

Penis & scrotum
Infectious
Lymphogranuloma venereum
Authors: Alcides Chaux, M.D., Antonio L. Cubilla, M.D.

Last author update: 1 February 2010
Last staff update: 27 October 2020
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Lymphogranuloma venereum penis

Table of Contents
Definition / general | Epidemiology | Etiology | Clinical features | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Electron microscopy descriptionCite this page: Chaux A, Cubilla AL. Lymphogranuloma venereum. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/penscrotumLGV.html. Accessed December 25th, 2024.
Definition / general
- Sexually transmitted disease caused by Chlamydia trachomatis, an obligate intracellular parasite (Wikipedia: Lymphogranuloma Venereum [Accessed 29 March 2018], eMedicine: Lymphogranuloma Venereum (LGV) in Emergency Medicine [Accessed 29 March 2018], eMedicine: Dermatologic Manifestations of Lymphogranuloma Venereum [Accessed 29 March 2018])
Epidemiology
- Incidence highest in the tropics and subtropics, although outbreaks have occurred in West among men who have sex with men (MMWR Morb Mortal Wkly Rep 2004;53:985)
Etiology
- Sexually transmitted disease caused by Chlamydia trachomatis, an intracellular bacteria
- Different genovars produce specific clinical manifestations; i.e. types A, B, Ba and C cause trachoma, types LGV I, II and III (serovars L1, L2 and L3) cause LGV and types D to K cause oculogenital diseases
Clinical features
- Causes either inguinal, rectal or rarely pharyngeal syndrome
- Inguinal syndrome: painless papule or ulcer at inoculation site appears and rapidly disappears; followed 1 - 2 weeks later by enlarged inguinal lymph nodes with suppurative inflammation; followed by lymphocytic hyperplasia and massive plasma cell infiltration; then get stellate abscess; then suppurative granuloma with sinuses and tracts
- Rectal syndrome: most patients have proctitis, many with severe symptoms (Clin Infect Dis 2007;44:26)
- LGV infection may facilitate transmission of HIV
- Diagnosis: based primarily on clinical findings, can be supported by culture (30 - 50% sensitive), complement fixation (80% sensitive but does not distinguish different serovars) or PCR (limited availability)
Treatment
- Tetracycline (except during pregnancy) or erythromycin
Clinical images
Images hosted on other servers:

Sinus tract
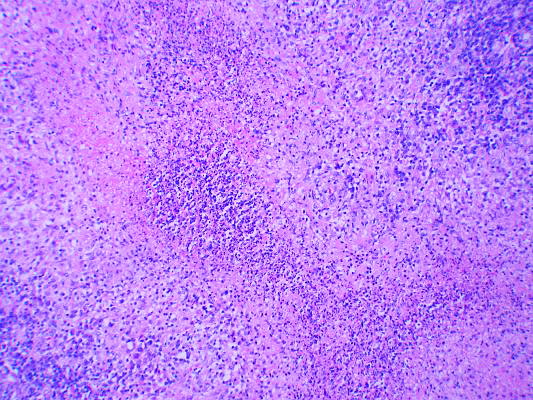
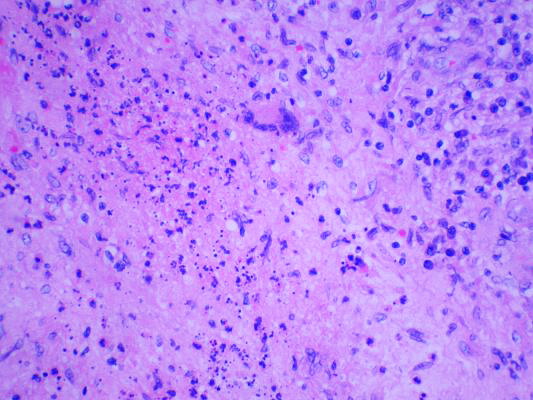
Microscopic (histologic) description
- Nonspecific features of ulceration and granulation tissue in dermis
- Suppurative inflammation of inguinal lymph nodes (neutrophils in necrotic foci); followed by lymphocytic hyperplasia and massive plasma cell infiltration; then stellate abscess from merging of microfoci of suppuration; then suppurative nonnecrotizing granuloma with epithelioid and multinucleated giant cells
- Sinuses and tracts can develop and fibrosis may ultimately replace most of lymph node architecture
- In lymph nodes, appear as intravacuolar organisms, associated with necrosis and suppuration
- Etiological agent is not apparent with routine stains
- Organisms are 0.2 - 2.0 micrometers in diameter, stain Gram negative with the Brown-Hopps tissue Gram stain, faintly blue with hematoxylin and eosin stain and black with Warthin-Starry stain (Mod Pathol 1995;8:924)
Microscopic (histologic) images
Images hosted on other servers:
Lymph nodes
Electron microscopy description
- Elementary and reticulate bodies and intermediate forms characteristic of the genus Chlamydia

