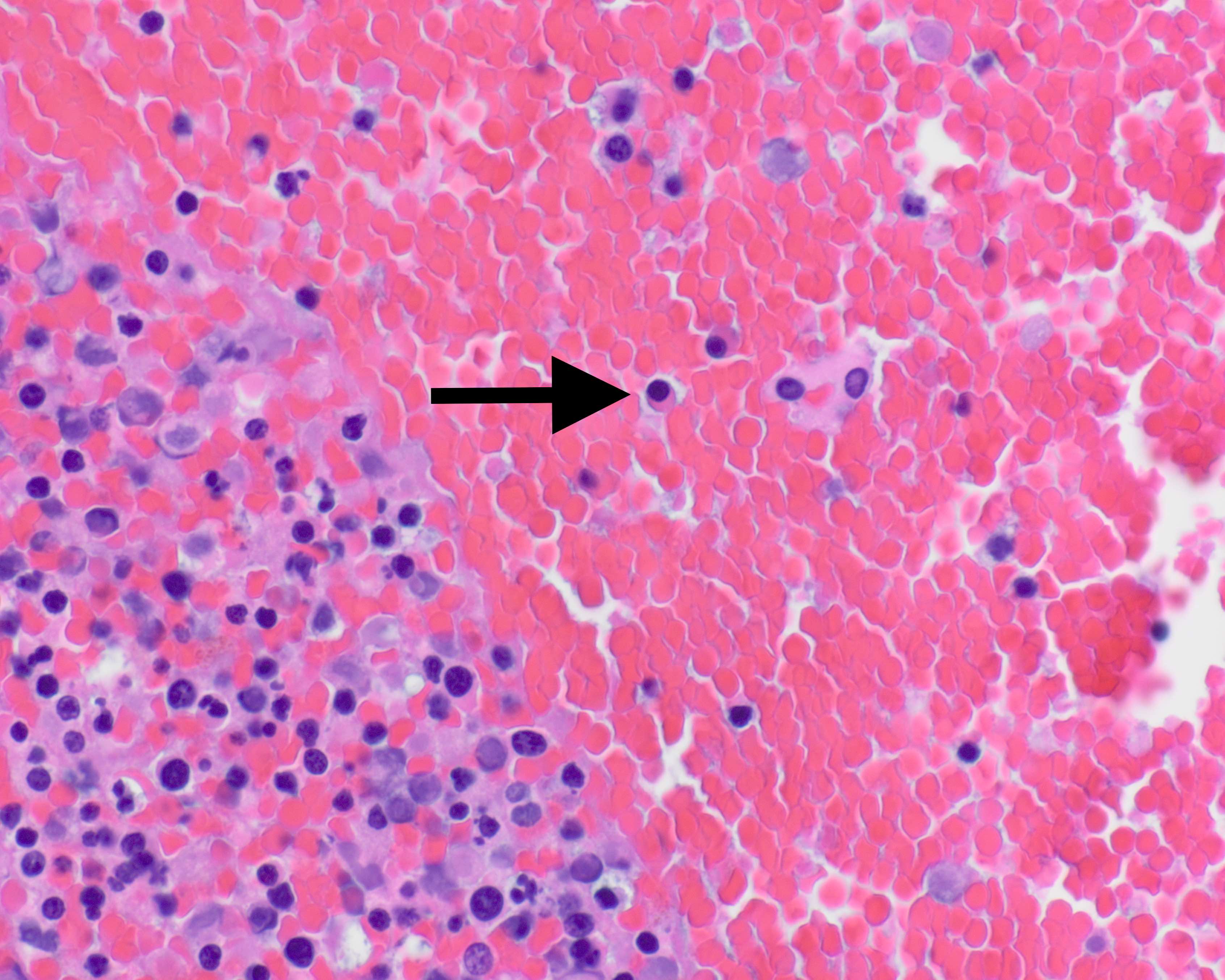
Nucleated fetal red blood cells
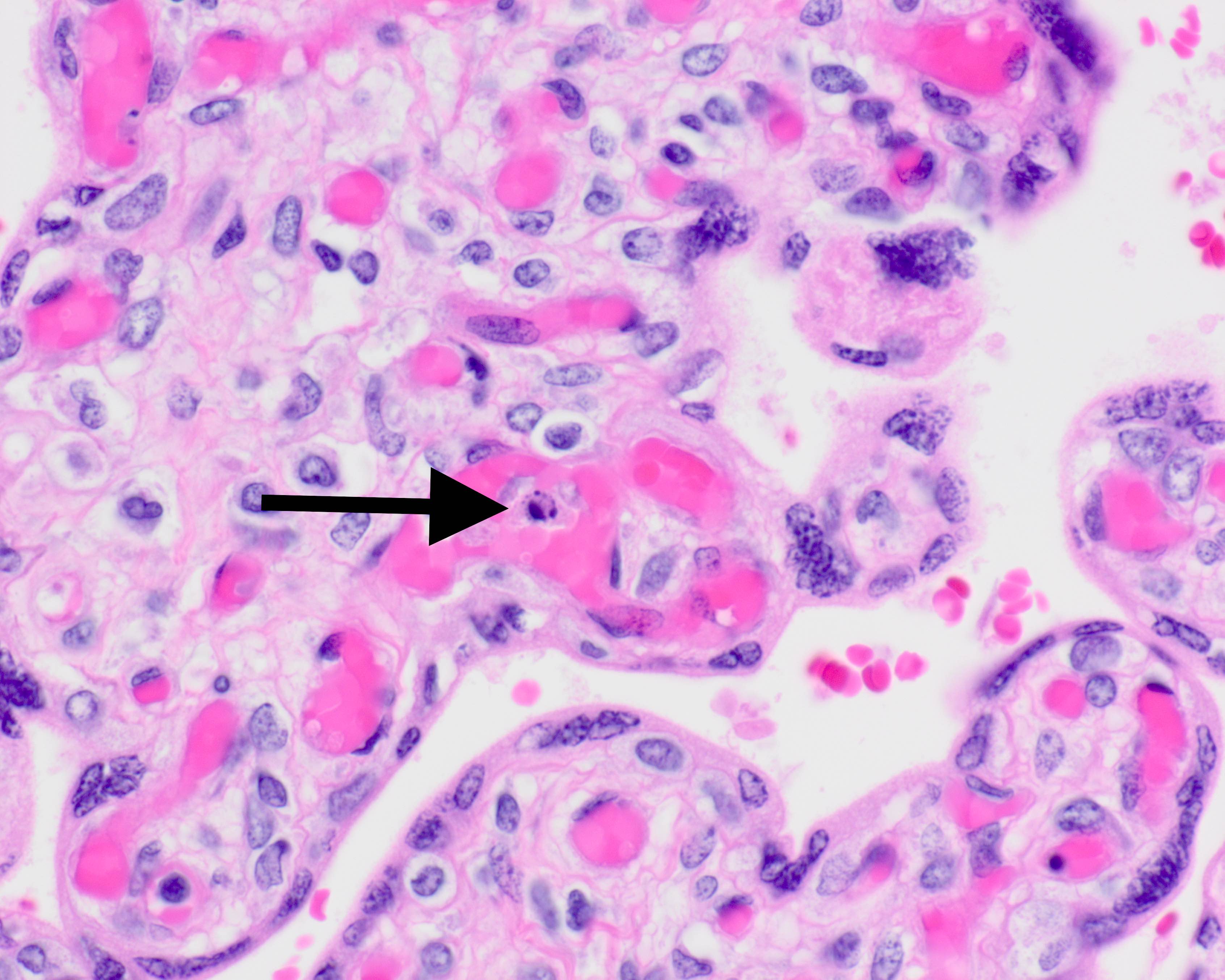
Intravascular karyorrhexis
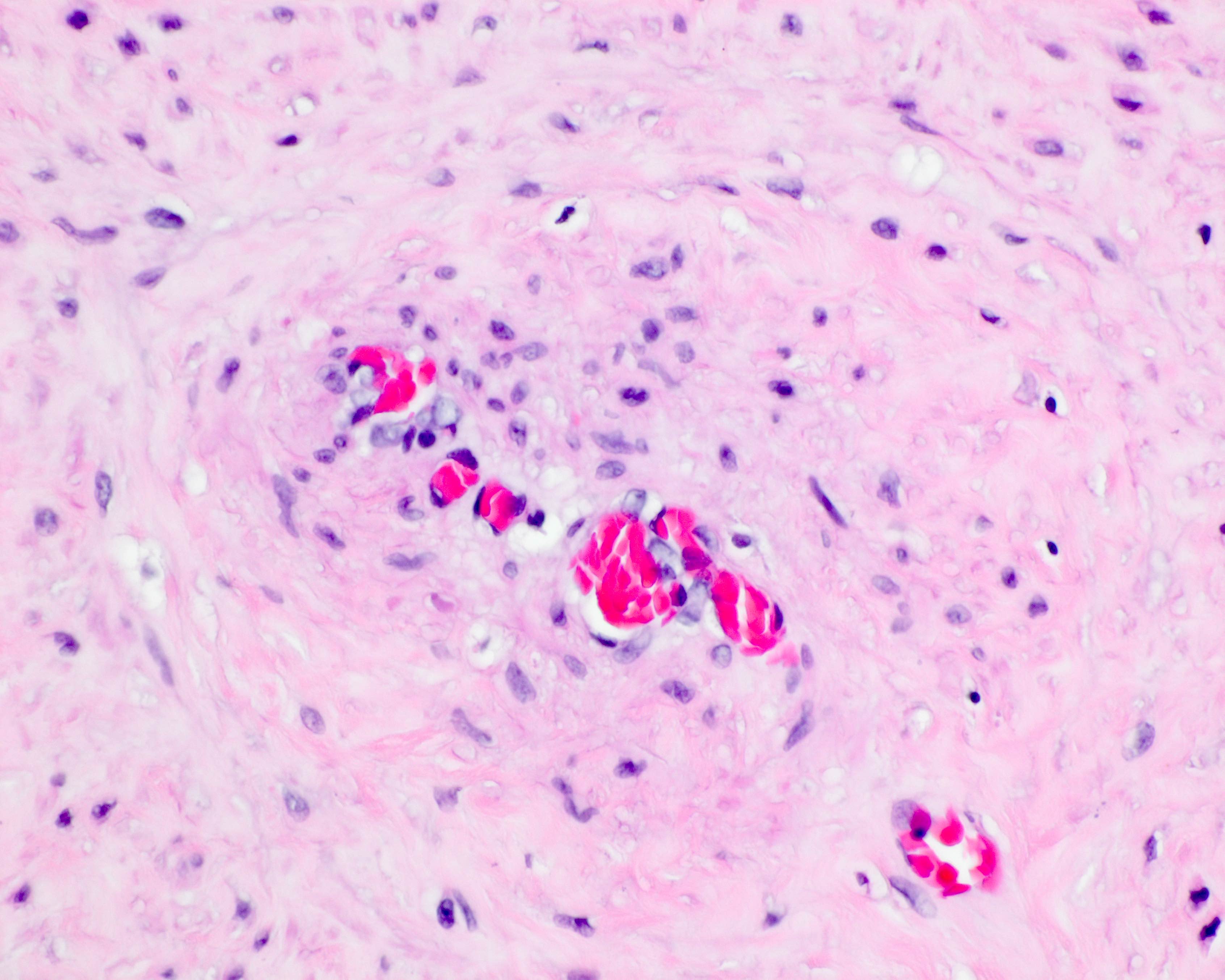
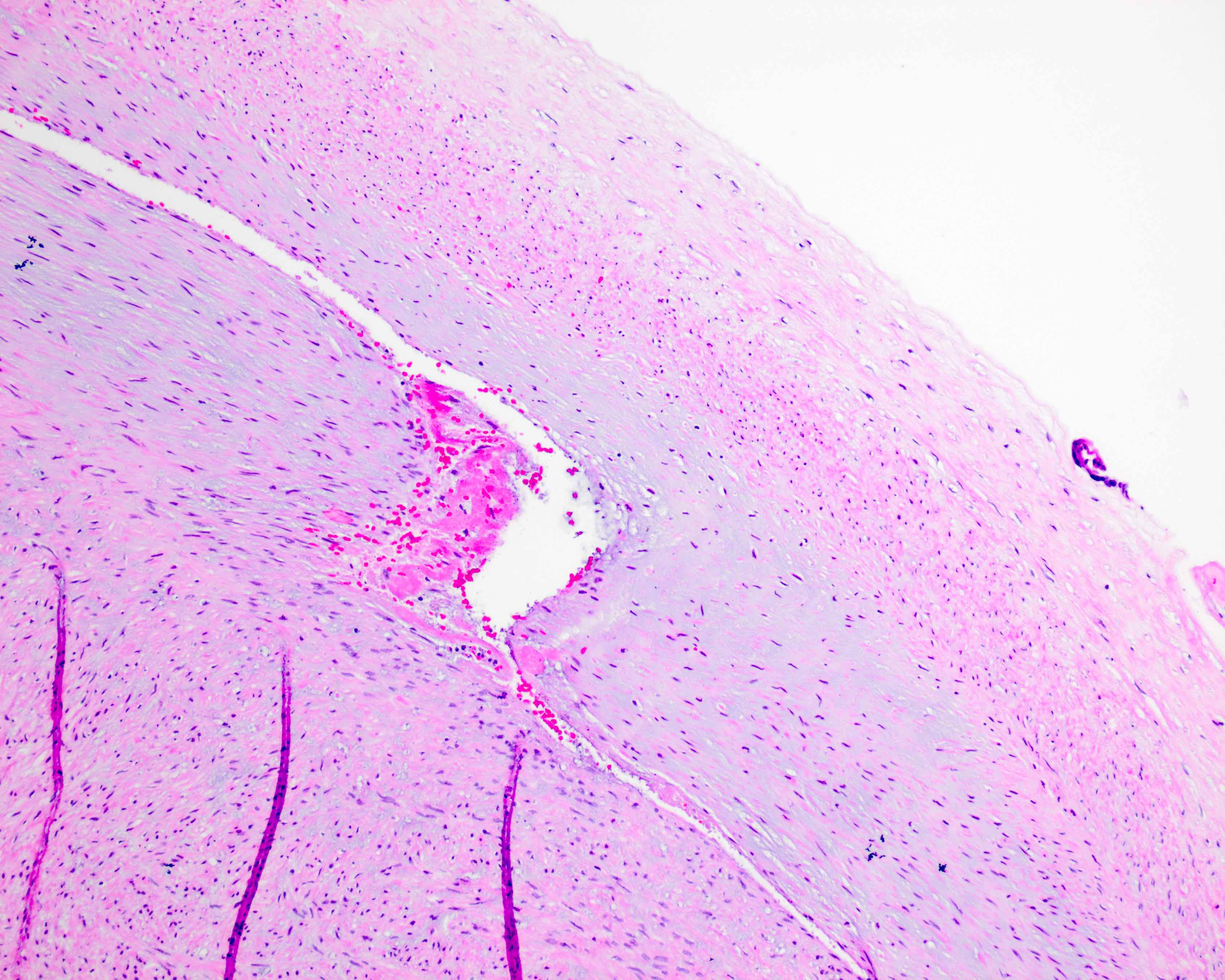
Stem vessel obliteration
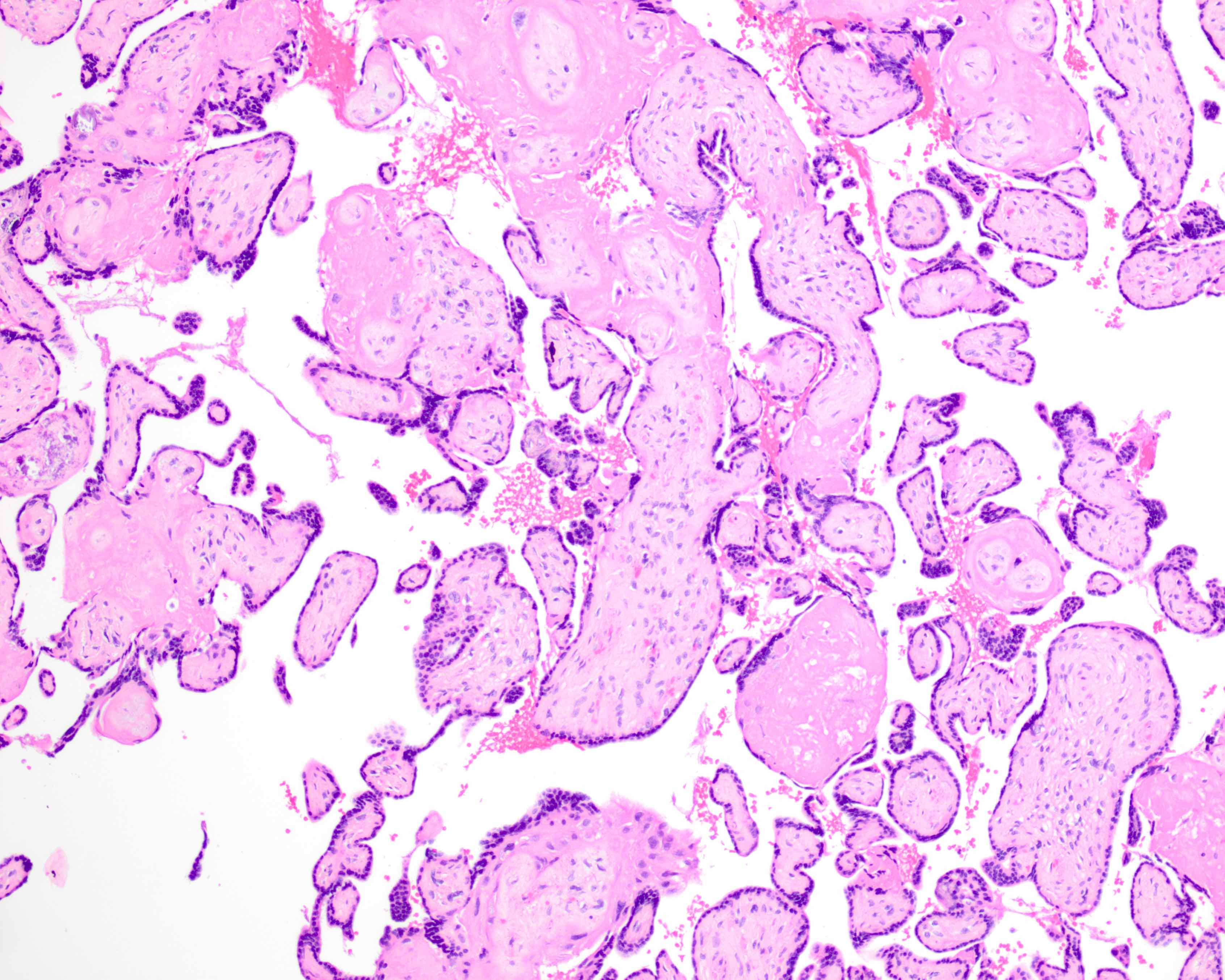
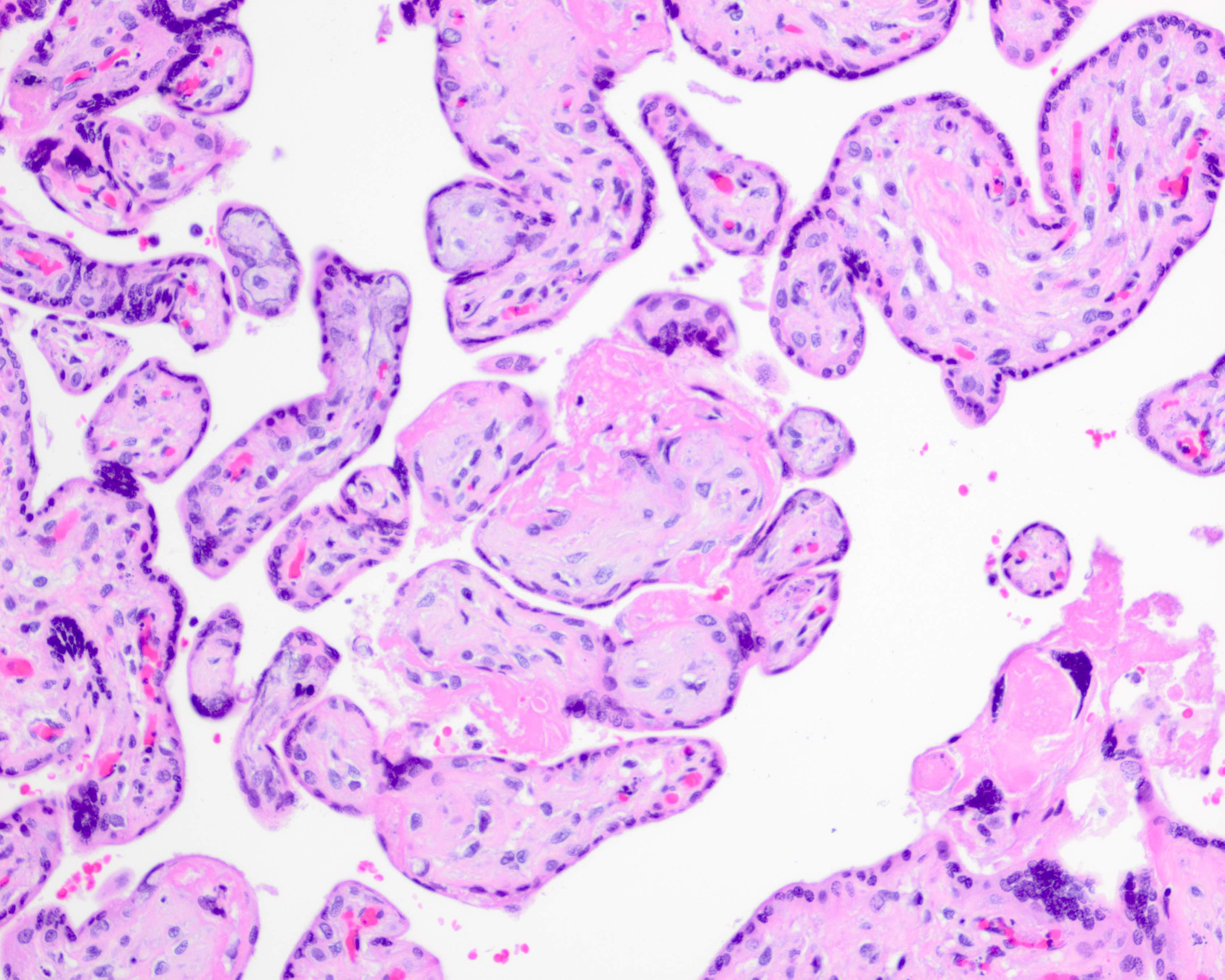
Avascular villi
Positive stains
- Infectious organisms: bacterial, protozoal, viral special stains / immunohistochemistry (e.g., Toxoplasma)
- Immune mediated disorder cell type immunohistochemistry if necessary (e.g., chronic histiocytic intervillositis)
Molecular / cytogenetics description
- Parental, fetal and placental genetic disorders: whole chromosomes, translocations, single gene mutations, isodisomy
Sample pathology report
- Placenta, stillbirth delivery at __/7 weeks gestation:
- __ gram [small / heavy] placenta (__ grams expected; __percentile [if < tenth or > ninetieth percentile]; fetal / placental weight ratio __/1 (expected __/1)
- Intrauterine demise attributable to __ (list all clinical, gross and microscopic supporting evidence individually)
- Additional findings (list additional information) (see comment)
- Comment: Intrauterine demise in this case is attributable to ___. (Paragraph regarding relevant etiology, statistics, recurrence risk). This placenta accompanies fetal postmortem examination ___.
Differential diagnosis
- Fetal vascular malperfusion (FVM) versus passive postmortem fetal vascular involution:
- Features of FVM are geographically and temporally heterogeneous
- Features of FVM precede fetal demise, if the time of fetal demise is discernible
- Fetal muscular vessels with recent / organizing / organized / remote thrombosis containing fibrin are always antemortem
- FVM is often accompanied by a known predisposing condition (e.g., umbilical hypercoiling, nuchal or body wrapped cord)
- Maternal vascular malperfusion (MVM) versus postmortem altered maternal perfusion:
- Features of MVM chronologically antedate the time of fetal demise if the latter is discernible
- Tendency for multiple coexistent pathologies: infarcts, abruption, accelerated villous maturation, increased syncytial knots, increased perivillous fibrin
- Decidual arteriopathy is antemortem only
- MVM features usually seen in the latter half of pregnancy
- Accompanied by placental and fetal growth restriction
- Noninfectious chronic villitis (VUE) versus infectious villitis (lymphoplasmacytic inflammation with or without viral cytopathic effect [CMV / HSV]) / cytoplasmic tachyzoites (Toxoplasma):
- VUE will be comprised solely of maternal lymphocytes and histiocytes
- Maternal lymphocytes and histiocytes may be also present trafficking the intervillous space
- Often accompanied by lymphoplasmacytic basal deciduitis
- No viral cytopathic effect in villous stroma
- No tachyzoites in villous stromal cells, amnion epithelium or Wharton jelly
- No villous stromal hemosiderin on H&E
- Amniotic fluid infection (AFI)
- Maternal inflammation versus postmortem maternal membrane inflammatory response to nonviable antigen(s) exposure:
- Maternal inflammatory response (MIR) with AFI can be of advanced grade and stage
- Coexisting fetal inflammatory response (FIR) may be present
- Coexisting acute subchorionitis (neutrophils beneath the chorionic plate) favors AFI
- Fetal inflammation versus umbilical vascular ischemic myocyte pyknosis:
- Fetal inflammatory response (FIR) will demonstrate nonpyknotic neutrophil nuclei with pale pink cytoplasm
- FIR may extend to perivascular stroma in Wharton jelly or chorionic plate stroma
Additional references
Board review style question #1
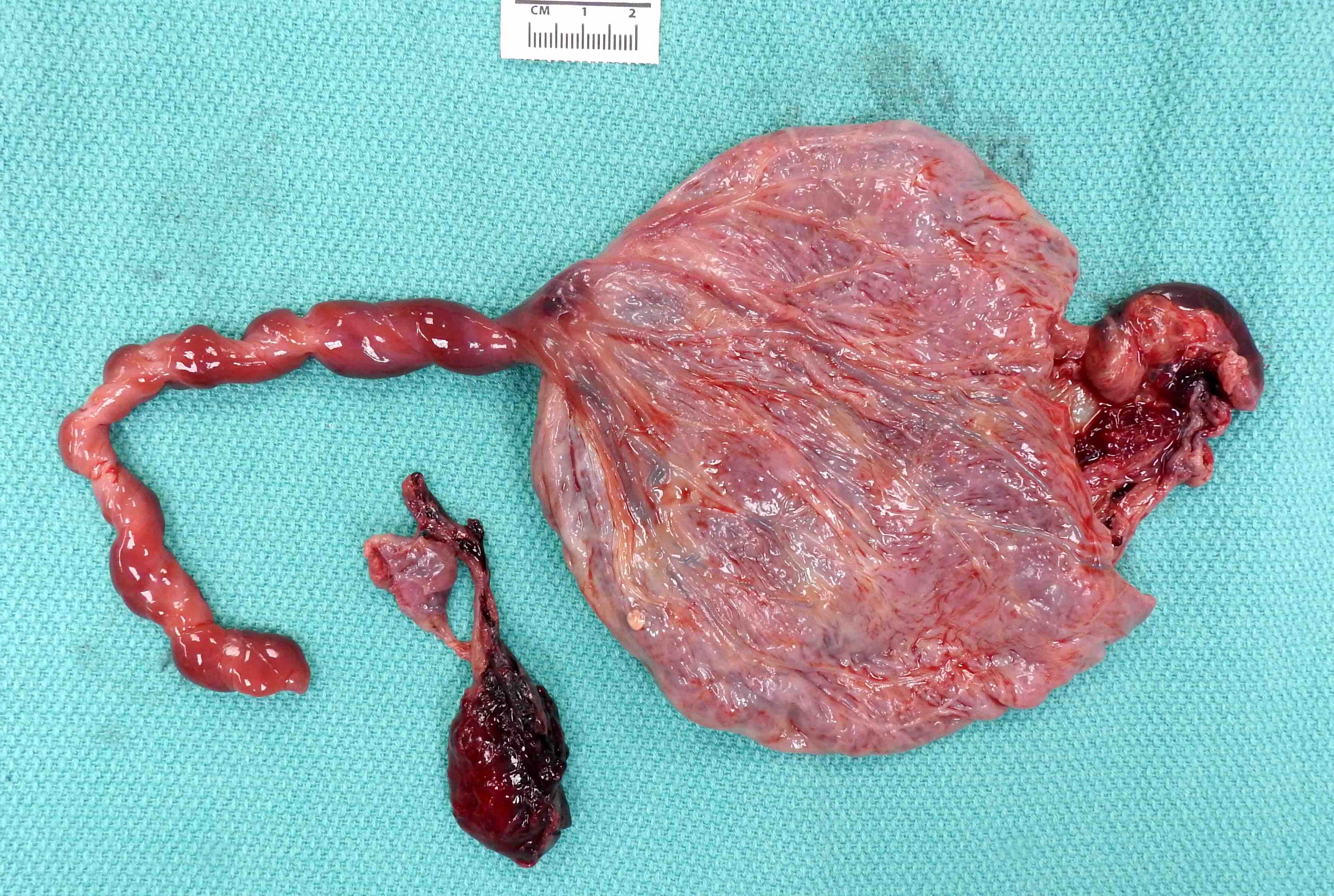
This is a placenta from a fetal demise at 28 weeks' gestation. What does the gross image above show?
- Abnormal umbilical cord insertion
- Amnion nodosum
- Heavy placenta
- Placental abruption
- Umbilical hypocoiling
Board review style answer #1
Board review style question #2
This is a microscopic image from a placenta at 28 weeks' gestation. What is depicted in the image above?
- Acute subchorionitis
- Chorionic vasculitis
- Perivillous fibrin
- Postmortem fetal vascular involution
- Recent chorionic thrombosis
Board review style answer #2
Board review style question #3
This is a microscopic image from a placenta at 28 weeks' gestation. What is depicted in the image above?
- Avascular villi due to fetal vascular malperfusion
- Avascular villi due to postmortem vascular involution
- Chronic villitis
- Massive perivillous fibrin
- Placental abruption
Board review style answer #3
A. Avascular villi due to fetal vascular malperfusion
Comment Here
Reference: Intrauterine fetal demise
Comment Here
Reference: Intrauterine fetal demise

