
Penis & scrotum
Other tumors
Myointimoma
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 16 May 2023
Last staff update: 12 August 2024
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Myointimoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Mohamed KS, Al-Quran SZ. Myointimoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/penismyointimoma.html. Accessed April 2nd, 2025.
Definition / general
- Benign myointimal proliferation with predilection to the corpus spongiosum of the glans penis
Essential features
- Benign mesenchymal neoplasm in the corpus spongiosum of the glans penis
- Intravascular proliferation of the vascular intimal cells
- Lesional cells stain with α smooth muscle actin but not desmin
Terminology
- Penile myointimoma
- Myointimoma of the penis
ICD coding
- ICD-O: 9137/0 - myointimoma
Epidemiology
- Rare tumor with ~28 cases reported in the literature (Am J Surg Pathol 2000;24:1524, Am J Surg Pathol 2007;31:1622, Int J Surg Pathol 2022 Aug 9 [Epub ahead of print])
- Previously described as intravascular leiomyoma, leiomyomatosis, late stage intravascular fasciitis, leiomyoma of the glans penis, solitary cutaneous myofibroma of the glans penis (Cancer 1970;25:1431, J Urol 2000;164:791, Am J Dermatopathol 1996;18:317)
- Wide age range (2 - 74 years old) (Am J Surg Pathol 2000;24:1524, Actas Dermosifiliogr 2009;100:511)
Sites
- Corpus spongiosum of the glans penis
Pathophysiology
- Intravascular proliferation from the intimal cells of the inner layer of the corpus spongiosum vasculature in the glans penis (Am J Surg Pathol 2000;24:1524)
Etiology
- Mesenchymal tumor unrelated to the status of circumcision, history of trauma or the presence of disease (Am J Surg Pathol 2000;24:1524, Actas Dermosifiliogr 2009;100:511)
Diagrams / tables
Images hosted on other servers:

Anatomy of corpus spongiosum in glans penis

Histology of intima
Clinical features
- Small, distinct, nonmobile, firm, painless nodule on the glans penis (J Am Acad Dermatol 2005;53:1084)
- Benign, rapidly growing lesions that remain stable for years, even after incomplete excision (Am J Surg Pathol 2000;24:1524)
Diagnosis
- Laboratory tests, including urine analysis and ultrasonic evaluation of the abdomen and the scrotum to exclude other potential causes (Pathol Int 2007;57:158, J Pediatr Surg Case Rep 2019;44:101189)
- Punch, incisional or excisional biopsy (Am J Surg Pathol 2000;24:1524)
Prognostic factors
- Benign outcome with no recurrence; spontaneous regression may occur (Am J Surg Pathol 2000;24:1524, Am J Surg Pathol 2007;31:1622, Int J Surg Pathol 2022 Aug 9 [Epub ahead of print)
Case reports
- 14 year old boy with a 1 cm nodule on the right side of his glans penis (J Cutan Pathol 2009;36:817)
- 49 year old man with a 12 month history of a palpable lesion involving the glans penis (Int J Impot Res 2021;33:583)
- 50 year old man with a nodule located in the glans penis (Pathol Int 2007;57:158)
Treatment
- Simple excision
Clinical images
Images hosted on other servers:

Nodule on the left side of glans penis
Gross description
- Firm white mass of 0.4 - 1.9 cm (Am J Surg Pathol 2007;31:1622, Am J Surg Pathol 2000;24:1524, J Am Acad Dermatol 2005;53:1084)
Gross images
Images hosted on other servers:

Excised nodule
Frozen section description
- Lesion may be present at margin of excision (Am J Surg Pathol 2007;31:1622)
Microscopic (histologic) description
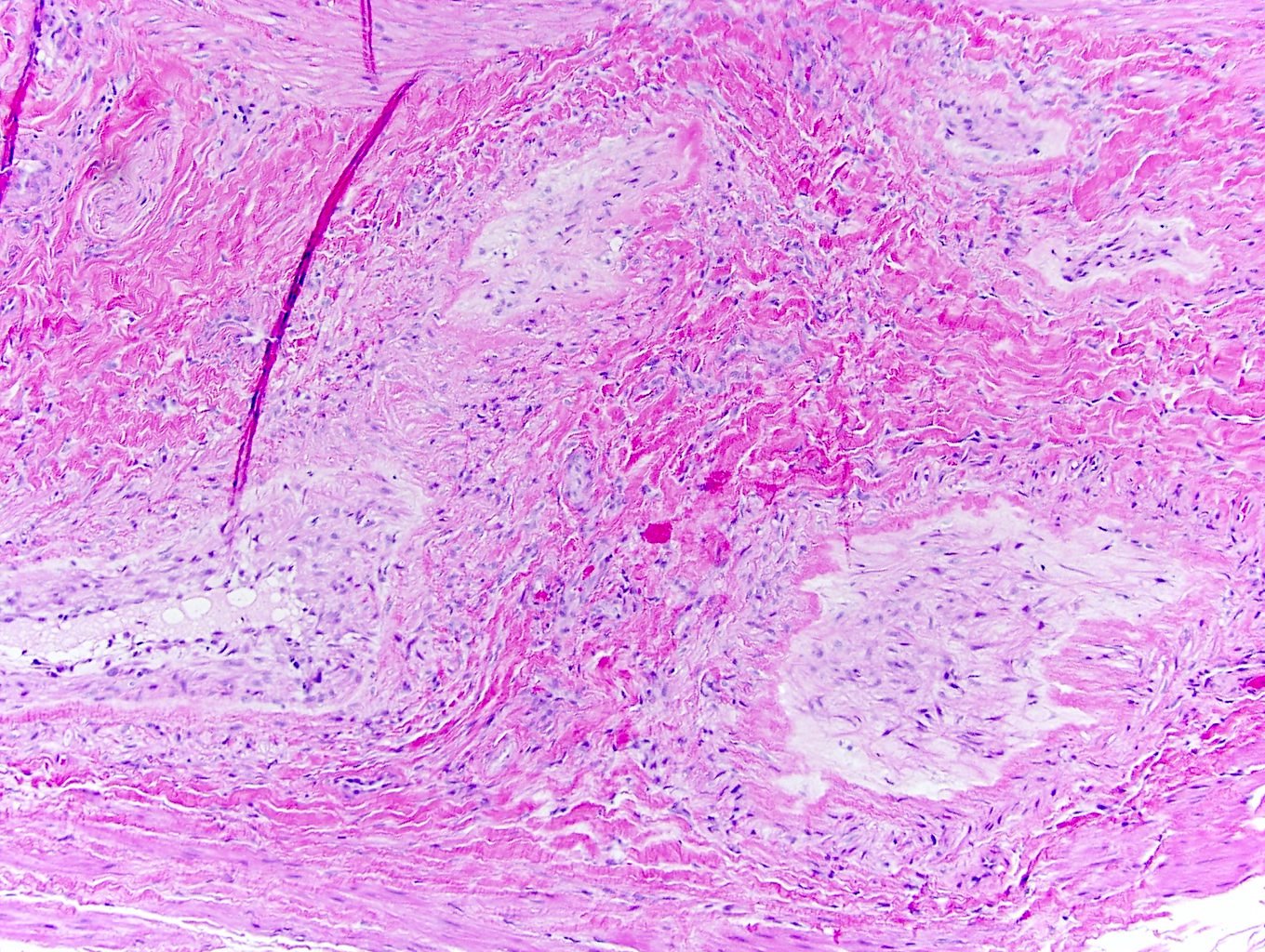
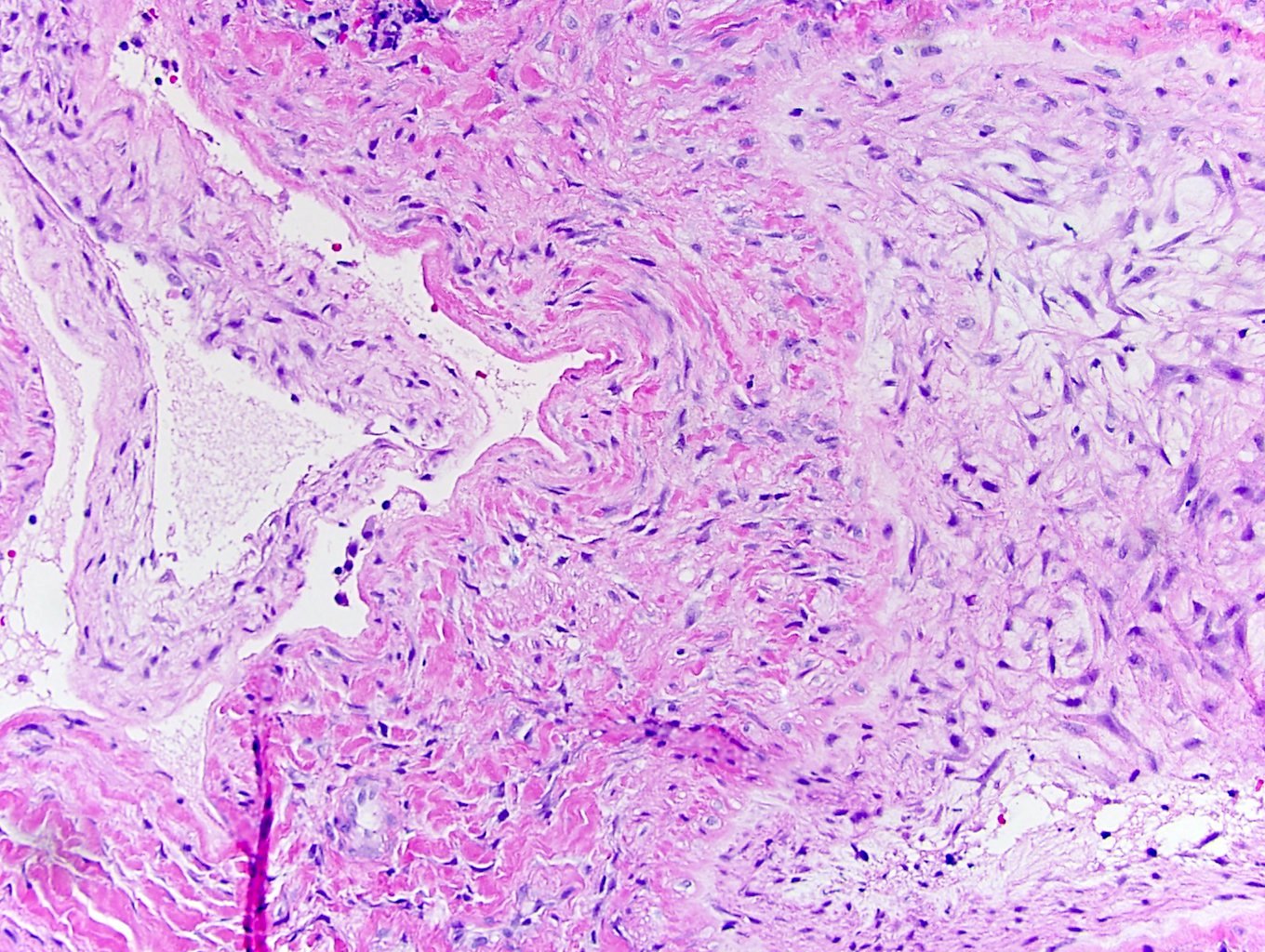
- Multinodular or plexiform pattern; composed of occlusive intravascular myointimal proliferation (Am J Surg Pathol 2000;24:1524)
- Nodules contain spindle or stellate shaped cells embedded in abundant fibromyxoid matrix or sometimes chondroid matrix (Am J Surg Pathol 2007;31:1622)
- Cells have long eosinophilic cytoplasmic processes, blunt ended nuclei, fine chromatin and juxtanuclear vacuoles
- Foci of degenerative changes appear as ghost cells (Am J Surg Pathol 2000;24:1524)
- No cytologic atypia, nuclear pleomorphism, prominent nucleoli or mitoses
- Residual smooth muscle bundles surrounding the tumor (Actas Dermosifiliogr 2009;100:511)
- Overlying skin may show slight hyperkeratosis (J Cutan Pathol 2009;36:817)
- No necrosis or significant inflammation
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D.

Plexiform architecture
Intravascular proliferation
Intravascular intimal proliferation

Fibromyxoid stroma

Bland myofibroblastic cells

SMA staining
Positive stains
Negative stains
- Desmin (shows the residual native smooth muscle of the vessel walls)
- CD34 / CD31 / factor VIII related antigen (highlight the penetrating capillaries and the residual endothelial cells)
- S100 protein
- AE1 / AE3 (Am J Surg Pathol 2000;24:1524)
- Verhoeff-van Gieson elastic histochemical stain (demonstrates the meshwork of the elastic fibers surrounding the nodules) (Am J Surg Pathol 2000;24:1524)
Sample pathology report
- Glans penis, excisional biopsy:
- Penile myointimoma (see comment)
- Comment: Sections show a plexiform vascular proliferation composed of spindle cells in a fibromyxoid background with occluded lumens. The neoplastic cells are α smooth muscle actin positive and desmin negative.
Differential diagnosis
- Plexiform fibrohistiocytic tumor:
- Not intravascular
- Common in extremities, trunk, head and neck
- Dimorphic population of cells:
- Epithelioid hemangioendothelioma:
- Myofibroma:
- Biphasic pattern of myoid nodules similar to myointimoma; however, there are hemangiopericytoma-like areas
- Can involve vessels but is not limited to intravascular lumina
- Intravascular fasciitis:
- May overlap
- Intralesional inflammatory cells, mucoid pools
- Nerve sheath tumor:
- Diffuse nuclear S100
- Leiomyoma:
Board review style question #1
The tumor in the image shown above is found in the penis corpus spongiosum. What is your diagnosis?
- Epithelioid hemangioendothelioma
- Leiomyoma
- Myointimoma
- Myofibroma
Board review style answer #1
