
Penis & scrotum
General
Grossing & features to report
Authors: Shaheed W. Hakim, M.D., Trevor A. Flood, M.D.
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 30 March 2023
Last staff update: 30 March 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Gross penectomy / circumcision specimens


Table of Contents
Definition / general | Grossing - penectomy specimens | Grossing - circumcision | Features to report | Features to report by organization | Gross images | Microscopic (histologic) images | Sample gross description report | Diagrams / tables | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Hakim SW, Flood TA. Grossing & features to report. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/penscrotumgrossingpenect.html. Accessed April 2nd, 2025.
Definition / general
- This topic describes how to gross specimens obtained from penectomy and partial penectomy procedures
- Essential clinical history: clinical diagnosis, procedure performed, prior biopsies
Grossing - penectomy specimens
- In the fresh state, cut the proximal resection margin en face
- 3 important areas of the resection margin need to sampled:
- Proximal urethra and surrounding periurethral cylinder composed of epithelium, subepithelial connective tissue (lamina propria), corpus spongiosum and penile fascia
- Urethra may be retracted but it is important to locate it and submit its circumference entirely
- Corpora cavernosa separated and surrounded by tunica albuginea and Buck fascia
- Skin of shaft with underlying corporal dartos
- Proximal urethra and surrounding periurethral cylinder composed of epithelium, subepithelial connective tissue (lamina propria), corpus spongiosum and penile fascia
- Fix the remaining specimen in 10% buffered formalin overnight
- After fixation, section the glans and shaft longitudinally (sagittally) in 2 halves, using the meatus and anterior urethra as a guide
- Do not probe the urethra as doing so can result in distortion of the urethral mucosa
- If foreskin is present:
- Measure its length and identify the presence / absence of phimosis
- If not affected by tumor, separate the foreskin, leaving a 3 mm margin from the coronal sulcus and include it as a circumcision specimen
- Do not remove foreskin if it is affected by tumor
- Document the tumor size, location, color, growth pattern and distance from resection margin
- Take a photograph of the specimen showing the maximum tumor depth of invasion
- Map the photograph according to sections submitted
- Section each half longitudinally along the specimen's longest axis, at 3 - 5 mm intervals
- Submit entirely the section which depicts the deepest anatomical level infiltrated by tumor
- If tumor affects multiple anatomical compartments, submit at least 3 sections of each compartment affected
- Sections should always attempt to include adjacent nontumoral mucosa
Grossing - circumcision
- Benign circumcision specimens:
- Sample with routine sections (1 - 2), including any grossly identified lesions / abnormalities
- Circumcision specimens containing tumor / suspicious for tumor:
- Lightly stretch and pin the specimen to cardboard / sheet of cork
- Fix in 10% buffered formalin overnight
- Measure and describe the specimen:
- Identify color and consistency
- Identify areas of flattening / thickening / induration
- Describe focal lesions, hemorrhage, exudates and edema
- Describe the tumor and its relation / distance to surgical resection margins
- Ink the mucosal and cutaneous margins of resection with different colors
- Take a photograph of the specimen
- Section the specimen transversally
- Map the photograph according to sections submitted, labeling each section in a clockwise fashion
- Submit the entire tumor and sample each surgical resection margin
- References: Eur Urol 2004;46:434, Am J Surg Pathol 2001;25:1091, Am J Surg Pathol 2003;27:994
Features to report
- Features to report are according to the College of American Pathologists Cancer Protocols (CAP: Cancer Protocol Templates [Accessed 24 January 2023])
- Foreskin: presence and type (Am J Surg Pathol 2003;27:994)
- Uncircumcised
- Phimosis
- Circumcised
- Uncircumcised
- Number of lymph nodes examined and involved
- Specimen size
- Tumor site
- Glans
- Foreskin (mucosal surface or skin surface)
- Coronal sulcus
- Skin of shaft
- Penile urethra
- Tumor size (greatest dimension + additional dimensions)
- Tumor focality
- Unicentric
- Multicentric
- Macroscopic features
- Flat
- Ulcerated
- Polypoid
- Verruciform
- Necrosis
- Hemorrhage
- Tumor deep borders
- Pushing
- Infiltrative
- Anatomic level of involvement: macroscopic and microscopic
- Glans
- Involving subepithelial connective tissue (lamina propria)
- Involving corpus spongiosum
- Involving tunica albuginea
- Involving corpus cavernosum
- Involving distal (penile) urethra
- Foreskin
- Involving subepithelial connective tissue (lamina propria)
- Involving tunica albuginea
- Involving corpus cavernosum
- Involving distal (penile) urethra
- Shaft
- Involves skin
- Involves dartos
- Involves Buck fascia
- Involves corpus spongiosum
- Involves corpus cavernosum
- Involves proximal urethra
- Glans
- Gross assessment of surgical resection margins
- Tumor type (invasive, noninvasive, in situ)
- Histological type
- Benign and precursor squamous lesions
- Condyloma acuminatum
- Squamous cell carcinoma precursors, HPV associated
- Penile intraepithelial neoplasia (PeIN), HPV associated
- Squamous cell tumors and precursors, HPV independent
- Differentiated penile intraepithelial neoplasia (PeIN), HPV independent
- Invasive epithelial tumors of the penis and scrotum
- Invasive squamous epithelial tumors
- HPV associated squamous cell carcinoma
- Basaloid squamous cell carcinoma
- Warty carcinoma
- Clear cell squamous cell carcinoma
- Lymphoepithelioma-like carcinoma
- Non-HPV associated squamous cell carcinoma
- Squamous cell carcinoma, usual type
- Verrucous (including carcinoma cuniculatum)
- Papillary squamous cell carcinoma
- Sarcomatoid squamous cell carcinoma
- Squamous cell carcinoma, NOS
- HPV associated squamous cell carcinoma
- Other epithelial tumors
- Adenosquamous carcinoma
- Mucoepidermoid carcinoma
- Paget disease, extramammary
- Other scrotal tumors
- Basal cell carcinoma of the scrotum
- Invasive squamous epithelial tumors
- Benign and precursor squamous lesions
- Histological grade
- Well differentiated (G1)
- Moderately differentiated (G2)
- Poorly differentiated (G3); % present (J Urol 2001;165:1138)
- Tumor thickness
- Lymphovascular invasion
- Perineural invasion
- Presence of associated lesions
- Squamous hyperplasia
- PeIN (differentiated, basaloid, warty, warty basaloid)
- Lichen sclerosus
- Depth of invasion (Mod Pathol 2001;14:963)
- From deepest malignant cell to highest overlying dermal papilla
- Note: if tumor replaces most of penis, measure tumor thickness from nonkeratinized tumor surface to the deepest point of invasion
- Prognostic index optional (Am J Surg Pathol 2009;33:1049)
Features to report by organization
Gross images
Contributed by Shaheed W. Hakim, M.D. and AFIP
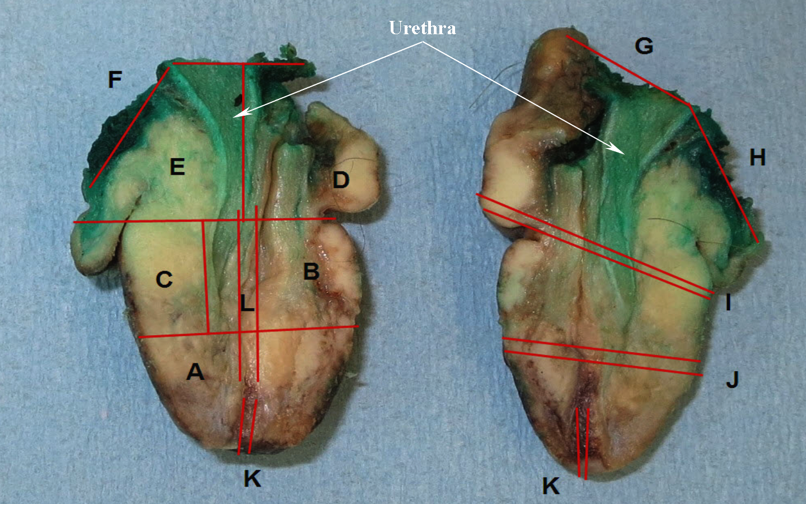
Mapped partial penectomy specimen
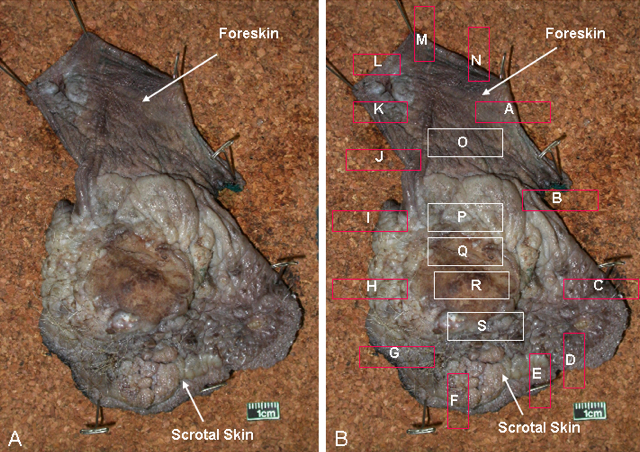
Foreskin

SCC involves corpora cavernosa
Partial penectomy specimen
Microscopic (histologic) images
Contributed by Shaheed W. Hakim, M.D. and AFIP
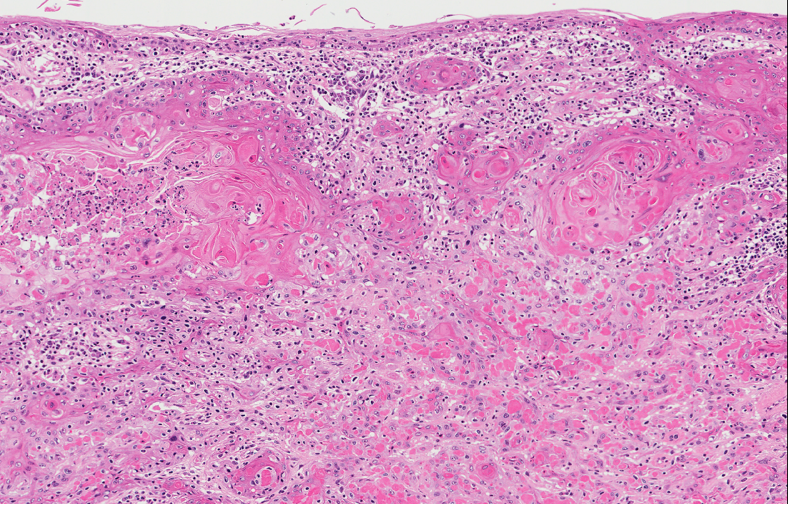
Grade 1
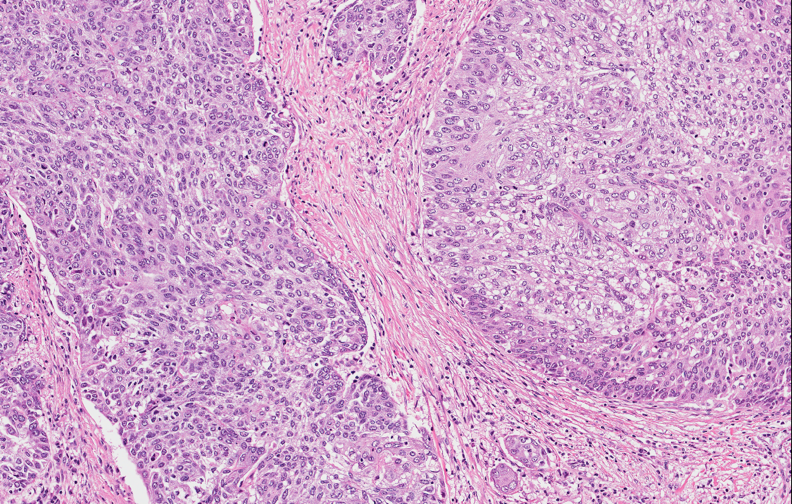
Grade 2, more disorganized growth

Grade 3
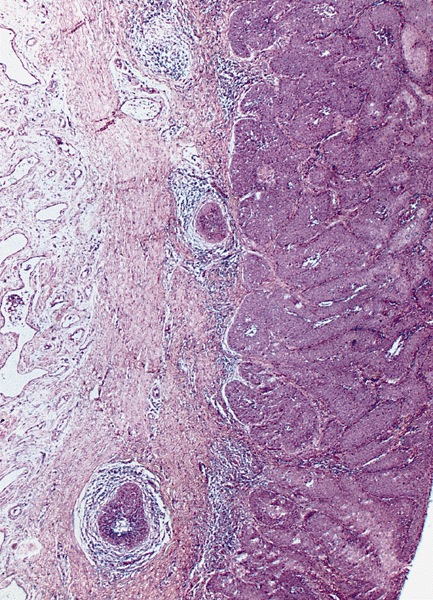
Lamina propria invasion
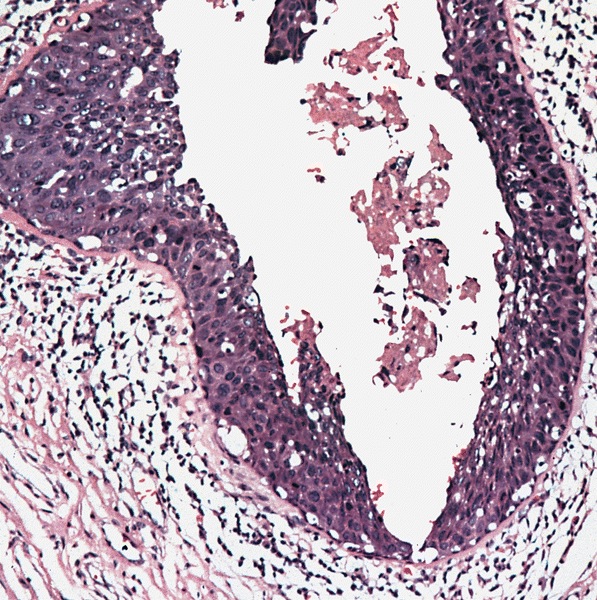
Urethral mucosal involvement
Sample gross description report
- Specimen labeled as the requisition and with the matching Co-Path tag as penis consists of a portion of penis and measures 5.5 cm in length by up to 4.3 x 3.5 cm in diameter.
- On the skin surface, a white ulcerated / granular mass in distal portion measuring up to 3.8 cm in length and involves up to 70% of luminal circumference, which is 1.5 cm from the proximal resection margin.
- The margin is inked with silver nitrate, skin margin inked green. On longitudinal sectioning, the tumor partially involves the distal 2 cm of the corpus cavernosum and spongiosum.
- The proximal shaft / urethral is free of tumor.
- Macroscopic digital photos taken and representative sections are submitted as follows:
- B1 - B4: the entire longitudinal section of specimen including proximal resection margin, into 4 quadrants, in toto
- B5 - B6: the remainder of proximal resection margin bisected in toto, en face
Diagrams / tables
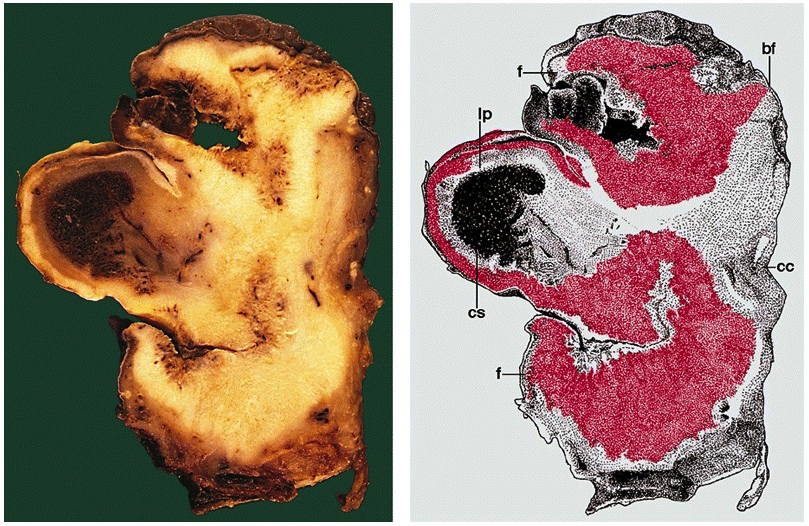
AFIP images
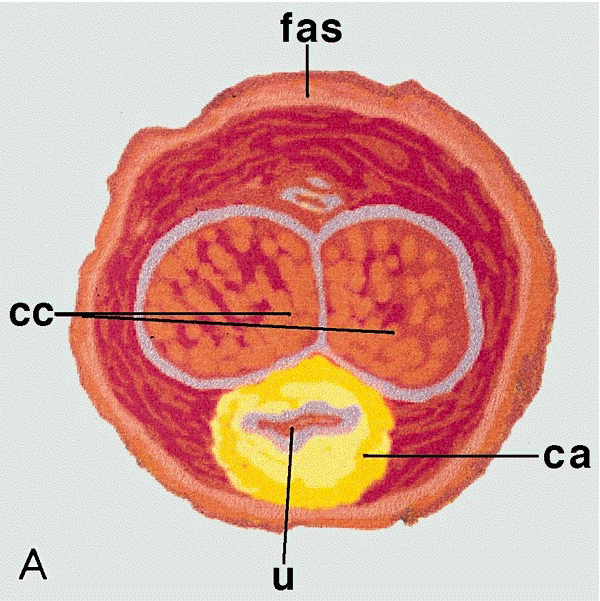
Periurethral corpus spongiosum involvement
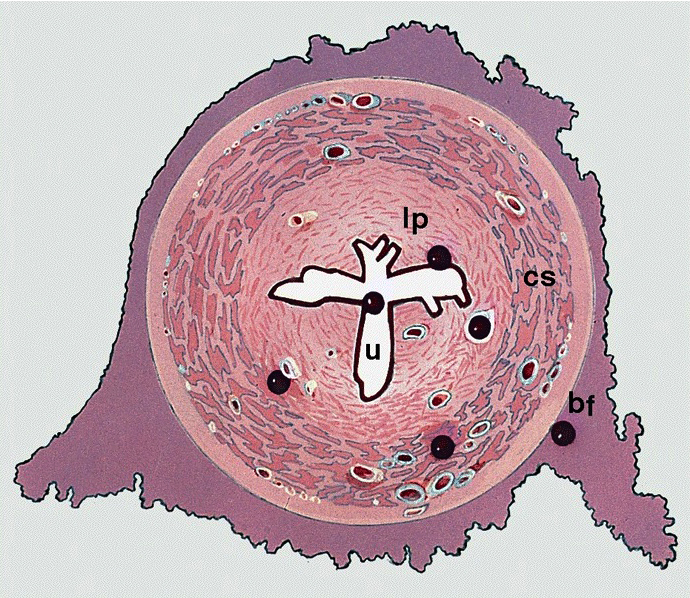
Possible sites of involvement
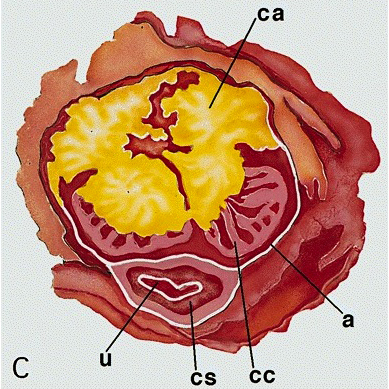
Tumor involvement in yellow
Images hosted on other servers:

Penis anatomy
Additional references
Board review style question #1
You are grossing a partial penectomy and note that the tumor affects multiple anatomical compartments. How would you approach gross evaluation of the specimen?
- Submit 2 - 3 representative sections per centimeter of specimen
- Submit at least 3 sections of each affected compartment
- Submit the section of the highest stage compartment
- Submit the specimen in toto
Board review style answer #1
B. Submit at least 3 sections of each affected compartment
Comment Here
Reference: Penis & scrotum - Grossing & features to report
Comment Here
Reference: Penis & scrotum - Grossing & features to report
