

Ovary
Sex cord stromal tumors
Pure sex cord tumors
Sex cord tumor with annular tubules
Editorial Board Member: Kyle Devins, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 15 November 2023
Last staff update: 15 November 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Ovarian sex cord tumor with annular tubules


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Lengyel K, Hanley K. Sex cord tumor with annular tubules. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarytumorsexcordannular.html. Accessed December 25th, 2024.
Definition / general
- Sex cord tumor with annular tubules (SCTAT) is a distinctive variant of sex cord stromal tumor that histologically exhibits a unique morphology, characterized by sharply circumscribed nests composed of ring-like tubules that encircle basement membrane-like material
Essential features
- Presence of characteristic tubular pattern, with antipodal distribution of nuclei and basement membrane-like material
- Rare tumor, < 1% of all sex cord stromal tumors
- 2 types: sporadic and syndromic, the latter is associated with Peutz-Jeghers syndrome
- Peak incidence between third and fourth decade
- Uncertain clinical behavior: syndromic types usually have a benign clinical course, up to 20% of sporadic type exhibit extraovarian spread
ICD coding
- ICD-O: 8623/1 - sex cord tumor with annular tubules
- ICD-10: D39.1 - neoplasm of uncertain behavior of ovary
- ICD-11: 2F76 & XH5BV8 - neoplasms of uncertain behavior of female genital organs & sex cord tumor with annular tubules
Epidemiology
- Overall rare tumor (accounting for < 1% of all sex cord tumors)
- Syndromic: associated with germline STK11 mutations on chromosome 19p13.3 (Peutz-Jeghers syndrome), incidental finding
- Nonsyndromic: mean age at presentation is 36 years of age (range: 6 - 76 years)
- References: Cancer 1982;50:1384, Crum: Diagnostic Gynecologic and Obstetric Pathology, 3rd Edition, 2017
Sites
- Peutz-Jeghers syndrome associated cases occur as bilateral ovarian lesions, sometimes multifocal
- Nonsyndromic / sporadic cases are unilateral ovarian lesions
Pathophysiology
- Peutz-Jeghers syndrome associated lesions harbor germline STK11 mutations
Etiology
- Unknown
Clinical features
- Lesions may be seen at any age, mainly in the third and fourth decade
- Incidental finding in a patient with Peutz-Jeghers syndrome
- Nonsyndromic
- Associated with nonspecific symptoms and signs
- Menstrual irregularities
- Premenstrual girls often have precocious pseudopuberty (Fletcher: Diagnostic Histopathology of Tumors, 5th Edition, 2020)
- Older women may have menstrual dysfunction or postmenopausal bleeding (Fletcher: Diagnostic Histopathology of Tumors, 5th Edition, 2020)
- Rarely, nonsyndromic cases may be associated with signs related to progesterone production
Diagnosis
- Histologic evaluation
Radiology description
- Ultrasound imaging (Pediatr Radiol 2007;37:1270)
- Multiple small, lobulated, discrete high echogenicity masses or tumorlets
- Occasionally may have calcifications
Prognostic factors
- Syndrome associated tumors are typically benign
- Nonsyndromic / sporadic cases may exhibit extraovarian spread in ~20% of patients
- Malignant potential of SCTAT cannot be reliably assessed on histologic evaluation as high risk features such as mitotic rate, lymphovascular invasion or ovarian surface involvement are not consistently associated with poor outcomes (Crum: Diagnostic Gynecologic and Obstetric Pathology, 3rd Edition, 2017)
- Malignant SCTAT may have early or late recurrences decades after initial presentation (Crum: Diagnostic Gynecologic and Obstetric Pathology, 3rd Edition, 2017)
- Sites of metastasis include pelvic peritoneum, retroperitoneum and lung (Crum: Diagnostic Gynecologic and Obstetric Pathology, 3rd Edition, 2017)
Case reports
- 11 year old girl with Peutz-Jeghers syndrome and unilateral ovarian tumor most consistent with Sertoli cell tumor associated SCTAT (Int J Surg Pathol 2016;24:269)
- 14 year old girl without Peutz-Jeghers syndrome and with stage III A1 malignant SCTAT (J Obstet Gynaecol Res 2016;42:224)
- 35 and 36 year old women with minimal deviation adenocarcinoma of the cervix, tumorlets of sex cord tumor with annular tubules of the ovaries and Peutz-Jeghers syndrome (J Gynecol Oncol 2013;24:92)
- 60 year old woman with primary diagnosis of granulosa cell tumor with SCTAT (J Obstet Gynaecol Can 2021;43:361)
Treatment
- Surgical management (salpingo-oophorectomy) is a feasible treatment option for nonsyndromic cases
- Complete resection in recurrent cases is advised
- Prognosis is overall favorable
- Reference: BMC Cancer 2015;15:270
Gross description
- Nonsyndromic tumors
- Unilateral masses ranging in size from several millimeters to 3 cm
- Solid, tan to yellow
- Cysts may be seen and occasionally may predominate (Pathology 2018;50:5)
- Syndromic tumors
- Bilateral and multifocal lesions
- Often microscopic; may not be grossly visible
- Gritty texture may be noted if there is a mass
Gross images
AFIP images

Predominantly solid tumor
Microscopic (histologic) description
- Syndromic and nonsyndromic tumors have similar morphology
- Variably size round nests of sharply delineated simple and complex tubules containing basement membrane-like material, which may also be present around the tubules
- Sertoliform tubules are classified as annular by their arrangement as small concentric secondary ring shaped acini peripherally arranged around the circumference of a larger tubule
- Tall cells with ample amount of pale cytoplasm and basally located round nuclei
- Often with antipodal nuclear distribution within the tubules
- Tumors associated with Peutz-Jeghers syndrome
- Calcifications within the tubules may be seen (Pathology 2018;50:5)
- May be associated with endocervical gastric type adenocarcinoma (adenoma malignum)
- Nonsyndromic / sporadic tumors
- May focally transition to granulosa or Sertoli cell morphology
- Cytologic atypia and mitotic activity may rarely be seen
- May be hyalinized
- Reference: Crum: Diagnostic Gynecologic and Obstetric Pathology, 3rd Edition, 2017
Microscopic (histologic) images
Contributed by Krisztina Lengyel, M.D. and AFIP
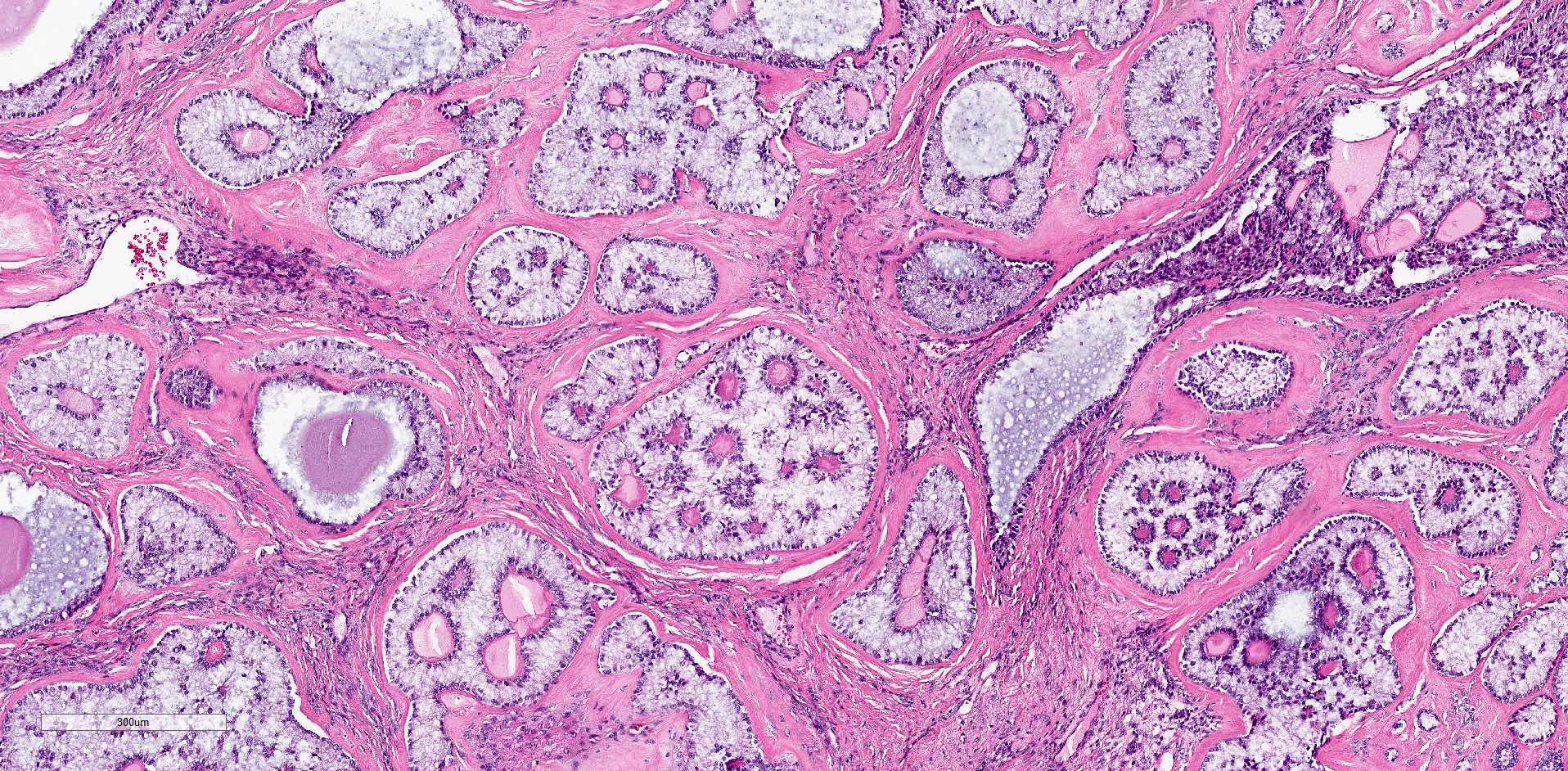
Sharply delineated bland nests
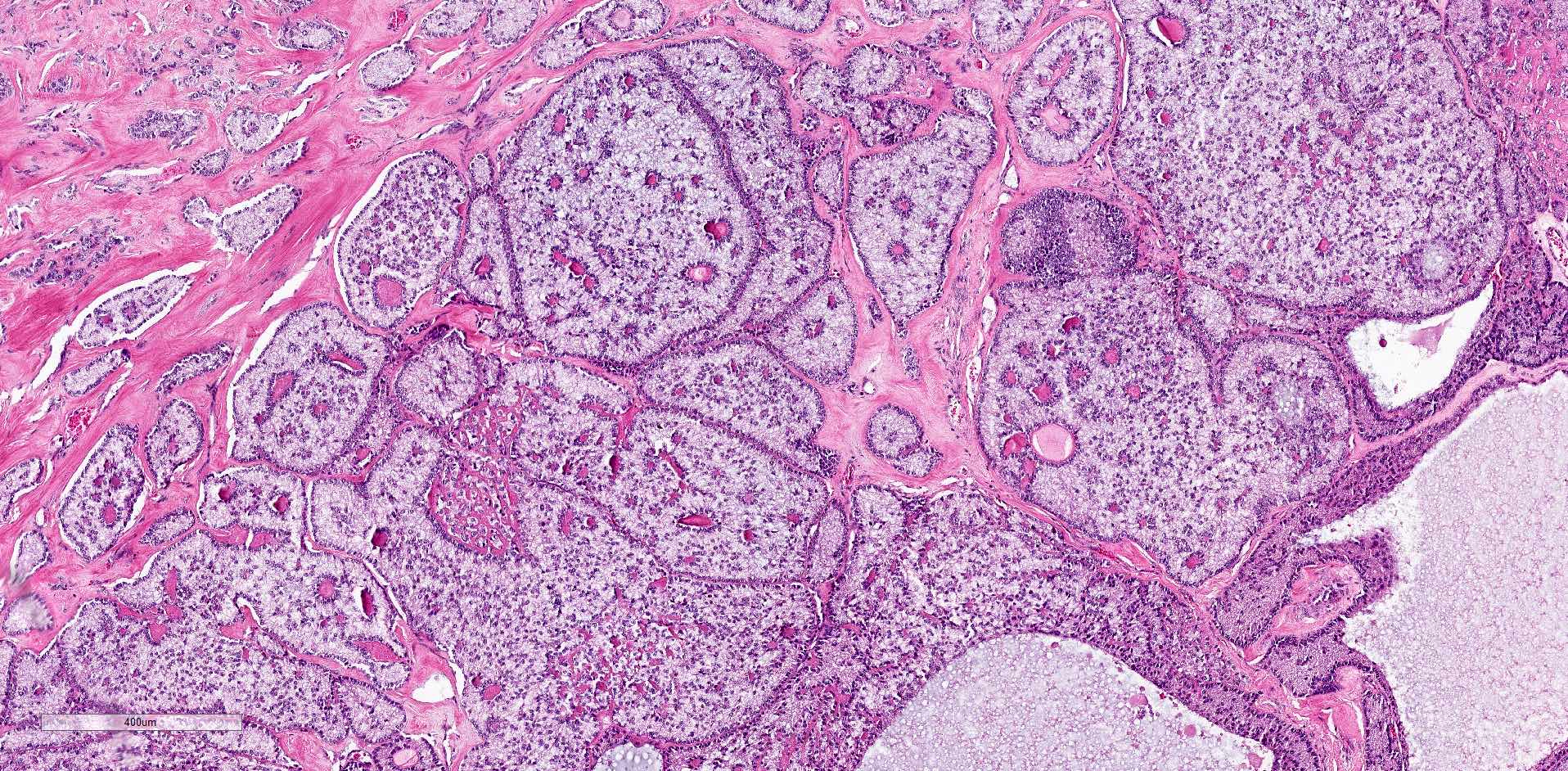
Variably sized nests
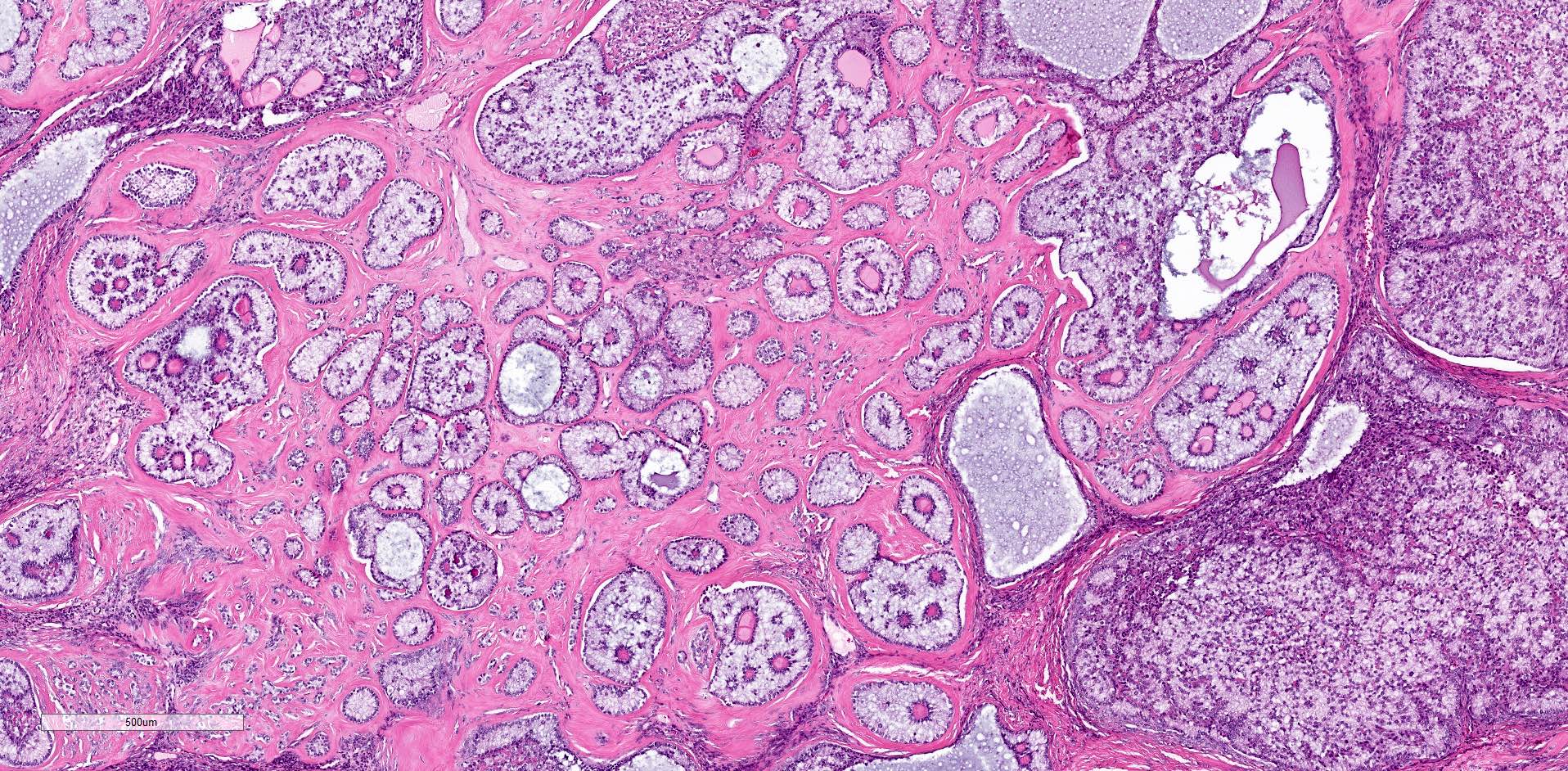
Variably sized discrete nests
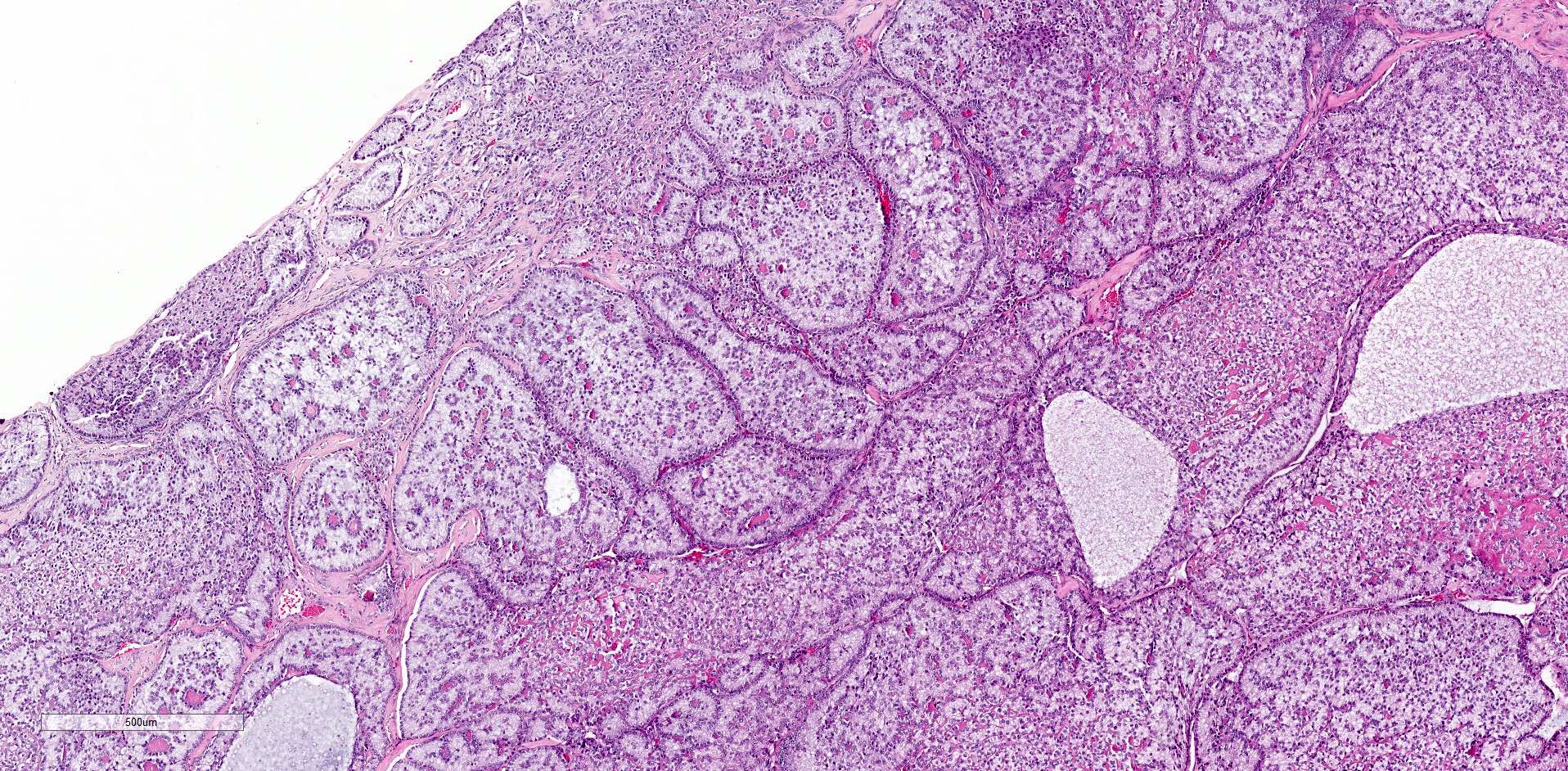
Numerous and variable nests
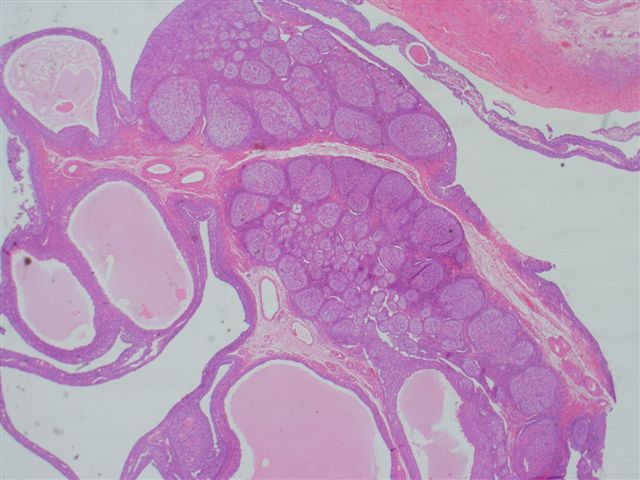
Multiple cysts and nests in young patient
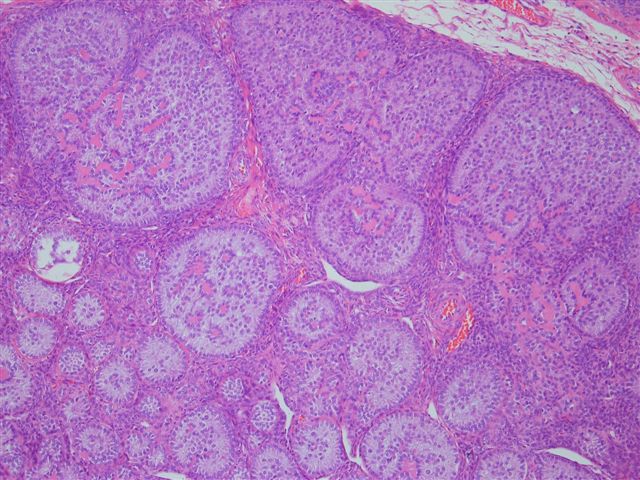
Multiple nests of cells
Positive stains
Molecular / cytogenetics description
- If syndromic, associated with a germline STK11 gene mutations on chromosome 19p13.3 (BMC Med Genet 2016;17:77)
Sample pathology report
- Right ovary, oophorectomy:
- Sex cord tumor with annular tubules (SCTAT), single 9 mm focus (see comment)
- Comment: This neoplasm is an incidental finding. There is no mitotic activity, cytologic atypia, lymphovascular invasion or ovarian surface involvement noted.
- Ovaries and fallopian tubes, bilateral salpingo-oophorectomy:
- Ovaries: bilateral multifocal sex cord tumor with annular tubules (SCTAT), ranging in size from 1.2 mm to 28 mm (see comment)
- Fallopian tubes: benign fimbriated, histologically unremarkable
- Comment: Given the presence of bilateral ovarian involvement and multifocal disease, a possibility of Peutz-Jeghers syndrome associated SCTAT should be considered and excluded. Germline testing for STK11 mutation is recommended.
Differential diagnosis
- Gonadoblastoma:
- Multiple variably sized round nests are distributed in a fibrous to cellular gonadal stroma
- Nests contain 3 components
- Germ cells
- Small sex cord cells
- Globular basement membrane deposits
- Sex cord cells may palisade at the periphery of nests and may resemble the appearance of SCTAT
- Adult granulosa cell tumor:
- Tumor cells of round to oval nuclei with irregular nuclear membrane and nuclear grooves (coffee bean nuclei) and scant cytoplasm
- May form small spaces containing eosinophilic material (Call-Exner bodies) in a microfollicular pattern
- Associated with FOXL2 point mutation (N Engl J Med 2009;360:2719)
- Sertoli cell tumor:
- Cuboidal or columnar cells with pale, at times lipid rich to eosinophilic cytoplasm
- Bland oval to round nuclei, with small nucleoli
- Lipid rich and oxyphilic tumors may be associated with Peutz-Jeghers syndrome
- Areas strongly resembling SCTAT may be seen, especially in patients with Peutz-Jeghers syndrome
- Subset may harbor DICER1 mutations (Mod Pathol 2015;28:1603)
Additional references
Board review style question #1
A 47 year old woman with mucocutaneous oral pigmentations and a history of prior gastrointestinal (GI) polyp resections (multiple hamartomatous polyps) presents for a total abdominal hysterectomy with bilateral salpingo-oophorectomy for menorrhagia. Patient's hysterectomy specimen has no significant histopathologic abnormalities, however, lesion is found in bilateral ovaries. The ovaries were grossly unremarkable. The patient harbors a germline mutation in which of the following genes?
- DICER1
- MMR deficiency
- PTEN
- STK11
Board review style answer #1
D. STK11. The patient has characteristic findings and history of Peutz-Jeghers syndrome. This includes mucocutaneous pigmentation, previous hamartomatous gastrointestinal (GI) polyps. The incidental ovarian findings resemble sex cord tumor with annular tubules (SCTAT). This entity is frequently associated with Peutz-Jeghers syndrome and is often an incidental finding. They are grossly unremarkable and usually involve bilateral ovaries.
Answer A is not correct as DICER1 is associated with Sertoli-Leydig cell tumor, sarcoma and gynandroblastoma, as well as other nongynecologic tumors. Answer B is incorrect because MMR loss is associated with Lynch syndrome. Lynch syndrome predisposes to endometrioid endometrial adenocarcinoma, gastric and intestinal cancers to name a few. Answer C is incorrect because PTEN gene mutations are part of Cowden syndrome, which is associated with high prevalance of thyroid, breast and endometrial neoplasias.
Comment Here
Reference: Sex cord tumor with annular tubules
Answer A is not correct as DICER1 is associated with Sertoli-Leydig cell tumor, sarcoma and gynandroblastoma, as well as other nongynecologic tumors. Answer B is incorrect because MMR loss is associated with Lynch syndrome. Lynch syndrome predisposes to endometrioid endometrial adenocarcinoma, gastric and intestinal cancers to name a few. Answer C is incorrect because PTEN gene mutations are part of Cowden syndrome, which is associated with high prevalance of thyroid, breast and endometrial neoplasias.
Comment Here
Reference: Sex cord tumor with annular tubules

