
Placenta
Nonneoplastic placental conditions and abnormalities
Infectious
Acute chorioamnionitis
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 16 June 2022
Last staff update: 16 June 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Acute chorioamnionitis


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Norgan AP, Roberts DJ. Acute chorioamnionitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/placentachorioamnionitis.html. Accessed March 31st, 2025.
Definition / general
- Acute chorioamnionitis is defined by the presence of acute inflammation (neutrophils) within the chorion or amnion (or both) of the extraplacental membranes or chorionic plate (maternal inflammatory response [MIR]), with or without acute inflammatory cell extravasation from the umbilical cord vasculature or chorionic plate vessels (fetal inflammatory response [FIR])
Essential features
- Acute chorioamnionitis is due to a maternal (with or without accompanying fetal) inflammatory response
- Fetal inflammatory response (inflammatory cell extravasation from umbilical or chorionic plate vessels) is associated with longer term and more severe infections
- Commonly associated with ascending bacterial or fungal cervicovaginal flora infecting the amniotic fluid
- Uncommonly associated with hematogenously disseminated bacteria (e.g., Listeria)
- Associated with risk of neonatal sepsis and poor neonatal outcomes especially when there is a fetal inflammatory response
Terminology
- Histologic chorioamnionitis
- Necrotizing chorioamnionitis
- Chorionitis
- Subchorionitis
- Umbilical vein vasculitis
- Umbilical artery vasculitis
- Fetal vasculitis
ICD coding
Epidemiology
- More common in younger, nulliparous women
- Risk factors include:
- Longer duration rupture of membranes (Clin Infect Dis 1993;17:S100)
- Extended length of labor (Am J Obstet Gynecol 1997;177:1024)
- Number of intrapartum digital vaginal examinations (Am J Obstet Gynecol 1997;177:1024)
- Use of indwelling devices around labor (intracervical balloon catheter, fetal monitors) (Am J Obstet Gynecol 1996;175:304)
- Cervical insufficiency (Am J Obstet Gynecol 2003;189:746)
- Bacterial vaginosis (Am J Obstet Gynecol 1997;176:672)
- Group B Streptococcus colonization (J Infect Dis 1983;148:802)
- Meconium stained amniotic fluid (Am J Obstet Gynecol 2003;189:746)
- Pregnancy with a foreign body in situ (e.g., cerclage, IUD) (J Perinat Med 2010;38:45)
Sites
- Extraplacental membranes: chorion or amnion (MIR)
- Umbilical cord: vein or arteries (FIR)
- Chorionic plate: chorion or amnion (MIR) and vessels (FIR)
Pathophysiology
- Amniotic fluid infection by ascending cervicovaginal flora (common) or hematogenously or postprocedurally infecting organisms (uncommon) causes activation of material and fetal inflammatory responses
- In the maternal inflammatory response, maternal neutrophils migrate from the decidual circulation into the extraplacental decidua, chorion and amnion, or the intervillous circulation into the chorionic plate and overlying amnion
- In the fetal inflammatory response, fetal neutrophils extravasate from fetal vessels in the umbilical cord or chorionic plate and migrate toward the amniotic fluid (amniotropic)
- Release of cytokines and other inflammatory mediators can lead to rupture of membrane or onset of labor
- Reference: Pediatr Res 2022;91:289
Etiology
- Amniotic fluid infection is typically polymicrobial, often involving 2 or more organisms from vaginal or enteric flora; single pathogens may be seen in hematogenously disseminated infections or when 1 organism in a polymicrobial infection outcompetes the others
- Organisms that are commonly isolated from amniotic fluid infections include (J Infect Dis 1988;157:113):
- Ureaplasma urealyticum and Mycoplasma hominis (Clin Infect Dis 1993;17:S100)
- Gram negative anaerobic vaginal flora (e.g., Bacteroides spp., Gardnerella sp.)
- Group B Streptococcus
- Peptostreptococcus spp.
- Escherichia coli
- Enterococci
- Fusobacterium spp.
Clinical features
- Can be clinically silent
- Maternal fever > 37.5 °C, uterine tenderness, abdominal pain, foul smelling vaginal discharge, maternal and fetal tachycardia (BJOG 2017;124:775, J Perinat Med 2016;44:5, J Perinat Med 2016;44:23)
- Associated with fetal infection, neonatal sepsis, stillbirth, spontaneous preterm birth and fetal central nervous system injury (Semin Perinatol 2015;39:2)
- Fetal inflammatory response associated with multiorgan injury, including chronic lung disease, periventricular leukomalacia and cerebral palsy (Front Immunol 2020;11:531543, Clin Perinatol 2010;37:339, Am J Obstet Gynecol 2020;223:745.e1, Am J Reprod Immunol 2018;79:e12803)
Diagnosis
- Clinical diagnosis (Obstet Gynecol 2016;127:426, J Perinat Med 2016;44:23):
- Clinical chorioamnionitis (or intrauterine inflammation or infection) is diagnosed by a combination of physical examination findings and laboratory results
- Isolated maternal fever:
- Clinically documented fever ≥ 39.0 °C once or ≥ 38.0 °C (oral) twice
- Suspected intrauterine inflammation or infection:
- Fever (as above), plus 1 or more of the following:
- Fetal tachycardia (greater than 160 beats per minute for 10 minutes or longer)
- Elevated maternal white blood count (> 15,000 per mm3; in the absence of corticosteroids)
- Purulent fluid from the cervical os
- Fever (as above), plus 1 or more of the following:
- Confirmed intrauterine inflammation or infection:
- Suspected intrauterine inflammation or infection findings, plus:
- Positive amniotic fluid Gram stain or culture
- Low amniotic fluid glucose (e.g., ≤ 14 mg/dL)
- Elevated amniotic fluid white cell count (> 30 cells/mm3; in the absence of red blood cells indicating blood contamination)
- Histopathologic evidence of acute chorioamnionitis
- Suspected intrauterine inflammation or infection findings, plus:
Laboratory
- Positive:
- Amniotic fluid Gram stain
- Amniotic fluid culture
- Placental tissue culture
- Fetal tissue culture (e.g., lung tissue) in cases of fetal demise
- Placental tissue (fresh or FFPE) molecular testing (e.g., PCR)
- Neonatal blood cultures within day 1 of life
Prognostic factors
- Unfavorable factors:
- Necrotizing chorioamnionitis
- Fetal inflammatory response
- References: Front Immunol 2020;11:531543, Am J Reprod Immunol 2018;79:e12803, Neurotoxicology 2017;61:47
Case reports
- 25 and 34 year old women with chorioamnionitis with placental listeriosis (Obstet Gynecol Sci 2018;61:688)
- 26 year old woman chorioamnionitis caused by S. marcescens (Open Med (Wars) 2020;16:81)
- 31 year old woman with necrotizing chorioamnionitis due to Kingella kingae (Diagnostics (Basel) 2021;11:243)
- 36 year old woman with Klebsiella pneumoniae chorioamnionitis (Microorganisms 2021;9:96)
- 41 year old woman with Candida chorioamnionitis (Case Rep Womens Health 2020;27:e00239)
Treatment
- Maternal and neonatal antibiotic therapy (Clin Microbiol Infect 2011;17:1304, Pediatrics 2016;137:e20152323)
Gross description
- Dull, opaque membranes with yellow-green discoloration and cloudy amniotic fluid, possibly with purulent exudate
- Can be grossly normal
- Acute marginal hemorrhage in preterm deliveries (ISRN Obstet Gynecol 2012;2012:856971)
- Multifocal umbilical cord surface microabscesses in C. albicans infections (APMIS 2018;126:570)
Gross images
Contributed by Drucilla J. Roberts, M.D.

Patchy surface, plaque-like lesions
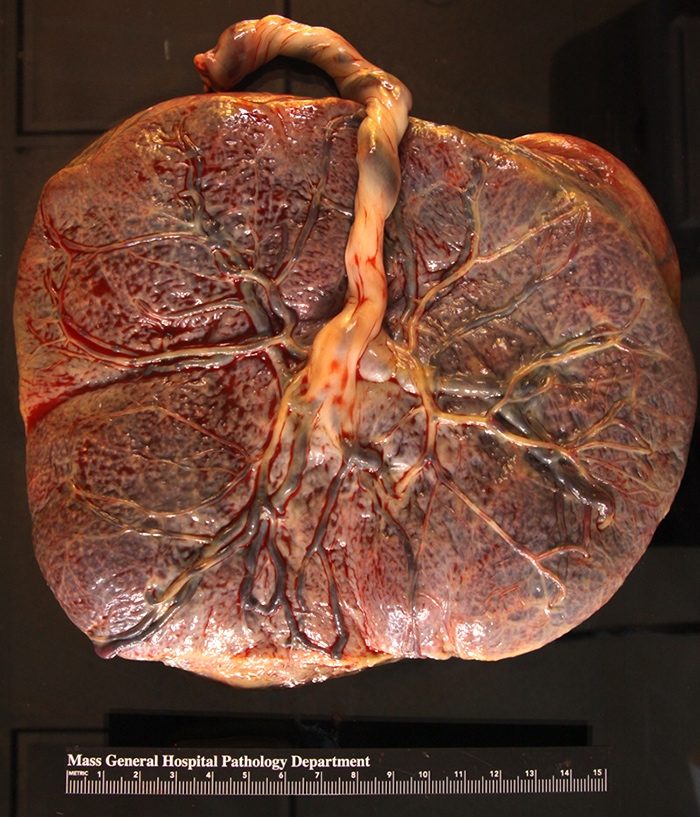
Yellow / cloudy fetal surface of placenta
Microscopic (histologic) description
- Acute chorioamnionitis should be staged and graded based on MIR and FIR (Arch Pathol Lab Med 2016;140:698, Roberts: Atlas of Placental Pathology, 2021)
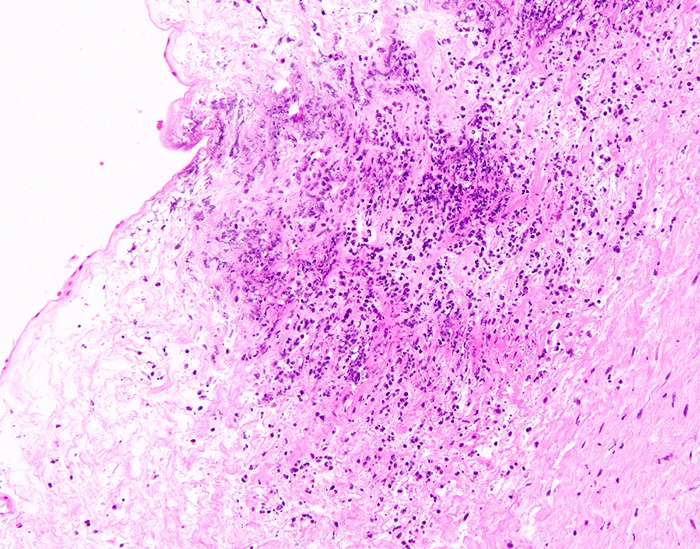
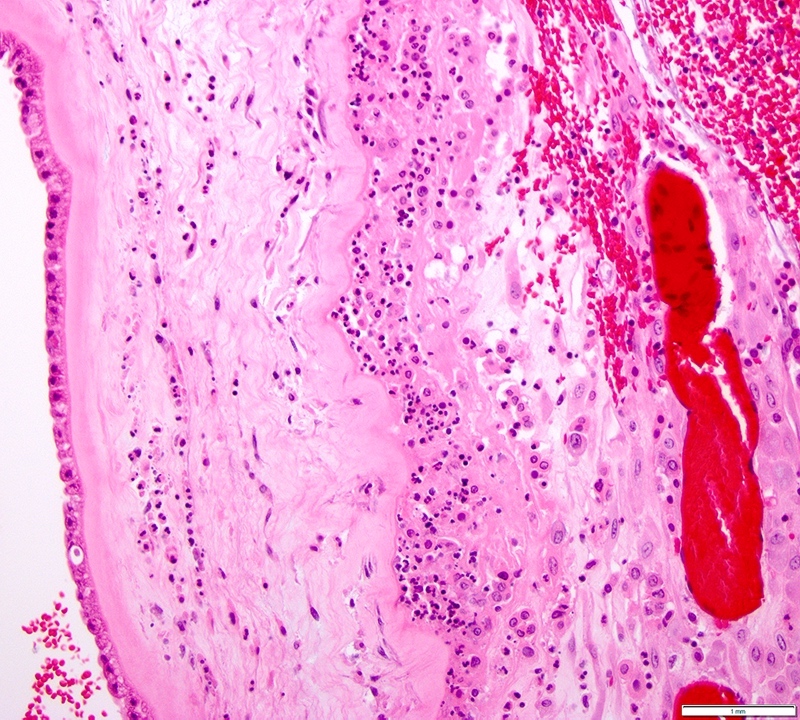
- MIR stage (location):
- Stage 0 (preacute chorioamnionitis): neutrophils in the subchorial intervillous space beneath the chorionic plate (subchorionitis)
- Stage 1 (early): neutrophils in chorion laeve of the extraplacental membranes (chorionitis)
- Stage 2 (intermediate): neutrophils within chorionic or amnionic mesoderm
- Stage 3 (advanced): stage 2, plus necrosis of amnionic epithelium or neutrophil necrosis
- MIR grade (severity):
- Grade 1 (mild to moderate): anything less than severe, as described below
- Grade 2 (severe): confluent neutrophils or > 3 foci of > 200 neutrophils
- FIR stage:
- Stage 1 (early): fetal inflammatory cells within chorionic plate vessel walls (fetal vasculitis) or umbilical vein vessel wall (umbilical vein vasculitis)
- Stage 2 (intermediate): fetal inflammatory cells within umbilical arteries (umbilical artery vasculitis) or vein
- Stage 3 (advanced): necrotizing funisitis (perivascular bands of necrotic Wharton jelly containing dense neutrophils)
- FIR grade:
- Grade 1 (mild to moderate): anything less than severe, as described below
- Grade 2 (severe): confluent fetal inflammatory cells with attenuation / degeneration of smooth muscle
- Accompanying findings:
- Acute intervillositis: aggregates of neutrophils in the intervillous space; often due to Listeria monocytogenes
- Peripheral funisitis: wedge-like foci of neutrophils with necrosis at the periphery of the umbilical cord; often due to Candida
Microscopic (histologic) images
Contributed by Drucilla J. Roberts, M.D. and AFIP
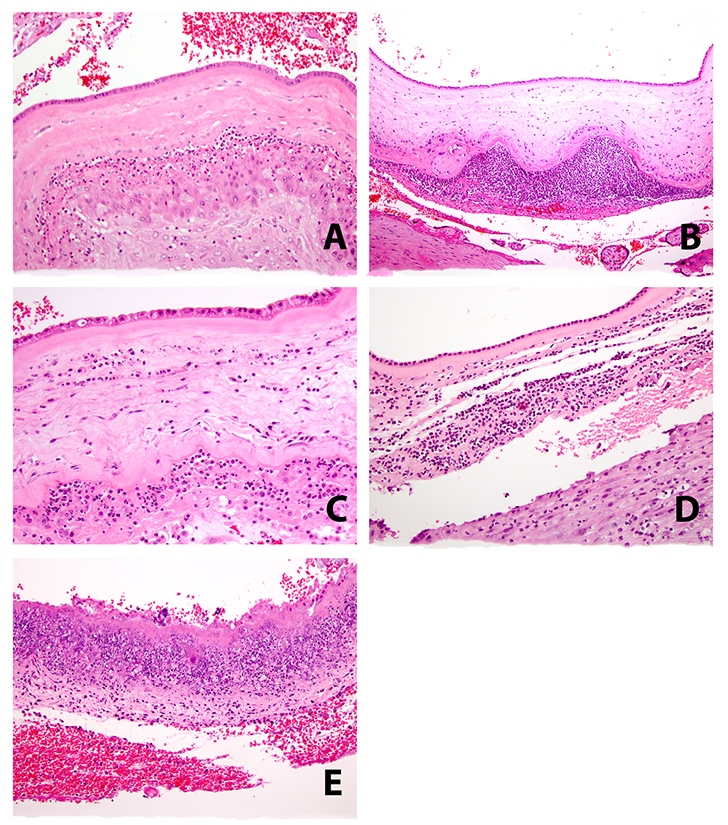
MIR stages and grades
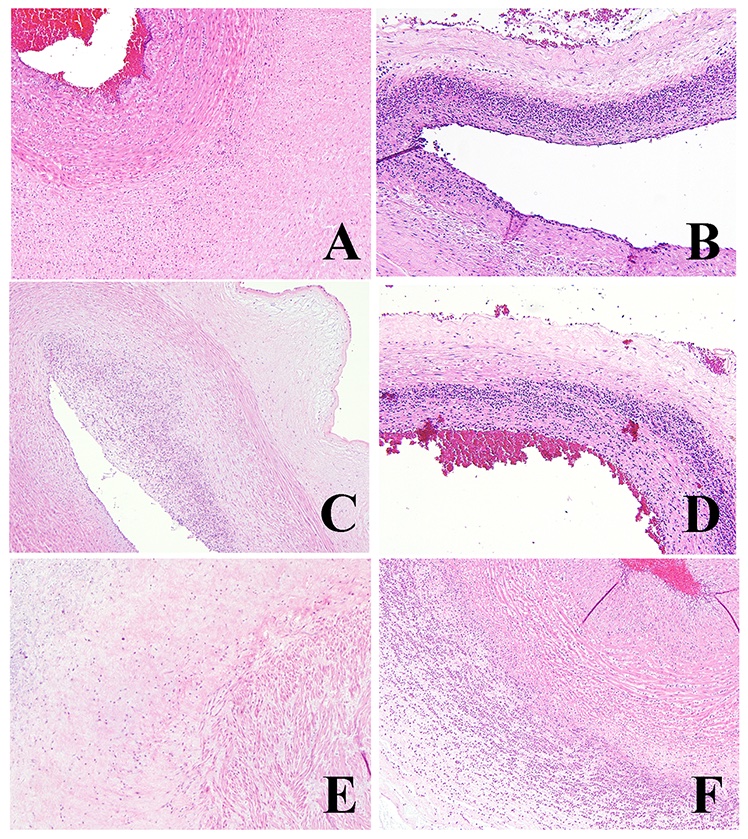
FIR stages and grades
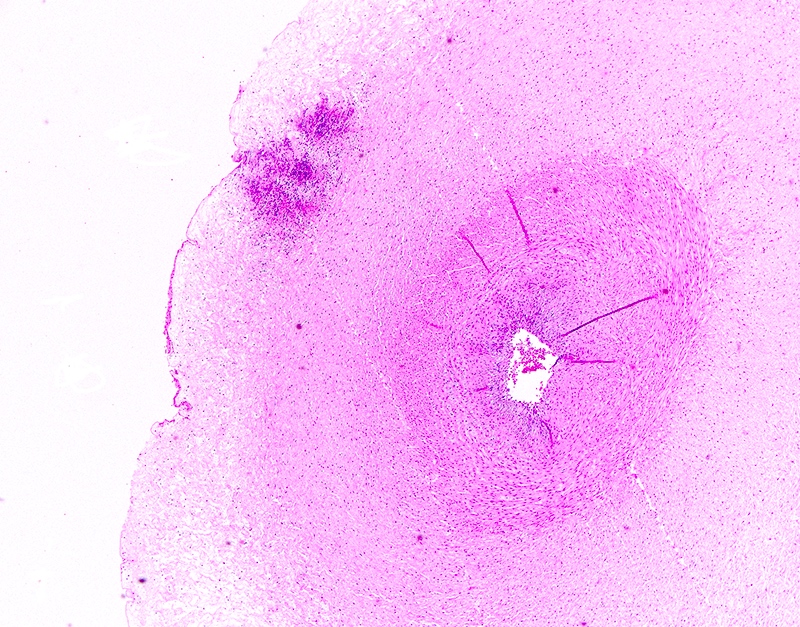
Umbilical cord with surface abscess

GMS stain showing invasive fungal hyphae
Virtual slides
Images hosted on other servers:

17 week placenta with stage 2 grade 2 MIR


24 week gestation with clinical suspicion for acute chorioamnionitis with umbilical cord microabscesses
Sample pathology report
- Singleton placenta, delivery:
- Acute chorioamnionitis (maternal stage X; grade X) with fetal vascular involvement (fetal stage X; grade X)
Differential diagnosis
- Chronic chorioamnionitis:
- Mononuclear infiltrate in the chorion laeve or chorion and amnion
- Often associated with villitis of unknown etiology
- Thought to be a host versus graft-like reaction
- Has a recurrence risk
- Meconium histiocytic infiltrate:
- Meconium pigment within histiocytes in the membranes
- Often accompanies acute chorioamnionitis
- Acute inflammation in the space between the amnion and chorion:
- Inflammation is not within the soft tissue or epithelium but in the space between the 2 membranes
- Often associated with vernix caseosa or loose meconium
- Not true acute chorioamnionitis unless the inflammatory cells are within tissue
- Acute deciduitis:
- Acute inflammation retained only within the decidua capsularis or parietalis, not in the chorion laeve epithelium
- Feature of labor, not infection
Board review style question #1
A yellow / green discolored and cloudy placenta shows which of the following histologies of the membranes and umbilical cord?
- Stage 0 grade 1 acute chorioamnionitis, maternal inflammatory response with a fetal inflammatory response stage 1 grade 1
- Stage 1 grade 1 acute chorioamnionitis, maternal inflammatory response with a fetal inflammatory response stage 2 grade 1
- Stage 2 grade 2 acute chorioamnionitis, maternal inflammatory response with a fetal inflammatory response stage 2 grade 1
- Stage 3 grade 2 acute chorioamnionitis, maternal inflammatory response with a fetal inflammatory response stage 2 grade 2
Board review style answer #1
C. Stage 2 grade 2 acute chorioamnionitis, maternal inflammatory response with a fetal inflammatory response stage 2 grade 1
Comment here
Reference: Acute chorioamnionitis
Comment here
Reference: Acute chorioamnionitis
Board review style question #2
This umbilical cord shows patchy white / yellow lesions on the surface. What is the most likely diagnosis?
- Candidal funisitis
- Fusobacterial funisitis
- Meconium myonecrosis
- Syphilitic funisitis
Board review style answer #2
