
Colon
Infectious colitis
Cryptosporidium parvum
Author: Elliot Weisenberg, M.D.

Last author update: 1 September 2015
Last staff update: 7 November 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Cryptosporidium parvum colitis


Table of Contents
Definition / general | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunohistochemistry & special stains | Differential diagnosis | Additional referencesCite this page: Weisenberg E. Cryptosporidium parvum. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/coloncryptosporidium.html. Accessed December 15th, 2024.
Definition / general
- Disease caused by infection with Cryptosporidium species, a protozoal parasite
- Traditionally considered a coccidian parasite but recent evidence suggests it may be a gregarine parasite (Wikipedia: Gregarinasina [Accessed 13 October 2023])
Epidemiology
- Cryptosporidium has a worldwide distribution (excepting Antarctica)
- Infection is usually person to person through the fecal-oral route, via ingestion of infective oocysts
- In some cases, zoonotic infection from sheep, cows, pigs, rodents, companion animals and other animals may occur
- The oocysts are hardy and are not killed by chlorination of drinking water
- Developing world: primarily affects children under age 5 and in most cases persistent diarrhea occurs that may be compounded by malnutrition; uncommon in adults
- Developed world:
- More common in children but not to the extent of the developing world
- Disease due to:
- Spread of pediatric cases in day care centers
- Travel to developed countries
- Spread in mental institutions
- Contaminated recreational water, including swimming pools, rivers, lakes, fountains
- Cryptosporidium is the most common cause of waterborne disease in recreational water
- Animal handlers
- Food borne spread
- Breakdowns in municipal water purification systems
- United States: 300,000 to 750,000 cases each year, more commonly in summer
- The largest known outbreak occurred in Milwaukee, Wisconsin in 1993, affecting an estimated 400,000 people, although this type of spread is now uncommon in the developed world
- Sexual transmission in men who have sex with men has been reported
- Disease is common in immunosuppressed patients especially AIDS patients with CD4 counts under 100
- There are over 20 species of cryptosporidium:
- C. hominis, the human genotype that primarily infects people and C. parvum, the bovine genotype, are the most important causes of human disease
- C. hominis was formerly known as C. parvum anthroponotic genotype 1
- C. meleagridis, C. Canis, C. felis, C. ubiquitum, C. cuniculus, C. suis, C. muris and other species are known to cause human disease
Sites
- Infection is most common in terminal ileum and proximal colon
- Disease also occurs in proximal small intestine, distal colon, gallbladder, bile ducts and pancreas
- Widespread disease generally occurs with severe immunosuppression and may involve respiratory tract
Pathophysiology
- Ingested oocysts excyst in stomach and small intestine, releasing 4 infective sporozoites that bind to intestinal epithelial cells
- The sporozoite becomes embedded in cell membrane in a parasitophorous vacuole
- Inside the vacuole, the sporozoite undergoes merogony (asexual reproduction) to become trophozoites
- The trophozoites divide to become type I meronts that mature, causing the parasitophorous vacuole to rupture, releasing motile merozoites that bind to epithelial cells and are engulfed
- Merogony is repeated or sexual differentiation occurs and merozoites differentiate into micro and macrogamonts
- The microgamonts release microgametes that penetrate cell walls of cells infected with macrogamonts
- The macrogamont and microgametes fuse and form zygotes
- The zygote undergoes meiosis to form an oocyst containing 4 sporozoites
- There are thin walled and thick walled forms of oocysts
- The thin walled form excysts in the host causing autoinfection while the thick walled oocyst is shed in the environment
- Infection causes enterocolitis or malabsorption
Clinical features
- The incubation period is usually about one week but may be from 1 to 30 days
- In immunocompetent individuals, acute but self-limited profuse watery diarrhea usually occurs
- In children in the developing world, persistent diarrhea occurs but most patients recover
- In immunosuppressed patients, chronic diarrhea occurs that is often debilitating
- In immunosuppressed patients, acalculous cholecystitis, sclerosing cholangitis, pancreatitis, biliary strictures and respiratory disease may occur
Diagnosis
- The diagnosis is usually made by visualization of cysts in stool using immunofluorescence or a modified acid fast stain
- It is important to communicate with the laboratory if there is a suspicion of cryptosporidiosis, as not all laboratories routinely test stool for Cryptosporidiium
- On occasion, the diagnosis is made on biopsy (see Microscopic (histologic) description)
Prognostic factors
- In immunocompetent adults, self limited diarrhea lasting one or two days is the rule
- If the CD4 count is under 100, chronic diarrhea occurs
- In HIV+ patients with CD4 counts under 50 and other immunosuppressed patients with markedly suppressed T cell function, fulminant diarrhea occurs
- In HIV+ patients with CD4 counts greater than 150 - 180, self-limited diarrhea usually occurs
- The ultimate prognosis in chronic and fulminant diarrhea in HIV+ patients is related to the success of therapy to reconstitute the immune system
- In the developing world, children under 5 usually suffer from persistent diarrhea that is often complicated by malnutrition
Case reports
- 2 year old boy with Cryptosporidium infection and celiac disease (J Postgrad Med 2012;58:160)
- 15 year old boy with several day history of profuse watery diarrhea after returning from swimming camp (Pritt: Creepy Dreadful Wonderful Parasites Blog - Case of the Week 543 [Accessed 13 October 2023])
- 43 year old man with cholangiocarcinoma complicating secondary sclerosing cholangitis from cryptosporidiosis (Int Arch Allergy Immunol 2012;159:204)
- 64 year old woman with Cryptosporidiosis causing severe persistent diarrhea (Indian J Med Paediatr Oncol 2014;35:93)
- Pulmonary cryptosporidiosis and immune reconstitution inflammatory syndrome (Int J STD AIDS 2013;24:333)
- Opportunistic parasite infections in patients receiving alemtuzumab (J Clin Pathol 2012;65:92)
Treatment
- Nitazoxanide reduces the severity of disease in immunocompetent patients and has been approved by the FDA for these patients; its effectiveness in immunocompromised patients is unclear although it is used in that setting
- Reconstitution of the immune system through highly active anti-viral therapy in AIDS patients or reduction in immunosuppression in other settings is important
Microscopic (histologic) description
- In tissue biopsies, 2 - 5 μm basophilic round bodies are seen protruding from the apex of enterocytes ("blue beads") within the cell membrane; highlight with Giemsa stain
- Cryptosporidium spp. oocysts measure 4 - 6 micrometers in diameter (Pritt: Creepy Dreadful Wonderful Parasites Blog - Answer to Case 543 [Accessed 13 October 2023])
- Villous atrophy, crypt hyperplasia, cryptitis and increased mixed inflammatory cells within the lamina propria may be seen
Microscopic (histologic) images
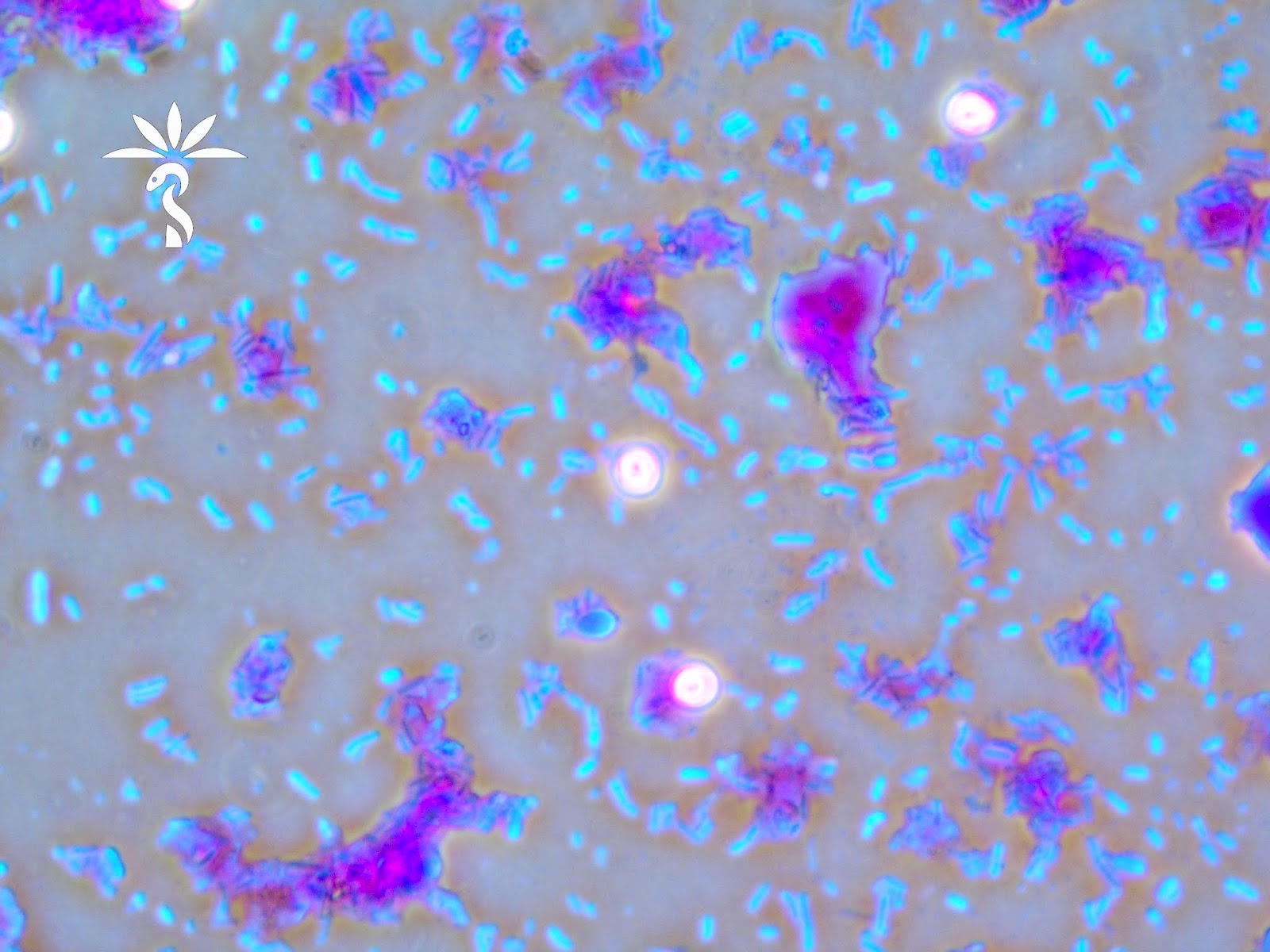
Contributed by Bobbi Pritt, M.D. and Institute of Tropical Medicine Antwerp
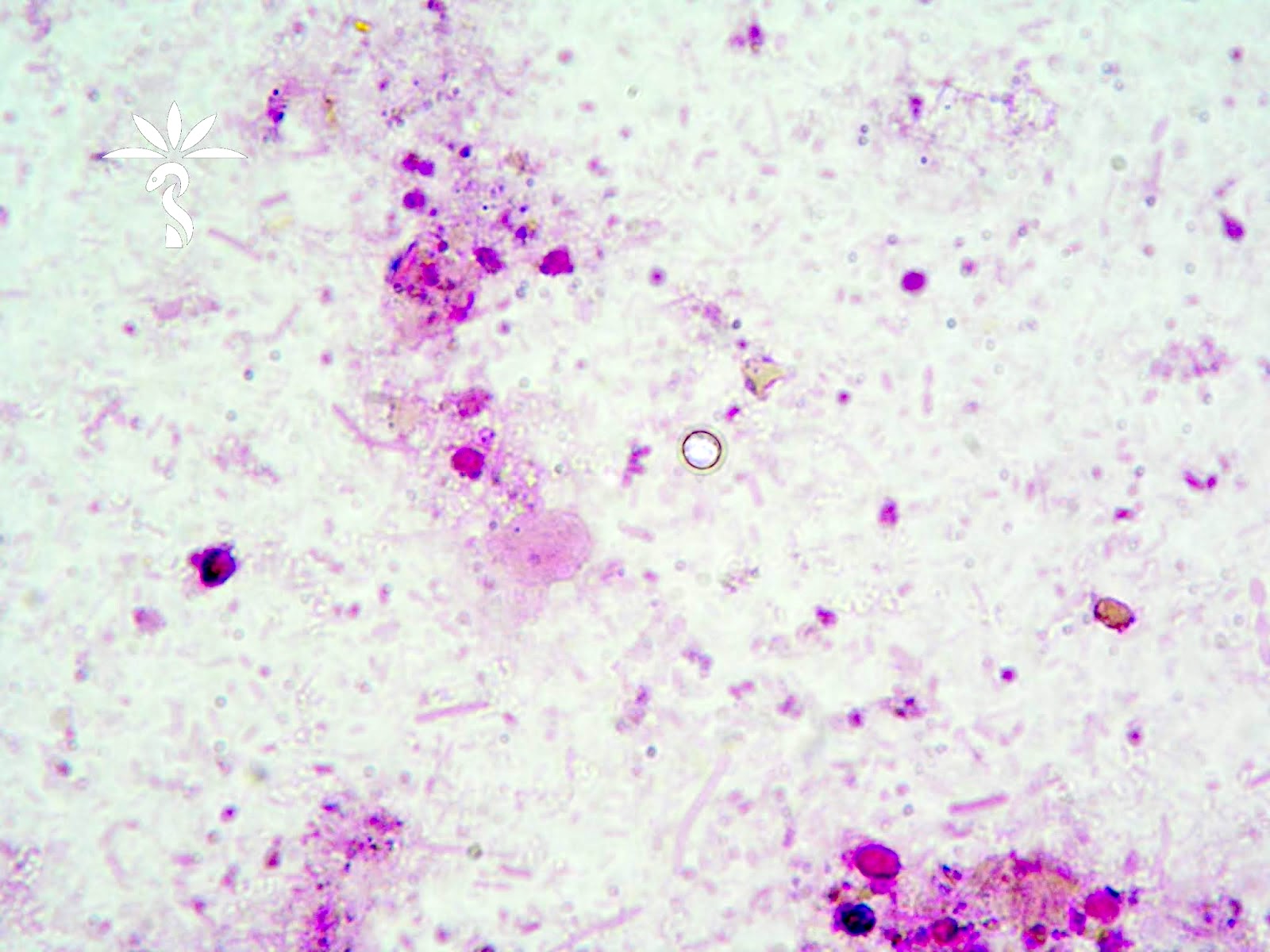
Negative fuchsine staining according to Heine
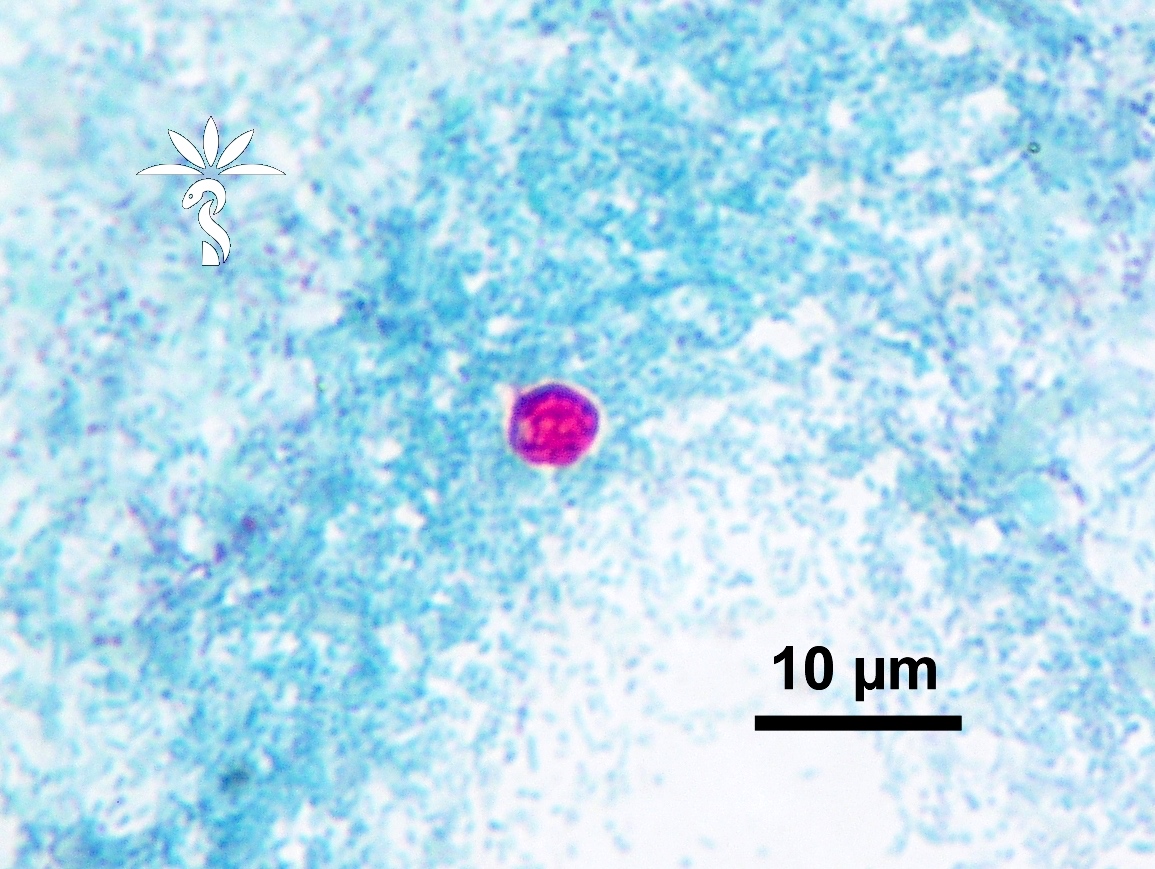
Ziehl-Neelsen staining
Images hosted on other servers:

Oocysts: auramine-rhodamine stain

Small blue organisms at luminal border

Modified acid-fast oocyst in stool
Immunohistochemistry & special stains
- Cryptosporidium spp. oocysts are red-pink using a modified acid fast stain (Pritt: Creepy Dreadful Wonderful Parasites Blog - Answer to Case 543 [Accessed 13 October 2023])
- Not all oocysts will reliably stain; some may appear as ghost cells or negative outlines
- Modified safranin stain can also be used and may more reliably stain the oocysts
Differential diagnosis
- Cyclospora:
- Oocysts are 8 μm, not 2 - 5 microns
- Isospora:
- Oocysts are 20 - 30 μm
- Microsporidium:
- An intracellular fungus that is not modified acid fast but may coinfect with Cryptosporidium
Additional references

