
Ovary
Other nonneoplastic lesions
Endosalpingiosis
Editorial Board Member: Gulisa Turashvili, M.D., Ph.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 28 January 2022
Last staff update: 28 January 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Endosalpingiosis [TIAB] ovary


Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Busca A, Parra-Herran C. Endosalpingiosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarynontumorendosalpingiosis.html. Accessed April 2nd, 2025.
Definition / general
- Presence of ectopic glands lined by fallopian tube type ciliated epithelium
Essential features
- Defined as ectopic glands lined by fallopian tube type ciliated epithelium outside the fallopian tube
- Incidental finding in resection specimens
- Diagnosed by microscopic examination
- Dilated glands measure less than 1 cm in size (if more than 1 cm, serous cystadenoma)
Epidemiology
- Typically seen in women of reproductive age
- In 33% of cases, endosalpingiosis is associated with endometriosis (Gynecol Oncol 2016;142:255)
Sites
- Ovaries, omentum, fallopian tube serosa, uterine serosa, bladder, lymph nodes
Pathophysiology
- Multiple hypotheses, including distal fallopian tube implants in the ovarian cortex during ovulation or metaplastic changes of the ovarian surface epithelium or peritoneal cells (Reprod Sci 2013;20:1030)
- Papillary tubal hyperplasia (PTH) is a term that has been proposed to describe small rounded clusters of tubal epithelial cells and small papillae, with or without associated psammoma bodies, that are present within the tubal lumen; PTH has been linked to endosalpingiosis and serous tumor (Am J Surg Pathol 2011;35:1605)
Etiology
- No specific etiology identified
Clinical features
- Mostly asymptomatic and incidentally found in resection specimens
- Rarely mass forming cystic lesion or mass related symptoms (BMJ Case Rep 2014;2014:bcr2013201645)
Diagnosis
- By histopathological examination, with confirmation of morphology and exclusion of endometriosis
Radiology description
- Typically no specific imaging findings
- Multilocular cysts if mass forming (Abdom Imaging 2015;40:471)
Prognostic factors
- Considered a benign finding
- Relationship with development of epithelial malignancies is not clear but patients with endosalpingiosis have been found to be more likely to have concurrent endometriosis as well as uterine and ovarian cancer (Gynecol Oncol 2016;142:255)
Case reports
- 30 year old pregnant woman with cystic endosalpingiosis (Case Rep Obstet Gynecol 2016;2016:8621570)
- 31 year old woman with florid cystic endosalpingiosis, masquerading as a malignancy (BMJ Case Rep 2014;2014:bcr2013201645)
- 55 year old woman with florid cystic endosalpingiosis presenting as an ovarian cyst (Gynecol Minim Invasive Ther 2016;5:170)
Treatment
- Surgery for the mass forming lesions
Gross description
- Simple cysts on ovarian surface
- Florid cystic endosalpingiosis can form a multicystic tumor-like mass (BMJ Case Rep 2014;2014:bcr2013201645)
Gross images
Images hosted on other servers:

Multiple lesions
Microscopic (histologic) description
- Glands lined by ciliated tubal type epithelium
- 3 types of cells:
- Ciliated columnar cells
- Nonciliated columnar secretory mucous cells
- So called intercalated or peg cells
- May have psammoma bodies
- Absence of endometrial stroma
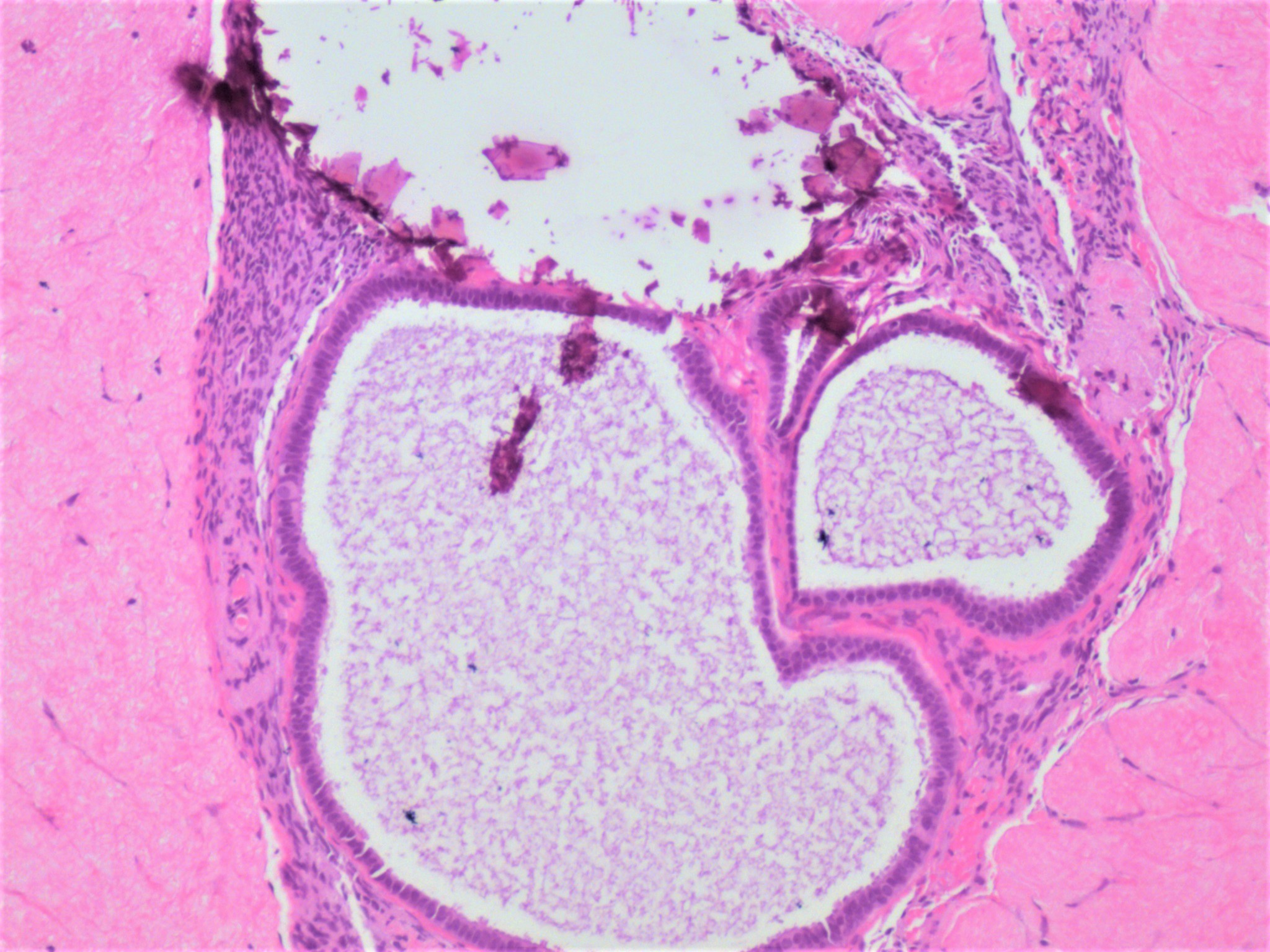
- Glands can be cystically dilated; they are usually found in the superficial ovarian cortex, either scattered or in loose clusters
- Reference: Clement: Atlas of Gynecologic Surgical Pathology, 4th edition, 2019
Microscopic (histologic) images
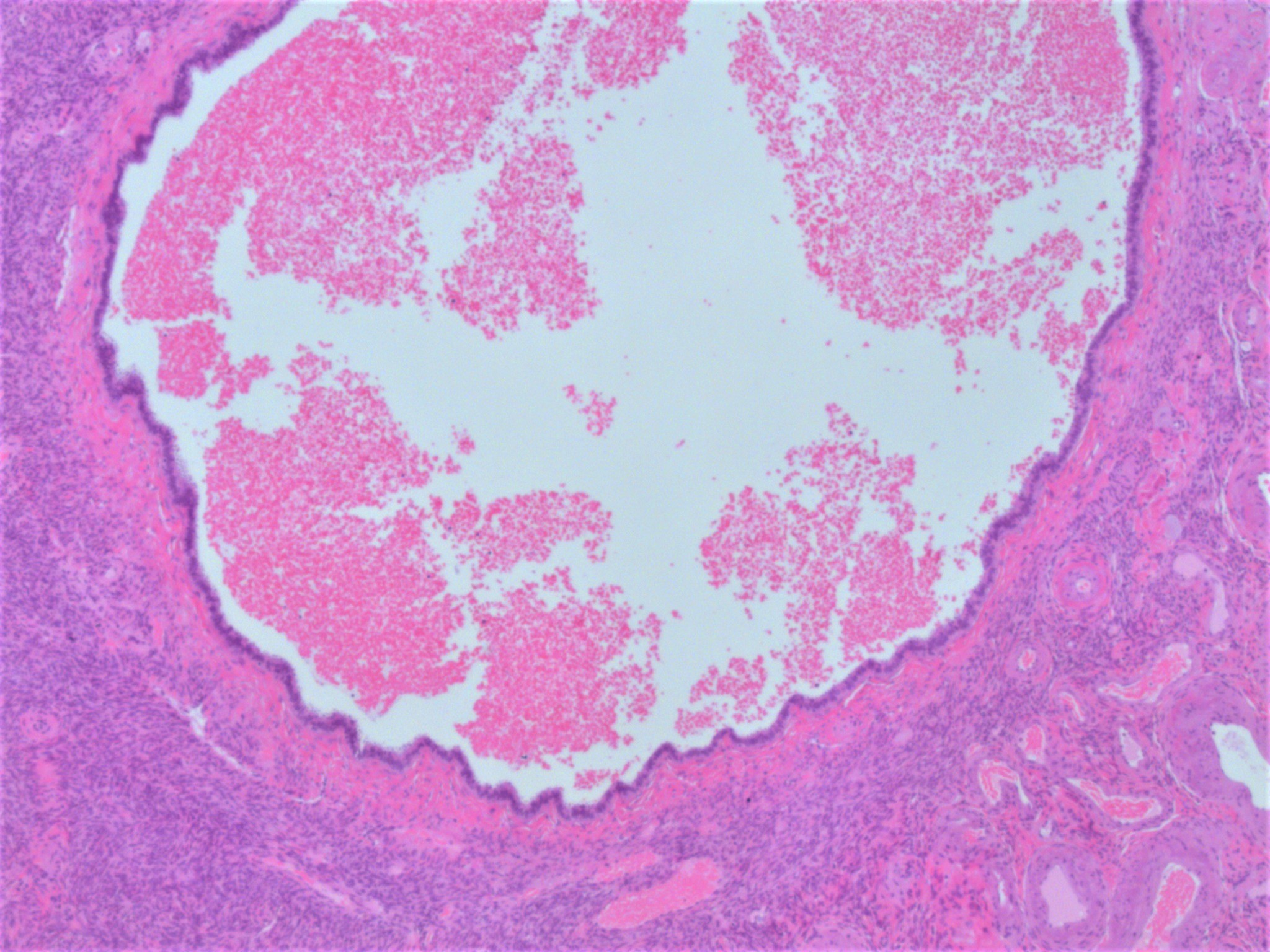
Contributed by Aurelia Busca, M.D., Ph.D.
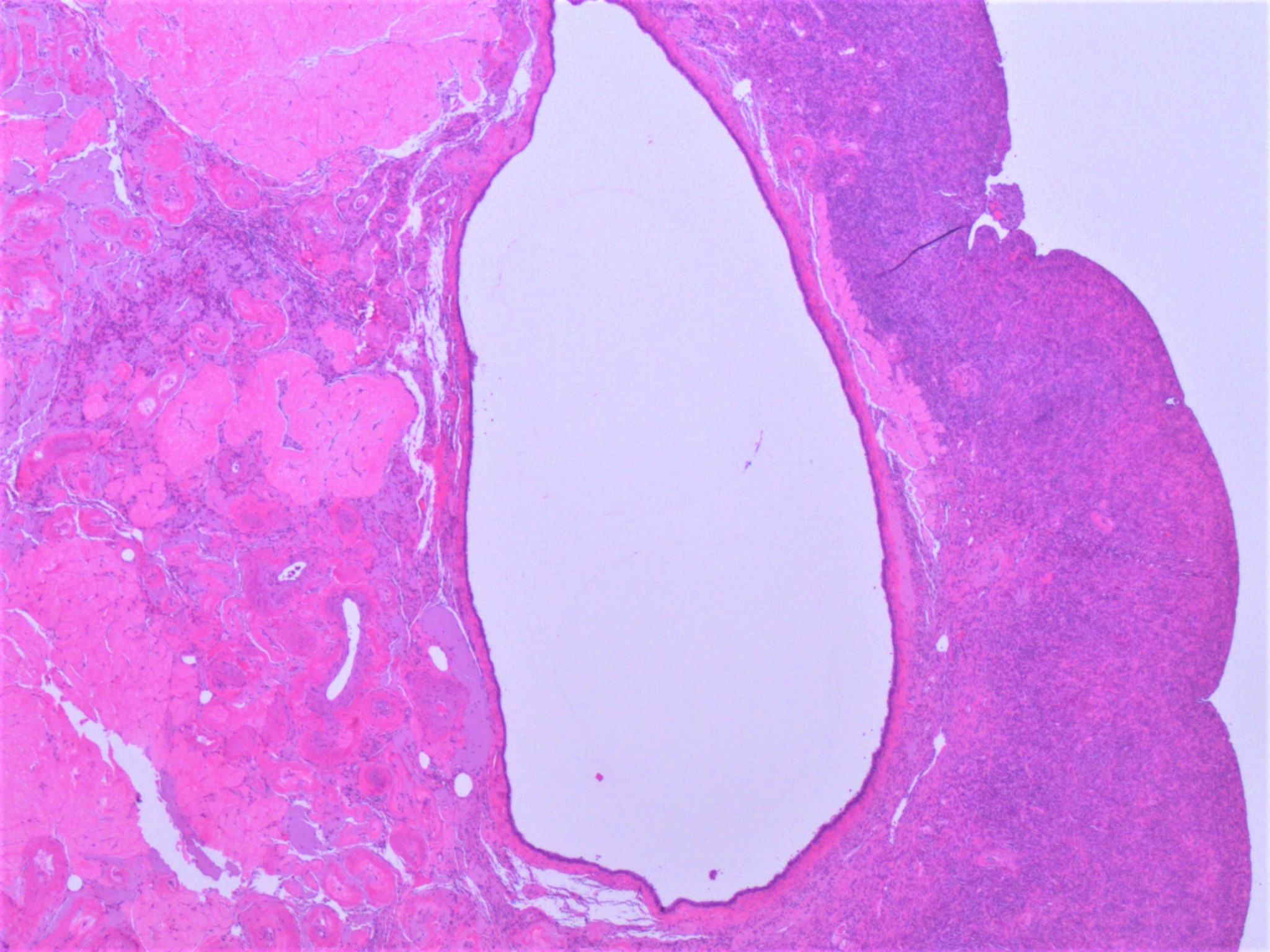
Cystically dilated glands
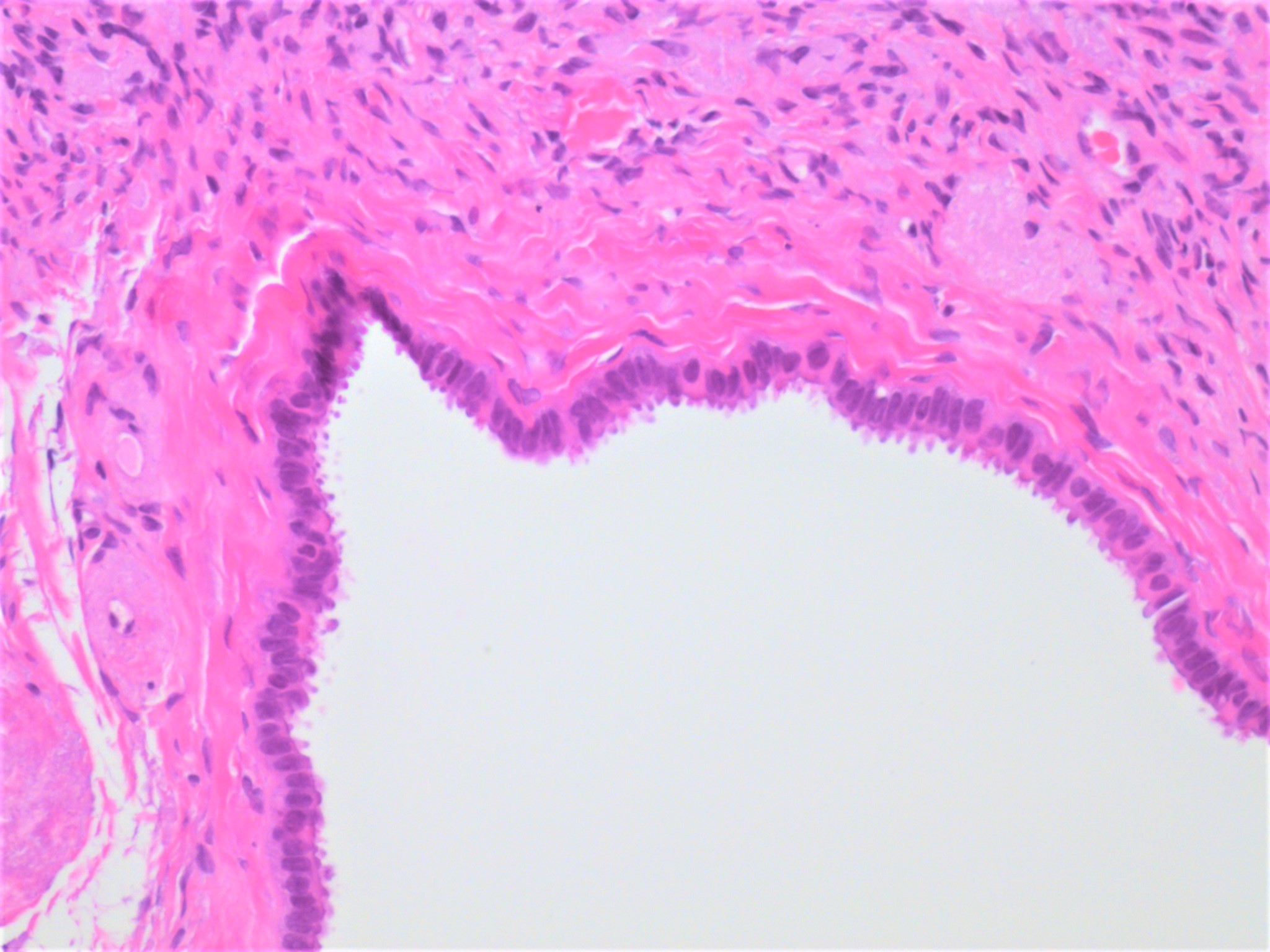
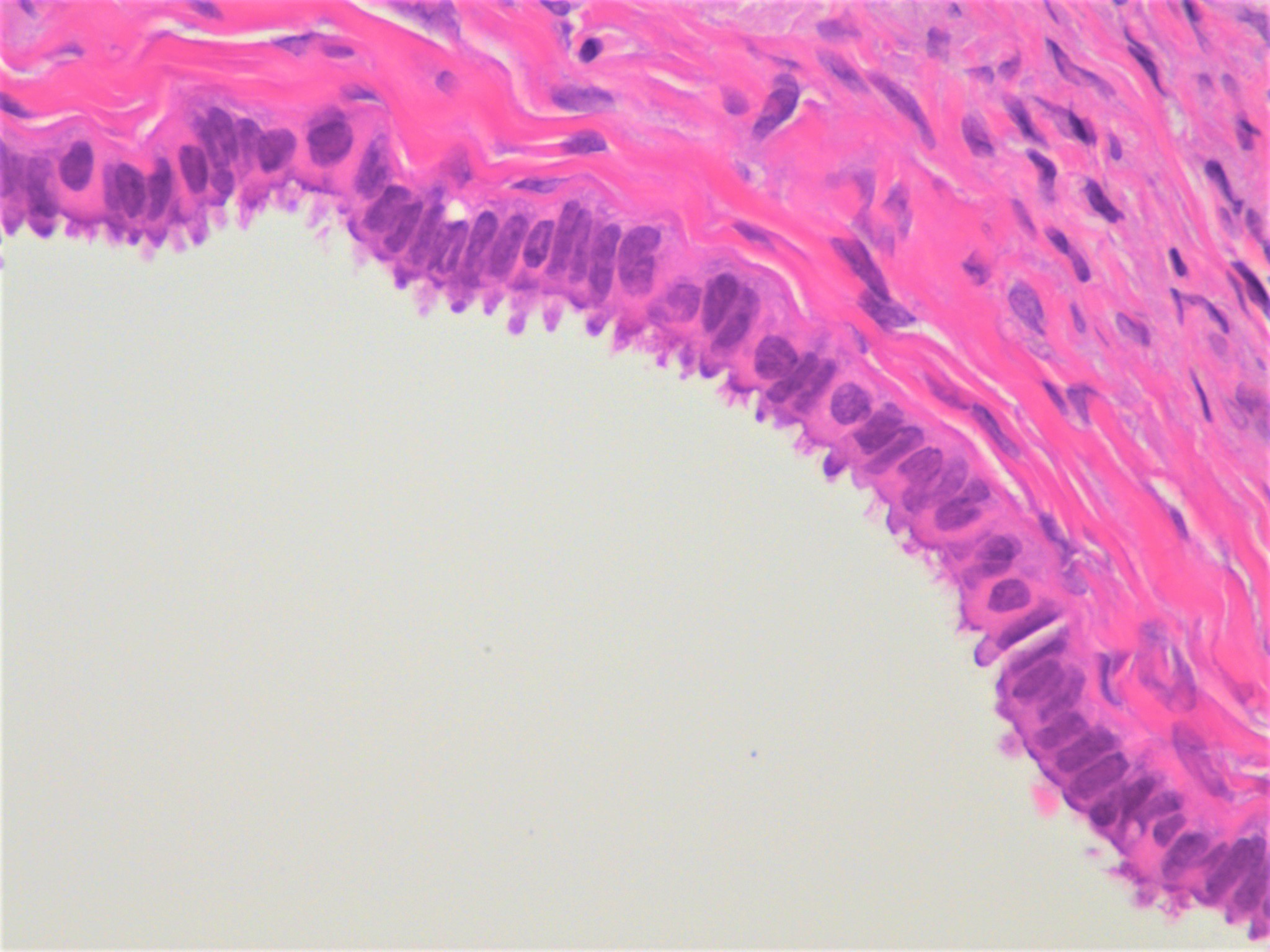
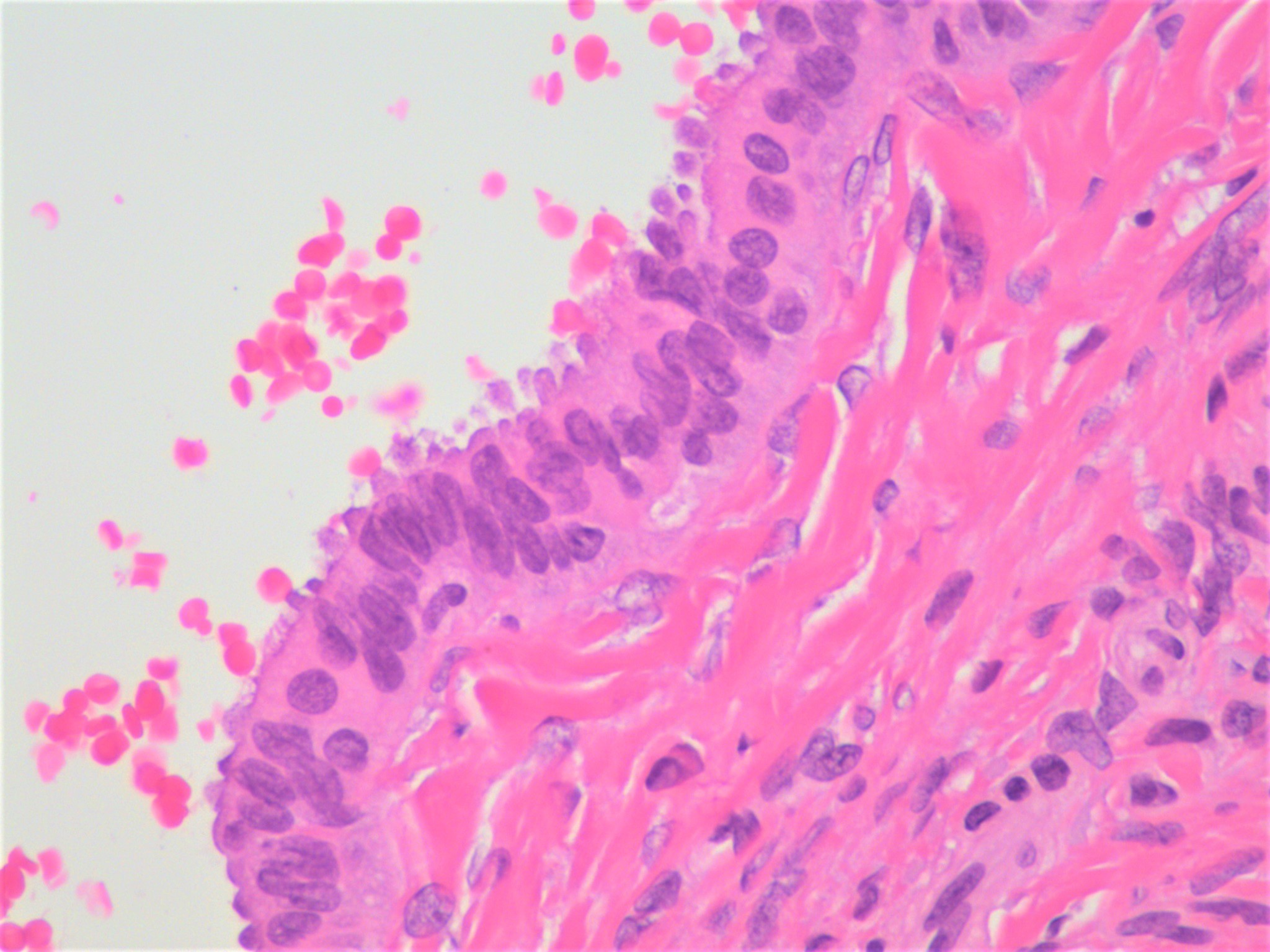
Cystically dilated glands with tubal differentiation
Cystically dilated glands with stromal microcalcifications
Positive stains
- PAX2, PAX8 (Am J Surg Pathol 2011;35:1837, Case Rep Obstet Gynecol 2016;2016:8621570)
- WT1, ER, PR (Am J Surg Pathol 2014;38:1612, Abdom Imaging 2015;40:471)
- Endosalpingiosis has a similar biomarker profile to normal fallopian tube and serous neoplasms (phospho-SMAD2, BCL2 and FOXJ1), which is distinct from ovarian surface epithelium (Gynecol Oncol 2014;132:316)
Negative stains
Sample pathology report
- Right and left ovaries, bilateral oophorectomies:
- Benign ovaries with focal endosalpingiosis
- Note: many pathologists do not report the finding of endosalpingiosis since it is common and benign
Differential diagnosis
- Cystic ovarian neoplasms when mass forming:
- Other types of epithelial cysts (mucinous, peritoneal inclusion type, transitional type) have distinct epithelia
- Serous cystadenoma:
- Lined by tubal type epithelium
- Distinction relies (arbitrarily) on size > 1 cm for cystadenomas
- Endometriosis:
- Has endometrial stroma and hemosiderin laden macrophages
Additional references
Board review style question #1
Which of the following is true about the finding illustrated in the photo of the ovary shown above?
- It represents an indication for resection
- Tubal differentiation distinguishes it from endometriosis
- Typically PAX8 negative
- Usually an incidental finding
Board review style answer #1
D. Usually an incidental finding. Endosalpingiosis is typically benign incidental finding in resection specimens, Müllerian derived (PAX8 positive). Absence of endometrial stroma distinguishes it from endometriosis, as tubal differentiation can be seen in both entities.
Comment Here
Reference: Endosalpingiosis
Comment Here
Reference: Endosalpingiosis
Board review style question #2
What feature below is most important to distinguish endosalpingiosis from endometriosis?
- Location
- Presence of endometrial stroma
- Presence of tubal epithelium
- Reactivity for PAX8
Board review style answer #2
B. Presence of endometrial stroma. Endometrial stroma is seen in endometriosis but not endosalpingiosis. Endometriosis can have tubal differentiation. It tends to have a similar anatomic distribution as endosalpingiosis and to express markers of Müllerian derivation, such as PAX8.
Comment Here
Reference: Endosalpingiosis
Comment Here
Reference: Endosalpingiosis
