
Penis & scrotum
Infectious
Syphilis
Authors: Alcides Chaux, M.D., Antonio L. Cubilla, M.D.

Last author update: 1 February 2010
Last staff update: 21 September 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Syphilis


Table of Contents
Definition / general | Terminology | Epidemiology | Etiology | Clinical features | Laboratory | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy images | Differential diagnosisCite this page: Chaux A, Cubilla AL. Syphilis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/penscrotumsyphilis.html. Accessed March 31st, 2025.
Definition / general
- Caused by Treponema pallidum; humans are the only natural host (Wikipedia: Syphilis [Accessed 30 March 2018])
- Sexually transmitted disease with primary, secondary and tertiary phases (not very infectious in tertiary stage) (eMedicine: Syphilis [Accessed 30 March 2018])
Terminology
- Historically called lues
Epidemiology
- U.S. incidence dropped through 2000 but has risen since with more cases in men having sex with men
Etiology
- Caused by Treponema pallidum, subspecies pallidum, a microaerophilic spirochete that is pathogenic only to humans
Clinical features
- Called "the great imitator" because it may mimic other disorders if presentation is unusual
- 30% transmission rate from sexual intercourse
Primary syphilis:
- Painless hard chancre (ulcer with indurated and punched out base) at site of inoculation, often in glans
- Most common affected sites are inner foreskin, coronal sulcus, penile shaft and penile base
- Chancres are usually solitary
Secondary syphilis:
- Bacteremic stage with greatest number of organisms in the body
- Classically has widespread rash (small red macular lesions), including on palms and soles and mucous membranes
- Condyloma lata, formed by soft, flat topped, moist, red / rose / gray to pale maculopapules, nodules or plaques, is the characteristic anogenital lesion and may become confluent; are common in scrotum
- May have varied clinical presentation
Tertiary syphilis:
- Gummatous form is characteristic: granulomas with epithelioid and giant cells, obliterative endarteritis and necrosis
- Also cardiovascular form and neurosyphilis
- Accelerated time course occurs with HIV infection (1 year to neurosyphilis)
Laboratory
- Screening tests: rapid plasma reagin (RPR, Wikipedia: Rapid Plasma Reagin [Accessed 30 March 2018]) and VDRL (Wikipedia: Venereal Disease Research Laboratory Test [Accessed 30 March 2018])
- Confirmatory tests: fluorescent treponemal antibody absorption (FTA-ABS) or Treponema pallidum hemagglutination assay
- Note: patients receiving IV immunoglobulin may passively acquire treponemal antibodies (Arch Pathol Lab Med 2002;126:1237)
Case reports
- 22 year old man with nodular and annular skin lesions over face, back and limbs (Dermatol Online J 2003;9:9)
- 26 year old homosexual man with secondary syphilis localized to penis / scrotum (G Ital Dermatol Venereol 2009;144:725)
Treatment
- Penicillin G
Clinical images
AFIP images

Sharply delineated lesion

Two well circumscribed, minimally elevated lesions
Images hosted on other servers:


Primary chancre

Atrophic scar with condylomata lata
Secondary rash / lesions:




Palm, limbs and hands


Back



Face, teeth

"Kissing" lesions

Various images
Microscopic (histologic) description
- Presence of obliterative endarteritis surrounded by a predominantly plasmocytic infiltrate is characteristic of all stages
- Spirochetes can be identified in primary and secondary lesions but are difficult to demonstrate in gummas
- Primary syphilis: ulceration, granulation tissue and obliterative endarteritis at ulcer base; plasma cells and lymphocytes underlying ulcer, endothelial cell proliferation and capillaritis
- Secondary syphilis: psoriasiform epidermal hyperplasia or spongiform pustular lesions with superficial or deep obliterative endarteritis and lymphoplasmacytic infiltrate at the dermal epidermal junction; perivascular infiltrate and possible granulomas; also nodal involvement with florid follicular hyperplasia, unusually shaped follicles, endothelial swelling and perivascular cuffs of plasma cells and lymphocytes
- Tertiary syphilis: gummas formed by granulomas with epithelioid and multinucleated giant cells, obliterative endarteritis and necrotic foci
Microscopic (histologic) images
AFIP images
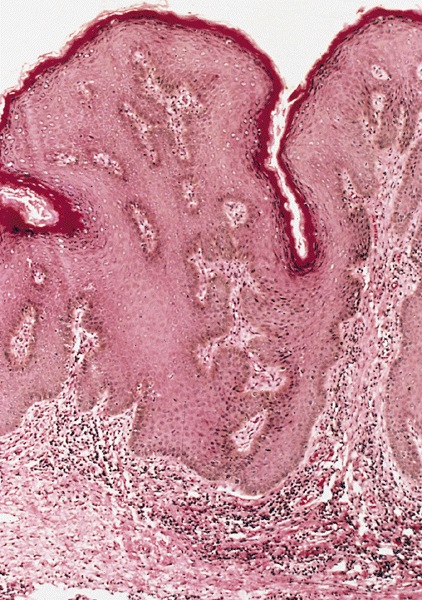
Lesion characterized by acanthosis
Images hosted on other servers:

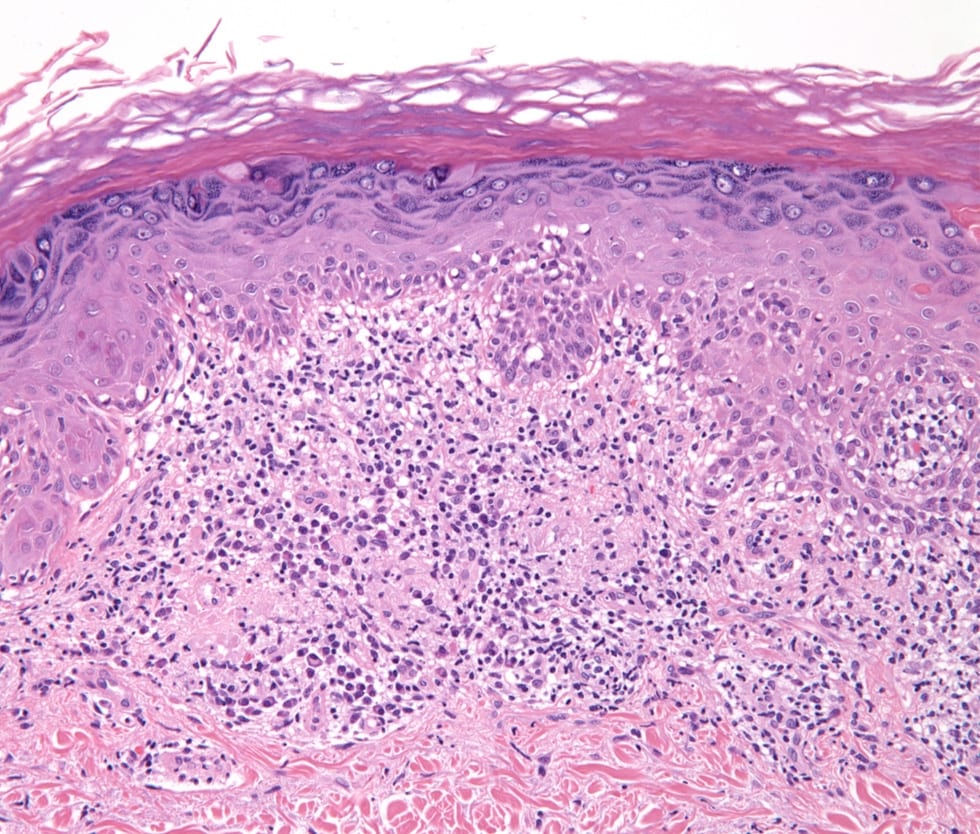
Perivascular dermal infiltrate
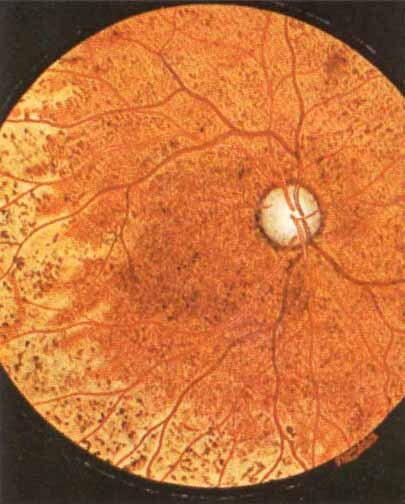
Chorioretinitis of congenital syphilis


Darkfield microscopy

Patchy infiltrate

Epithelioid cells surrounded by lymphomono-nuclear cells
Various images
Positive stains
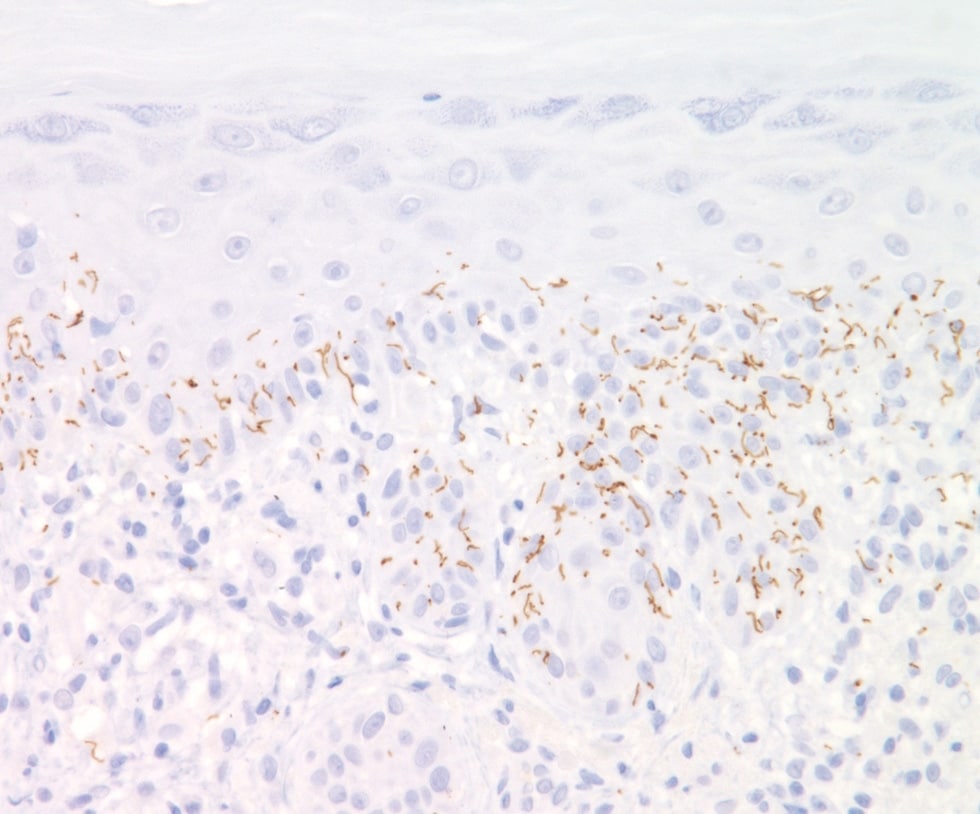
- Spirochete identified by darkfield microscopy, Warthin-Starry stain or Steiner stain
- Treponema pallidum immunostain is more sensitive than Warthin-Starry stain (Hum Pathol 2009;40:624)
Electron microscopy images
Images hosted on other servers:


Spirochete in culture
Differential diagnosis
- Lymphoma: monoclonal lymphoplasmacytic infiltrate; no clinical or laboratory evidence of syphilis
- Plasma cell myeloma: monoclonal plasma cells, often binucleated; monoclonal gammopathy; no clinical or laboratory evidence of syphilis
