

Pancreas
Neuroendocrine neoplasms
Mixed neuroendocrine nonneuroendocrine neoplasms (MiNENs)
Editorial Board Member: Wei Chen, M.D., Ph.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 7 April 2022
Last staff update: 7 April 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Mixed neuroendocrine non-neuroendocrine neoplasms pancreas

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ziebell J, Esnakula AK. Mixed neuroendocrine nonneuroendocrine neoplasms (MiNENs). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasmixed.html. Accessed November 26th, 2024.
Definition / general
- Pancreatic mixed neuroendocrine nonneuroendocrine neoplasms (MiNENs) are rare and heterogeneous malignancies characterized by histologically recognizable neuroendocrine (i.e., carcinoma and rarely, a well differentiated neuroendocrine tumor) and exocrine (usually ductal carcinoma, acinar carcinoma or both) components, each composing ≥ 30% of the neoplasm volume (Endocr Pathol 2016;27:284)
Essential features
- Histologically recognizable neuroendocrine and nonneuroendocrine components each comprise ≥ 30% of the neoplasm
- Neuroendocrine component is mostly a poorly differentiated neuroendocrine carcinoma (NEC); rarely a well differentiated neuroendocrine tumor (NET)
- Exocrine component can either be pancreatic ductal adenocarcinoma (PDAC) or acinar cell carcinoma (ACC); very rarely, both acinar and ductal carcinoma
- Neuroendocrine and nonneuroendocrine components are confirmed with immunohistochemistry (IHC)
- Poor prognosis
Terminology
- Subtypes: mixed ductal neuroendocrine carcinoma, mixed acinar neuroendocrine carcinoma, mixed acinar neuroendocrine ductal carcinoma
- Not recommended: composite carcinoid, mucin producing carcinoid, argentaffin cell adenocarcinoma, goblet cell carcinoid, adenocarcinoid, small cell undifferentiated carcinoma (Cancers (Basel) 2012;4:11)
ICD coding
- ICD-O: 8154/3 - mixed pancreatic endocrine and exocrine tumor, malignant
- ICD-10:
- ICD-11: 2C10.0 & XH8E54 - mixed neuroendocrine nonneuroendocrine neoplasm (MiNEN)
Epidemiology
- M = F
- Average age at presentation is 68 years (ranges from 21 - 84 years) (Am J Surg Pathol 1994;18:765)
- Mixed ductal neuroendocrine carcinomas comprise 0.5 - 2% of all ductal adenocarcinomas (Virchows Arch 2003;442:258)
- Mixed acinar neuroendocrine carcinomas comprise 15 - 20% of all acinar carcinomas (Am J Surg Pathol 2012;36:1782)
Sites
- Anywhere in the pancreas
- Mixed ductal neuroendocrine carcinomas are more common in the head of the pancreas
Pathophysiology
- Unclear
- May arise as the combination of 2 neoplastic clones or as the proliferation of 1 precursor cell with divergent differentiation; however, molecular and genetic studies point towards a monoclonal origin of both components (Endocr Pathol 2016;27:284, J Clin Med 2020;9:273)
- Behavior is thought to be driven by the neuroendocrine component (J Clin Med 2020;9:273)
Etiology
- Unknown
Clinical features
- Presentation is nonspecific and depends on the tumor size and degree of metastatic disease
Diagnosis
- Histomorphology and IHC on surgical resection specimens
- Biopsy may be used but is vulnerable to limited sampling and inadequate quantification of tumor components (Int J Surg Pathol 2017;25:585)
Laboratory
- Similar to pancreatic adenocarcinomas
- Increase in biliary and pancreatic enzymes may occur with obstruction of the common bile duct or main pancreatic duct (BMJ Case Rep 2020;13:e234855, Int J Surg Pathol 2017;25:585)
Radiology description
- Radiologic features of MiNENs can resemble either pancreatic adenocarcinoma or pancreatic neuroendocrine neoplasms on abdominal CT scan with contrast (Pancreatology 2021;21:224)
- Imaging findings similar to pancreatic adenocarcinomas (including hypodense hypoenhancing mass with ill defined border) are commonly seen with mixed ductal neuroendocrine carcinomas
- Imaging findings similar to pancreatic neuroendocrine neoplasms (including heterogeneously enhancing mass with or without cystic component and well defined margins) are commonly seen with mixed acinar neuroendocrine carcinomas
Radiology images
Images hosted on other servers:

MiNEN in the head of the pancreas on CT

MiNEN in pancreas head with portal vein narrowing on CT
Prognostic factors
- Tumor size and resectability are the most important prognostic factors
- Mixed ductal neuroendocrine carcinoma: 5 year survival rates are similar to PDAC and NEC
- Mixed acinar neuroendocrine carcinoma: similar to 5 year survival rate (36 - 72%) of pure acinar cell carcinoma (Am J Surg Pathol 2012;36:1782)
- Recent study demonstrated that acinar MiNEN patients have a worse prognosis than ACC and NEC (Pancreatology 2021;21:224)
- A poorly differentiated neuroendocrine carcinoma component comprising > 50% of the tumor is associated with distant metastasis and poor prognosis (J Chin Med Assoc 2015;78:454)
Case reports
- 33 year old man with uncinate mass and a 66 year old man with pancreatic tail mass (Diagn Cytopathol 2018;46:971)
- 49 year old Indian man presented with constant, dull, aching epigastric pain (Int J Surg Case Rep 2021;88:106524)
- 61 year old man was admitted to the hospital with incidental pancreatitis (Asian J Surg 2022;45:520)
- 63 year old man presented with hyperglycemia (Surg Case Rep 2016;2:133)
- 70 year old man who was asymptomatic underwent a FNA after an incidental pancreatic mass was found on ultrasound (Clin J Gastroenterol 2022;15:244)
- 81 year old man presented with painful progressive jaundice for 1 month (BMJ Case Rep 2020;13:e234855)
Treatment
- No clear treatment guidelines due to rarity of tumors
- Some recommend treatment based on the neuroendocrine component since it seems to be the most aggressive (Neuroendocrinology 2016;103:186, J Clin Med 2020;9:273)
- Radical surgical resection with or without adjuvant chemotherapy for localized cases
- Chemotherapy (platinum based) for extensively metastatic cases
Gross description
- Mixed ductal neuroendocrine carcinomas are solid tumors with infiltrative margins similar to ductal adenocarcinomas
- Mixed acinar neuroendocrine carcinomas are usually nodular, fleshy, hemorrhagic and necrotic, similar to neuroendocrine carcinoma and acinar cell carcinoma (Am J Surg Pathol 1994;18:765)
Gross images
Images hosted on other servers:

Mixed ductal neuroendocrine carcinoma
Microscopic (histologic) description
- Neuroendocrine and nonneuroendocrine components are intimately intermixed and sometimes can only be differentiated with IHC (Int J Surg Pathol 2017;25:585)
- Both components must comprise ≥ 30% of the neoplasm (Endocr Pathol 2016;27:284)
- Neuroendocrine component can either be poorly differentiated neuroendocrine carcinoma or well differentiated neuroendocrine tumor (Surg Pathol Clin 2020;13:377)
- Poorly differentiated neuroendocrine carcinoma (90% of MiNENs) (J Clin Med 2020;9:273):
- Poorly formed trabeculae and nests or diffuse sheets of cells
- Can be large cell types (moderate to abundant eosinophilic cytoplasm, fine to vesicular chromatin and prominent nucleoli) or small cell types (high nuclear to cytoplasmic ratio, hyperchromatic nuclei with fine chromatin, inconspicuous nucleoli)
- Multiple foci of necrosis or geographic necrosis and numerous apoptotic bodies
- Mitoses are frequent
- Perineural and vascular invasion is common
- Well differentiated neuroendocrine tumor:
- Nested, lobular or trabecular architecture composed of monomorphic, regularly arranged cells
- Nuclei with stippled (salt and pepper) chromatin
- Inconspicuous nucleoli
- Poorly differentiated neuroendocrine carcinoma (90% of MiNENs) (J Clin Med 2020;9:273):
- Ductal adenocarcinoma component:
- Identical to conventional pancreatic ductal adenocarcinoma
- Grade ranges from well differentiated to poorly differentiated adenocarcinoma
- Infiltrating, well to poorly formed glandular, cribriform, solid or trabecular structures surrounded by desmoplastic stroma
- Mucin production
- Perineural and vascular invasion are common
- Acinar cell carcinoma component:
- Identical to acinar cell carcinoma
- Highly cellular
- Cystic, acinar or glandular architecture
- Abundant eosinophilic granular cytoplasm
- Monomorphic nuclei with a single prominent nucleolus
- Perineural and vascular invasion are common
Microscopic (histologic) images
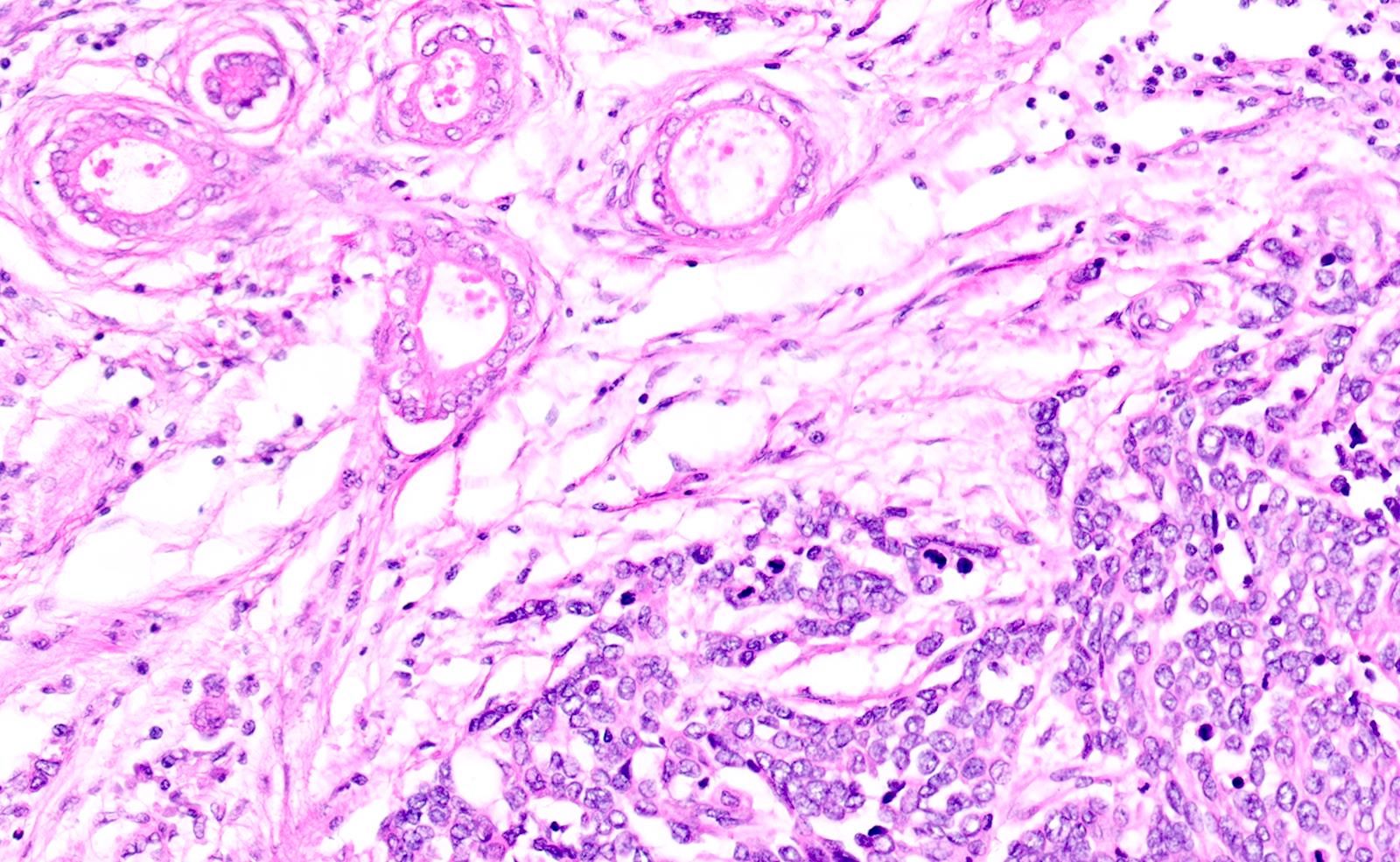
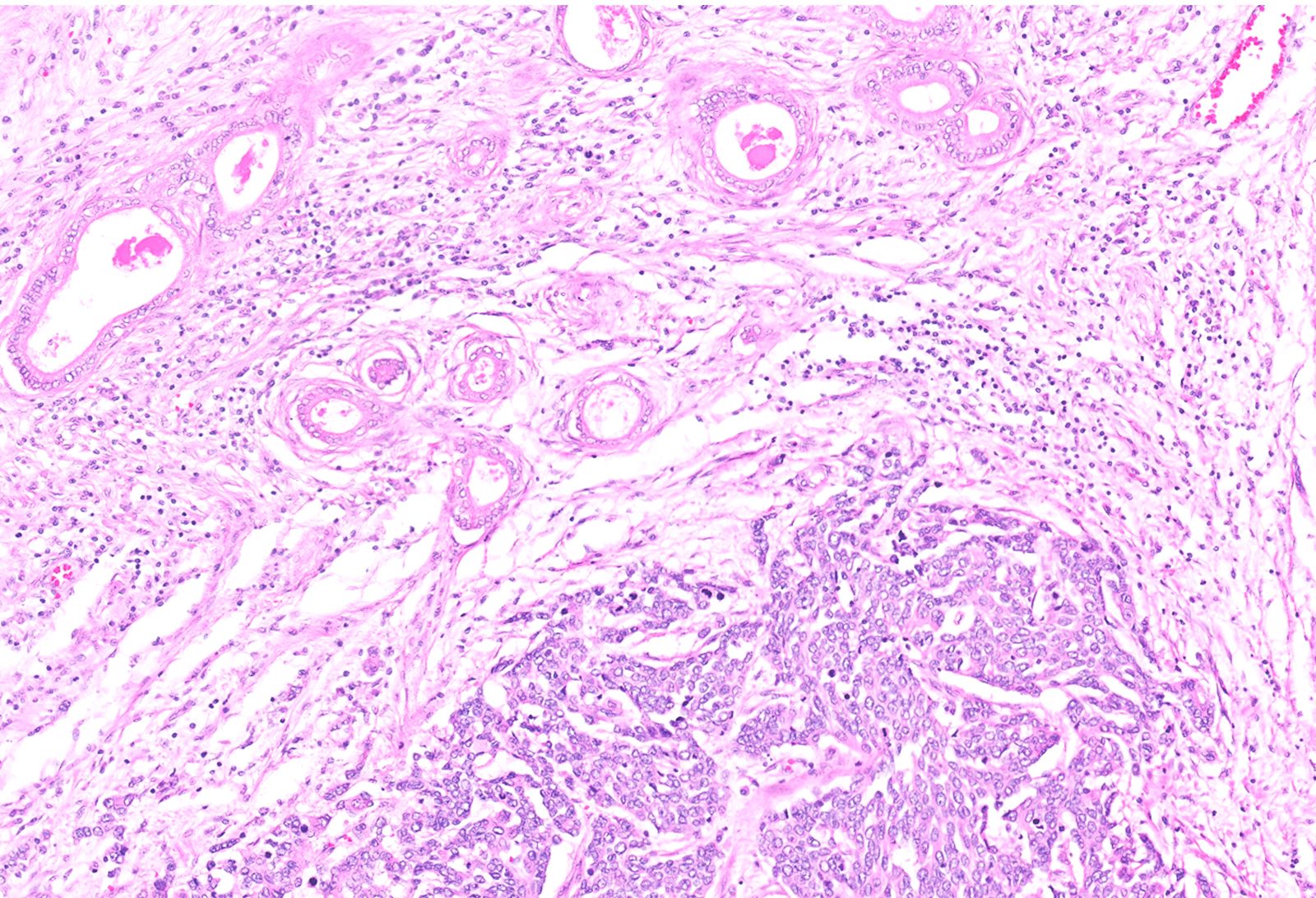
Contributed by Jennifer Ziebell, M.D. and Ashwini Esnakula, M.D., M.S.
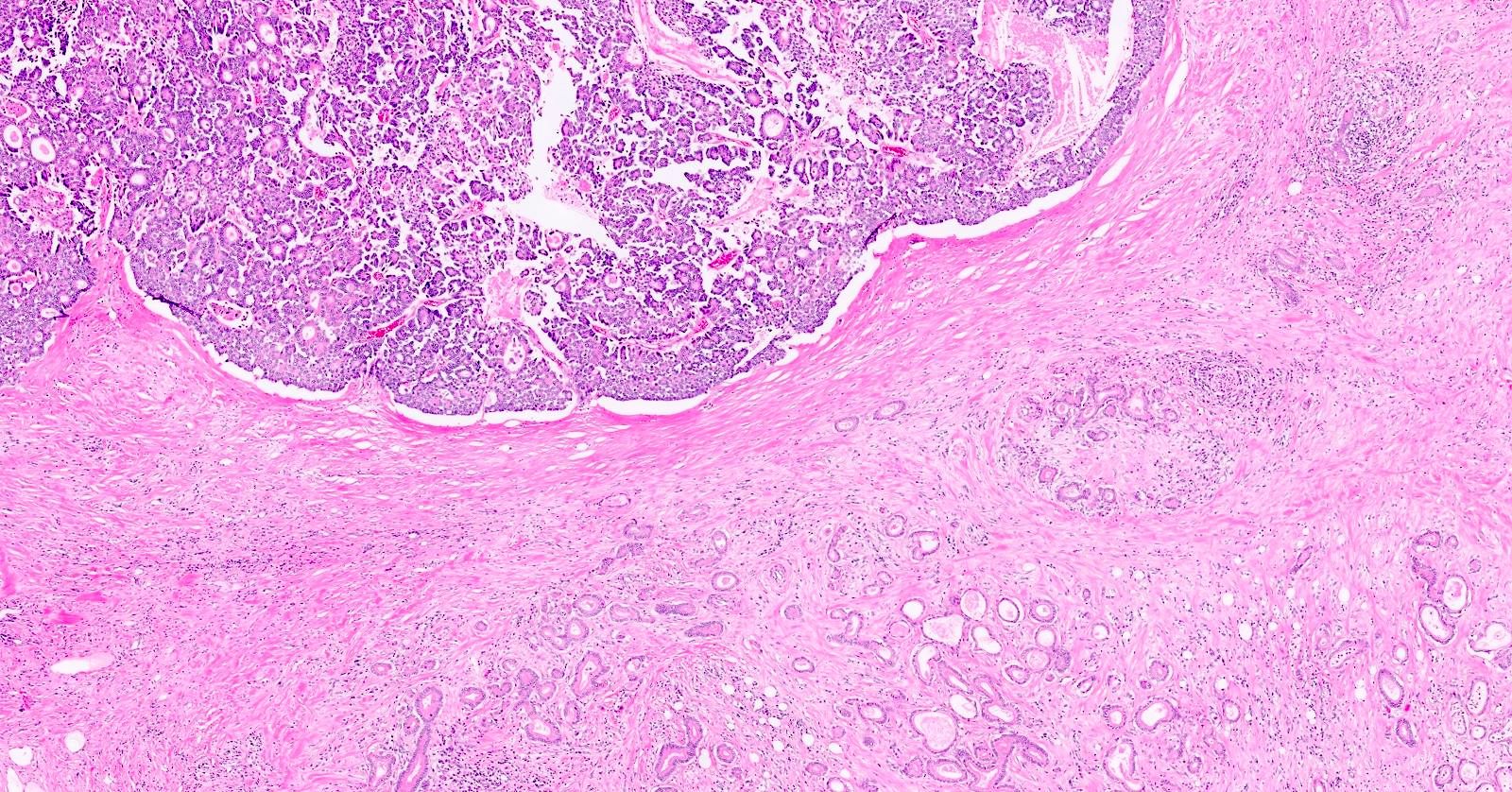
Mixed ductal neuroendocrine carcinoma
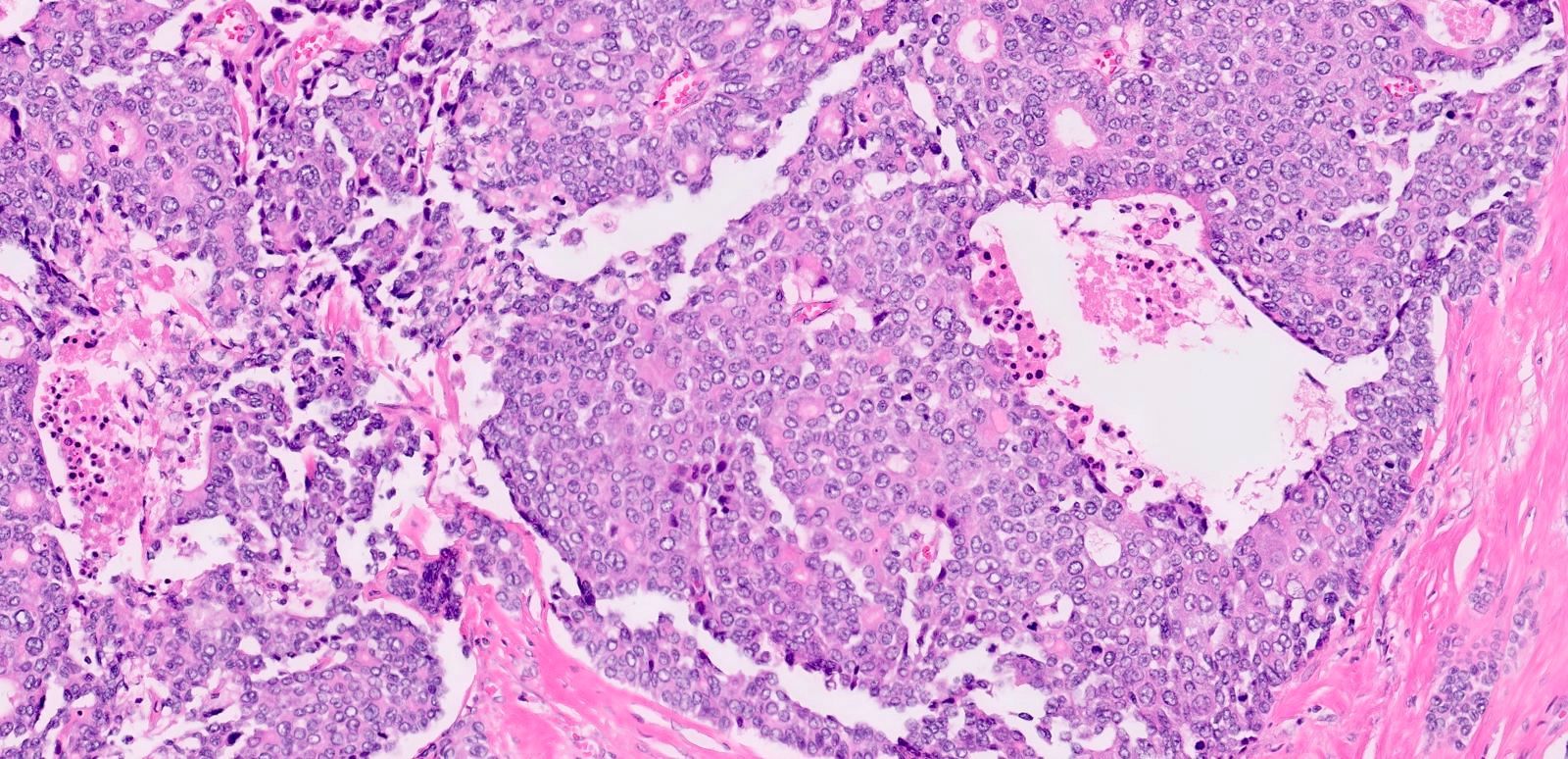
Neuroendocrine carcinoma component
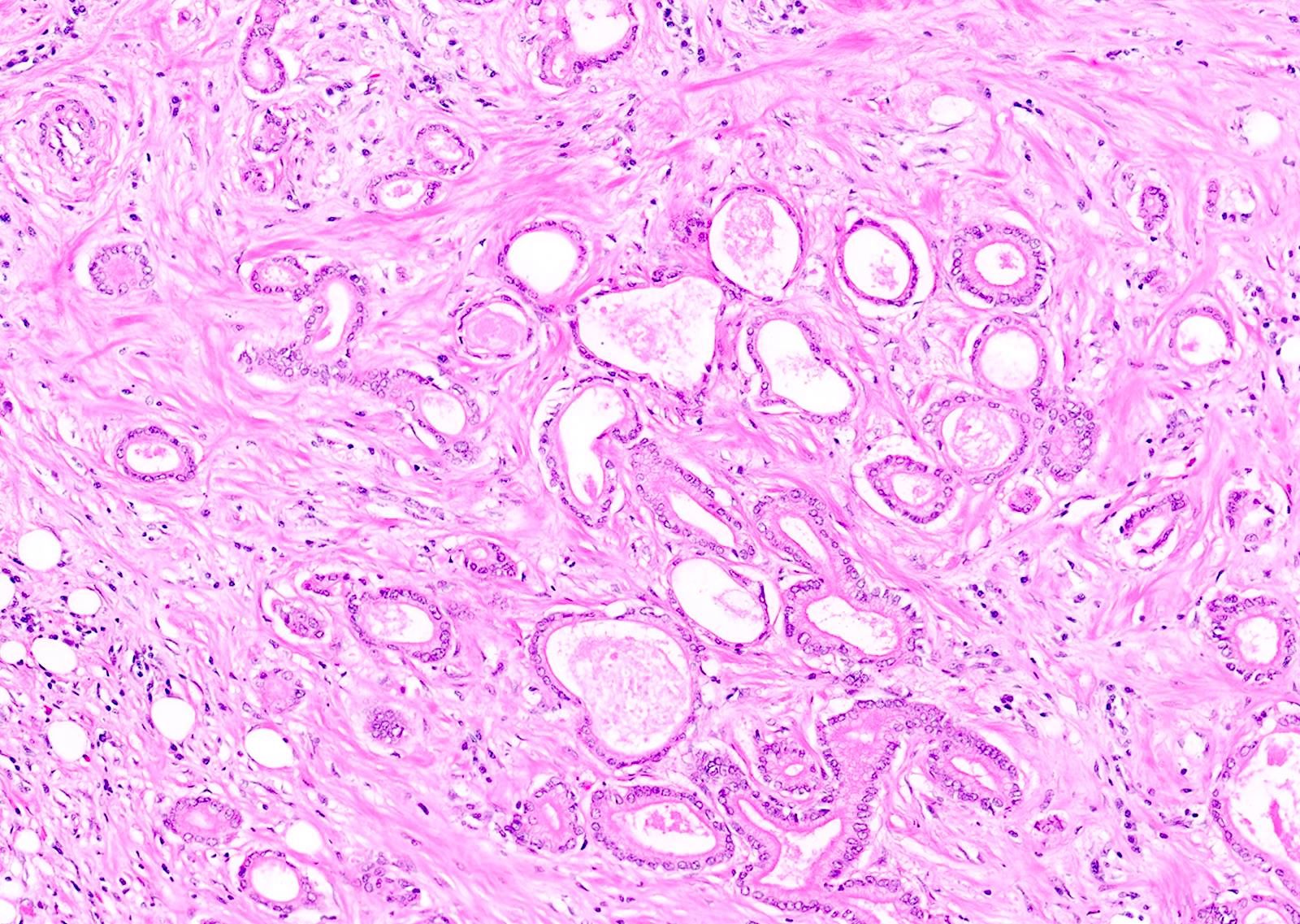
Ductal adenocarcinoma component
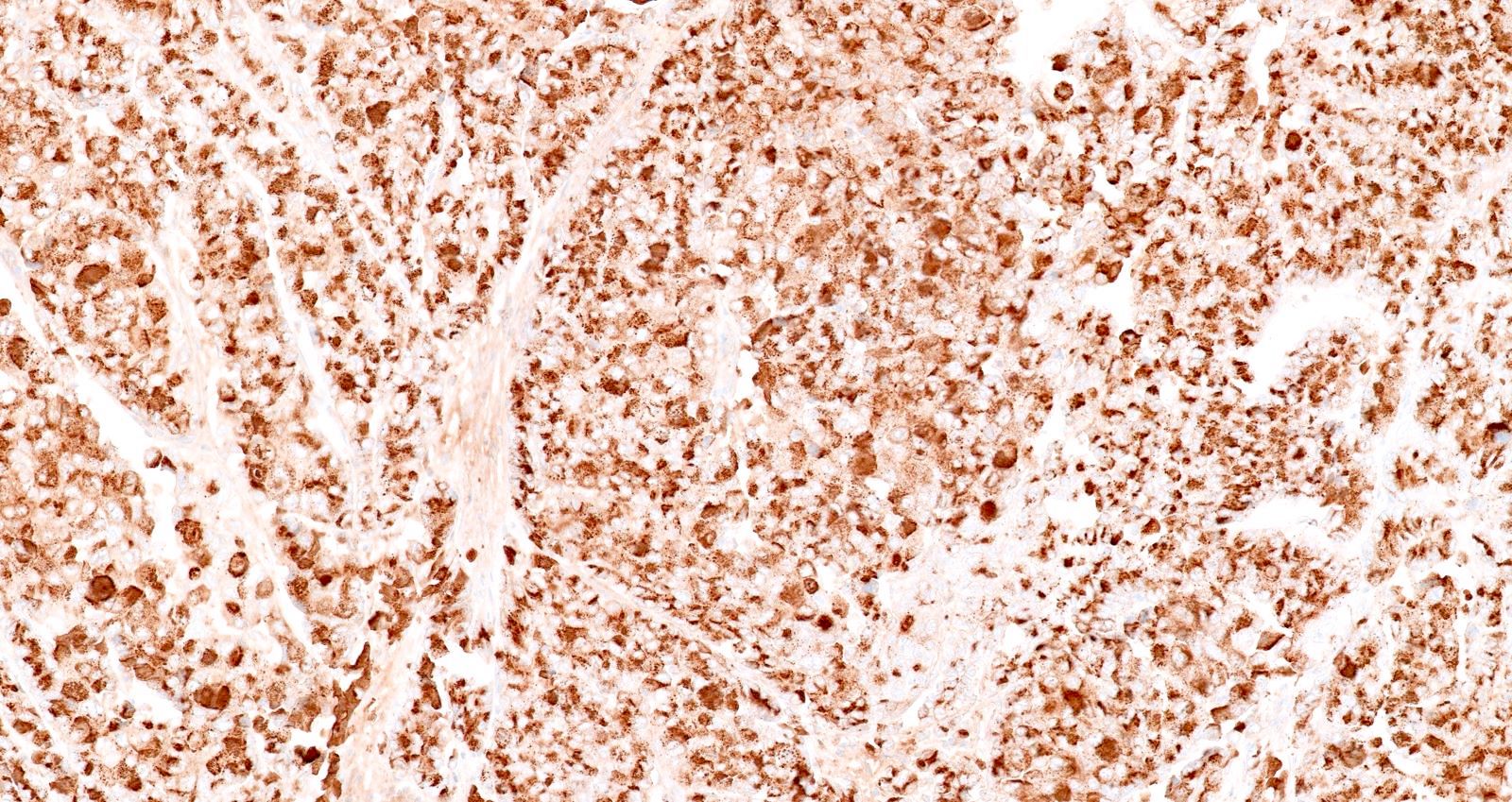
Chromogranin A
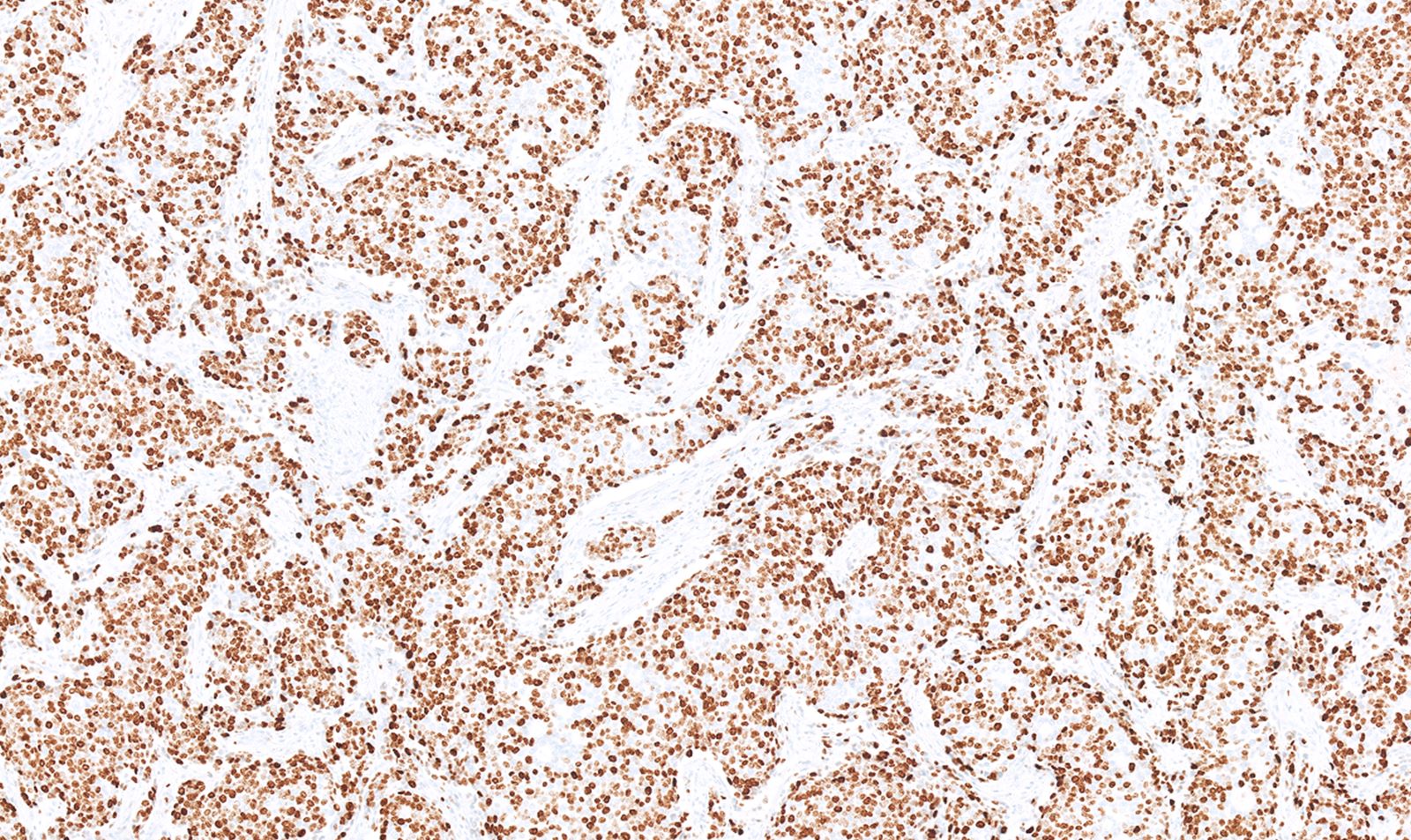
Ki67 neuroendocrine carcinoma component
Cytology description
- Diagnosis of MiNENs on FNA is exceedingly challenging due to cytomorphologic variability, sampling bias and the often minimal quantity of tissue available for cell block and (IHC (Diagn Cytopathol 2013;41:164, Acta Cytol 2013;57:296, Diagn Cytopathol 2018;46:971)
- Mixed cytologic features of neuroendocrine and exocrine component (adenocarcinoma or acinar) should raise suspicion of MiNEN
- IHC is helpful to demonstrate the endocrine and exocrine components
Positive stains
- IHC expression is similar to the respective component of MiNENs (Endocr Pathol 2016;27:284)
- Neuroendocrine component (Pathology 2020;52:336):
- Positive stains:
- Synaptophysin (diffusely and strongly positive)
- Chromogranin A (may be reduced in poorly differentiated neuroendocrine components)
- INSM1 (Am J Clin Pathol 2015;144:579)
- Cytokeratins CAM5.2, AE1 / AE3, CK8/18
- Ki67: proliferation index is typically high in poorly differentiated NEC (> 50%); required for grading of well differentiated NET component, grade 1 (< 3%), grade 2 (3 - 20%) and grade 3 (> 20%)
- Panel to differentiate poorly differentiated neuroendocrine carcinoma from well differentiated neuroendocrine tumor components (Arch Pathol Lab Med 2019;143:1317)
- Positive stains:
- Ductal adenocarcinoma component:
- Common expression of CEA, CAM5.2, AE1 / AE3, CK7, CK8/18, CK19, EMA (MUC1), MUC3, MUC4, MUC5AC, CA 19-9, CA125
- Maspin, placental S100 (S100P), IMP3 (Arch Pathol Lab Med 2012;136:601, Hum Pathol 2013;44:503)
- Acinar cell carcinoma component (Pathology 2020;52:336):
Negative stains
- Neuroendocrine component:
- Trypsin (Am J Surg Pathol 2002;26:893)
- Chymotrypsin, BCL10 (Arch Pathol Lab Med 2019;143:1317)
- Ductal adenocarcinoma component:
- CK20, synaptophysin, chromogranin, trypsin, chymotrypsin, lipase
- pVHL (Hum Pathol 2013;44:503)
- Loss of SMAD4 / DPC4 (Am J Clin Pathol 2001;116:831)
- Acinar cell carcinoma component:
- Chromogranin and synaptophysin (synaptophysin can be focally positive)
Electron microscopy description
- Electron microscopy diagnostic findings (Am J Surg Pathol 1994;18:765, Pathol Int 2021;71:485):
- Secretory zymogen granules in acinar cell component; usually > 500 nm in size
- Neuroendocrine granules in neuroendocrine component; usually 100 - 200 nm in size
- Mucinous granules in ductal adenocarcinoma component
Molecular / cytogenetics description
- Not well understood but may show molecular alterations similar to conventional neuroendocrine neoplasms, ductal adenocarcinomas and acinar carcinomas, as highlighted below (Endocr Pathol 2016;27:284)
- Neuroendocrine carcinoma component:
- TP53 and RB1 (Am J Surg Pathol 2012;36:173)
- Ductal adenocarcinoma component:
- KRAS, CDKN2A (P16), TP53 and SMAD4 (DPC4) (J Clin Med 2020;9:273, Cancer Cell 2017;32:185, Hum Pathol 2009;40:612)
- Acinar carcinoma component:
- APC / beta catenin alterations, BRAF fusions (Virchows Arch 2014;464:553, Cancer Discov 2014;4:1398, J Clin Med 2020;9:273)
- Neuroendocrine carcinoma component:
- No known association with genetic syndromes
Videos
MiNEN basics
Sample pathology report
- Pancreas tail and spleen, distal pancreatectomy:
- Mixed neuroendocrine and nonneuroendocrine neoplasm (MiNEN) of pancreas composed of ductal adenocarcinoma and neuroendocrine carcinoma, 3.5 cm (see comment and synoptic report)
- Tumor infiltrates the peripancreatic soft tissue
- Prominent lymphovascular and perineural invasion is identified
- Pancreatic parenchymal resection margin is negative for tumor
- Metastatic neuroendocrine carcinoma is identified in 8 of 21 lymph nodes
- Pathology stage: pT3 / N2
- Spleen with no significant diagnostic alterations
- Comment: The sections of the pancreatic tail mass show a biphasic appearance with histologically distinct ductal and neuroendocrine carcinoma components. The neuroendocrine component comprises approximately 60% of the tumor and is characterized by infiltrating sheets and nests of high grade tumor cells with moderate eosinophilic cytoplasm, vesicular chromatin and viably prominent nucleoli. Frequent mitoses are noted (up to 25/HPF). Areas of tumor necrosis are identified. A well differentiated ductal adenocarcinoma component, characterized by infiltrating well formed tubules, is seen intricately associated with the neuroendocrine carcinoma component. Neuroendocrine carcinoma shows diffuse and strong expression for neuroendocrine markers chromogranin and synaptophysin. The ductal carcinoma component is negative for neuroendocrine markers. Neuroendocrine carcinoma shows a Ki67 proliferative index of approximately 90%. Overall, the findings are consistent with mixed ductal neuroendocrine carcinoma of the pancreas.
- Mixed neuroendocrine and nonneuroendocrine neoplasm (MiNEN) of pancreas composed of ductal adenocarcinoma and neuroendocrine carcinoma, 3.5 cm (see comment and synoptic report)
Differential diagnosis
- Amphicrine carcinoma (Pathol Int 2021;71:485):
- May represent a variant of MiNEN but does not fit under the current definition of MiNEN
- Rare tumor where each neoplastic cell displays exocrine and endocrine differentiation confirmed with IHC
- Mixed intraductal papillary mucinous neoplasm (IPMN) neuroendocrine tumor (Virchows Arch 2021;478:1215):
- Rare tumor characterized by low or high grade IPMN associated with a well differentiated neuroendocrine tumor in the papillae
- Recent evidence suggests common clonal origin with shared molecular abnormalities in both components
- May represent a variant of MiNEN
- Ductal adenocarcinoma with neuroendocrine component:
- Neuroendocrine component < 30% of the tumor
- Pancreatic neuroendocrine tumor with entrapped ductules (Am J Surg Pathol 2004;28:813):
- Entrapment of preexisting nonneoplastic ductules by neuroendocrine tumor
- Acinar cell carcinoma with a neuroendocrine component:
- Neuroendocrine cells comprises < 30% of the tumor
- May be focally positive for synaptophysin but should be negative for chromogranin; in contrast, in acinar MiNEN, immunohistochemistry for acinar and neuroendocrine cell markers demonstrates distinct compartments in the tumor tissue
- Collision tumors:
- Neuroendocrine and nonneuroendocrine components are distinct from each other and not intimately intermixed
- Pancreatoblastoma:
- Commonly a childhood malignant pancreatic neoplasm with predominantly acinar differentiation and squamoid nests
- Can have neuroendocrine component
- Squamoid nests are critical for diagnosis
Additional references
Board review style question #1
A 55 year old man presented with a 4 cm large pancreatic head mass. The sections from the resected tumor showed a mixed neoplasm with varied histologic findings, as highlighted in the image above. What is the most common component of such neoplasms?
- Acinar carcinoma
- Ductal adenocarcinoma
- Poorly differentiated neuroendocrine carcinoma
- Squamous cell carcinoma
- Well differentiated neuroendocrine tumor
Board review style answer #1
C. Poorly differentiated neuroendocrine carcinoma. The tumor is likely pancreatic mixed neuroendocrine nonneuroendocrine neoplasms (MiNENs) with ductal adenocarcinoma and poorly differentiated neuroendocrine carcinoma components. Poorly differentiated neuroendocrine carcinoma is the most common component seen in around 90% of MiNENs.
Comment Here
Reference: Mixed neuroendocrine nonneuroendocrine neoplasms pancreas (MiNENs)
Comment Here
Reference: Mixed neuroendocrine nonneuroendocrine neoplasms pancreas (MiNENs)
Board review style question #2
In a mixed neuroendocrine nonneuroendocrine neoplasm (MiNEN), what is the lowest percentage of the neoplasm the neuroendocrine component can comprise in order to classify as a MiNEN?
- 20%
- 30%
- 40%
- 50%
- 60%
Board review style answer #2

