

Ovary
Germ cell tumors
Monodermal teratomas
Monodermal cystic teratoma
Editorial Board Members: Lucy Ma, M.D., David B. Chapel, M.D.


Last author update: 22 May 2024
Last staff update: 23 May 2024
Copyright: 2023-2024, PathologyOutlines.com, Inc.
PubMed Search: Monodermal cystic teratoma


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Mashayekhi A, Turashvili G. Monodermal cystic teratoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarymonodermalcysticteratoma.html. Accessed December 19th, 2024.
Definition / general
- Benign cystic tumor comprising mature tissues derived from a single germ layer (ectoderm or endoderm), except for struma ovarii, carcinoid and neuroectodermal type tumors (malignant tumors of central neuroectodermal derivation)
Essential features
- Cystic tumor lined by benign keratinizing squamous epithelium or neuroectodermal tissues
- May contain pituitary type adenomas
- Benign with excellent prognosis
Epidemiology
- Monodermal teratomas are rare (Pediatr Dev Pathol 2015;18:341)
- Neuroectodermal cysts have been reported in children and young women
- Epidermoid cysts occur across a wide age range
Sites
- Ovary
Pathophysiology
- Unknown
Etiology
- Unknown
Clinical features
- Abdominal distension or pain
- Amenorrhea due to lactotroph adenoma (Obstet Gynecol 1990;75:540)
- Central obesity and hirsutism due to corticotroph adenoma (Am J Surg Pathol 1987;11:218)
Diagnosis
- Histologic examination
Laboratory
- Elevated prolactin in lactotroph adenoma (JAMA 1990;263:2472)
- Increased cortisol and lack of suppression of either low dose or high dose dexamethasone suppression test in corticotroph adenoma (Am J Surg Pathol 1987;11:218)
Radiology description
- Wide spectrum of radiologic presentation ranging from a purely cystic to a complex cystic mass with a considerable solid component
Radiology images
Contributed by Azin Mashayekhi, M.D., M.B.A. and Gulisa Turashvili, M.D., Ph.D.
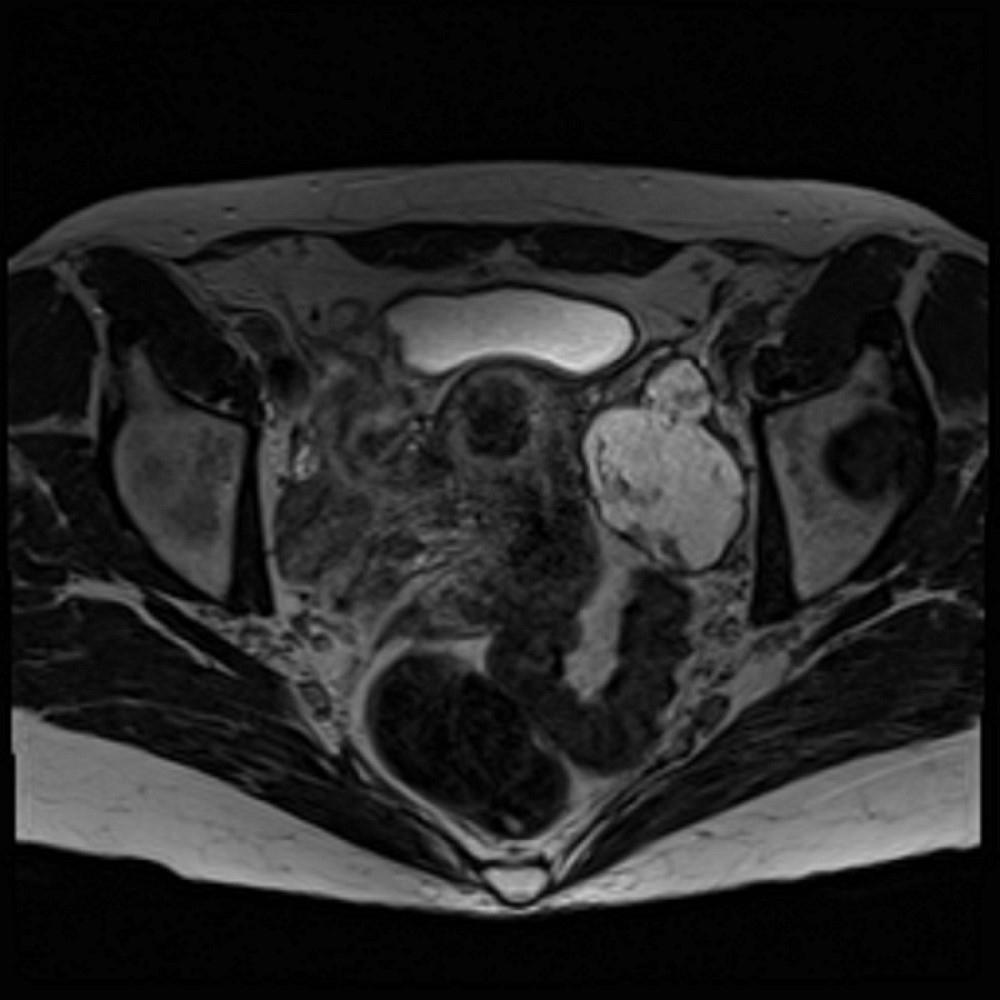
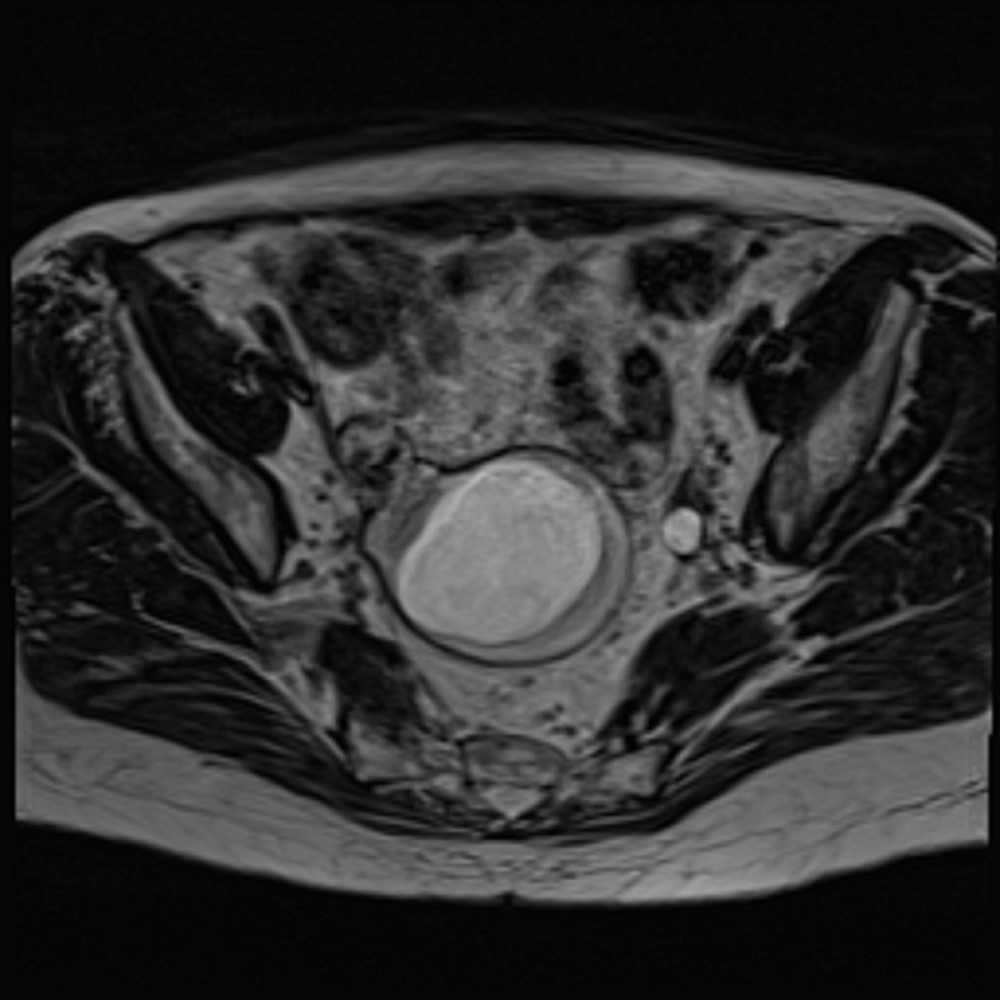
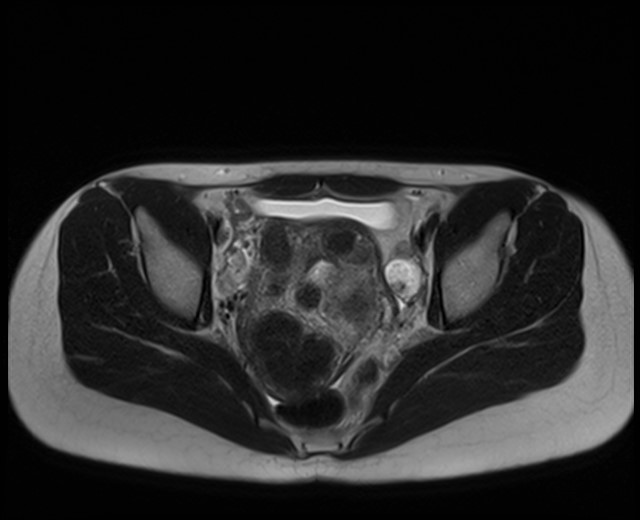
Magnetic resonance imaging (MRI) of pelvis
Prognostic factors
- Benign with excellent prognosis
Case reports
- 2.5 year old girl with ovarian epidermoid cyst torsion associated with appendicitis (Int J Surg Case Rep 2022;100:107731)
- 10 year old girl with neurogenic ovarian cyst (Pediatr Dev Pathol 2015;18:341)
- 36 year old woman with epidermoid cyst treated with laparoscopic cystectomy (Gynecol Minim Invasive Ther 2018;7:40)
- 50 year old woman with a giant (17 cm) epidermoid cyst (J Clin Diagn Res 2012;6:1584)
- 65 year old woman with epidermoid cyst associated with stromal hyperplasia (J Cancer Res Ther 2015;11:1046)
Treatment
- Ovarian cystectomy (Pediatr Dev Pathol 2015;18:341)
- Oophorectomy
Gross description
- Neuroectodermal cysts are thin walled, simple to multilocular cysts filled with clear yellow fluid, ranging from 8 - 15 cm (J Obstet Gynaecol Res 2001;27:21)
- Epidermoid cysts are simple thin walled cysts, with white-grey cheesy material, ranging from 1 - 15 cm (Int J Gynecol Pathol 2009;28:193)
Gross images
Contributed by Azin Mashayekhi, M.D., M.B.A. and Gulisa Turashvili, M.D., Ph.D.

Cystic lesion
Frozen section description
- Rarely performed but usually shows a cystic lesion lined by benign squamous epithelium or neuroectodermal tissues
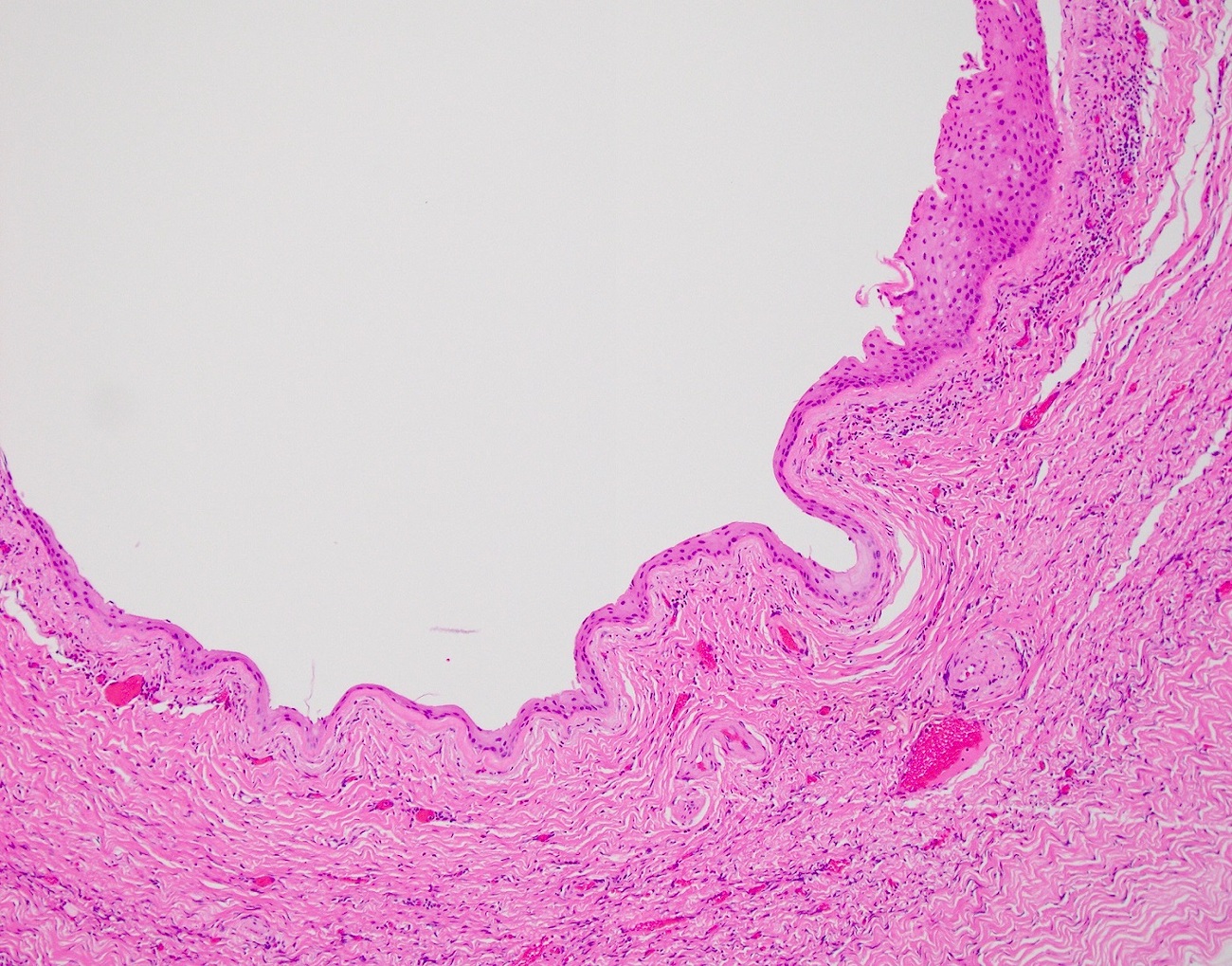
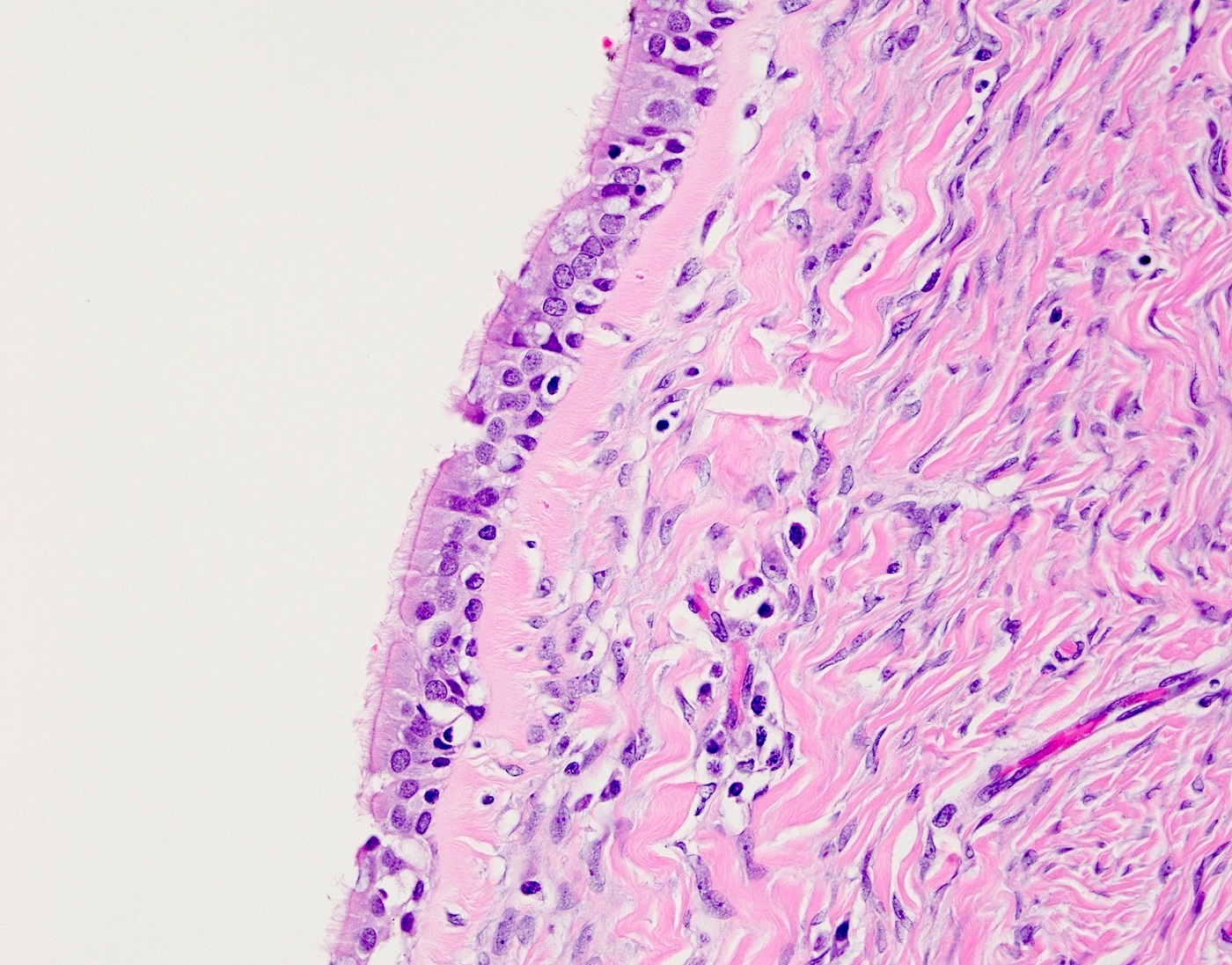
Microscopic (histologic) description
- Neuroectodermal cyst
- Lined by ependymal cells
- May show choroid plexus-like epithelium along the cyst lining
- Astrocytes, oligodendrocytes, microglia and ganglion cells may be present adjacent to the cyst lining (Histopathology 1994;24:477)
- Epidermoid cyst
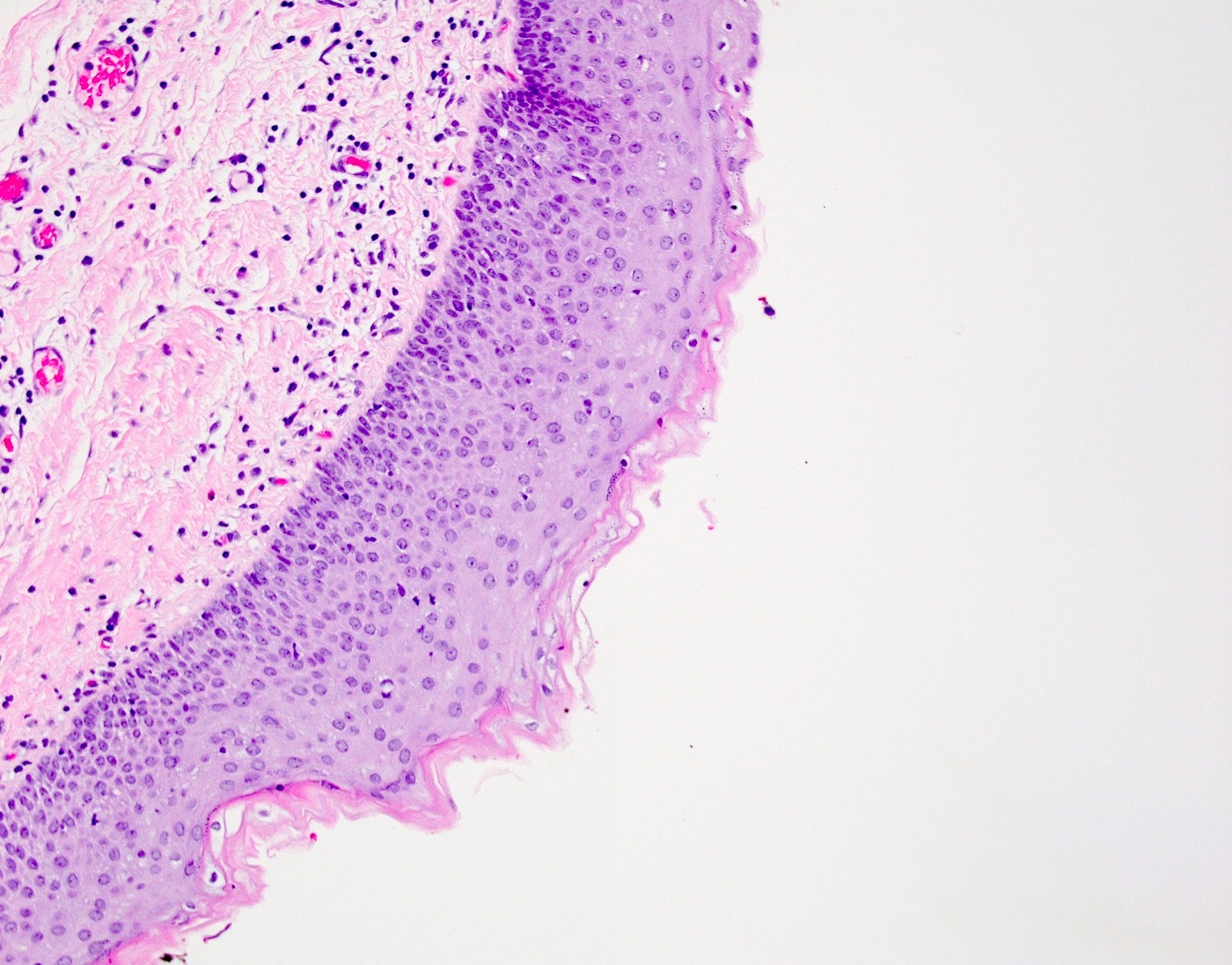
- Lined by mature, often keratinizing, stratified squamous epithelium
- Surrounded by a rim of collagenous stroma containing fibroblasts
- Keratinaceous debris fills the cyst lumen, with no evidence of hair or a Rokitansky tubercle (Int J Gynecol Pathol 1996;15:69)
- Rarely, cysts are lined by respiratory type epithelium (Cancer 1979;43:383)
- Lactotroph adenoma
- Closely packed nests of small cells with eosinophilic cytoplasm as seen in the anterior hypophysis (Obstet Gynecol 1990;75:540)
- Corticotroph adenoma
- Monomorphic cells with round nuclei and vacuolated or eosinophilic cytoplasm, growing in nests or cords (Am J Surg Pathol 1987;11:218)
Microscopic (histologic) images
Contributed by Azin Mashayekhi, M.D., M.B.A. and Gulisa Turashvili, M.D., Ph.D.
Cystic lesion
Cystic lesion
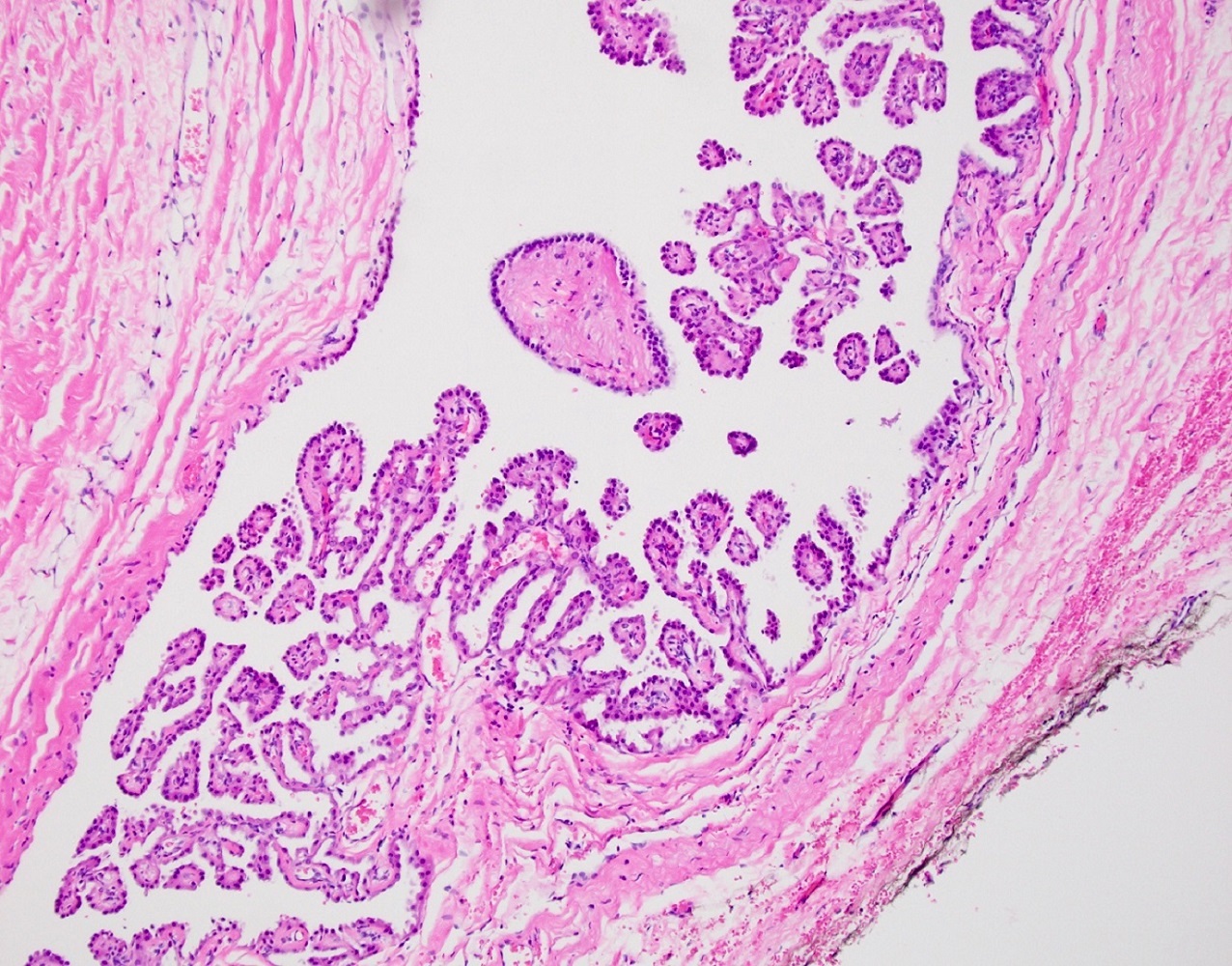
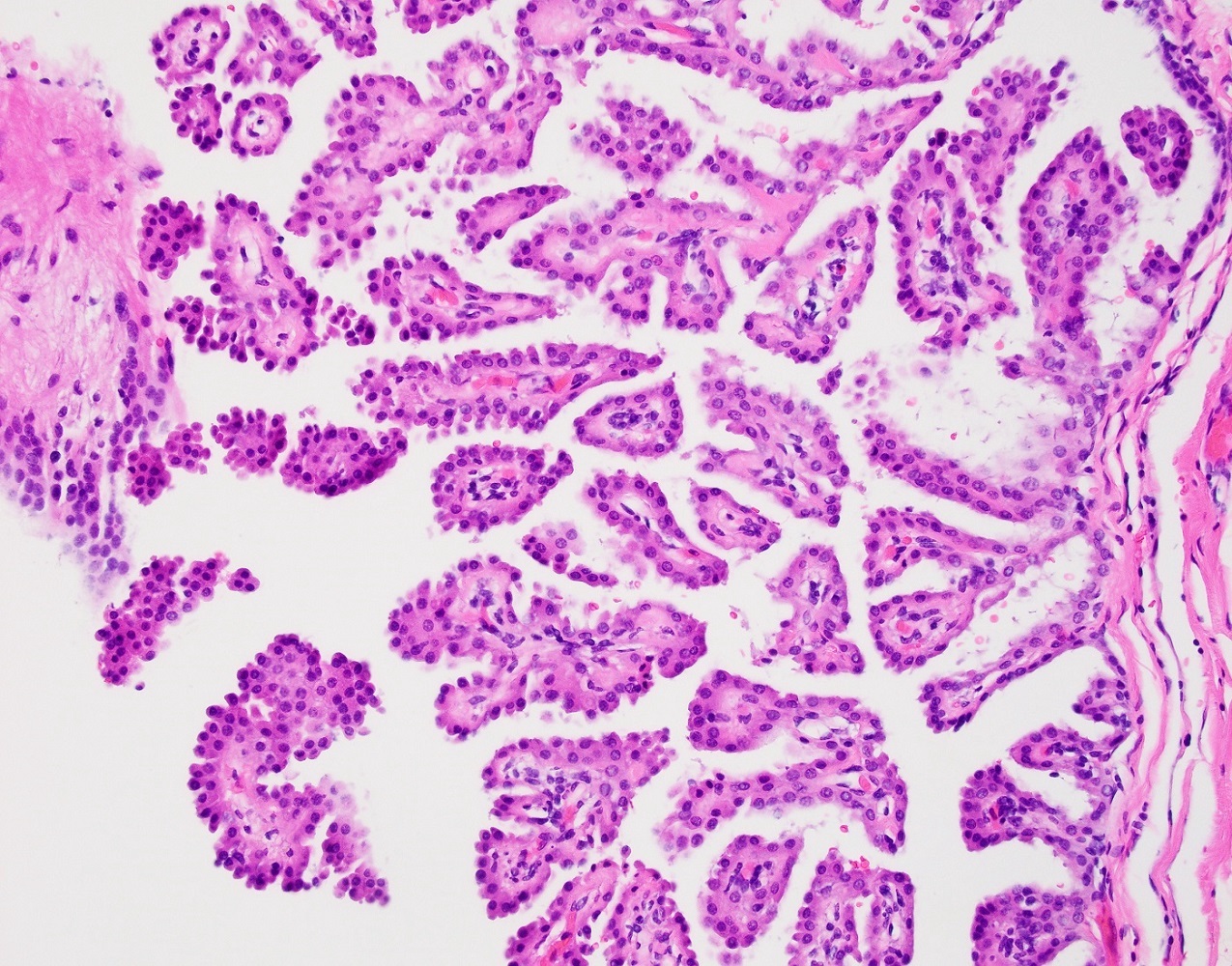
Intracystic proliferation
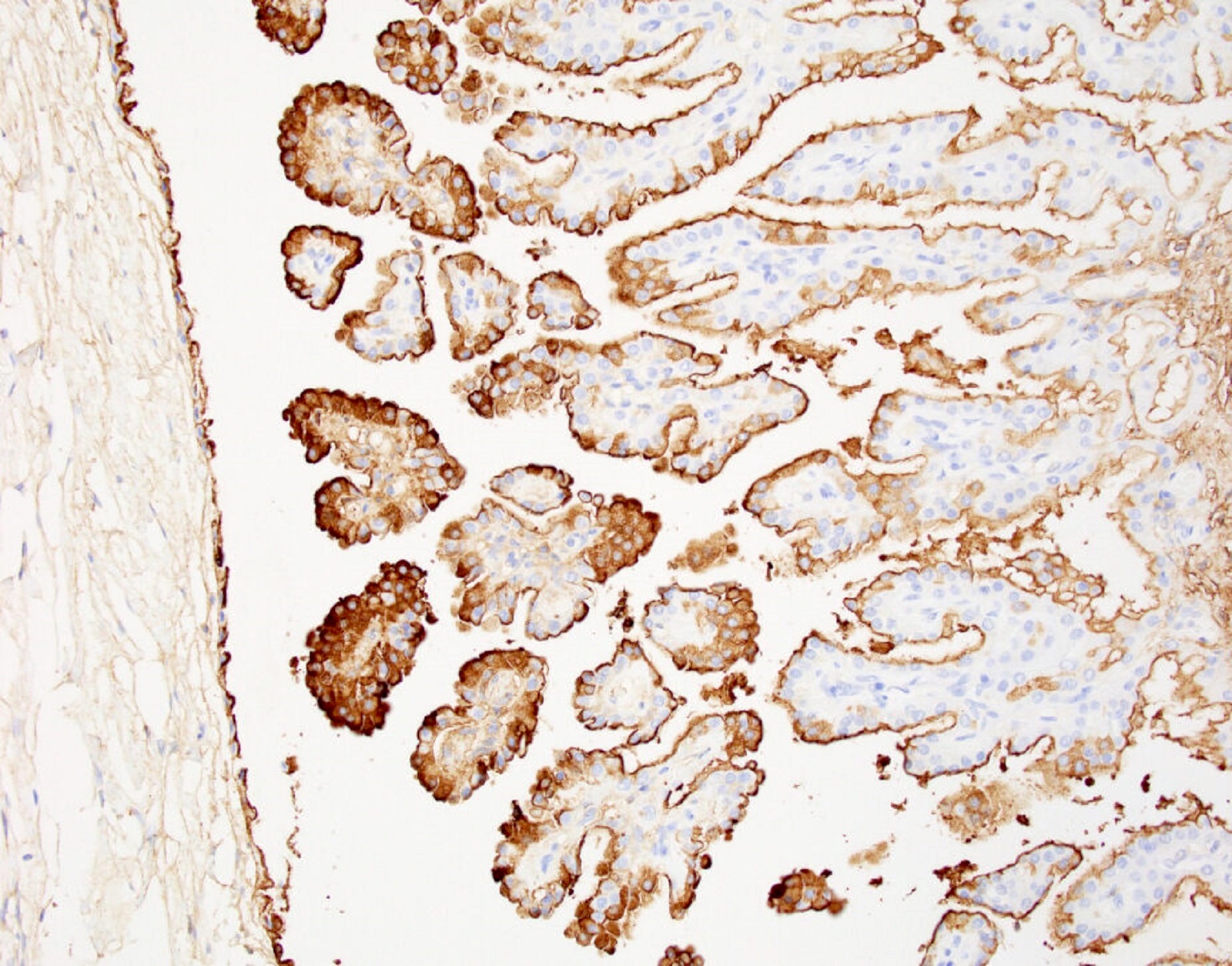
GFAP
Positive stains
- Immunohistochemistry has a limited role in diagnosis of monodermal cystic teratoma
- Prolactin in lactotroph adenoma (Obstet Gynecol 1990;75:540)
- ACTH in corticotroph adenoma (Am J Surg Pathol 1987;11:218)
- GFAP in neuroectodermal cyst (Histopathology 1994;24:477)
Sample pathology report
- Ovary, right, cystectomy:
- Epidermoid cyst (monodermal cystic teratoma)
Differential diagnosis
- Mature teratoma:
- Mature tissue representing at least 2 germ layers (BMC Cancer 2019;19:217)
- Malignant transformation occurs rarely (most commonly squamous cell carcinoma)
- Immature teratoma:
- Malignant germ cell tumor (Obstet Gynecol 2006;107:1075)
- Contains variable amounts of immature tissue (typically immature neuroepithelium comprising primitive appearing cells with scant cytoplasm, hyperchromatic nuclei and frequent mitoses)
- Steroid cell tumor:
- Pituitary type adenomas may be mistaken for steroid cell tumors with eosinophilic (lipid poor) cells
- Association with ependymal lined neuroectodermal cyst as well as prolactin expression in lactotroph adenoma and ACTH expression in corticotroph adenoma along with negative sex cord stromal markers (inhibin, calretinin, SF1) are helpful clues
Additional references
Board review style question #1
The image above is a representative section of an ovarian cyst from a 40 year old woman. What is the most likely diagnosis?
- Epidermoid cyst
- Immature cystic teratoma
- Monodermal cystic teratoma with respiratory epithelium
- Struma ovarii
Board review style answer #1
A. Epidermoid cyst. This ovarian cyst is lined by benign keratinizing squamous epithelium, consistent with epidermoid cyst. Answer D is incorrect because struma ovarii is exclusively composed of benign thyroid tissue.
Answer C is incorrect because some monodermal cystic teratomas are lined by respiratory epithelium.
Answer B is incorrect because immature cystic teratoma exhibits immature neuroepithelium in addition to endodermal, mesodermal and ectodermal elements.
Comment Here
Reference: Monodermal cystic teratoma
Comment Here
Reference: Monodermal cystic teratoma

