

Nasal cavity, paranasal sinuses, nasopharynx
Other nonneoplastic lesions
Respiratory epithelial adenomatoid hamartoma
Author: Bin Xu, M.D., Ph.D.
Editorial Board Member: Molly Housley Smith, D.M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 29 June 2023
Last staff update: 29 June 2023
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Respiratory epithelial adenomatoid hamartoma nasal

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Xu B. Respiratory epithelial adenomatoid hamartoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalrespepithadenohamart.html. Accessed November 28th, 2024.
Definition / general
- Acquired overgrowth of surface glands characterized by pseudostratified epithelium with cilia surrounded by a thickened basement membrane
- Currently classified as nonneoplastic hamartoma in the WHO classification 5th edition (Head Neck Pathol 2022;16:1)
- Chondro-osseous respiratory epithelial (CORE) hamartoma is considered a subtype of respiratory epithelial adenomatoid hamartoma (REAH) (Head Neck Pathol 2022;16:1)
Essential features
- Overgrowth of medium sized glands displacing normal elements (such as seromucinous glands)
- Lining of glands is pseudostratified respiratory epithelium with cilia
- Glands are surrounded by thickened basement membrane
Terminology
- Glandular hamartoma (not recommended)
- Subtype: chondro-osseous and respiratory epithelial hamartoma
ICD coding
- ICD-10: Q85.9 - phakomatosis, unspecified
Epidemiology
- M:F = 3:1 to 7:1 (Ann Otol Rhinol Laryngol 1995;104:639, Am J Rhinol Allergy 2013;27:322)
- Median age: 58 years (range: 27 - 81 years) (Ann Otol Rhinol Laryngol 1995;104:639, Am J Rhinol Allergy 2013;27:322)
Sites
- Most commonly occurs in the posterior septum of nasal cavity, particularly the olfactory cleft (Ann Otol Rhinol Laryngol 1995;104:639, Am J Rhinol Allergy 2013;27:322)
- Other sites of involvement include lateral wall of nasal cavity, middle meatus, nasal turbinate, nasopharynx, paranasal sinuses (ethmoid, maxillary or frontal) (Laryngoscope Investig Otolaryngol 2022;7:1292, Ann Otol Rhinol Laryngol 1995;104:639, Am J Rhinol Allergy 2013;27:322)
Etiology
- > 66% are associated with atopic disease or chronic rhinosinusitis (Am J Rhinol Allergy 2020;34:610, Am J Rhinol Allergy 2013;27:322)
Clinical features
- Patients commonly present with nonspecific symptoms (e.g., nasal congestion / obstruction, headache, rhinorrhea and epistaxis)
- Often has a longstanding history of chronic rhinosinusitis (Ann Otol Rhinol Laryngol 1995;104:639)
- May be unilateral or bilateral (Ann Otol Rhinol Laryngol 1995;104:639, AJNR Am J Neuroradiol 2013;34:1086)
Diagnosis
- Identifying diagnostic histologic features in an endoscopic resection specimen is necessary for the diagnosis
Radiology description
- Expansion of the maximum olfactory cleft width (especially when > 10 mm) is a common finding on computed tomography (CT) (Am J Rhinol Allergy 2013;27:322, AJNR Am J Neuroradiol 2013;34:1086)
- No evidence of destructive growth or bone invasion
Radiology images
Images hosted on other servers:

Widened olfactory cleft
Prognostic factors
- Benign lesion: negligible risk of recurrence if resected completely (Am J Rhinol Allergy 2013;27:322)
- Local recurrence is rare
Case reports
- 17 year old boy with respiratory epithelial adenomatoid hamartoma (Ear Nose Throat J 2022 May 9 [Epub ahead of print])
- 62 year old man with respiratory epithelial adenomatoid hamartoma of the maxillary sinus (Acta Otorhinolaryngol Ital 2006;26:225)
- 75 year old man with bilateral nasal mass (Proc (Bayl Univ Med Cent) 2017;30:221)
- 83 year old woman with chondro-osseous respiratory epithelial adenomatoid hamartoma (Case Rep Otolaryngol 2019;2019:5247091)
Treatment
- Complete excision, often through the endoscopic approach, is considered curative
Gross description
- Polypoid or exophytic, rubbery, tan-brown, with a firm to gritty consistency
Gross images
Images hosted on other servers:

Polypoid glistening mass
Microscopic (histologic) description
- Respiratory epithelial adenomatoid hamartoma (REAH)
- Proliferation (often polypoid) of medium sized glands lined by ciliated epithelium
- Glands are surrounded by thick eosinophilic basement membranes
- Lesion replaces background normal elements, often resulting in a decreased number of seromucinous glands
- Features of chronic rhinosinusitis (chronic inflammation) and inflammatory sinonasal polyp (edematous stroma admixed with chronic inflammation) may be seen in the background
- Chondro-osseous respiratory epithelial (CORE) hamartoma subtype (Int Arch Otorhinolaryngol 2013;17:218, Int J Surg Pathol 2022;30:448)
- CORE hamartoma is composed of 2 components, often intimately intermixed with each other
- Glandular component composed of glands lined by respiratory type epithelium with cilia; the extent of glandular component is often less prominent compared with REAH
- Mesenchymal component that ranges from immature mesenchyme, cartilage, bone trabeculae or chondromyxoid matrix
- CORE hamartoma is composed of 2 components, often intimately intermixed with each other
Microscopic (histologic) images
Contributed by Bin Xu, M.D., Ph.D.
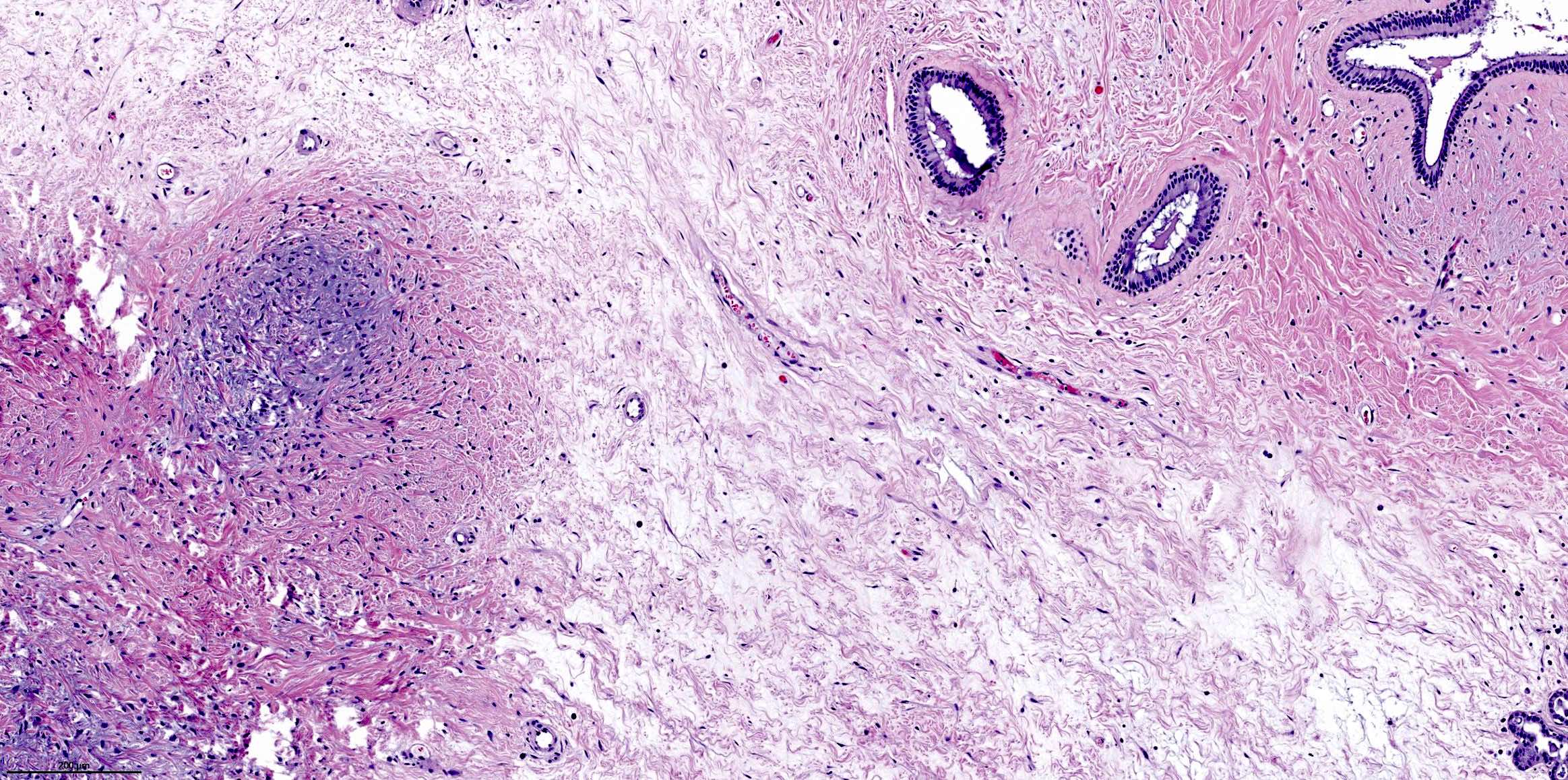
Respiratory epithelial adenomatoid hamartoma (REAH)
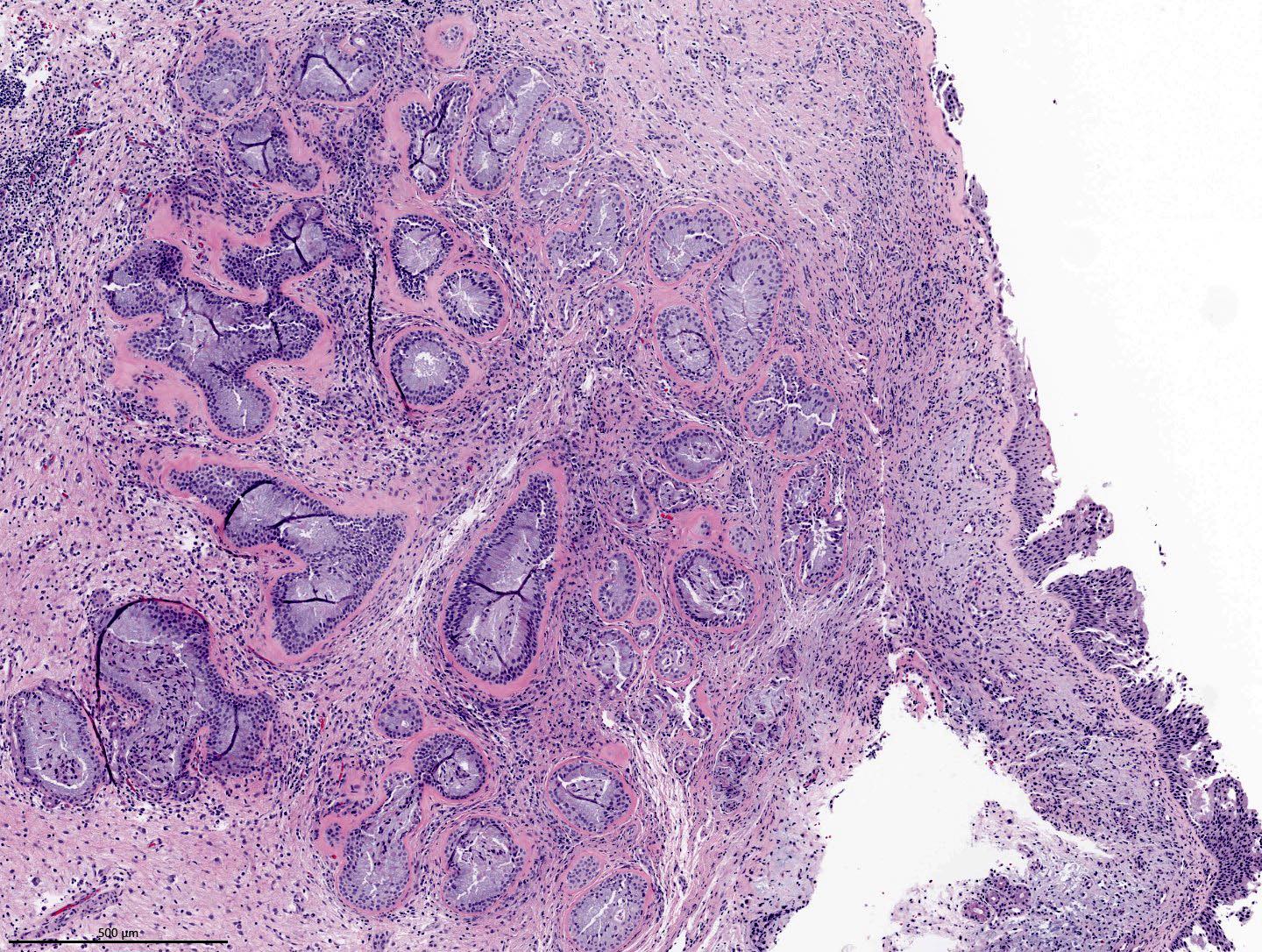
Proliferation of medium sized glands
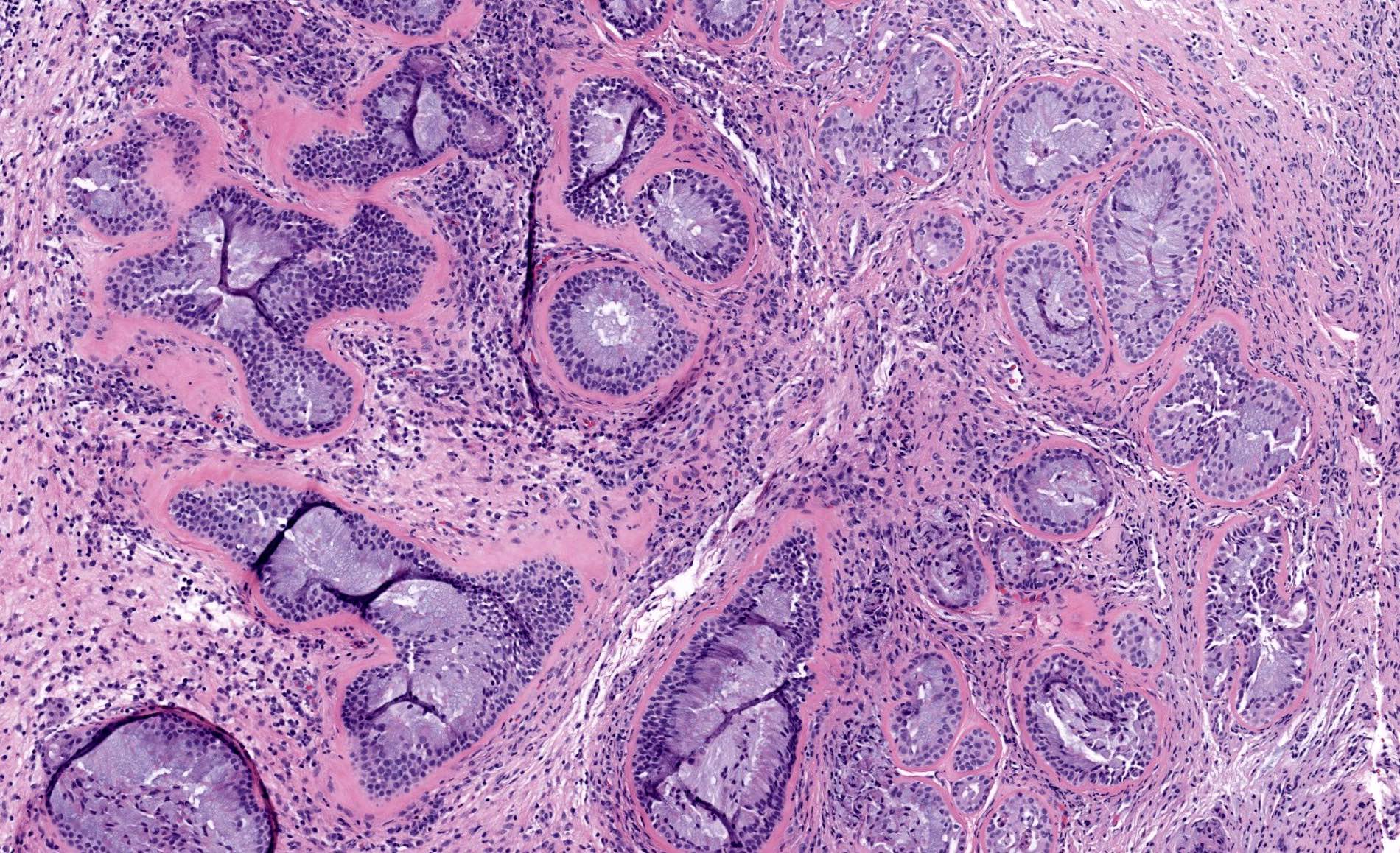
Thickened basement membrane
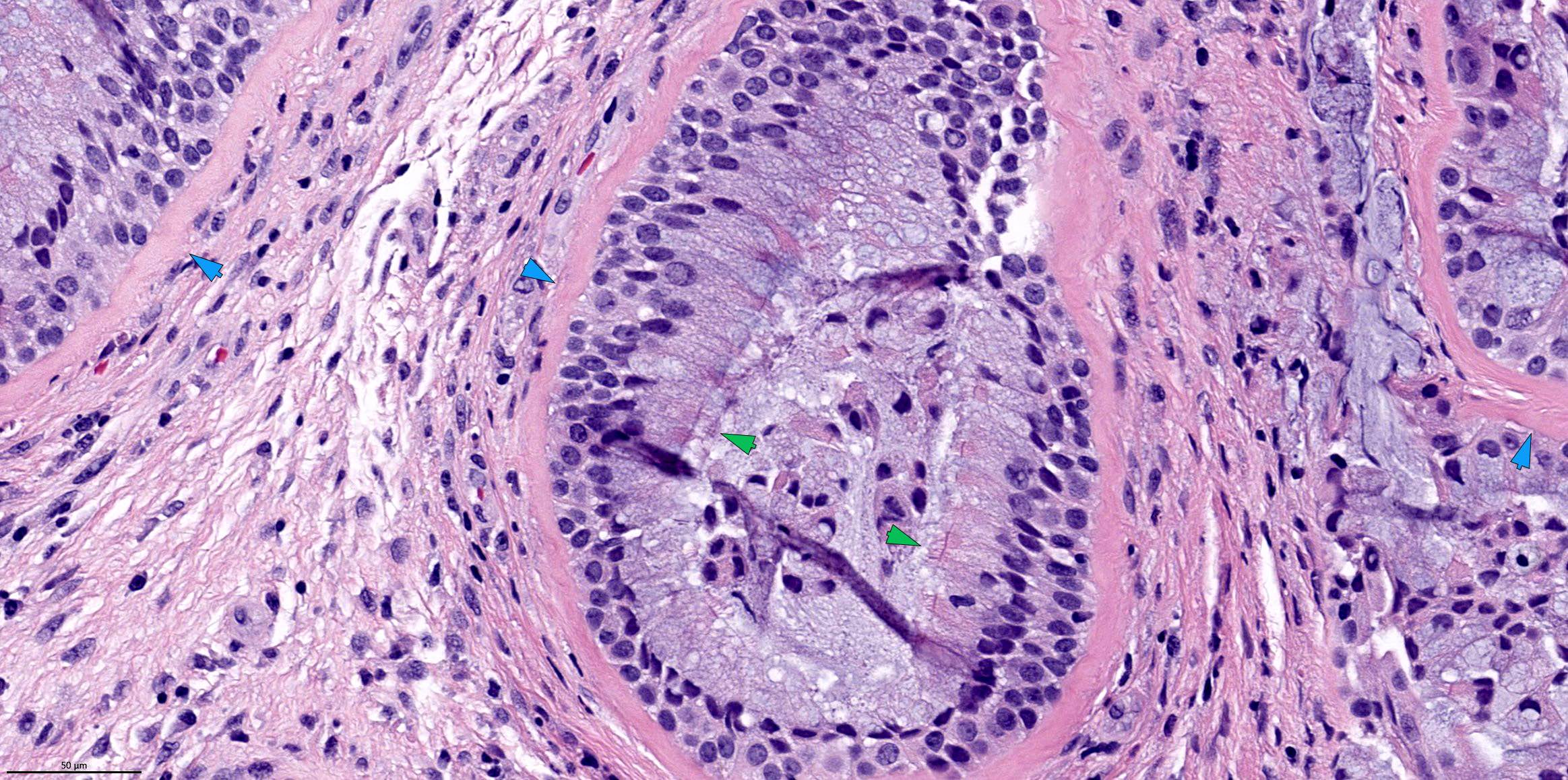
Glands with cilia
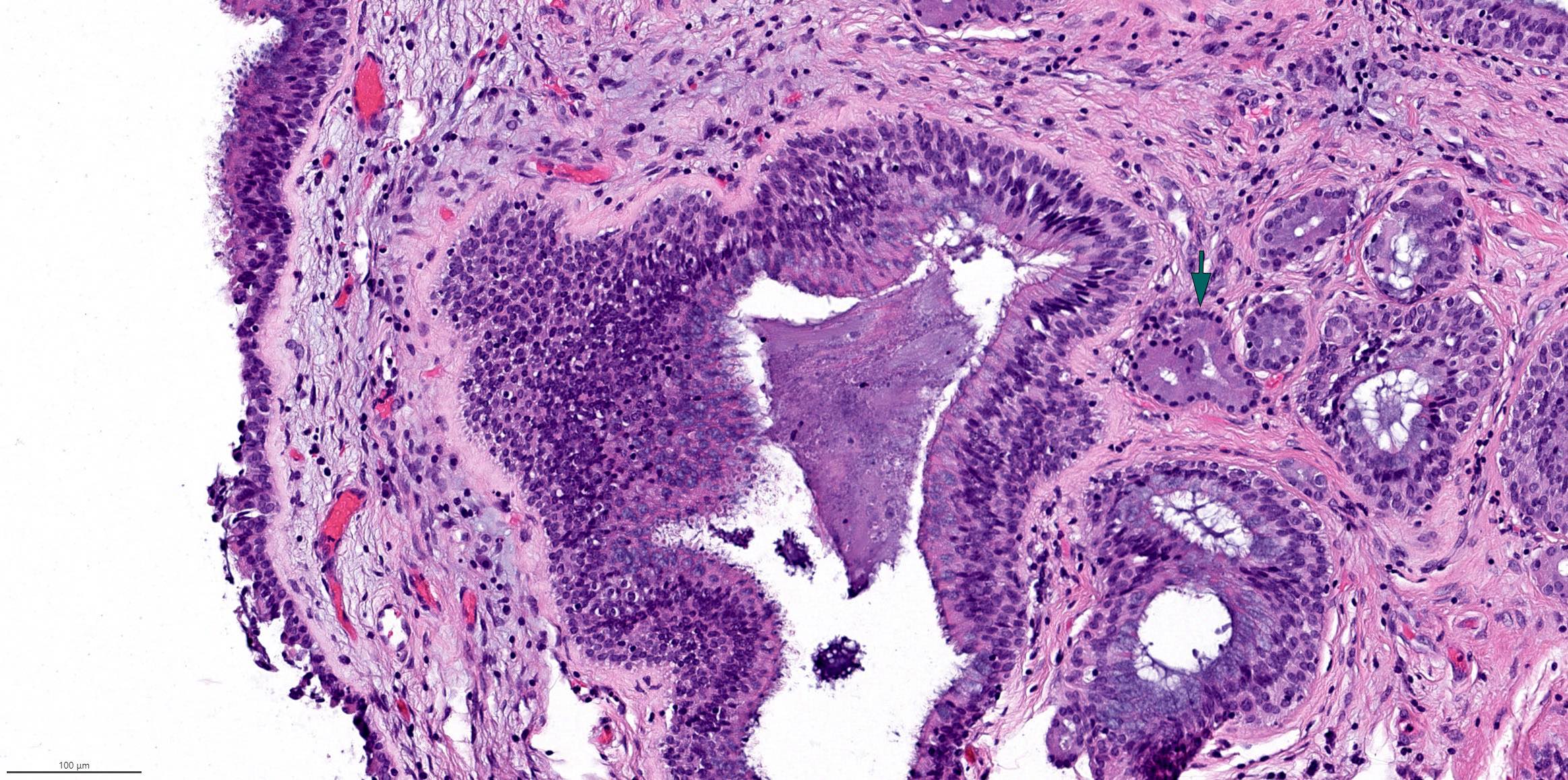
Scattered seromucinous glands
Chondro-osseous respiratory epithelial (CORE) hamartoma
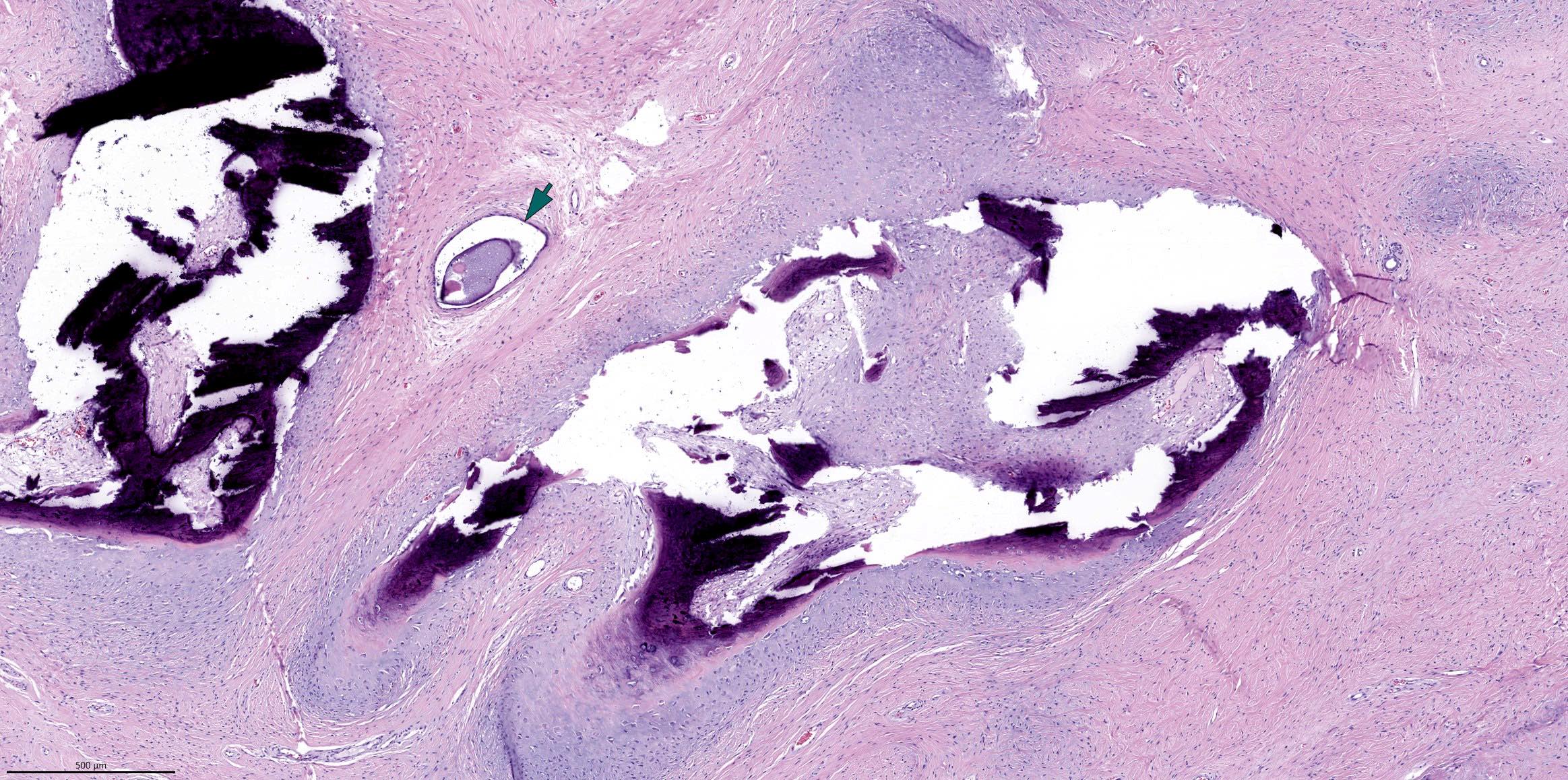
Glands and chondromyxoid stroma
Myxoid mesenchyme and gland

Epithelium with cilia
Positive stains
- Diagnosis is typically rendered based on H&E alone; immunohistochemistry is not required for this entity
- CK7 (Head Neck Pathol 2008;2:203)
Negative stains
Molecular / cytogenetics description
- Currently considered as a nonneoplastic hamartoma in the WHO classification 5th edition; however, increased fractional allelic loss is detected, suggesting a possible neoplastic nature (Am J Surg Pathol 2006;30:1576)
Sample pathology report
- Left nasal cavity, excision:
- Respiratory epithelial adenomatoid hamartoma
Differential diagnosis
- Inflammatory sinonasal polyp:
- May have occasional invagination of surface epithelium but lacks proliferation of glandular component and the thickened surrounding basement membrane
- Sinonasal papilloma, inverted type:
Respiratory epithelial adenomatoid hamartoma Sinonasal papilloma, inverted type Location Commonly on the posterior septum close to the olfactory cleft Typically on the lateral nasal wall High risk HPV Negative May be positive Thickened basement membrane Present Absent Epithelial lining Respiratory type epithelium of normal thickness with cilia Hyperplastic (thickened) squamous, transitional or respiratory type epithelium Transmigrating neutrophils / neutrophilic microabscesses Absent Present
- Sinonasal adenocarcinoma, nonintestinal type:
- Complex architecture manifested as densely packed back to back tubular glands or fused / cribriform glandular architecture
- Lacks cilia and thickened basement membrane
- May show other malignant features (e.g., nuclear pleomorphism, prominent mitotic activity, necrosis, perineural invasion and lymphovascular invasion)
- May harbor diagnostic mutations or fusions involving NTRK3, MET, NRG1, PRKACA, AKT1, BRAF and CTNNB1 genes (Mod Pathol 2022;35:1160)
- Biphenotypic sinonasal sarcoma:
Board review style question #1
An excision of a nasal polyp from 50 year old man shows the histology pictured above. What is the diagnosis?
- Inflammatory sinonasal polyp
- Respiratory epithelial adenomatoid hamartoma (REAH)
- Sinonasal adenocarcinoma, nonintestinal subtype
- Sinonasal papilloma, inverted subtype
Board review style answer #1
B. Respiratory epithelial adenomatoid hamartoma (REAH). The H&E shows typical histologic findings of respiratory epithelial adenomatoid hamartoma, characterized by proliferation of medium sized glands with cilia surrounded by thickened basement membrane. See Differential diagnosis section for features to distinguish REAH from its diagnostic mimickers, such as inverted papilloma, inflammatory polyp and nonintestinal sinonasal adenocarcinoma.
Comment Here
Reference: Respiratory epithelial adenomatoid hamartoma
Comment Here
Reference: Respiratory epithelial adenomatoid hamartoma
Board review style question #2
Which of the following statements about respiratory epithelial adenomatoid hamartoma (REAH) is true?
- 30% of REAH is associated with high risk human papillomavirus
- Classified as a benign neoplasm in the WHO classification
- Commonly located on the nasal septum rather than lateral nasal wall
- Has ~15% risk of recurrence and a small risk of distant metastasis
Board review style answer #2
C. Commonly located on the nasal septum rather than lateral nasal wall. Answer A is incorrect because REAH is not associated with high risk human papillomavirus. Answer B is incorrect because REAH is classified as a nonneoplastic lesion in WHO classification. Answer D is incorrect because REAH has a very low (if any) risk of recurrence if completely excised and no distant metastasis has been reported.
Comment Here
Reference: Respiratory epithelial adenomatoid hamartoma
Comment Here
Reference: Respiratory epithelial adenomatoid hamartoma

