

Ovary
Sex cord stromal tumors
Pure stromal tumors
Leydig cell tumor
Editorial Board Member: Lucy Ma, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 11 September 2024
Last staff update: 11 September 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed search: Leydig cell tumor


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Lengyel K, Hanley K. Leydig cell tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarytumorleydig.html. Accessed December 25th, 2024.
Definition / general
- Benign steroid cell tumor composed of polygonal cells with abundant eosinophilic cytoplasm and Reinke crystals
Essential features
- Postmenopausal occurrence
- Predominantly located in the ovarian hilus, close to nerve fibers
- Often lobulated or nodular growth
- Reinke cytoplasmic crystals present
Terminology
- Hilus cell tumor (not recommended)
ICD coding
- ICD-10: D27.9 - benign neoplasm of unspecified ovary
- ICD-11: 2F32.Y & XH5XQ2 - other specified benign neoplasm of ovary & Leydig cell tumor of the ovary, NOS
Epidemiology
- 15 - 20% of ovarian steroid cell tumors
- Age range: 32 - 82 years (mean: 58 years) (Int J Gynecol Pathol 1989;8:299)
Etiology
- Arise from ovarian hilus cells that resemble the Leydig cells of the testis
Clinical features
- May cause elevated levels of serum testosterone and urinary 17 ketosteroids
- Androgenic symptoms, rarely estrogenic (Int J Gynecol Pathol 1989;8:299)
- Hirsutism, baldness, voice changes, male pattern musculature, clitoromegaly
Diagnosis
- May be incidental
- Unilateral adnexal mass, may be noted on ultrasound
- WHO (5th edition) criteria
- Essential: well circumscribed tumor centered in the ovarian hilus, consisting of bland steroid cells
- Desirable: cytoplasmic Reinke crystals
Radiology description
- Ultrasound: large mass with heterogenous appearance is commonly seen; however, this is characteristic of sex cord stromal tumors in general (J Oncol Pract 2016;12:940)
Prognostic factors
- Almost always benign
Case reports
- 39 year old woman (gravida 1, para 1) who presented with a high serum testosterone level and secondary amenorrhea, hirsutism and weight gain (Case Rep Womens Health 2021;30:e00298)
- 55 year old postmenopausal woman who presented with a 3 year history of frontal balding and virilization (J Clin Endocrinol Metab 2014;99:12)
- 71 year old woman who presented with postmenopausal hirsutism with 10 years of evolution (BMJ Case Rep 2021;14:e240937)
Treatment
- Surgical removal - oophorectomy
Gross description
- Unilateral, lobulated, solid mass
- Yellow, orange or red-brown soft cut surface
- May have multifocal hemorrhagic areas
- Mostly < 5.0 cm (mean: 2.5 cm) but may be up to 15 cm (Int J Gynecol Pathol 1989;8:299)
Gross images
AFIP images
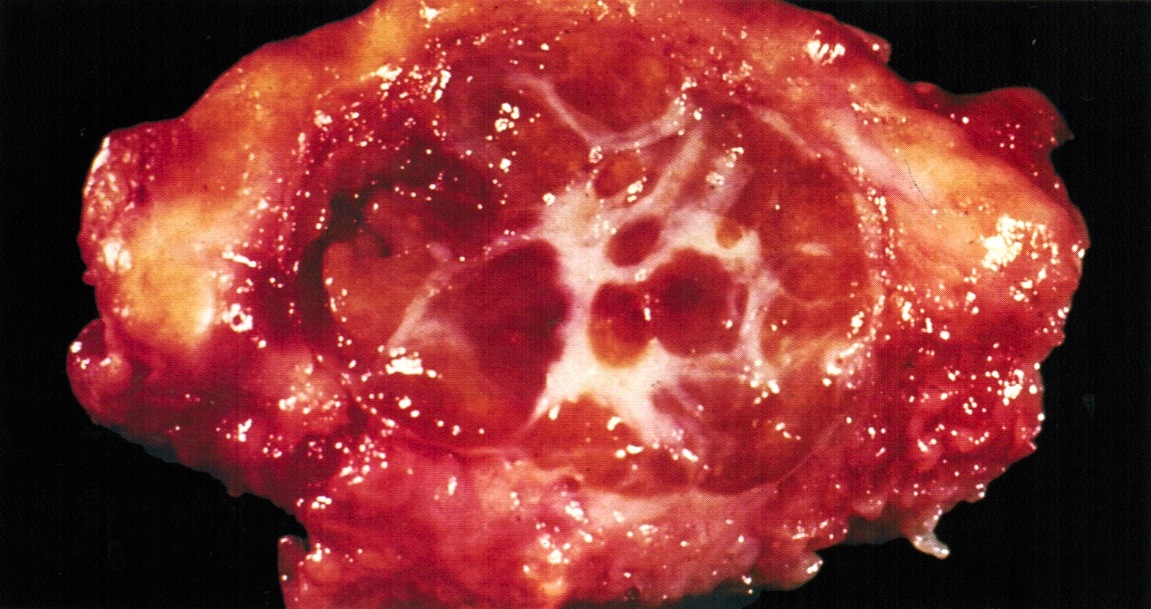
Red-brown mass
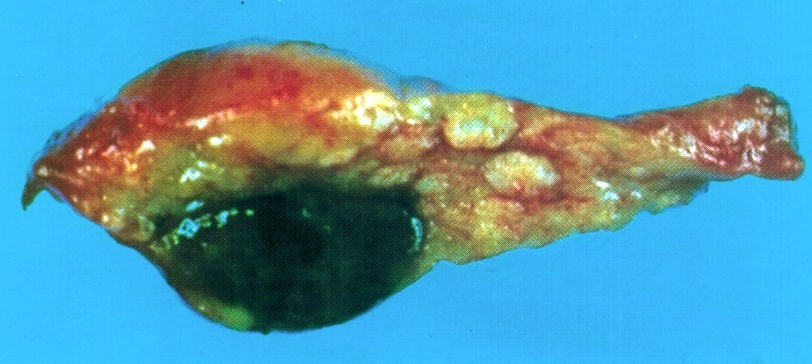
Brown-black nodule
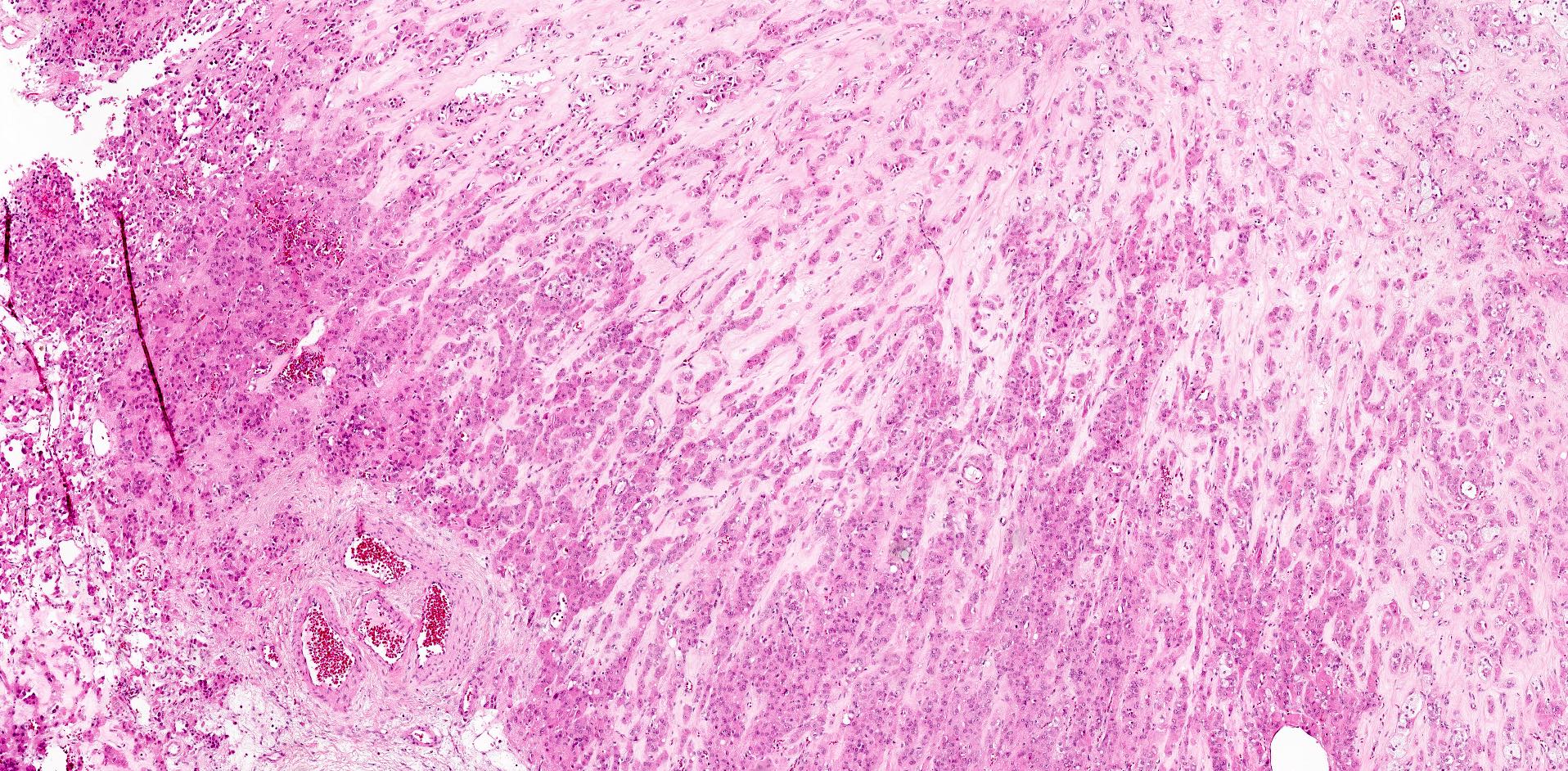
Microscopic (histologic) description
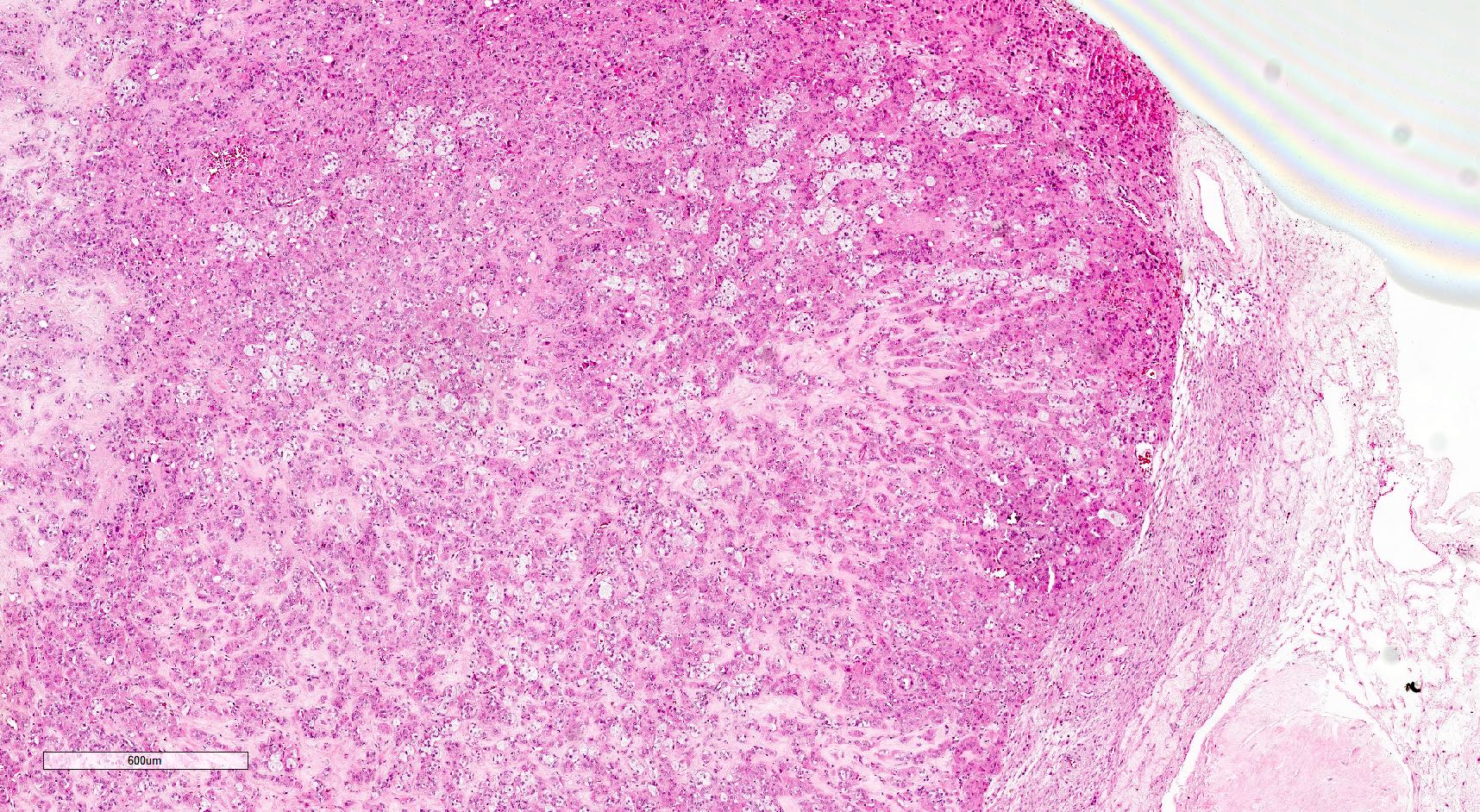
- Unencapsulated neoplasms with smooth or irregular borders located in the hilus, next to nonmedullary nerve fibers
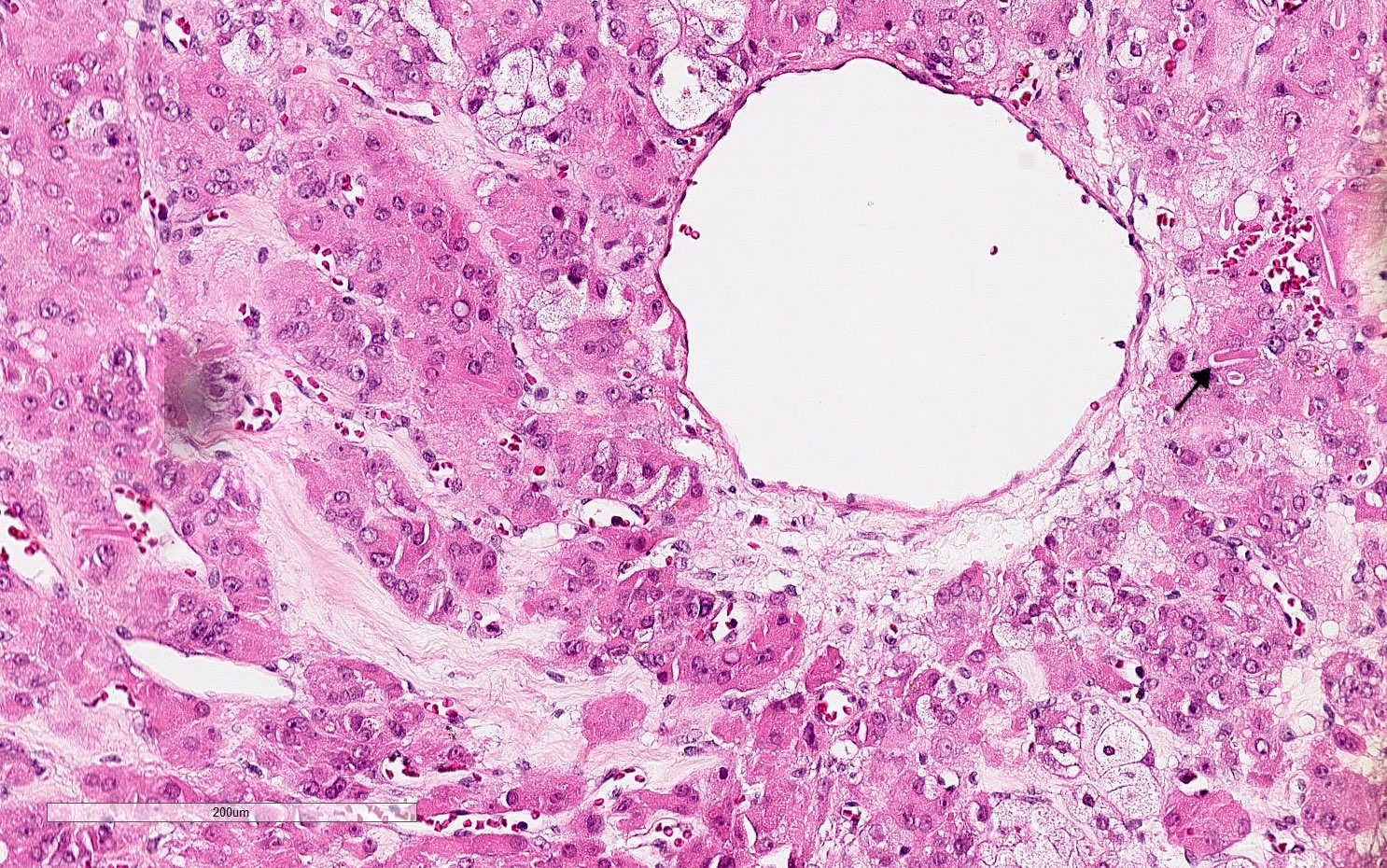
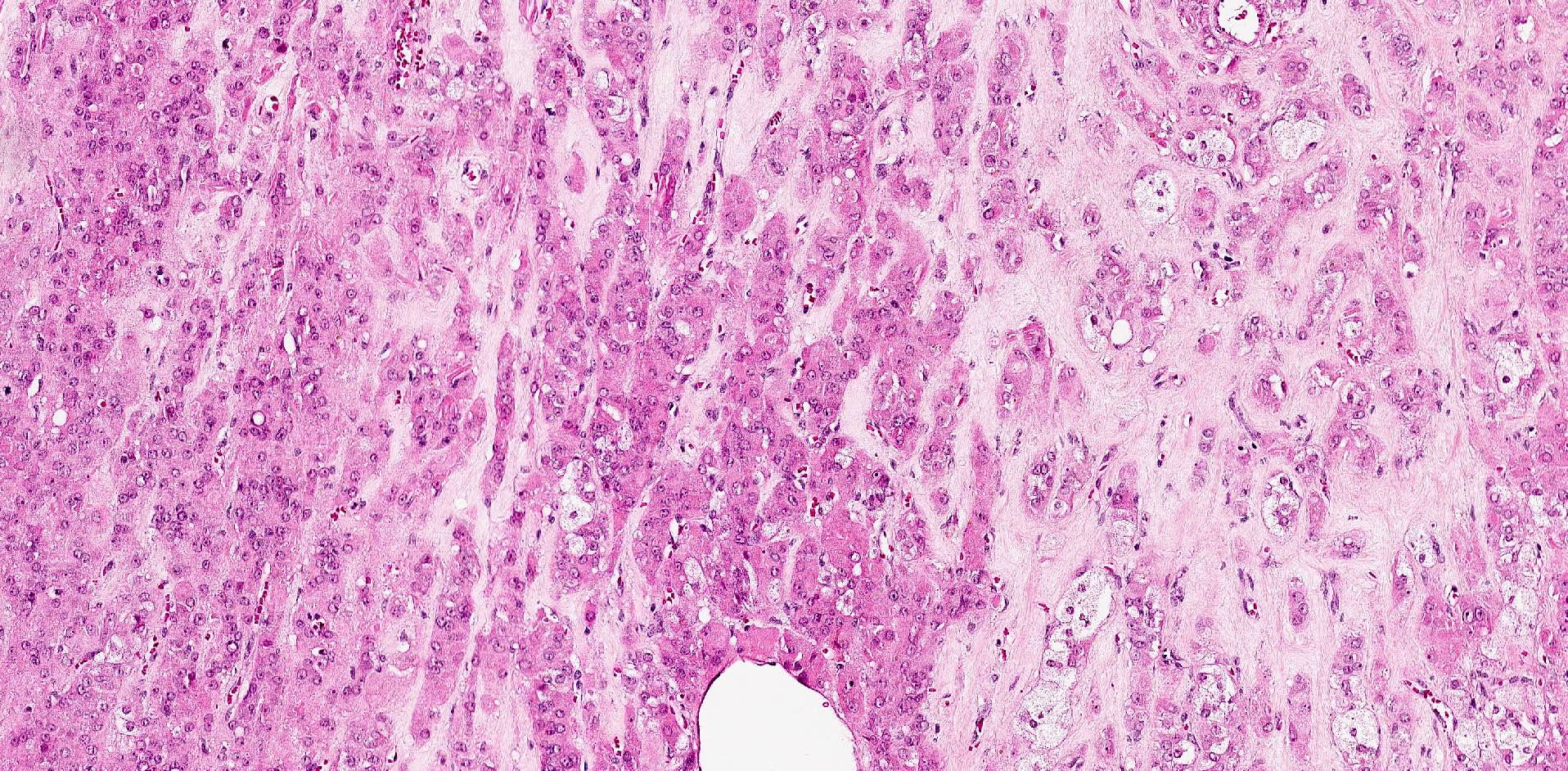
- Round to polygonal cells with abundant eosinophilic or vacuolated cytoplasm and round nuclei with small nucleoli
- Reinke crystals: eosinophilic, cytoplasmic rod, rectangular or hexagonal crystals
- Lipochrome pigment is common
- May have cytoplasmic pseudoinclusions or bizarre nuclear atypia
- May have diffuse or lobulated or nodular growth with collagenous septa
- Sheets, nests or rarely cords
- Variably hyalinized or edematous stroma
- May have nuclear clustering with intervening acellular zones
- Fibrinoid degeneration of vessel walls (characteristic)
- May have background hilar cell hyperplasia (Nucci: Gynecologic Pathology - A Volume in Foundations in Diagnostic Pathology Series, 2nd Edition, 2020)
Microscopic (histologic) images
Contributed by Krisztina Lengyel, M.D., Lucy Ma, M.D. and AFIP
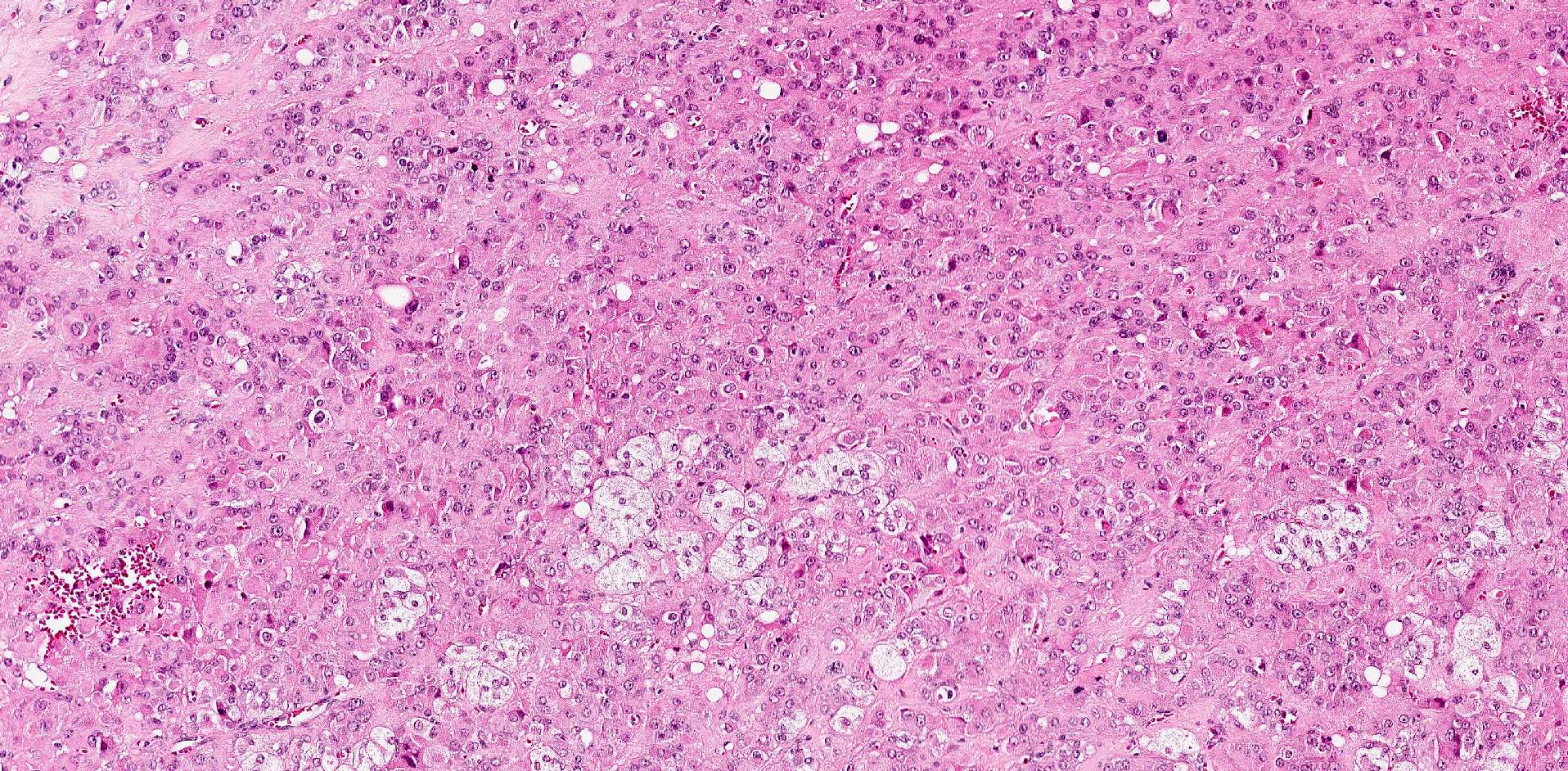
Eosinophilic clusters
Eosinophilic cells in cords and clusters
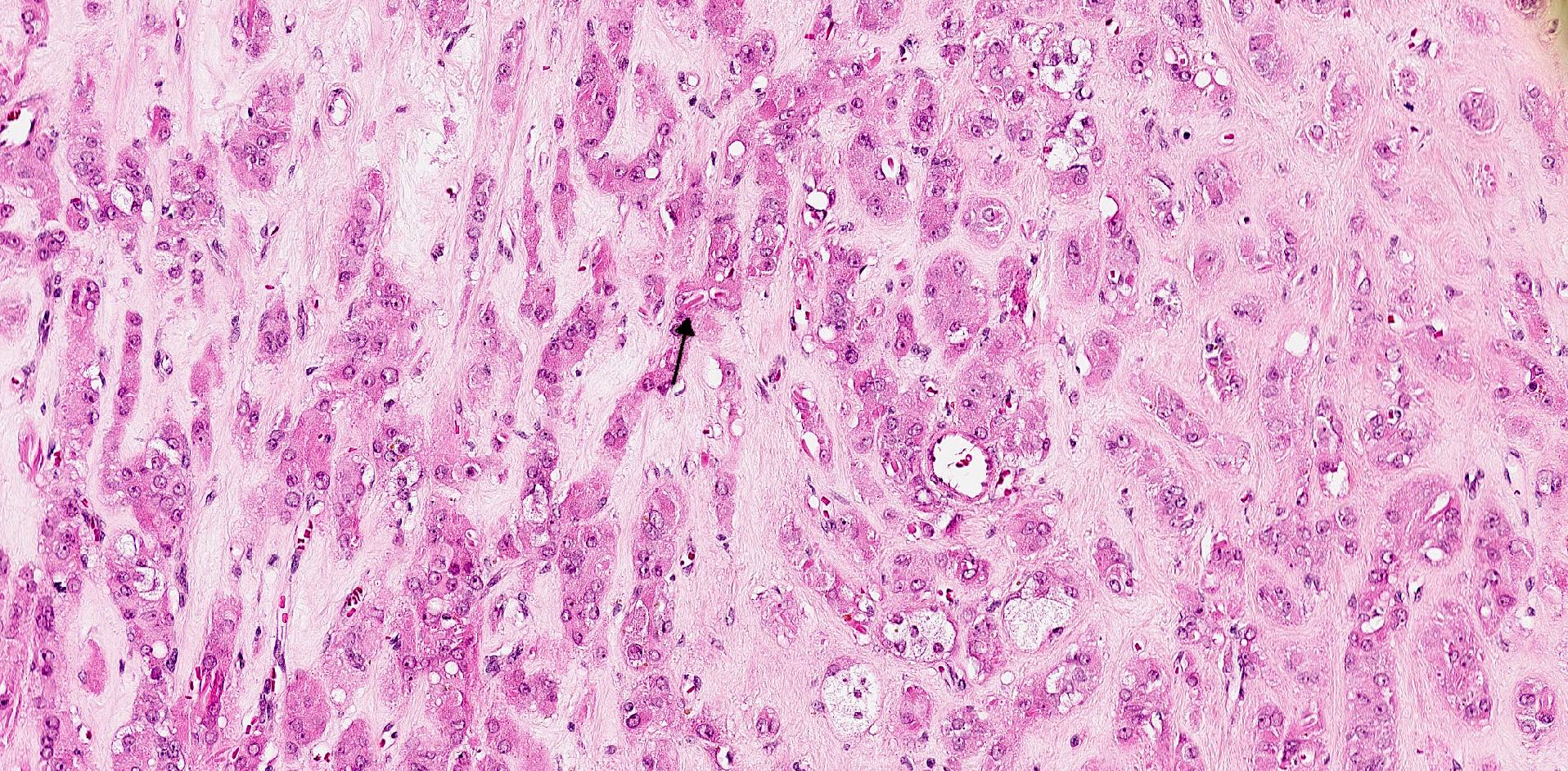
Eosinophilic Leydig cells with Reinke crystals
Reinke crystals
Eosinophilic Leydig cells
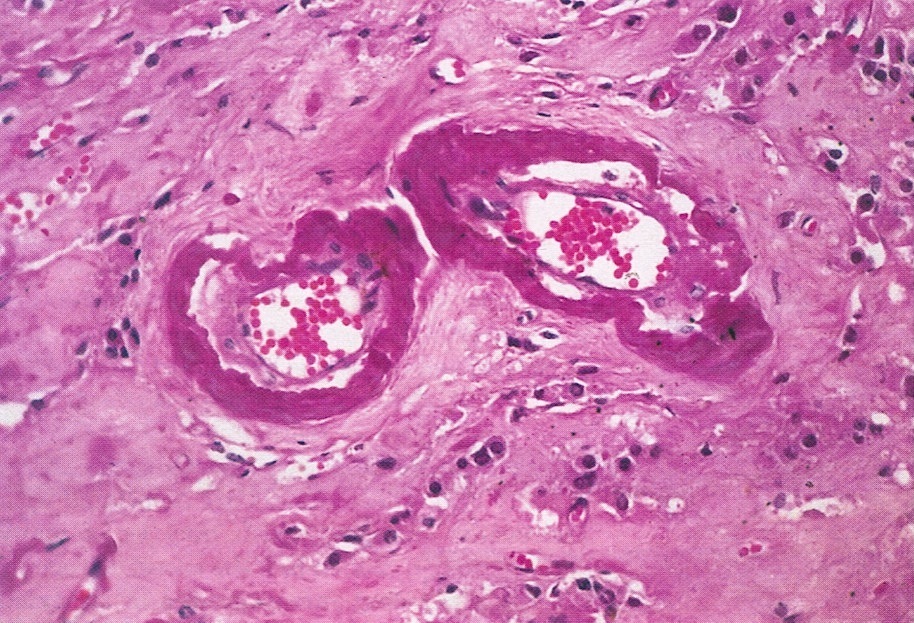
Fibrinoid replacement
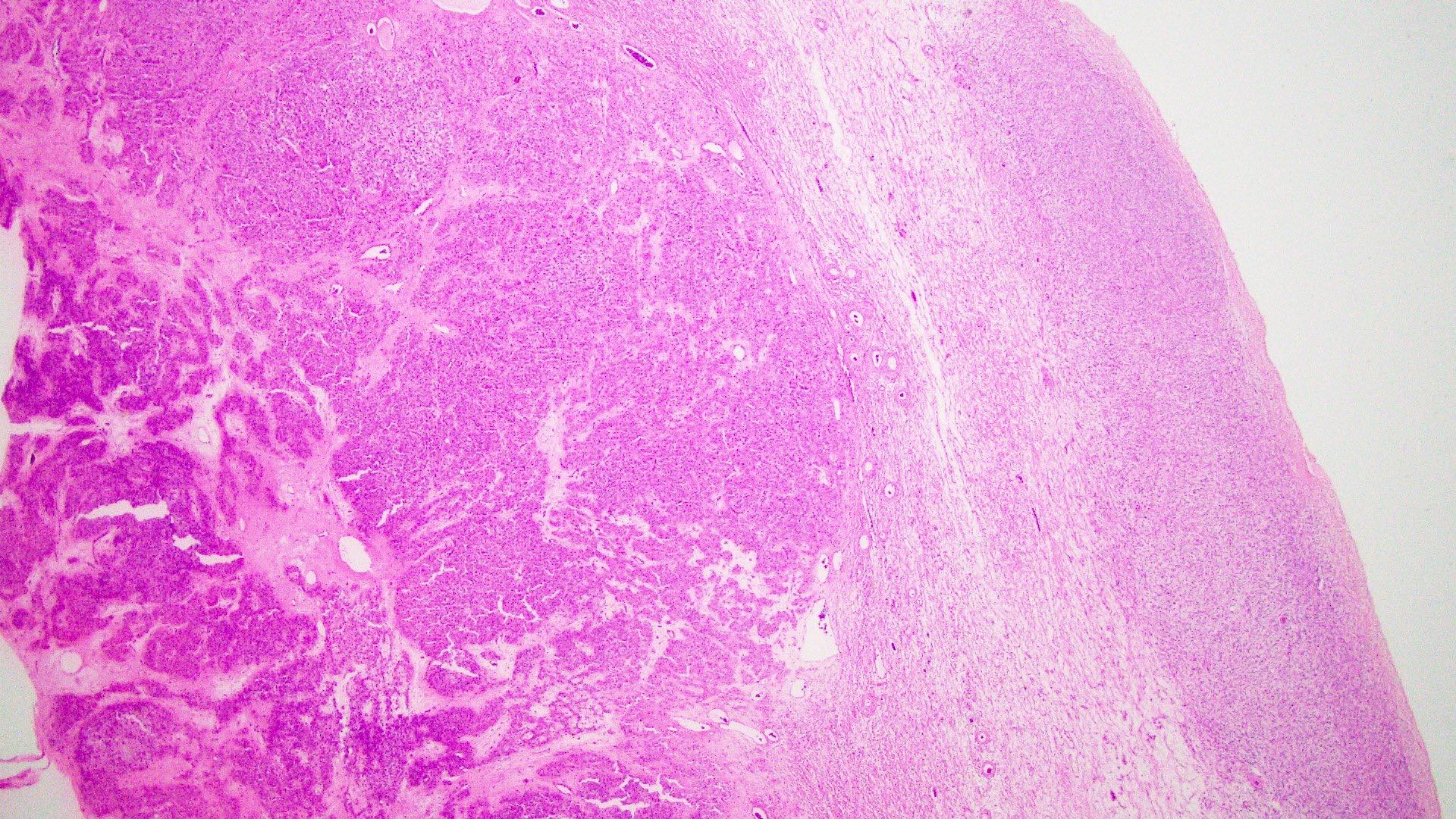
Hilar based steroid cell tumor
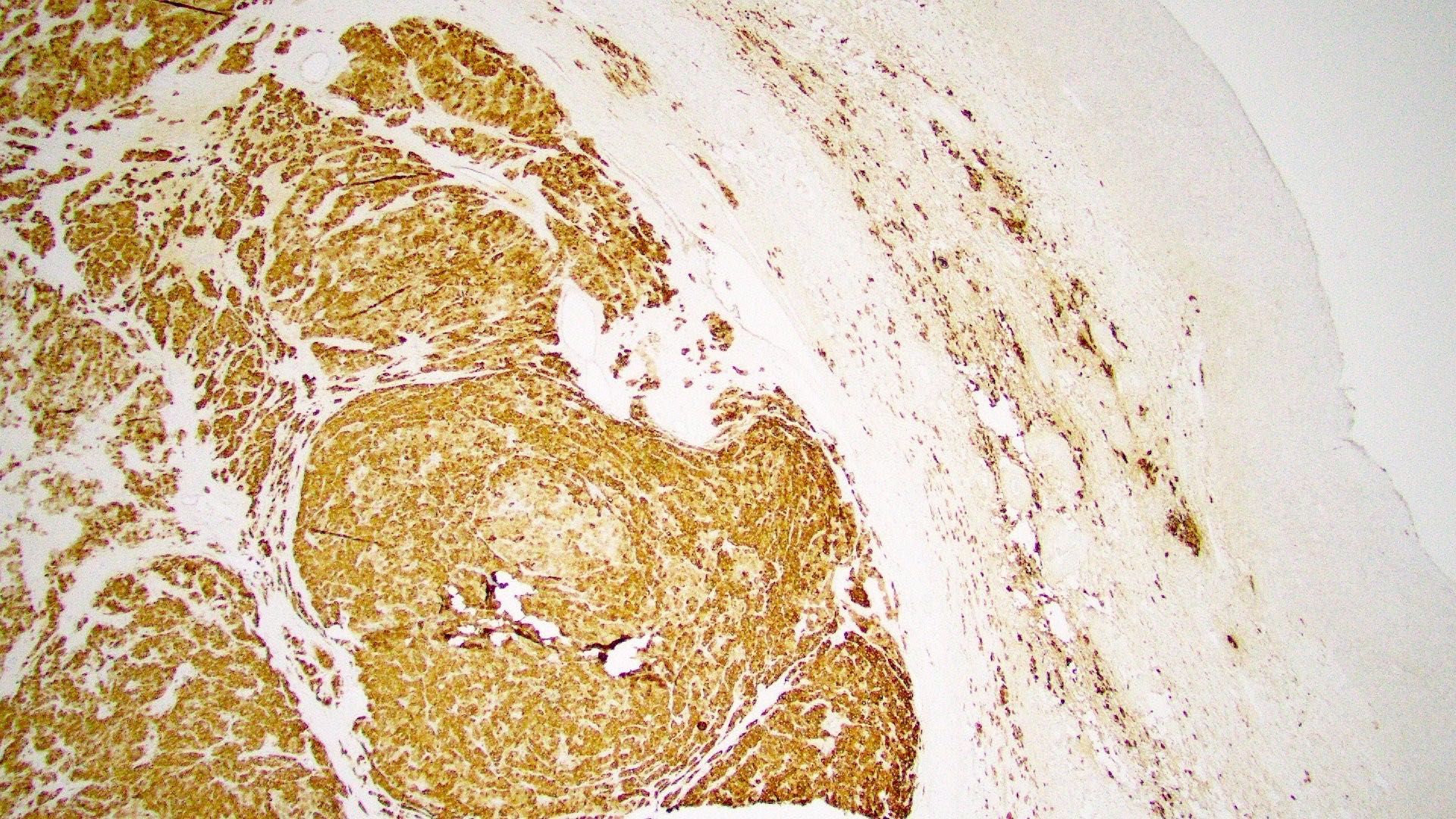
Inhibin positive
Positive stains
Negative stains
Sample pathology report
- Ovary, right, oophorectomy:
- Leydig cell tumor (see comment)
- Comment: The right ovary shows a well circumscribed tumor centered in the ovarian hilus, consisting of bland steroid cell containing cytoplasmic Reinke crystals and measuring 3 cm. Leydig / hilus cell hyperplasia is identified in the adjacent right ovarian tissue.
Differential diagnosis
- Stromal luteoma:
- More commonly presents with estrogenic manifestations
- Located in the ovarian parenchyma
- Irregularly shaped pseudoacini may be present
- Commonly associated with stromal hyperthecosis
- No Reinke crystals
- Pregnancy luteoma:
- Occurs during pregnancy and puerperium
- Multiple and bilateral
- Follicle-like spaces
- No Reinke crystals
- Stromal hyperthecosis:
- Located in the ovarian cortex
- Nodular aggregates of lutein cells < 1.0 cm
- No Reinke crystals
Additional references
Board review style question #1
A 45 year old woman presents with hirsutism, deepening of the voice and clitoromegaly. Imaging reveals a unilateral solid ovarian mass. Which of the following is the most likely diagnosis?
- Adult granulosa cell tumor
- Dysgerminoma
- Fibroma
- Leydig cell tumor
- Thecoma
Board review style answer #1
D. Leydig cell tumor. Leydig cell tumors usually present in postmenopausal women with androgenic manifestations (hirsutism, voice deepening, clitoromegaly). Answer A is incorrect because adult granulosa cell tumors usually present with estrogenic manifestations such as abnormal uterine bleeding and concomitant endometrial thickening / hyperplasia. Answer E is incorrect because thecoma is an ovarian stromal tumor composed predominantly of cells resembling theca cells and presents more frequently with estrogenic symptoms or with symptoms related to an adnexal mass. Answer C is incorrect because fibromas are associated with Gorlin syndrome (nevoid basal cell carcinoma syndrome) or Meigs syndrome (ascites and pleural effusion). Answer B is incorrect because dysgerminomas arise in children or young women, with abdominal pain and a mass with elevated lactic dehydrogenase (LDH).
Comment Here
Reference: Leydig cell tumor
Comment Here
Reference: Leydig cell tumor
Board review style question #2
A 71 year old woman underwent a total abdominal hysterectomy (TAH) and bilateral salpingo-oophorectomy (BSO) for abnormal uterine bleeding (AUB). She concomitantly reported hirsutism. An incidental finding in the left ovary showed the findings in the image above. What is true about this neoplasm?
- Cytoplasmic Reinke crystals are desirable but not essential for diagnosis of this tumor
- Patients present with estrogenic manifestation
- These neoplasms are frequently bilateral
- This tumor is associated with STK11
Board review style answer #2
A. Cytoplasmic Reinke crystals are desirable but not essential for diagnosis of this tumor. Cytoplasmic Reinke crystals occur rarely but are characteristic in Leydig cell tumor. In the WHO, these are in the desirable category and are not essential for the diagnosis of Leydig cell tumor if the tumor is located in the hilum. Answer D is incorrect because sex cord tumor with annular tubules (SCTAT) are associated with STK11 gene alterations. Answer B is incorrect because adult granulosa cell tumors present with estrogenic manifestations, whereas Leydig cell tumors present most commonly with androgenic manifestations. Answer C is incorrect because Leydig cell tumors most commonly occur unilaterally.
Comment Here
Reference: Leydig cell tumor
Comment Here
Reference: Leydig cell tumor

