

Ovary
Metastases to ovary
Metastases to ovary
Author: Lucy Ma, M.D.
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.

Last author update: 8 August 2023
Last staff update: 8 August 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Metastases ovary


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ma L. Metastases to ovary. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarytumormetastatic.html. Accessed January 21st, 2025.
Definition / general
- Secondary involvement of ovary from malignant neoplasms of extraovarian primary sites
Essential features
- Ovary is the most common site of metastasis within the gynecologic tract
- Colorectal and breast carcinoma are the most common primary tumors to metastasize to the ovary
- Usually bilateral, small (< 10 cm), multinodular tumors with extraovarian spread
Terminology
- Krukenberg tumor
- Designation should be reserved for tumors with an appreciable component (> 10%) of signet ring cells (Gynecol Oncol 2006;101:152)
- Most commonly of gastric primary (Arch Pathol Lab Med 2006;130:1725)
ICD coding
Epidemiology
- ~15% of ovarian malignancies are of metastatic origin (range: 3 - 30%) (Int J Gynecol Cancer 2009;19:1160)
- Ovarian metastasis may present either synchronously or metachronously with primary tumor
- Ovary is the most common site of metastasis within the gynecologic tract (Int J Gynecol Pathol 2019;38:363)
- Colorectal carcinoma is the most common primary tumor to metastasize to the ovary, followed by breast carcinoma (Int J Gynecol Pathol 2023;42:414, Int J Gynecol Cancer 2009;19:1160)
Sites
- Ovary and primary organ site, with or without other organs
Pathophysiology
- Tumors can spread to the ovary by several pathways, depending on the primary
- Direct extension
- Lymphovascular / hematogeneous spread (Obstet Gynecol Int 2011;2011:612817)
- Transcoelomic / transperitoneal dissemination (e.g., Krukenberg tumors of gastric primary)
- Tumor cell exfoliation / transtubal spread (e.g., concurrent low grade endometrioid endometrial and ovarian carcinomas [FIGO stage IIIA endometrial carcinoma] simulating independent primary tumors) (Histopathology 2020;76:37)
Etiology
- Malignant tumor of extraovarian primary site
Clinical features
- Clinical features often relate to the primary tumor
- Pelvic (ovarian) mass may be the first manifestation of the disease from a clinically occult primary (Virchows Arch 2017;470:69)
Diagnosis
- Comprehensive medical history, physical evaluation, intraoperative evaluation, imaging, endoscopy
- Final diagnosis is rendered by histopathology and immunohistochemistry (with or without molecular studies)
Laboratory
- CA-125 is not a useful biomarker in the primary diagnostics of metastases to the ovary (Clin Exp Metastasis 2017;34:295)
- CA-125/CEA ratio may be of clinical use in distinguishing primary ovarian tumors from colorectal carcinoma metastases (Tumour Biol 1992;13:18)
Radiology description
- No specific imaging features differentiate primary ovarian malignancy from metastatic ovarian tumors (Magn Reson Imaging Clin N Am 2023;31:93)
- MRI appearances that suggest a mucinous lesion should trigger a search on the scan for an alternative primary mass in the gastrointestinal tract
Radiology images
Images hosted on other servers:
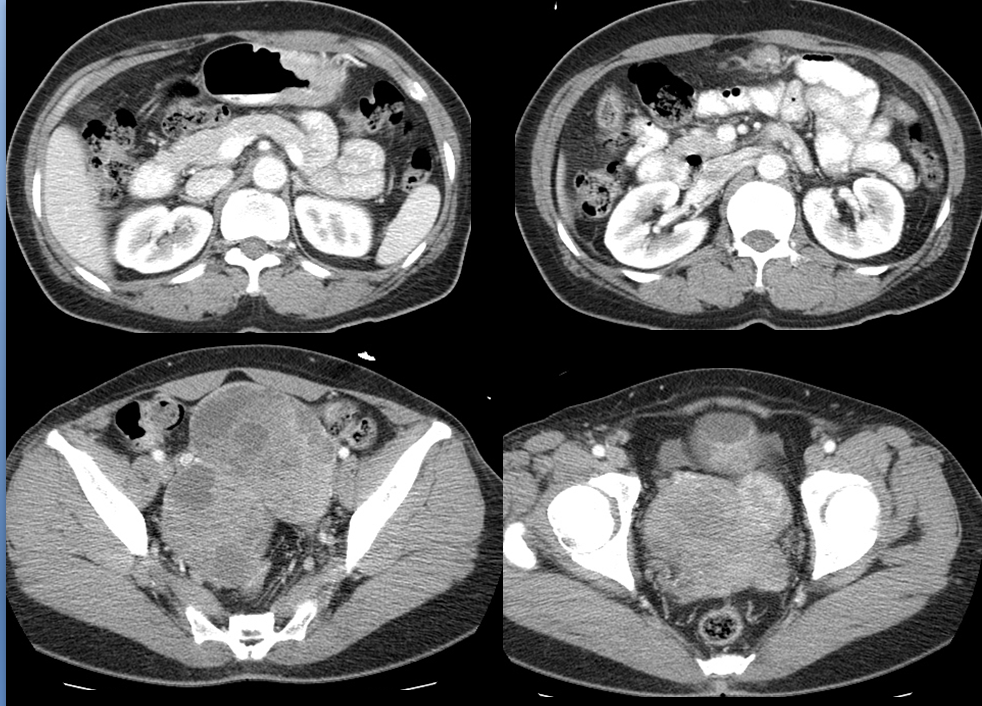

Solid and cystic bilateral ovarian masses
Prognostic factors
- Ovarian metastases from colorectal carcinoma are often unresponsive to chemotherapy and are associated with poor survival (Cancer 2017;123:1134)
Case reports
- 37 year old woman with primary jejunal adenocarcinoma presenting as bilateral ovarian metastasis (Gastroenterology Res 2017;10:366)
- 57 year old Japanese woman with malignant phyllodes tumor of the breast metastasizing to the ovary (Int J Surg Pathol 2022;30:427)
- 61 year old woman with metastatic angiosarcoma to an ovarian Brenner tumor (Int J Gynecol Pathol 2023;42:176)
- 64 year old woman with isolated ovarian metastasis from pancreatic adenocarcinoma and the role of molecular analysis in establishing diagnosis (J Pancreat Cancer 2021;7:74)
- 66 year old woman with primary colorectal carcinoma and metachronous ovarian metastasis (Am J Case Rep 2019;20:1515)
Treatment
- Debulking surgery with or without chemotherapy
Gross description
- Bilateral ovarian involvement (overall occurs in 40 - 80% of cases)
- Primary mucinous ovarian tumors, uncommonly bilateral
- Size: usually < 10 cm
- Generally applied to metastatic mucinous tumors, though may be less reliable than previously reported (Gynecol Oncol 2006;101:152)
- Multinodular, solid and cystic, or friable
- Surface involvement
- Hilar involvement (common in hematogenous spread)
Gross images
Images hosted on other servers:

Bilateral ovarian masses with multinodular cut surfaces
Microscopic (histologic) description
- Morphology varies with appearance of primary tumor
- General features
- Involvement of ovarian surface and superficial cortex
- Infiltrative growth pattern with stromal desmoplasia
- Heterogenous nodular invasive growth (Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019)
- Metastatic tumors more often envelop preexisting normal ovarian structures than primary tumors
- Extensive lymphovascular invasion
- Colorectal adenocarcinoma
- Dilated glands with cribriform epithelium draped along the periphery of luminal dirty necrosis (garland pattern)
- Low grade appendiceal mucinous neoplasm
- Hypermucinous columnar epithelium with low grade cytologic atypia
- Retraction of epithelium from underlying stroma is commonly seen
- Abundant pseudomyxoma ovarii
- Gastric carcinoma
- Frequently presents as Krukenberg tumor (composed predominantly of signet ring cells)
- Stroma may alternate from hypercellular to hypocellular (edematous)
- Breast carcinoma
- Lobular or ductal differentiation
- Signet ring cells may be present
- Endocervical adenocarcinoma
- HPV associated
- Variety of glandular patterns
- Epithelium with hyperchromatic nuclei, apical mitoses, basal apoptoses
- HPV independent, gastric type
- Mucinous epithelium with clear / pale cytoplasm with distinct borders
- Cytologic atypia may range from minimal to severe
- HPV associated
- Endometrial adenocarcinoma
- Endometrioid histotype is more common than serous
- Synchronous endometrial and ovarian endometrioid carcinomas
- May apply Scully criteria, though recent studies suggest that these neoplasms are clonally related (J Natl Cancer Inst 2016;108:djv427, J Natl Cancer Inst 2016;108:djv428)
- Melanoma
- Follicle-like spaces are frequently seen
- Diffuse or nodular growth is common
- Intracytoplasmic melanin pigment
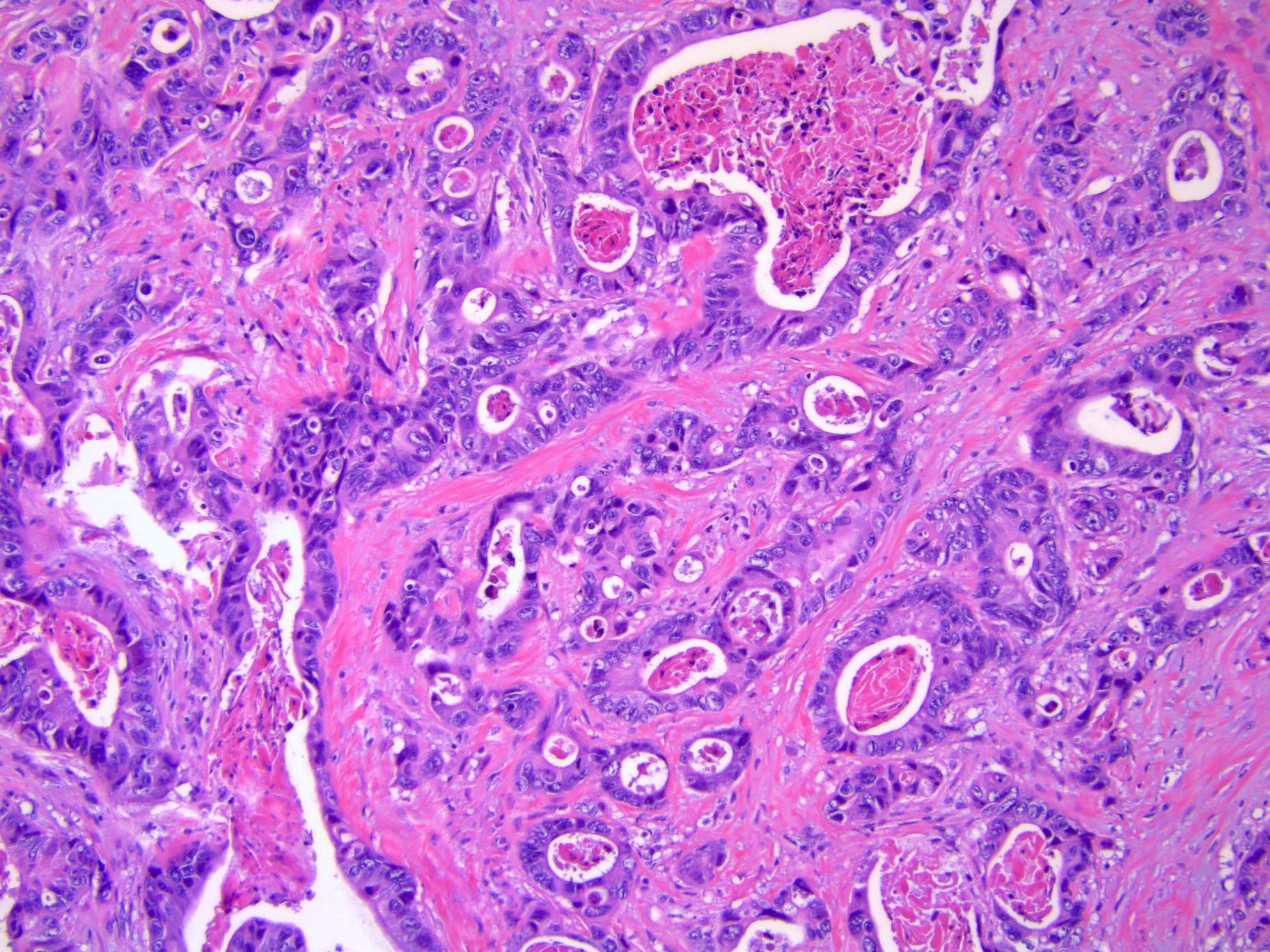
Microscopic (histologic) images
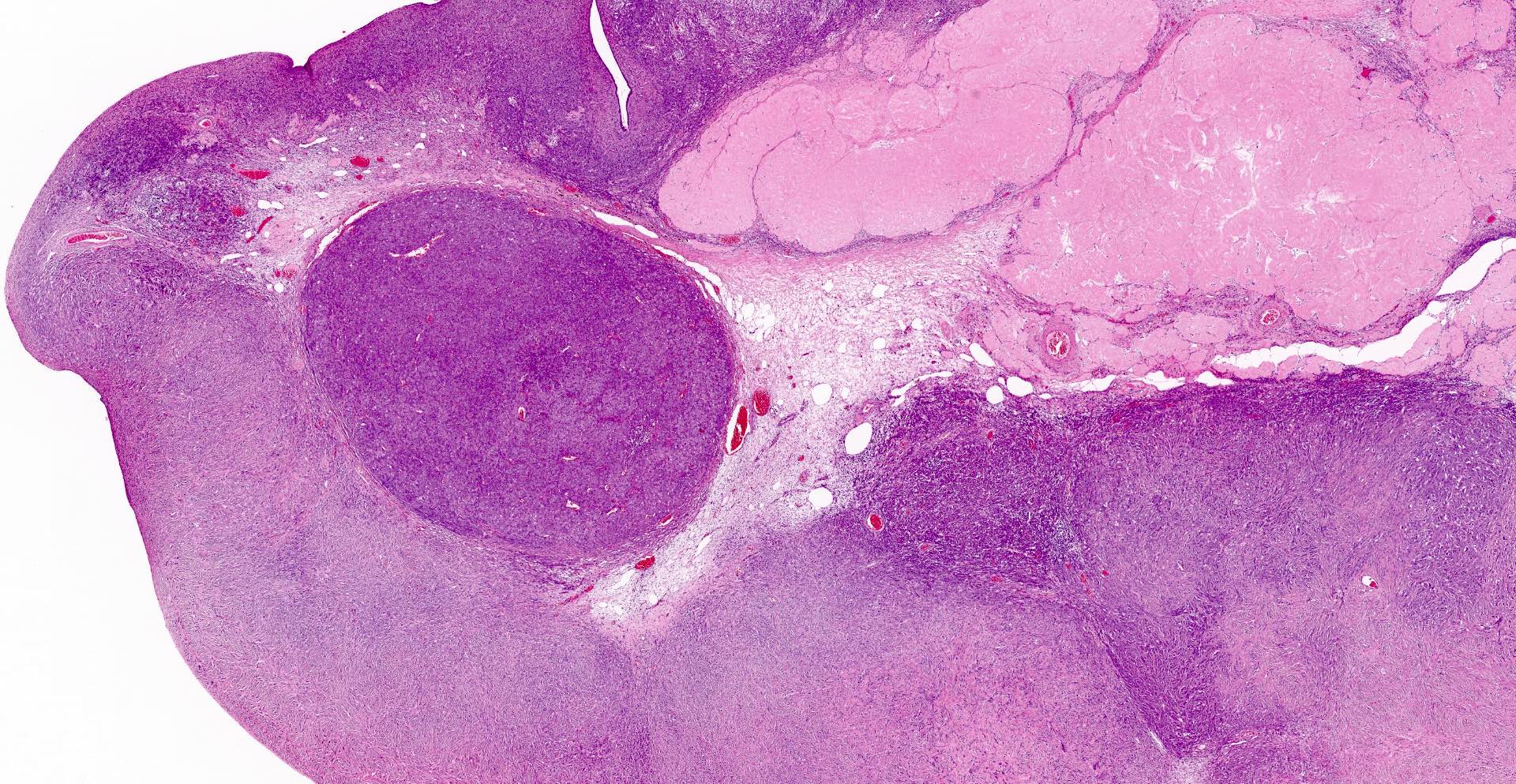
Contributed by Lucy Ma, M.D.
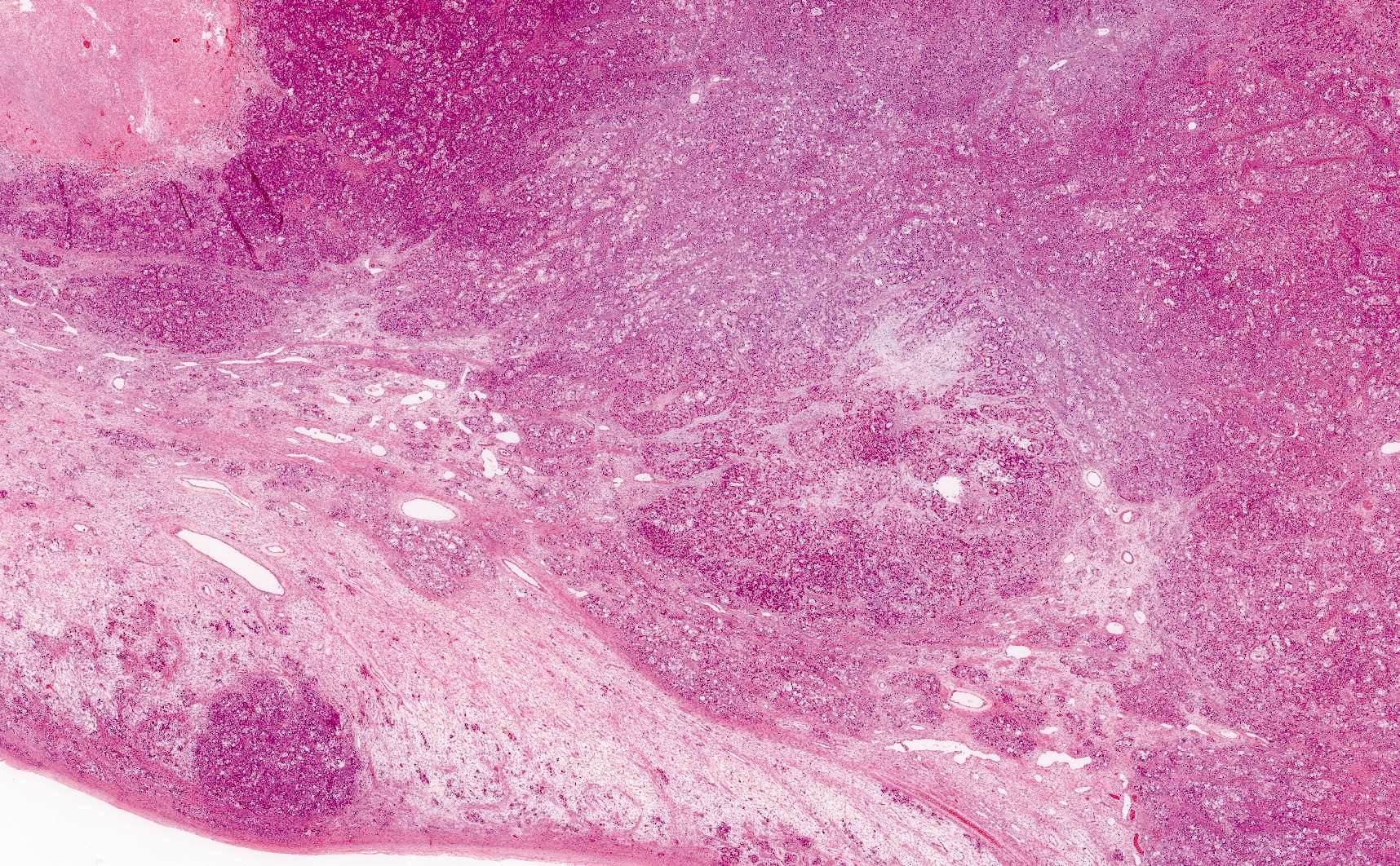
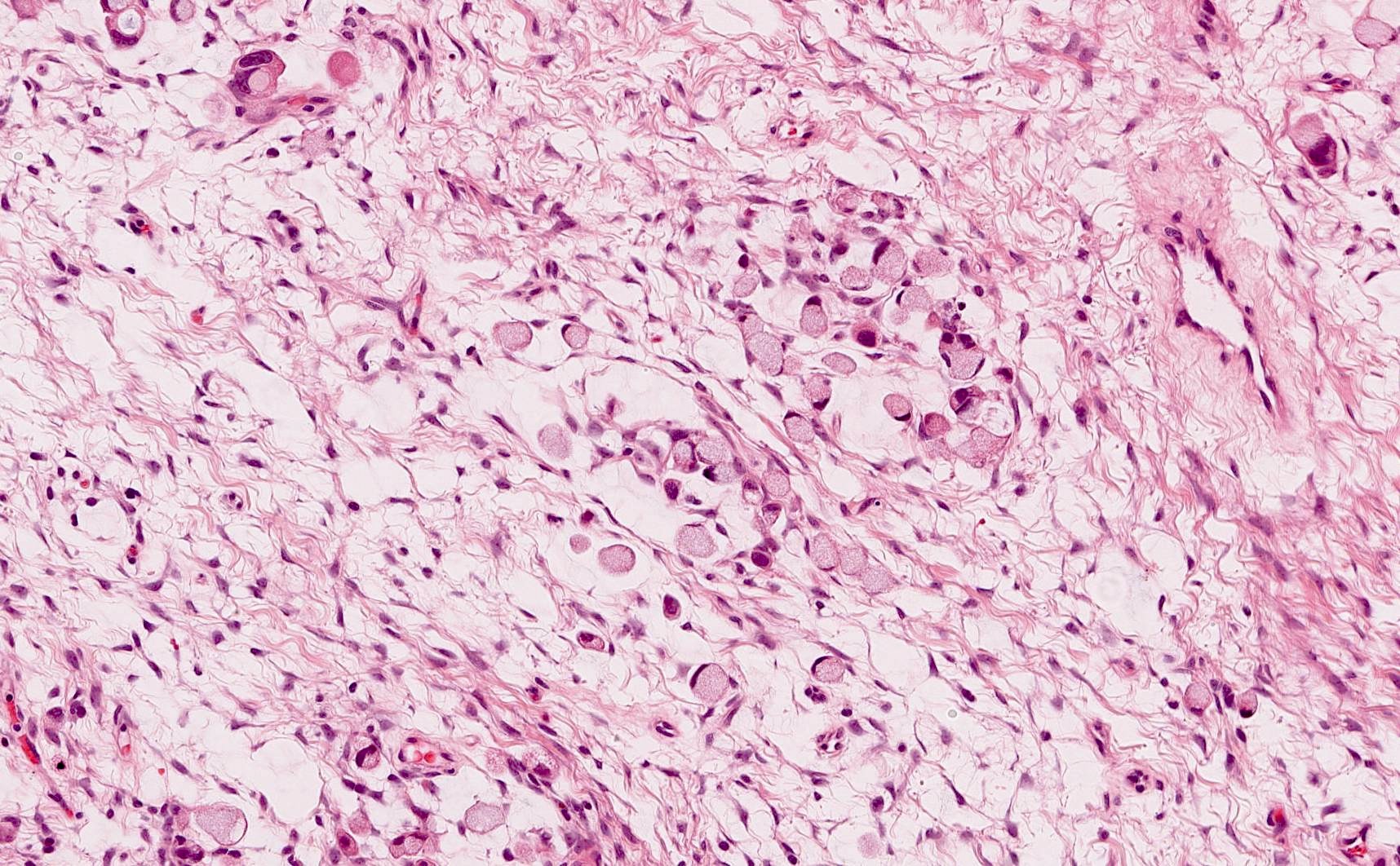
Krukenberg tumor
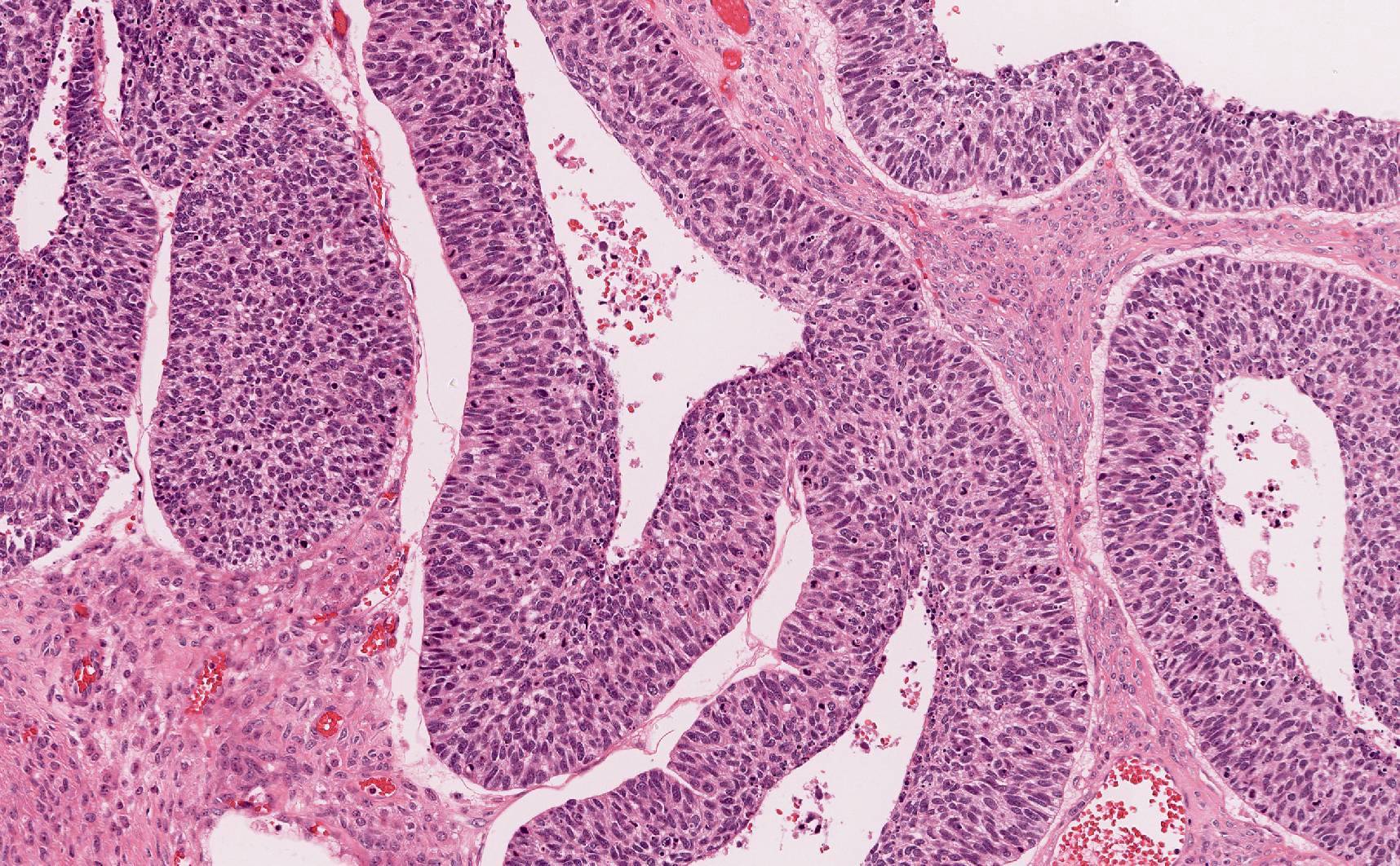
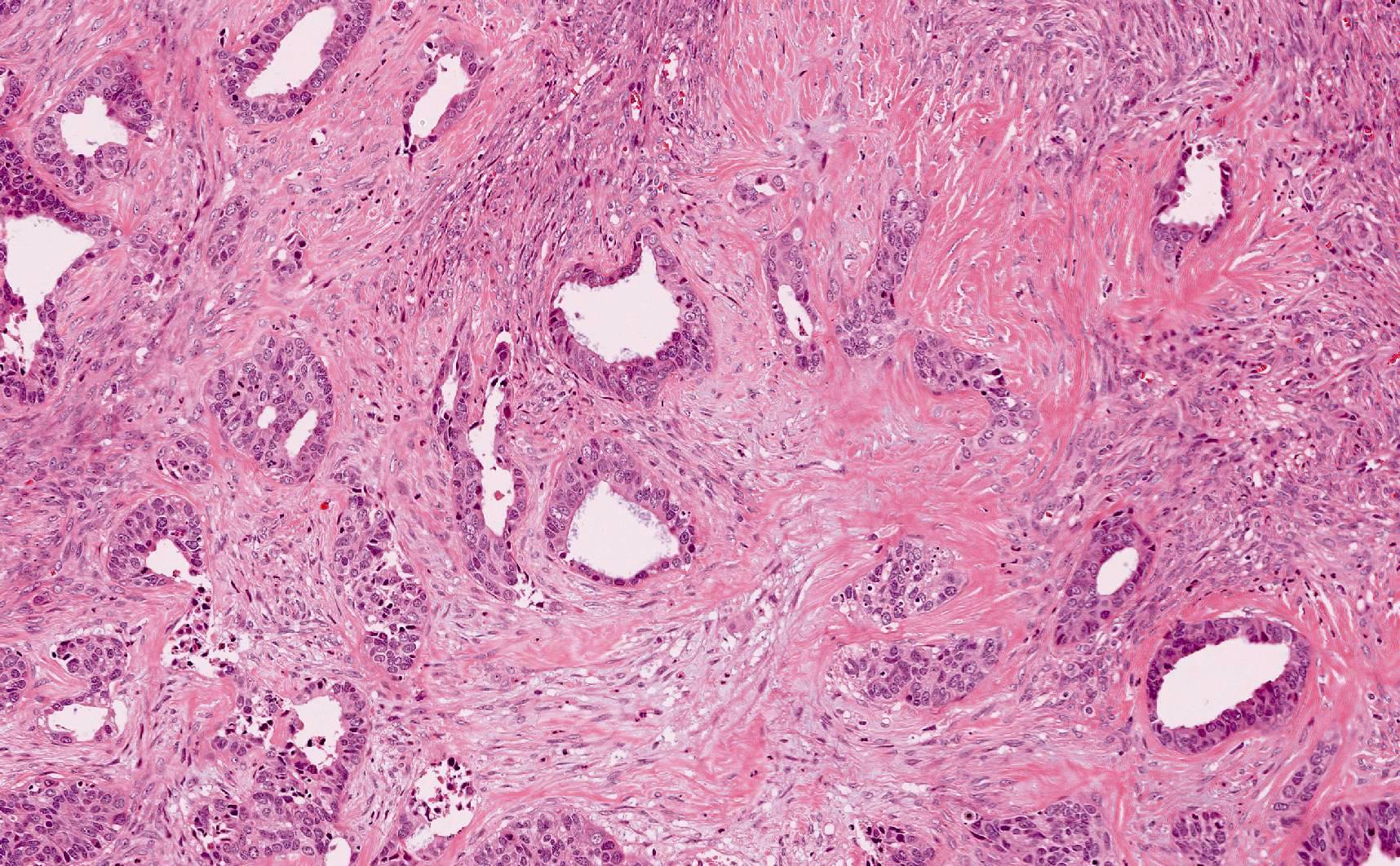
Metastatic cervical adenosquamous carcinoma
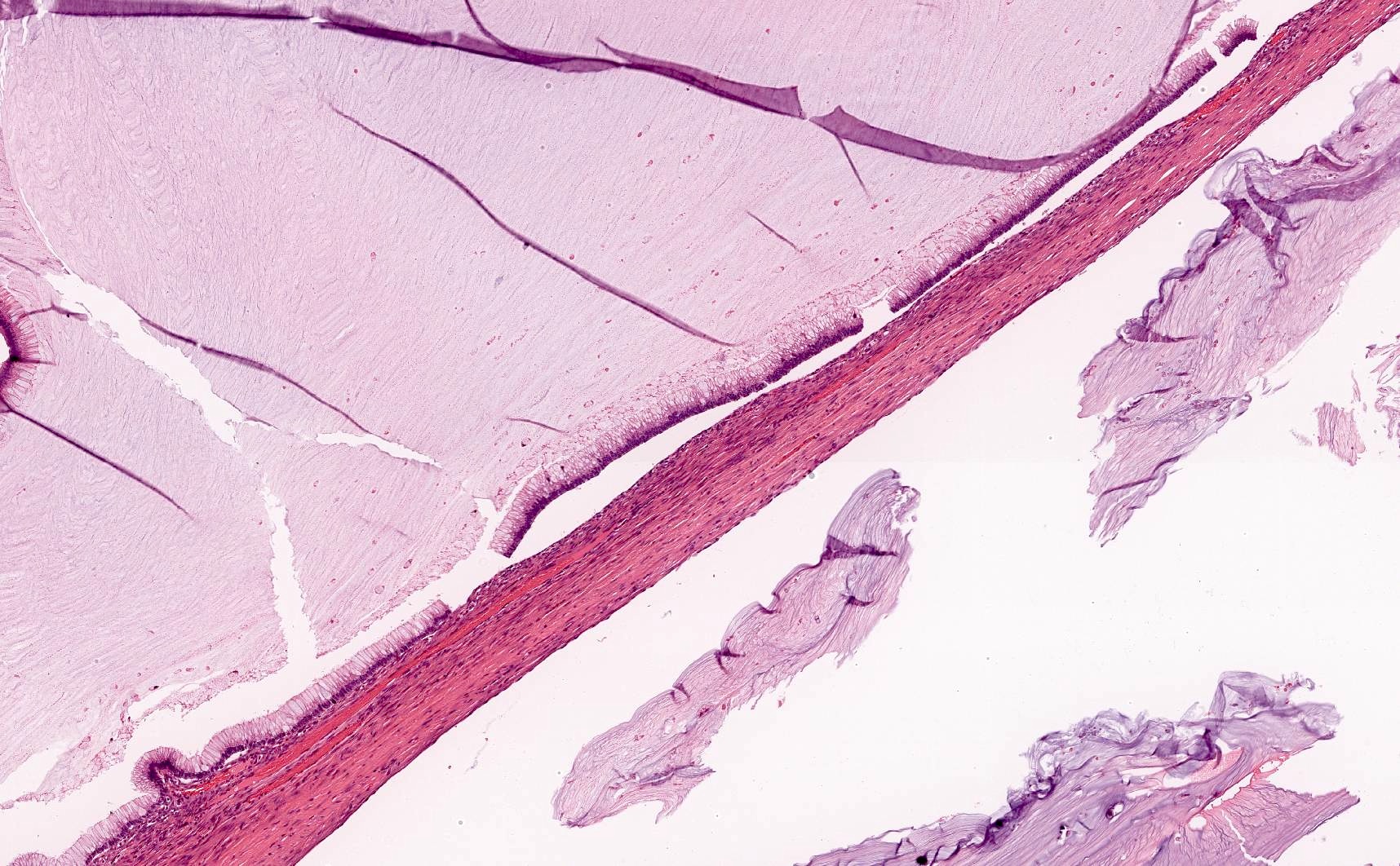
Metastatic low
grade appendiceal
mucinous
neoplasm
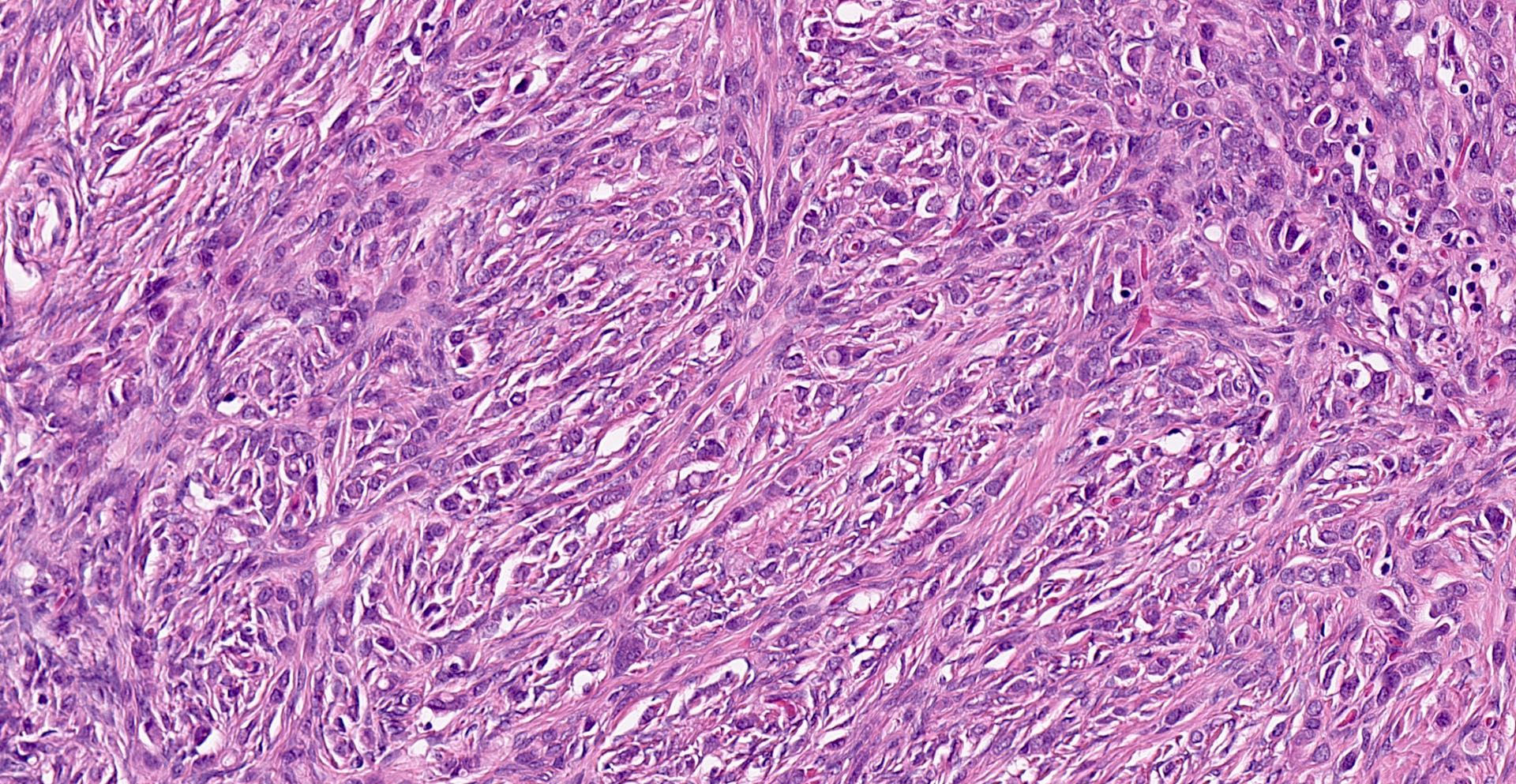
Metastatic lobular breast carcinoma
Virtual slides
Images hosted on other servers:

Metastatic breast carcinoma to the ovary

Metastatic malignant melanoma to the ovary

Metastatic pancreatic adenocarcinoma to the ovary

Metastatic hepatocellular carcinoma to the ovary
Positive stains
- Depends on the primary tumor
- References: J Clin Pathol 2012;65:596, Int J Gynecol Pathol 2015;34:257
Negative stains
Molecular / cytogenetics description
- KRAS, SMAD4 and NTKR1 mutations are more frequent in cases of ovarian metastasis from colorectal carcinoma than in cases of colorectal carcinoma without ovarian metastasis (Cancer 2017;123:1134)
Sample pathology report
- Fallopian tube and ovary, right and left, bilateral salpingo-oophorectomy:
- Metastatic carcinoma, consistent with patient's known history of breast primary, involving bilateral ovaries (see comment)
- Bilateral fallopian tubes, negative for tumor
- Comment: On immunohistochemistry, the tumor cells are positive for GATA3, mammaglobin and GCDFP-15, while negative for PAX8. These findings support the diagnosis above.
Differential diagnosis
- Primary ovarian mucinous cystic tumor:
- Differential diagnosis for metastatic low grade appendiceal mucinous neoplasm
- Typically unilateral
- Rarely associated with pseudomyxoma peritonei
- May be associated with Brenner tumor or mature cystic teratoma
- CK7+, CK20-, SATB2-
- Primary ovarian endometrioid carcinoma:
- Differential diagnosis for metastatic colorectal adenocarcinoma
- Commonly associated with endometriosis or adenofibromatous component
- Squamous differentiation may be seen
- CK7+, ER+, PAX8+
- Differential diagnosis for metastatic endometrial endometrioid carcinoma in cases of synchronous endometrial and ovarian endometrioid carcinomas
- Scully criteria favoring primary ovarian endometrioid carcinoma (Scully: Tumors of the Ovary, Maldeveloped Gonads, Fallopian Tube, and Broad Ligament: Atlas of Tumor Pathology, 1st Edition, 1998)
- Associated with endometriosis or endometriotic lesions, a subset of which are clonal and demonstrate cancer associated mutations (J Pathol 2015;236:201)
- Low grade (FIGO grade 1 or 2)
- Histologic dissimilarity between ovarian and endometrial tumors
- No or superficial myometrial invasion of endometrial tumor
- No vascular space invasion, surface implants,or predominantly hilar location in ovary
- Ovarian tumor is unilateral
- Regardless of histopathologic criteria, genomic studies suggest that most cases are clonally related (J Natl Cancer Inst 2016;108:djv427, J Natl Cancer Inst 2016;108:djv428)
- Clonal relationship may not apply to Lynch syndrome patients (Mod Pathol 2021;34:994)
- Scully criteria favoring primary ovarian endometrioid carcinoma (Scully: Tumors of the Ovary, Maldeveloped Gonads, Fallopian Tube, and Broad Ligament: Atlas of Tumor Pathology, 1st Edition, 1998)
- Differential diagnosis for metastatic colorectal adenocarcinoma
- Signet ring stromal tumor of the ovary:
- Differential diagnosis for metastatic signet ring cell carcinoma
- Signet ring morphology in a background of fibromatous stroma
- Signet ring cells contain a single large nonmucinous intracytoplasmic vacuole
- Eosinophilic hyaline globules are common
- SF1+, calretinin+, EMA-
Board review style question #1
A 65 year old woman with an ovarian mass undergoes an oophorectomy. A representative section of the mass is shown above. Which of the following immunoprofiles best supports a diagnosis of metastatic colorectal adenocarcinoma?
- CK7+, CK20+, PAX8-, GATA3+, CDX2-, SATB2-
- CK7+, CK20-, PAX8+, GATA3-, CDX2+, SATB2-
- CK7-, CK20+, PAX8-, GATA3-, CDX2+, SATB2+
- CK7-, CK20-, PAX8-, GATA3-, CDX2-, SATB2-
Board review style answer #1
C. CK7-, CK20+, PAX8-, GATA3-, CDX2+, SATB2+. Compared with the other answer choices, this immunoprofile best supports a colorectal adenocarcinoma primary, which is typically CK7-, CK20+, PAX8-, GATA3-, CDX2+ and SATB2+. Answer A is incorrect as it fits the immunoprofile for a metastatic urothelial carcinoma. Answer B is incorrect as it is more consistent with a primary ovarian endometrioid carcinoma. Answer D is incorrect as it is not immunoreactive to any typical adenocarcinoma markers.
Comment Here
Reference: Metastases to ovary
Comment Here
Reference: Metastases to ovary
Board review style question #2
Which of the following organs is the most common site of metastasis within the gynecologic tract?
- Cervix
- Endometrium
- Fallopian tube
- Ovary
- Vulva
Board review style answer #2
D. Ovary. The ovary is the most common site of metastasis within the gynecologic tract. Answers A, B, C and E are incorrect because the vagina is the second most frequent site of metastasis within the gynecologic tract following the ovary (Cancer 1984;53:1978).
Comment Here
Reference: Metastases to ovary
Comment Here
Reference: Metastases to ovary

