
Pancreas
Cystic and intraductal lesions
Serous cystadenoma
Authors: Pınar Bulutay, M.D., Volkan Adsay, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 21 April 2020
Last staff update: 1 September 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Serous cystadenoma pancreas


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Bulutay P, Adsay NV. Serous cystadenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasserous.html. Accessed April 1st, 2025.
Definition / general
- Benign pancreatic neoplasm of presumed ductal origin but of nonmucinous nature (Semin Diagn Pathol 2014;31:475, Am J Surg Pathol 2015;39:1597, Pancreatology 2009;9:182)
- Characterized by glycogen rich (nonmucinous; serous) epithelial cells with distinctive cytology showing uniform round nuclei with homogenous dense chromatin
- A prominent microvascular network hugging the epithelium as in other clear cell tumors with VHL pathway alterations (Am J Surg Pathol 2015;39:1597, Pancreatology 2009;9:182, Surgery 2012;152:S4)
- Microcystic pattern, which is the most common, creates a unique sponge-like configuration diagnostic of this tumor type
Essential features
- Rare, benign pancreatic neoplasm, more common in females and elderly patients (Semin Diagn Pathol 2014;31:475, Am J Surg Pathol 2015;39:1597, Pancreatology 2009;9:182)
- Characterized by numerous, small cystic spaces (synonym: microcystic adenoma) lined by distinctive glycogen rich epithelial cells (synonym: glycogen rich adenoma) with uniform round nuclei and a prominent microvascular network hugging the epithelium (Am J Surg Pathol 2015;39:1597, Pancreatology 2009;9:182, Surgery 2012;152:S4)
- Microcystic pattern, which is the most common, creates a unique sponge-like configuration diagnostic of this tumor type
Epidemiology
- Rare pancreatic tumor that often presents as a cystic mass occurring predominantly in women (F:M = 3:1)
- Mean age of patients is 58 years (Am J Surg Pathol 2015;39:1597)
Sites
- Can be found anywhere but more frequently in the tail of the pancreas
Etiology
- VHL pathway alterations (and can occur in VHL syndrome patients) but no known etiology
Clinical features
- Mean age: 58
- F:M = 3:1
- Frequently occurs sporadically but rarely arises in von Hippel-Lindau (VHL) syndrome
- VHL associated cases are sometimes patchy, multifocal (Pancreas 2012;41:380, Surgery 2012;152:1106)
- Often asymptomatic; rarely can be symptomatic due to obstruction of the biliary or GI tract (Am J Gastroenterol 2011;106:1521)
- Abdominal pain is occasionally attributed to this tumor
- Solid variant is often clinically misdiagnosed as pancreatic neuroendocrine tumor (PanNET)
- Macrocystic / oligocystic variants are often misdiagnosed as other cystic tumors
- Association with other tumors is common (13%), especially PanNET
- Typically, these minute cysts / glands are back to back and form a distinct mass but sometimes they can be dispersed in between native pancreatic elements
Radiology description
- CT typically demonstrates a demarcated, lobulated mass in the pancreas that is often interpreted as cystic (J Family Med Prim Care 2019;8:2744)
Prognostic factors
- Most serous tumors of the pancreas are benign with excellent prognosis (World J Surg 2003;27:319)
- Some of these tumors may attain a large size and push into (invade) the neighboring organs but overt malignant transformation and mortality is exceedingly uncommon (Dig Surg 2016;33:240)
- Synchronous or metachronous liver lesions are debated as to whether metastatic or multifocality (Am J Surg Pathol 2015;39:1597)
Case reports
- 17 year old girl with unilocular macrocystic serous cystadenoma of pancreas (Rev Med Brux 2017;38:39)
- 67 year old woman with serous cystic neoplasm at the pancreatic body and high grade PanIN lesions at the main and branch pancreatic ducts (Int J Surg Pathol 2018;26:551)
- 67 year old woman with macrocystic multilocular cystic lesion in the pancreatic head with proximal dilatation of Wirsung duct (J Gastrointest Surg 2019;23:176)
- 72 year old woman with hypervascular solid mass in the tail of the pancreas (Case Rep Surg 2016;2016:3730249)
- 75 year old woman with duodenal neuroendocrine tumor and pancreatic serous cystic neoplasm (Int J Surg Pathol 2018;26:551)
Treatment
- Watchful waiting because invariably benign (Zhonghua Wai Ke Za Zhi 2018;56:591)
- Surgical treatment should be proposed in a minority of patients, only for uncertain diagnosis remaining after complete workup, including CT scan, MRI and endoscopic ultrasound, significant and related symptoms or exceptionally, when concern for malignancy exists (Gut 2016;65:305)
- Rarely, local adhesion / infiltration into the adjacent lymph nodes or adjacent organs (colon, stomach) is seen in larger tumors
- Occurrence of similar tumors in the liver is being debated as whether synchronicity, multifocality or metastasis; behavior of those is also excellent
- True malignant degeneration or mortality due to this tumor is virtually nonexistent (exceedingly uncommon, dubious cases)
Gross description
- Favors the pancreatic body / tail region over the head / neck (ratio of 1.6:1) (Am J Surg Pathol 2015;39:1597)
- Well demarcated, large mass lesion (mean: 6 cm; range: 1 - 30 cm)
- Often has a central stellate scar
- Microcystic type: most common; characterized by a collection of innumerable microcysts (each within millimeters) creating the pathognomonic sponge-like configuration with gray to beige / cream color; rare large loculi measuring within centimeters are often seen dispersed within the lesion
- Oligocystic (macrocystic; megacystic) type: composed of fewer and larger loculi, with the overall picture closely resembling other megacystic tumors such as mucinous cystic neoplasms
- Solid type: homogenous, demarcated, beige-tan nodule with shiny gelatinous appearance; often mistaken as PanNETs clinically and grossly
- In the cystic types, the fluid is clear and watery; hemorrhage can occur
- Rarely multifocal or dispersed (especially VHL associated cases) (J Gastrointest Cancer 2010;41:197)
Gross images
Contributed by Pınar Bulutay, M.D.

Central scar

Thin fibrous septa
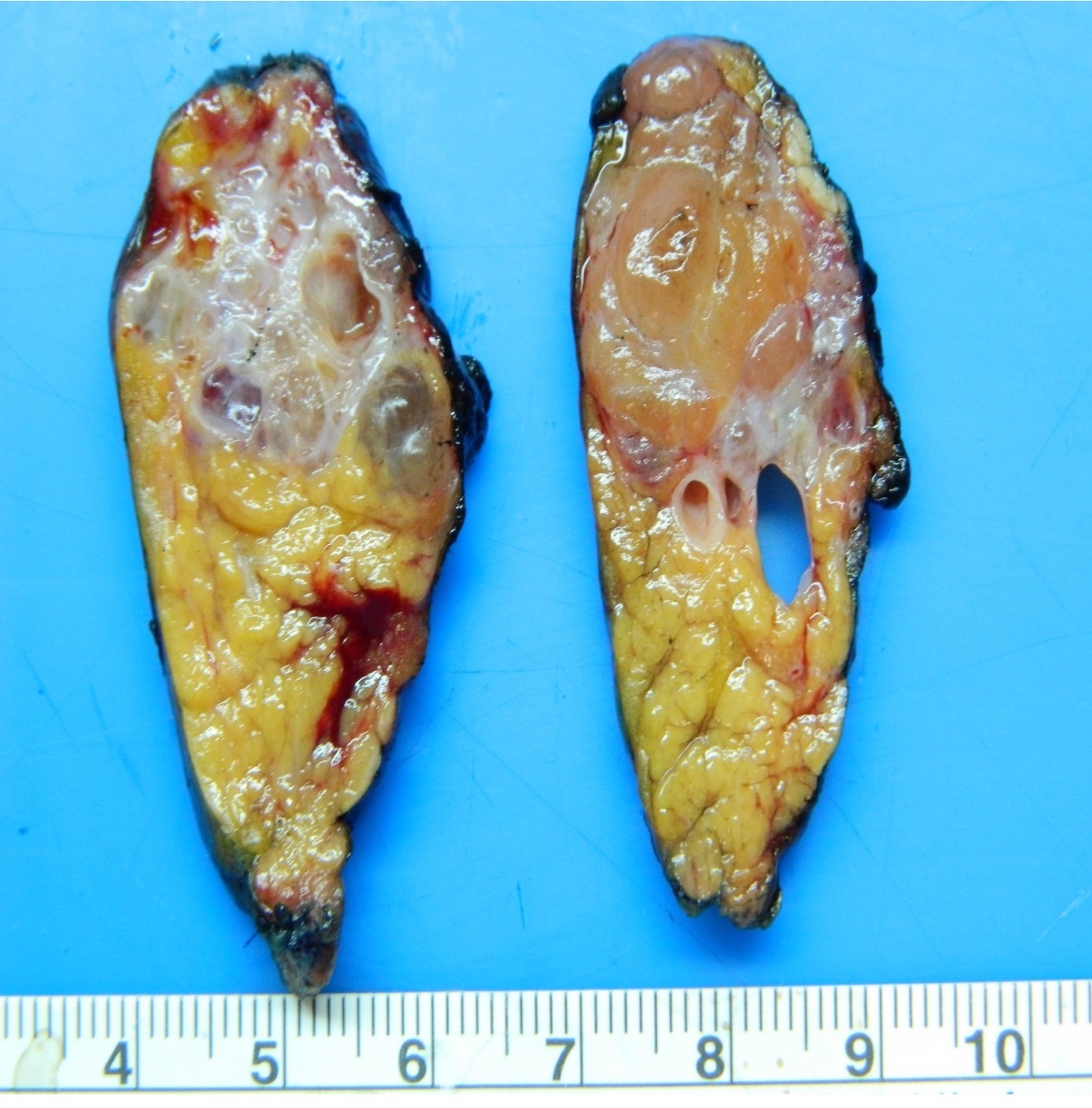
Macrocystic and solid variant
Images hosted on other servers:

Solid variant
Microscopic (histologic) description
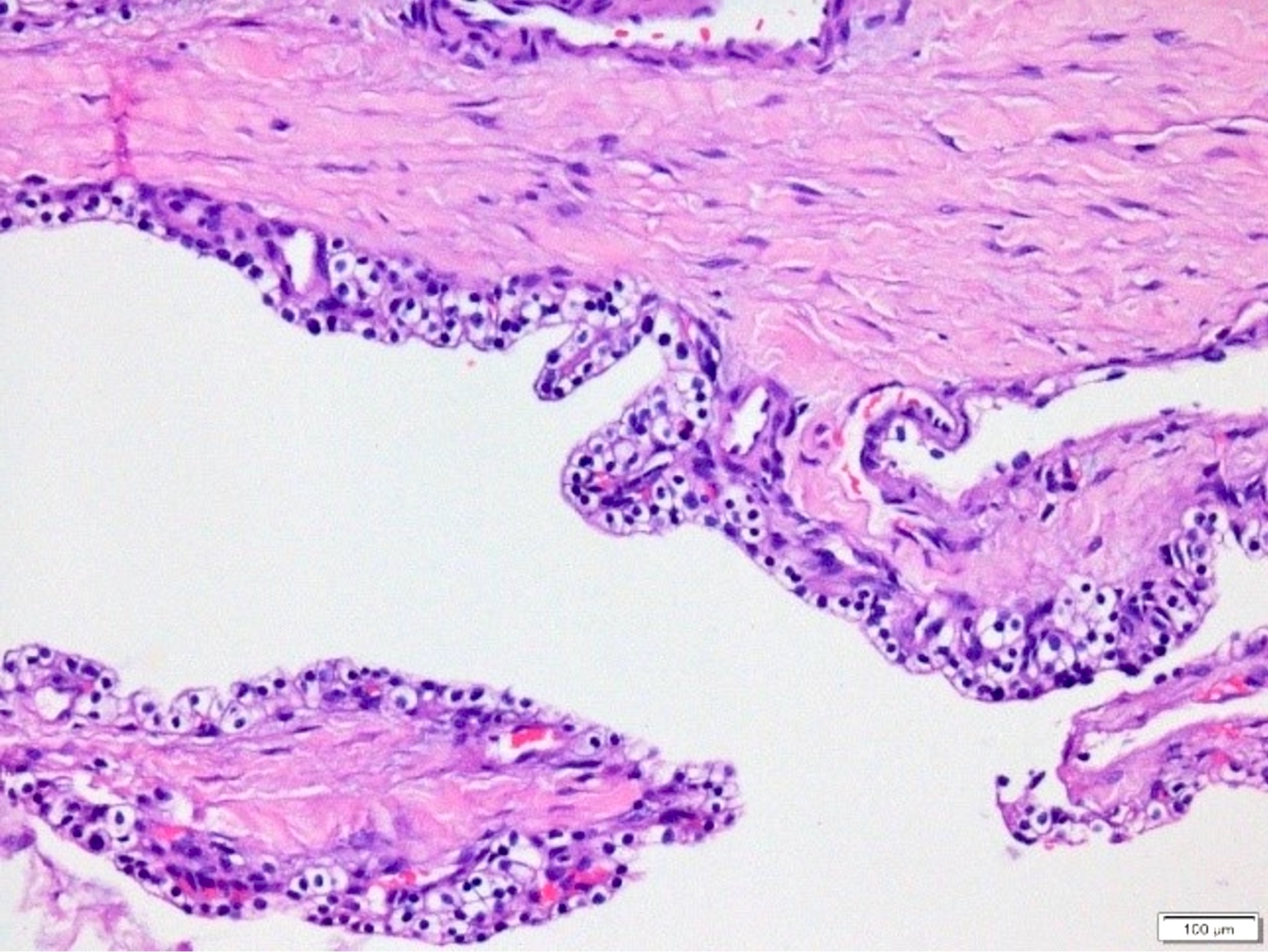
- Innumerable small, irregularly contoured tubular structures of variable shapes ranging from submillimeter to centimeters
- Cystic spaces lined by bland appearing cuboidal to low columnar epithelial cells with abundant clear, glycogen rich (PAS+, diastase sensitive) cytoplasm
- Nuclei are round and remarkably uniform with dense, homogenous chromatin and inconspicuous nucleoli
- Degenerative atypia leading to pleomorphic cells can be encountered as scattered cells
- Mitoses are typically absent
- Stroma ranges from edematous to fibrotic, myxoid or hyalinized with an intimately admixed capillary network; calcifications can be seen (Pancreatology 2009;9:182)
- Occasionally, the neoplastic cells form intraluminal minute papillary projections, usually without a fibrovascular stalk
- Some cases have more oncocytic cells with granular cytoplasm
- Solid variant is composed of tightly packed, back to back, uniform, small glands with only minimal or no lumen formation, showing the typical cytologic characteristics described above
Microscopic (histologic) images
Contributed by Pınar Bulutay, M.D.
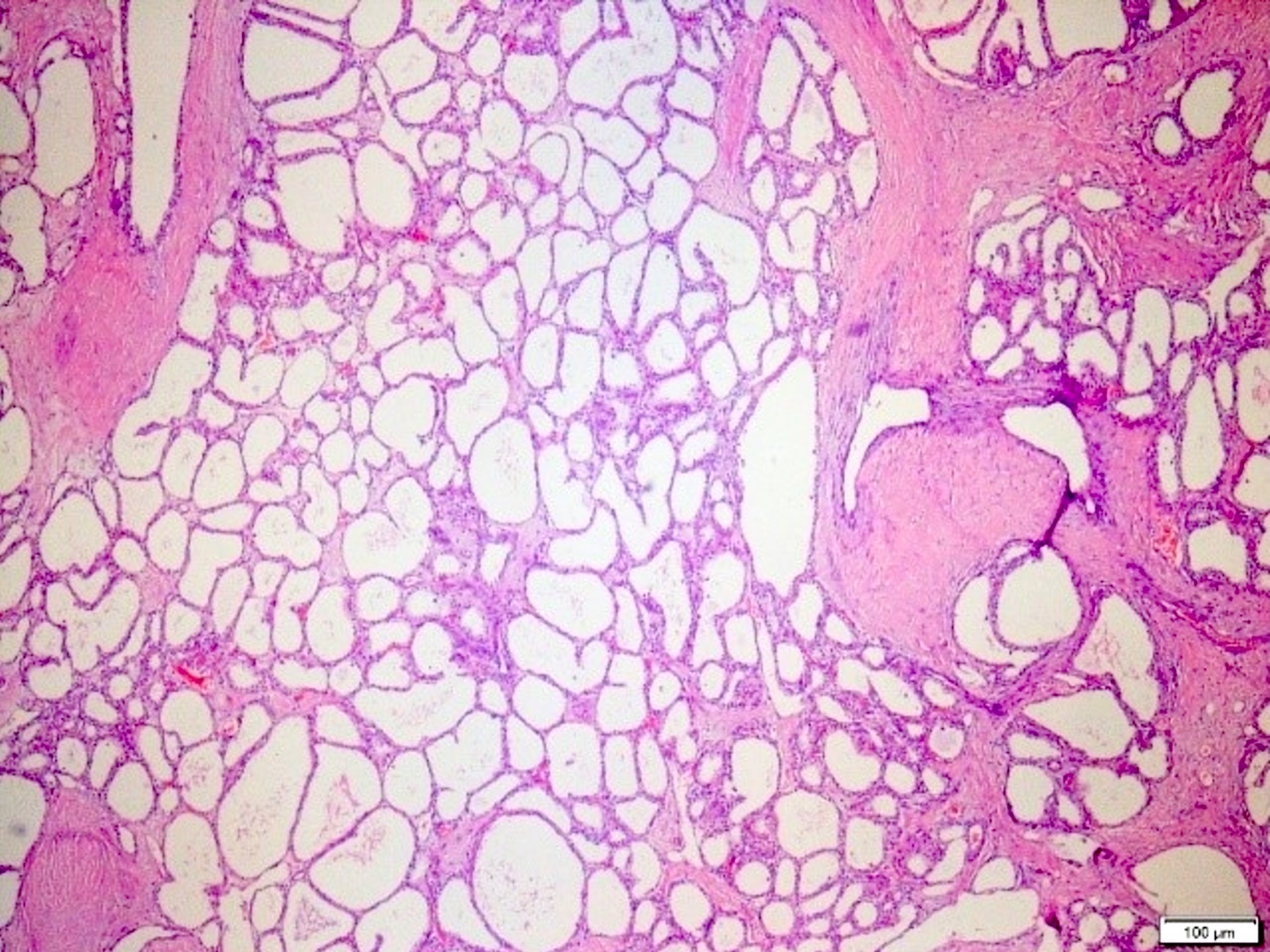
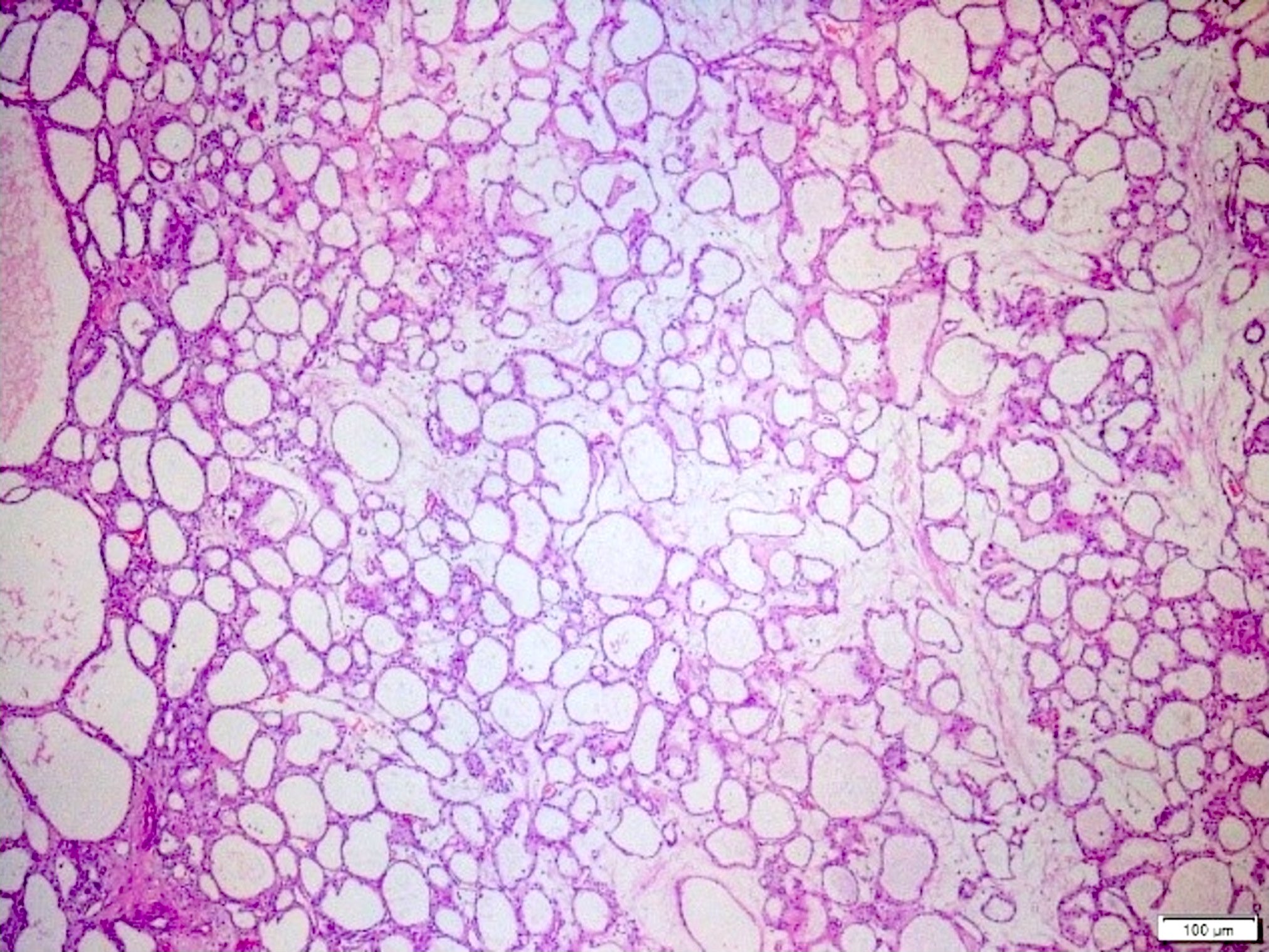

Innumerable submillimeter cysts
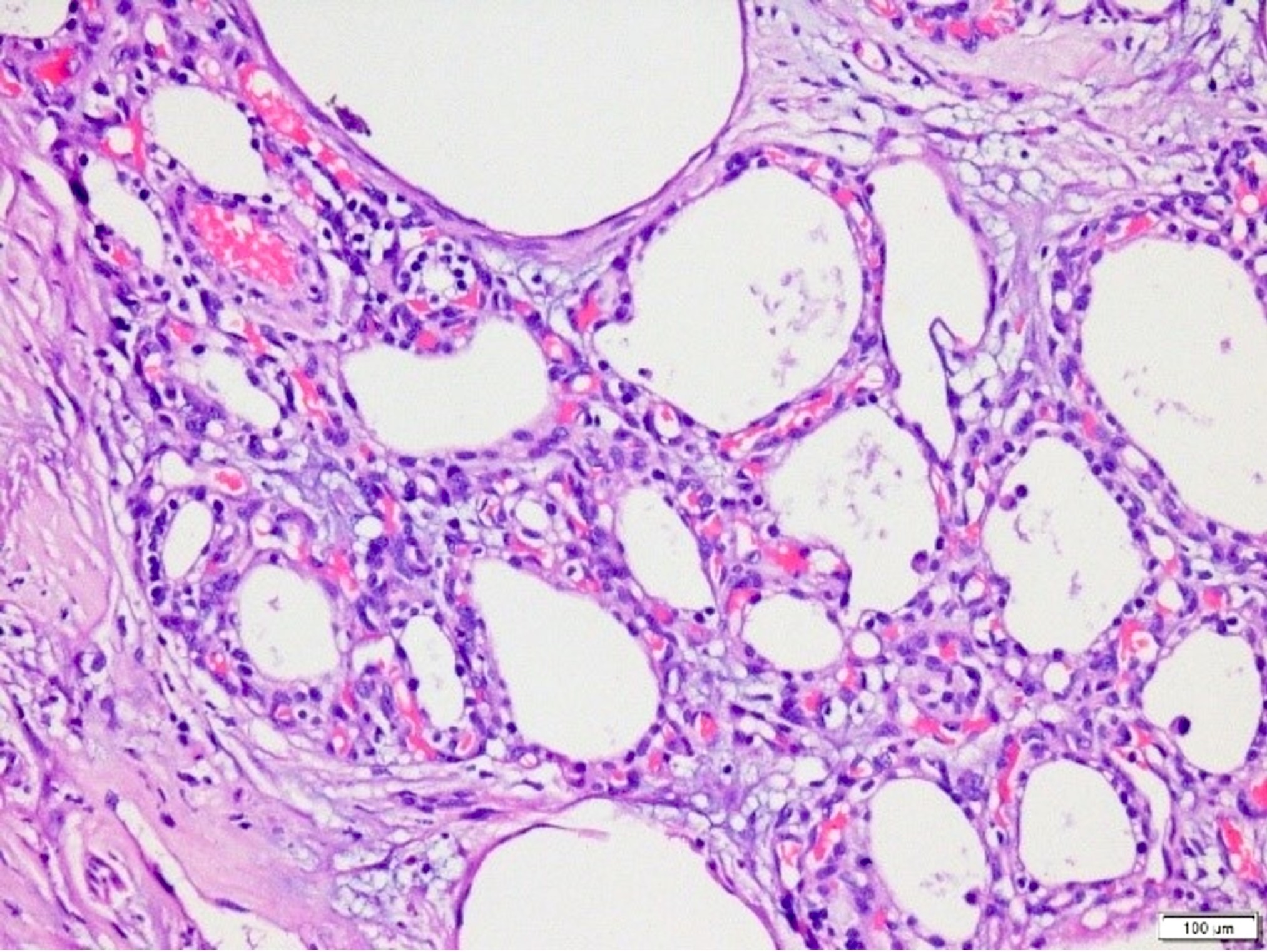
Prominent capillary network


Cellular details
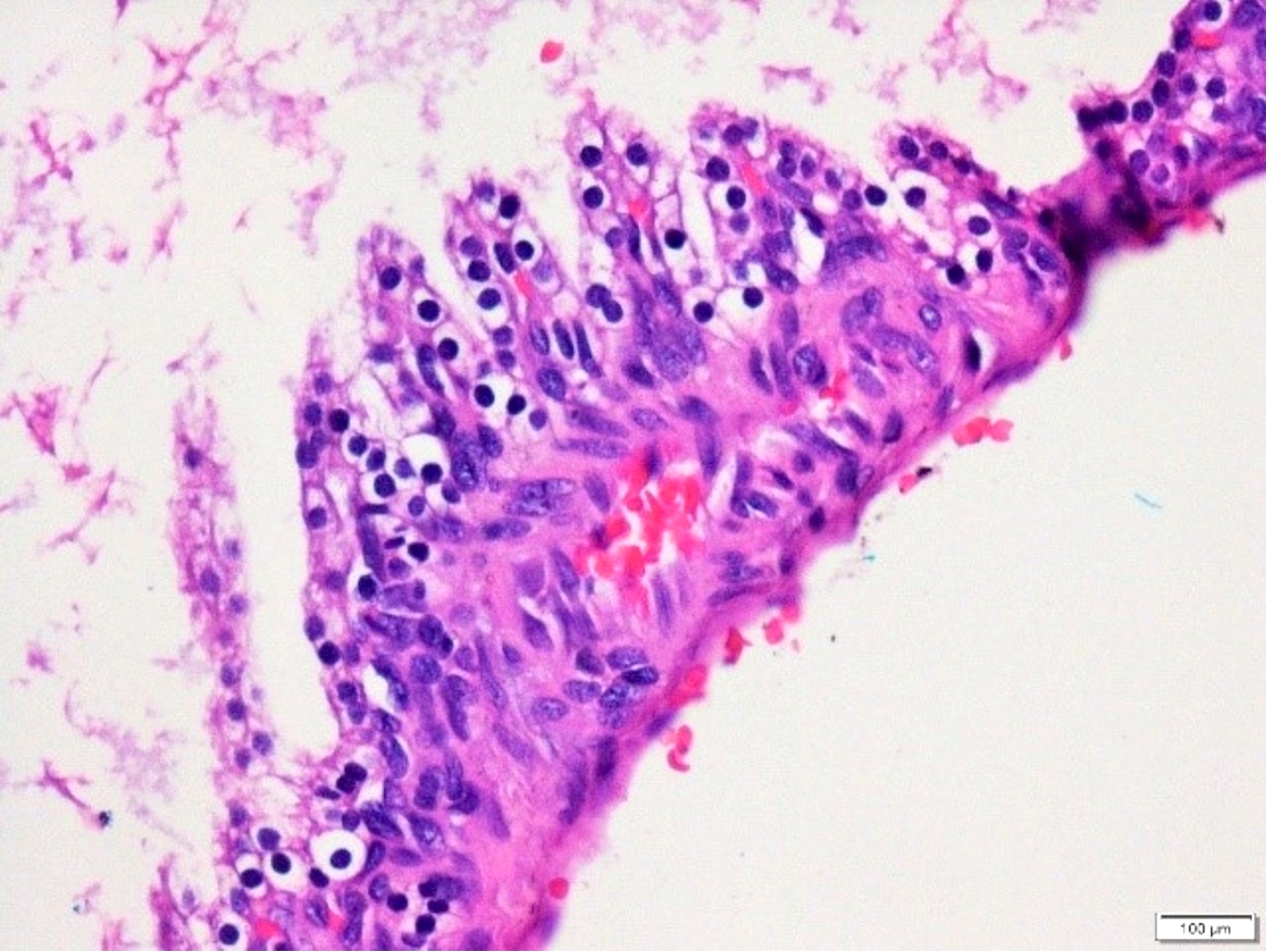
Intracystic papillary projections
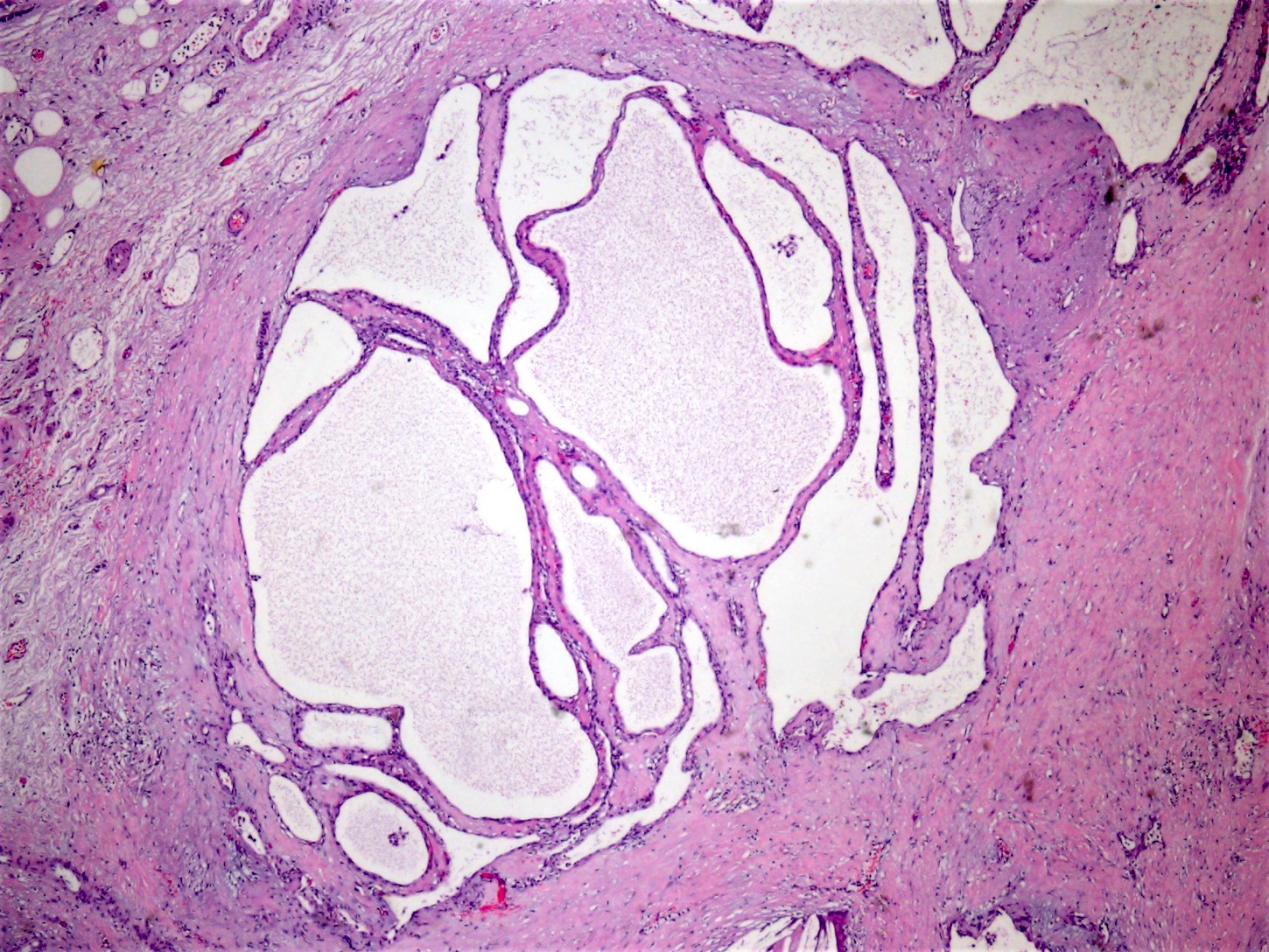
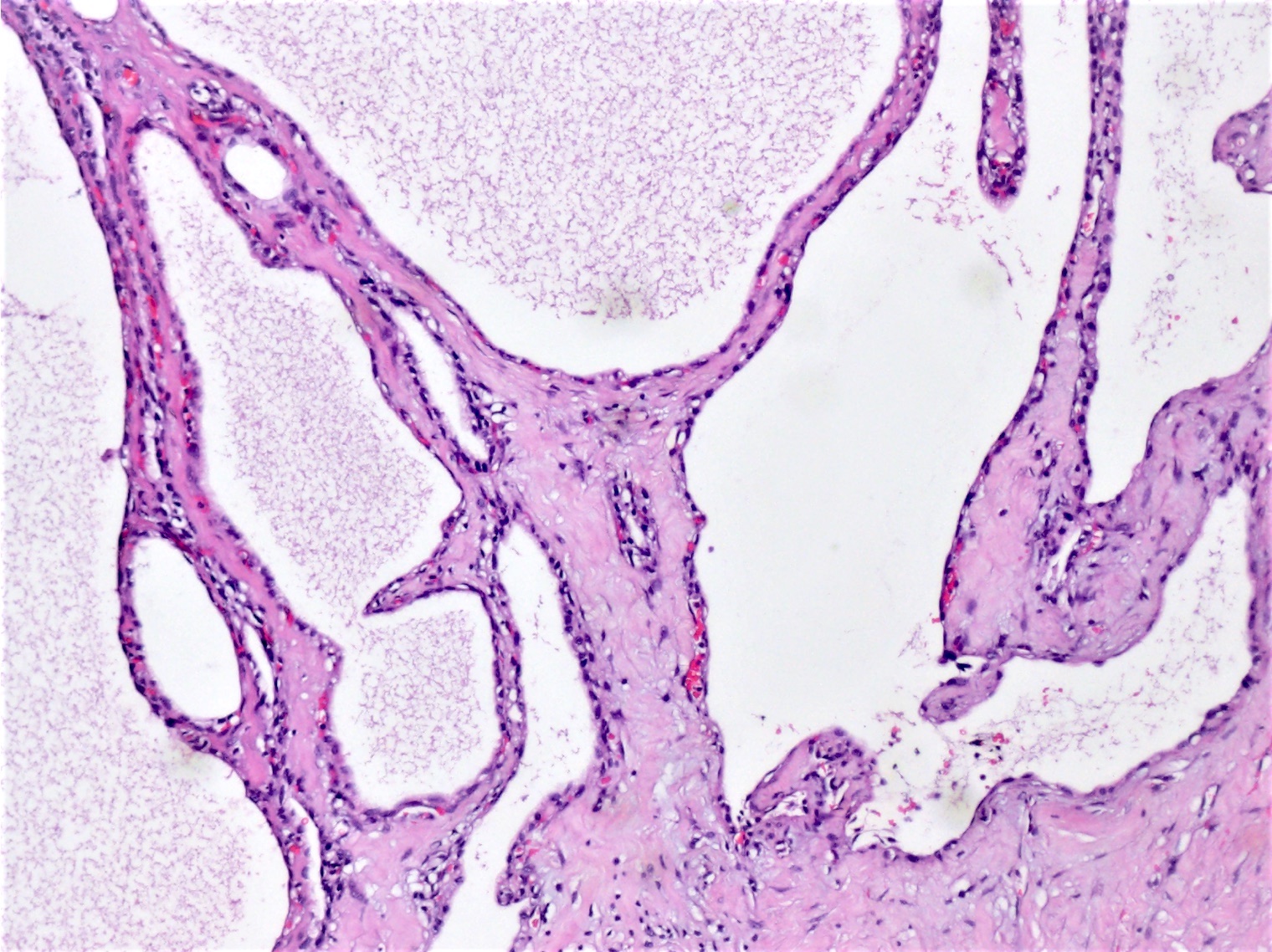
Macrocystic type
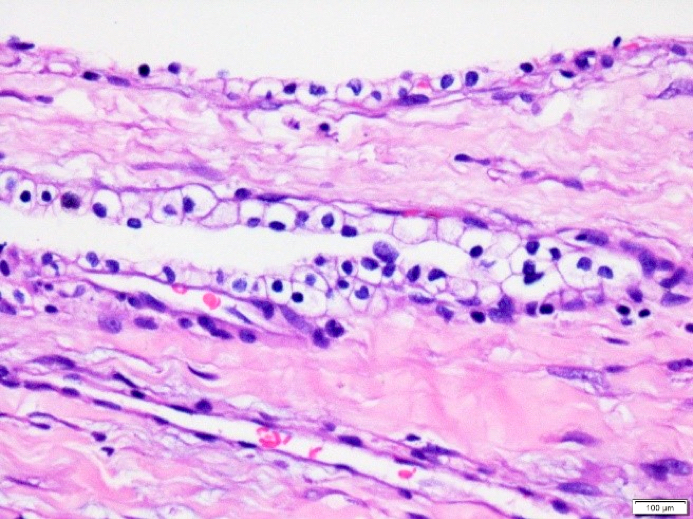
Cellular details, macrocystic type
Papillary projections, macrocystic type
Cytology description
- Scant amount of serous fluid
- Smears with very low cellularity, rich in protein; seldom diagnostic (Acta Cytol 2017;61:27)
- Epithelial cells arranged in flat sheets or singly (Cancer Cytopathol 2014;122:33)
- Stripped nuclei, clear cytoplasm
- Cytoplasmic borders well defined
- Round nuclei, evenly distributed chromatin
- Capillarization may be helpful
Positive stains
- Epithelial markers (keratins, EMA)
- MUC1 (often), MUC6 (common) (Am J Surg Pathol 2004;28:339)
- Inhibin A (Am J Surg Pathol 2004;28:339)
- GLUT1, HIF1α, CAIX, VEGF (Pancreatology 2009;9:182)
- Endothelial markers (highlight the rich periepithelial capillary network) (Pancreatology 2009;9:182)
Negative stains
Electron microscopy description
- Tumor tissue consists of cysts lined by columnar epithelium
- Tumor cells have intervening cell junctions and desmosomes
- Many small blood vessels in the subepithelial layer, the latter being intimately associated with the basal portions of epithelial tumor cells (Ultrastruct Pathol 2006;30:119)
- Organelle deficient and lack mucin, zymogen and dense glycogen granules; surface microvilli and cilia have rarely been reported (Pathology 2002;34:148)
- Myoepithelial cells have also rarely been reported (Ultrastruct Pathol 2006;30:119)
Molecular / cytogenetics description
- VHL gene alterations; loss of heterozygosity of the chromosome 3p region is most common in patients with VHL (Am J Pathol 2001;158:317)
- VHL gene alterations may also be detected in sporadic cases
Sample pathology report
- Partial distal pancreatectomy:
- Serous cystadenoma (see comment)
- Comment: There are multiple cystic spaces lined by a simple cuboidal to flattened epithelium with round, uniform nuclei and clear cytoplasm. Significant nuclear atypia or mitotic activity was not seen. There is some acellular fibrous tissue with a variable degree of hyalinization and edematous change in the stroma. Immunohistochemically the tumor cells are positive with EMA and MUC1 while negative for HMB45. The morphologic and immunohistochemical features are consistent with pancreatic serous cystadenoma.
Differential diagnosis
- Lymphangioma:
- Peripancreatic tissue, lymphoid aggregates between the cystic spaces attenuated cells with pale chromatin
- Cytokeratin-
- Metastatic renal cell carcinoma:
- Solid and acinar regions, prominent nuclear atypia, sinusoidal vascular pattern
- PAX8+
- Mucinous cystic neoplasm:
- Ovarian type stroma, mucinous or nonmucinous ductal cells (Am J Surg Pathol 2017;41:121)
- Clear cell (sugar) tumor (PEComa):
- Epitheloid spindle cells with cytoplasmic vacuolization
- HMB45+
Board review style question #1
Which of the following is true about pancreatic serous cystadenoma?
- It affects males and females equally
- It usually carries risk of malignant transformation
- Macrocystic type is the most frequent histologic subtype
- Some cases are associated with von Hippel-Lindau (VHL) syndrome
- Synaptophysin and chromogranin are positive for immunohistochemistry
Board review style answer #1
D. Some cases are associated with von Hippel-Lindau (VHL) syndrome. Pancreatic serous cystadenoma frequently occurs sporadically but rarely arises in von Hippel-Lindau (VHL) syndrome. VHL associated cases are sometimes patchy or multifocal.
Comment Here
Reference: Serous cystadenoma
Comment Here
Reference: Serous cystadenoma
Board review style question #2

A 47 year old woman presented with abdominal pain. CT images showed a 4 cm well circumscribed mass in the tail of the pancreas. Repeated fine needle aspiration biopsy did not yield specific diagnostic findings. The tumor was resected and showed a well demarcated tumor with innumerable tiny cystic spaces that created a sponge-like appearance, with beige-tan color and a central stellate scar. On microscopic examination, there were tightly packed small glandular / cystic elements of variable sizes lined by clear cells with nuclei that were small, round and uniform with dense homogeneous chromatin and devoid of mitotic activity (as shown in the picture). What is the most likely diagnosis and expected immunoprofile of this tumor?
- Mucinous cystic neoplasm: progesterone receptor in the stroma, mucicarmine, MUC5AC
- Pancreatic ductal adenocarcinoma: CEA, SMAD4 loss, p53
- Pancreatic serous cystadenoma: pancytokeratin, inhibin, GLUT1
- Solid pseudopapillary neoplasm: diffuse nuclear beta catenin, synaptophysin, CD10
- Solid serous adenoma: pancytokeratin, MUC6
Board review style answer #2
C. Pancreatic serous cystadenoma: pancytokeratin, inhibin, GLUT1
Comment Here
Reference: Serous cystadenoma
Comment Here
Reference: Serous cystadenoma
