
Pancreas
Cystic and intraductal lesions
Lymphoepithelial cysts
Authors: Jen Rytych, M.D., Katrina Krogh, M.D., Guang-Yu Yang, M.D., Ph.D., David J. Escobar, M.D., Ph.D.
Editorial Board Member: Wei Chen, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.

Last author update: 2 August 2023
Last staff update: 2 August 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Lymphoepithelial cysts


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Rytych J, Krogh K, Yang GY, Escobar D. Lymphoepithelial cysts. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreaslymphoepithelial.html. Accessed April 1st, 2025.
Definition / general
- Rare, nonneoplastic, true cysts lined by squamous epithelium surrounded by abundant, reactive lymphoid tissue
- Histologically similar to branchial cleft cysts arising in the neck
- First described in 1985 (Pathologe 1985;6:217)
- No association with salivary gland lymphoepithelial cysts
Essential features
- Consists of a squamous, epithelial lined cyst with surrounding reactive lymphoid tissue
ICD coding
- ICD-10: K86.2 - cyst of pancreas
Epidemiology
- Mean age: 56 years
- Range: 20 - 82 years
- 80% male
- 0.5% of resected pancreatic cysts (Diagnostics (Basel) 2022;13:65)
Sites
- Occurs anywhere in pancreas (head, body or tail) or extrapancreatic location
Pathophysiology
- May occasionally develop from epithelial remnants in lymph nodes or from accessory spleen in pancreas (Hum Pathol 1991;22:924, Mod Pathol 1998;11:1171)
Etiology
- Several proposed hypotheses (Case Rep Gastrointest Med 2016;2016:5492824)
- May originate from epithelial remnants within a lymph node
- Arise via cystic transformation and squamous metaplasia of pancreatic ducts
- May derive from a misplaced branchial cleft cyst that fused with the pancreas during embryogenesis
Clinical features
- Most common symptom is abdominal pain (~48%), particularly with larger cysts
- Significant portion are asymptomatic (~43%)
- Can occasionally present with fatigue or weight loss, mimicking malignancy (Case Rep Gastroenterol 2016;10:181)
- Not associated with immunosuppression or autoimmune diseases
Diagnosis
- Can be difficult to differentiate preoperatively from other pancreatic cystic lesions
- Cyst fluid chemistry may show elevated CA 19-9 or elevated carcinoembryonic antigen (CEA)
- Cytology / histology examination for final confirmation of diagnosis
- Reference: Arch Pathol Lab Med 2020;144:47
Laboratory
- Cyst fluid may have elevated CA 19-9 levels (50% of cases) and elevated CEA levels (up to 32% of cases) (diagnostic pitfall) (Case Rep Gastrointest Med 2016;2016:5492824)
Radiology description
- Imaging varies and is similar to other pancreatic cystic lesions but more likely to be extrapancreatic or exophytic
- CT: multilocular or unilocular cyst with possible solid component and slight hyperintensity of keratinized material (Case Rep Gastrointest Med 2016;2016:5492824)
- MRI: multilocular or unilocular cyst with possible solid component, hyperintensity on T1 weighted images, hypointensity on T2 weighted images and water restriction in diffusion weighted images (Jpn J Radiol 2021;39:118)
Radiology images
Images hosted on other servers:

CT

Large cystic mass

Mimicking serous / mucinous cystadenoma
Prognostic factors
- Benign; does not recur or progress
Case reports
- 41 year old woman who presented with abdominal discomfort, bloating and dyspepsia (Acta Chir Belg 2022 Mar 17 [Epub ahead of print])
- 43 year old man with a lymphoepithelial cyst occurring in a pancreatic accessory spleen (Clin Case Rep 2021;9:e04241)
- 49 year old man with diarrhea and weight loss (Int J Surg Case Rep 2019;55:192)
- 62 year old man with abdominal pain and a pancreatic mass (Case Rep Med 2020;2020:4590758)
- 65 year old man with prior pancreatoduodenectomy for carcinoma arising from the ampulla of Vater and a new pancreatic mass in the remnant pancreatic tail (Surg Case Rep 2021;7:108)
Treatment
- Asymptomatic patients with a confirmed diagnosis by FNA may be followed by serial imaging
- Symptomatic patients with a confirmed diagnosis by FNA may be treated with enucleation or drainage (Indian J Surg 2010;72:427)
- Resection is curative
Clinical images
Images hosted on other servers:

Intraoperative view
Gross description
- Mean size: 5 cm (range: 1 - 17 cm) (Mod Pathol 2002;15:492)
- Often round and well demarcated from surrounding pancreas
- Either multilocular (60%) or unilocular (40%)
- Cysts contain clear serous fluid or caseous / cheese-like material (Diagnostics (Basel) 2022;13:65)
Gross images
Contributed by Jen Rytych, M.D.

Sections of lymphoepithelial cyst
Images hosted on other servers:

Well demarcated cysts

Pancreas tail
Microscopic (histologic) description
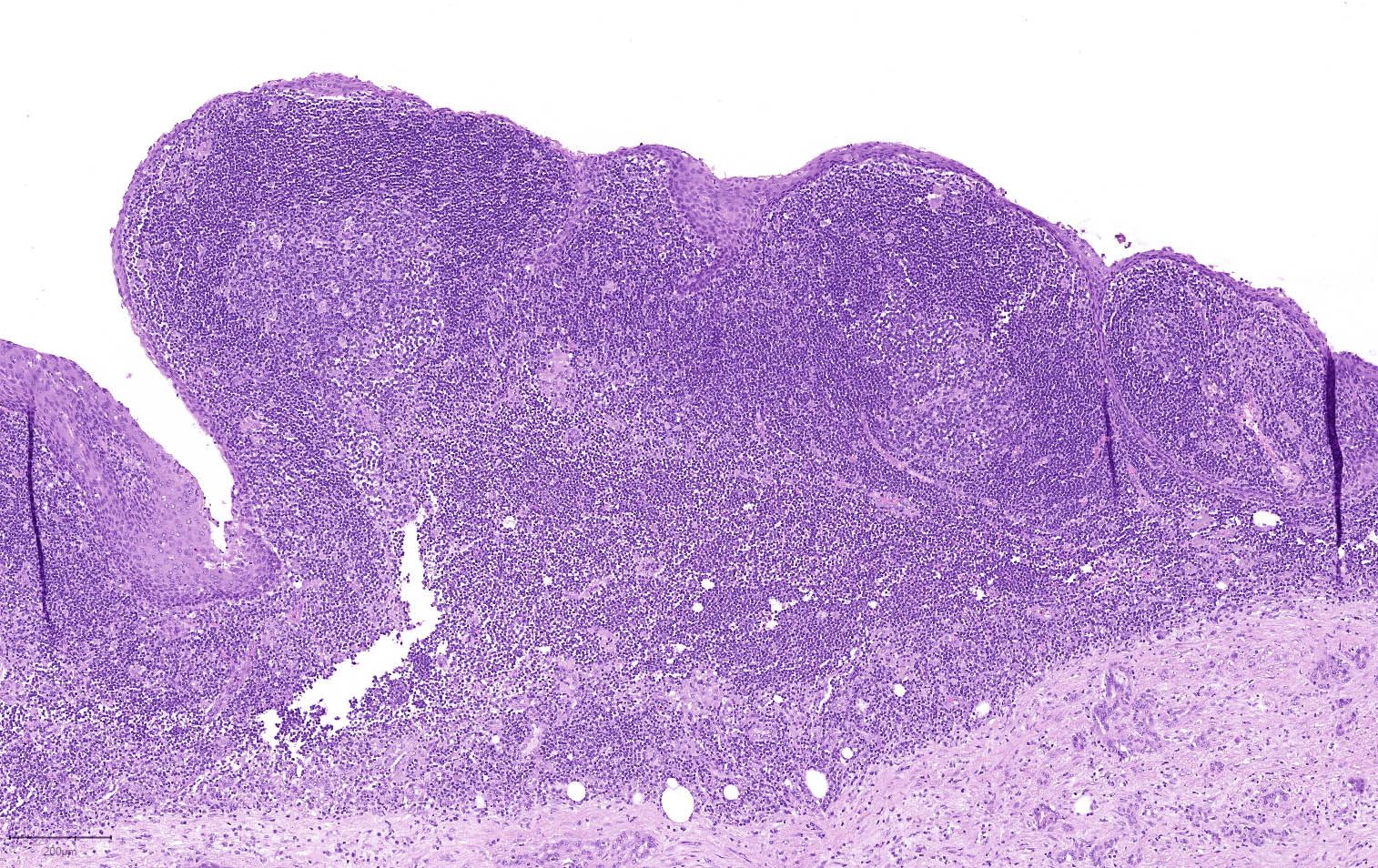
- Unilocular or multilocular cyst lined by squamous epithelium (nucleated or anucleated), with cyst wall containing lymphocyte rich cuff with germinal centers
- Combinations of squamous lining with other epithelial types (i.e., simple columnar) have been reported
- Lymphoid tissue, often a dense band
- With or without keratinous debris
- Occasional solid lymphoepithelial islands, rarely mucinous goblet cells
- Rare sebaceous differentiation, keratin granulomas, cholesterol clefts, multinucleated giant cells and foamy histiocytes may be present
- Reference: Diagnostics (Basel) 2022;13:65
Microscopic (histologic) images
Contributed by Jen Rytych, M.D. and Katrina Krogh, M.D.
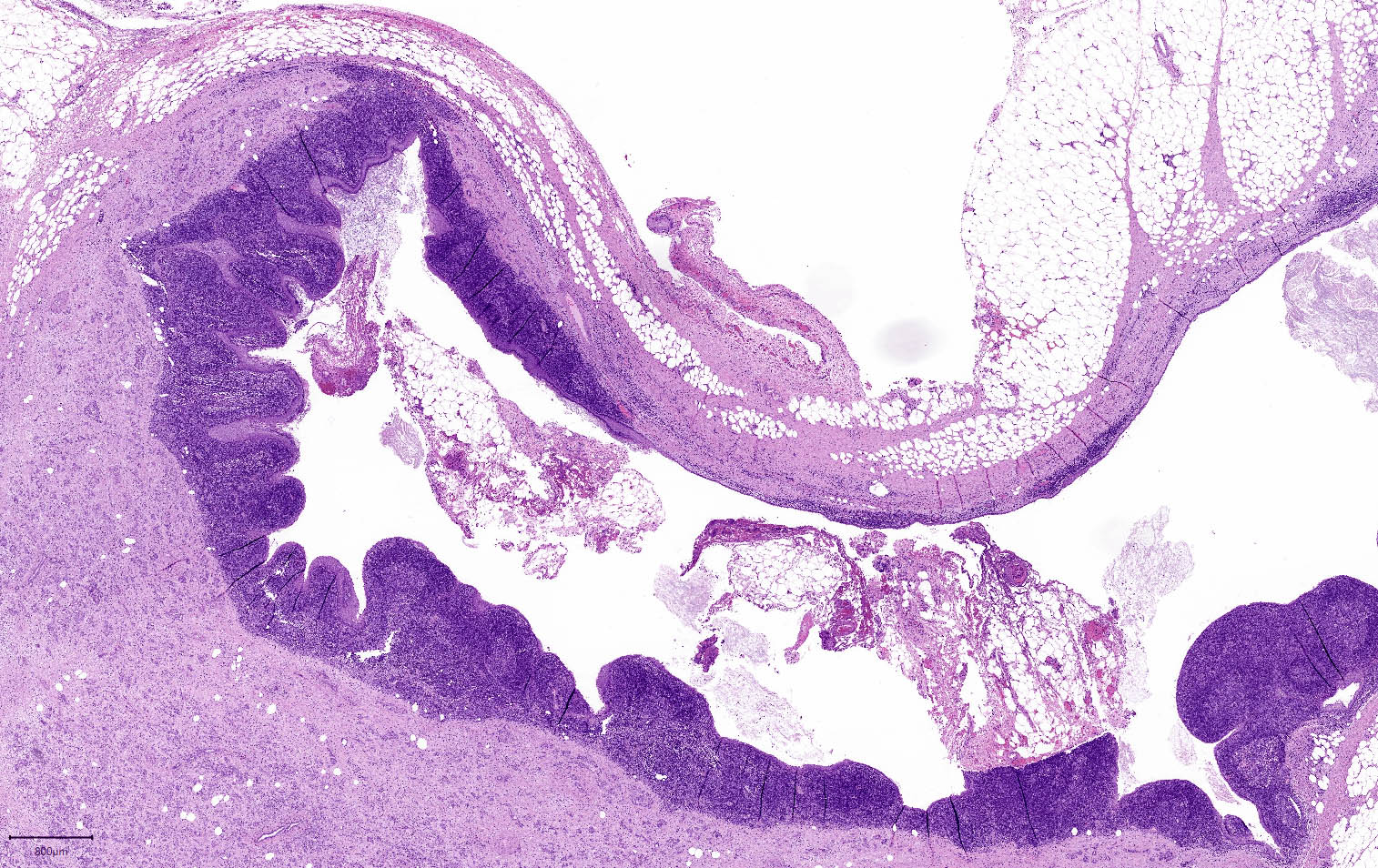
Squamous lined cyst
Cyst with lymphoid cuff
Abundant keratin debris
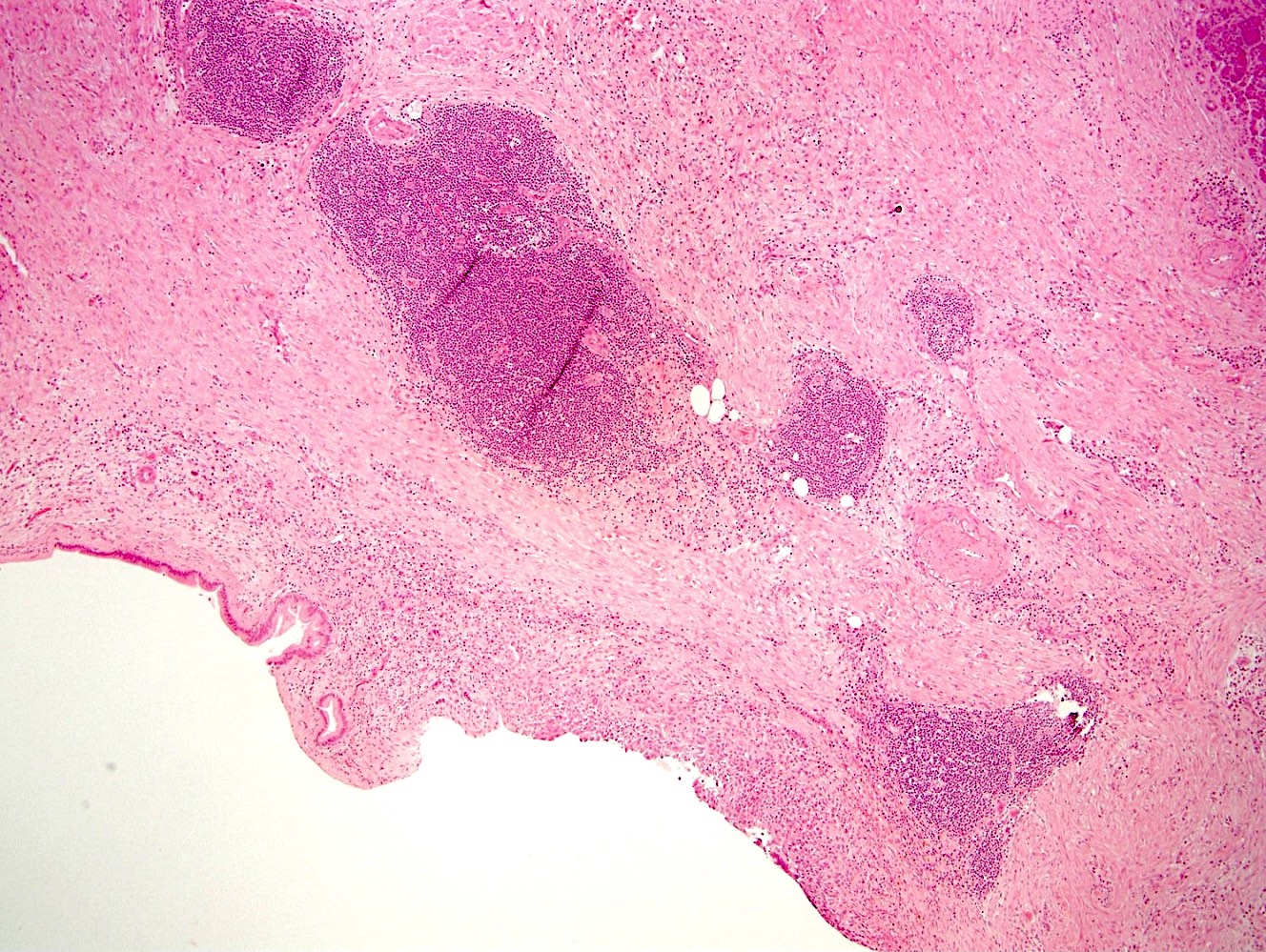
Simple columnar and stratified squamous linings
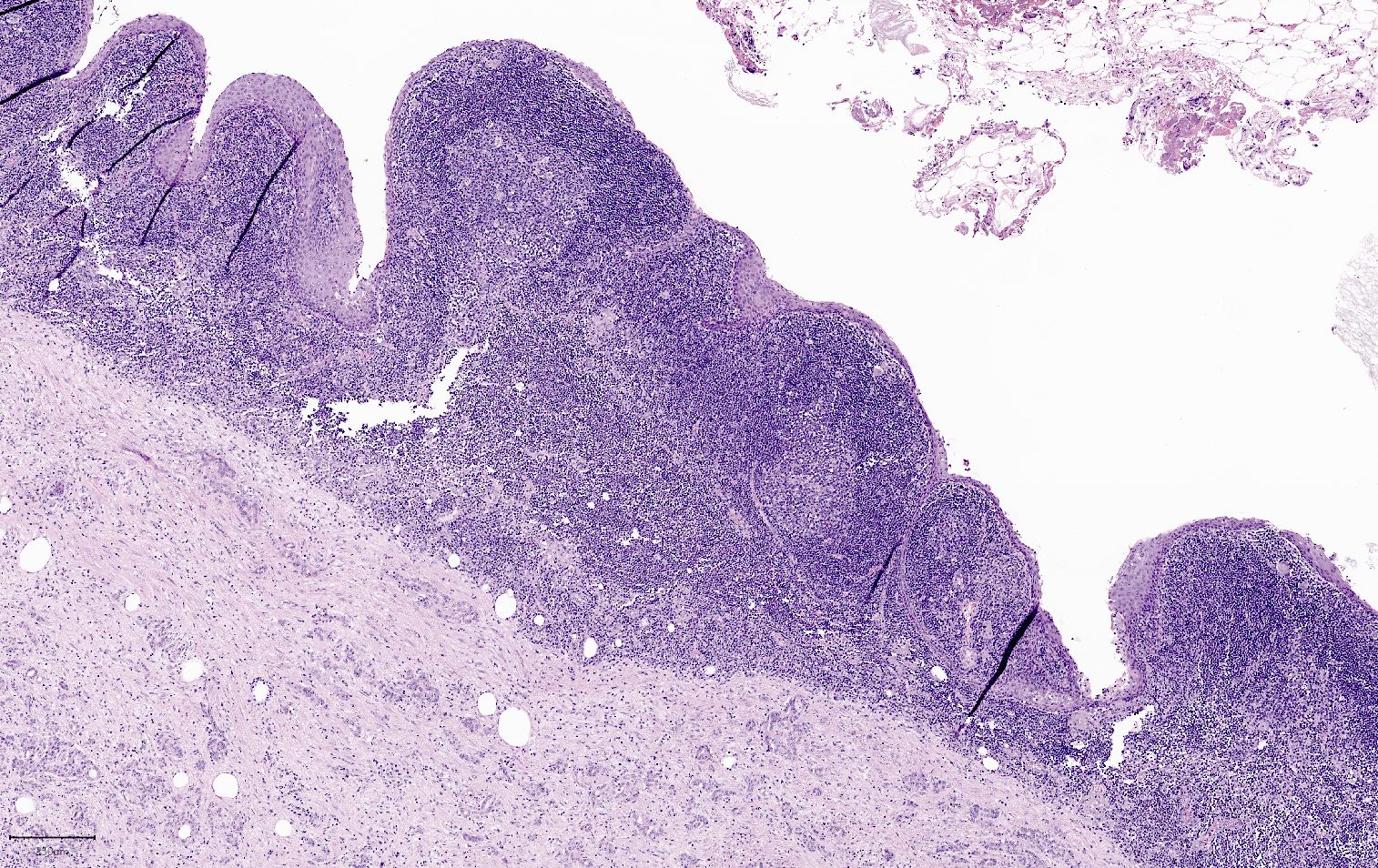
Squamous lined lymphoid tissue
Cytology description
- Predominantly mature squamous cells, anucleated squamous cells and keratin debris
- Lymphocytes, macrophages and cholesterol crystals are occasionally seen (Arch Pathol Lab Med 2020;144:47)
- May have mildly atypical mucinous glandular and parakeratotic epithelium
Cytology images
Contributed by Jen Rytych, M.D.

Degenerated squamous epithelial cells
Images hosted on other servers:

Squamous epithelium,
keratinaceous debris
and lymphocytes

Keratinaceous debris
Positive stains
Negative stains
- Squamous epithelial lining is negative for MUC2 and MUC6 (100%) (Mod Pathol 2010;23:1467)
Molecular / cytogenetics description
- No recurrent molecular / cytogenetic abnormalities identified
Sample pathology report
- Pancreas, cyst, excision:
- Lymphoepithelial cyst
Differential diagnosis
- Dermoid cyst (cystic teratoma):
- Requires the presence of microscopic elements such as dermal appendages, cartilage, respiratory mucosa or neural tissue
- Younger mean age
- Epidermoid cyst in intrapancreatic spleen:
- Lined by squamous epithelium and surrounded by splenic tissue (Acta Pathol Jpn 1991;41:916)
- Squamoid cysts:
- Smaller (median size: 1.5 cm)
- Lined exclusively by nonkeratinizing squamous epithelium without lymphoid tissue (Am J Surg Pathol 2007;31:291)
- Lymphangioma:
- Lined by a single flat or cuboidal epithelium that will be positive for endothelial and lymphatic markers (such as CD31 and D2-40)
- Typically contains small aggregates of lymphoid tissue rather than a dense band (Arch Pathol Lab Med 2020;144:47)
- Pseudocyst:
- No epithelial lining or lymphoid stroma
- Presence of granulation tissue and fibrosis
- Of note, while the imaging or clinical differential diagnosis may include mucinous cystic neoplasm, intraductal papillary mucinous neoplasm (IPMN) and intraductal oncocytic papillary neoplasm (IOPN), these neoplasms are not similar appearing on histologic examination and are not on the histologic differential diagnosis
Board review style question #1
Which of the following statements about the pancreatic lesion shown above is true?
- Carcinoembryonic antigen (CEA) is never elevated in cyst fluid
- This lesion does not undergo malignant transformation
- This lesion is more common than mucinous cystic neoplasm
- This lesion is more commonly found in women
Board review style answer #1
B. This lesion does not undergo malignant transformation. Lymphoepithelial cysts are benign and there have been no reported incidences of malignant transformation. Answer C is incorrect because lymphoepithelial cysts of the pancreas are rare (0.5% of resected pancreatic cysts) and are much less common than pancreatic mucinous cystic neoplasms (~8% of resected pancreatic cysts). Answer D is incorrect because lymphoepithelial cysts are more common in men than women (80% men). Answer A is incorrect because CEA levels (as well as CA 19-9) are commonly elevated in lymphoepithelial cysts. This is a diagnostic pitfall that increases the clinical concern for malignancy.
Comment Here
Reference: Lymphoepithelial cysts
Comment Here
Reference: Lymphoepithelial cysts
Board review style question #2
Which of the following statements about the pancreatic lesion shown above is true?
- Foamy histiocytes and multinucleated giant cells can be present
- This lesion is associated with immunosuppression or autoimmune dysfunction
- This lesion is associated with ovarian type stroma
- This lesion is the most common cystic lesion of the pancreas
Board review style answer #2
A. Foamy histiocytes and multinucleated giant cells can be present. Lymphoepithelial cysts are composed of squamous epithelium and reactive lymphoid tissue but may rarely show sebaceous differentiation, keratin granulomas, cholesterol clefts, multinucleated giant cells and foamy histiocytes. Answer D is incorrect because lymphoepithelial cysts of the pancreas are rare (0.5% of resected pancreatic cysts). The most common cystic lesion of the pancreas is intraductal papillary mucinous neoplasm (IPMN). Answer B is incorrect because while the etiology of lymphoepithelial cysts is not fully understood, it may originate from epithelial remnants within a lymph node, arise through cystic transformation of pancreatic ducts or be derived from a misplaced branchial cleft cyst that fused with the pancreas during embryogenesis. No association with immunosuppression or autoimmune dysfunction has been identified. Answer C is incorrect because lymphoepithelial cysts are composed of a squamous epithelial lined cyst with surrounding reactive lymphoid tissue. Mucinous cystic neoplasms (MCN) contain ovarian stroma.
Comment Here
Reference: Lymphoepithelial cysts
Comment Here
Reference: Lymphoepithelial cysts
