

Nasal cavity, paranasal sinuses, nasopharynx
Sinonasal adenocarcinoma
Intestinal type
Editorial Board Member: Bin Xu, M.D., Ph.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 23 May 2023
Last staff update: 27 February 2024
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Intestinal type adenocarcinoma nasal

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ilchenko V, Mannan R. Intestinal type. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalintestinaladeno.html. Accessed December 27th, 2024.
Definition / general
- Sinonasal intestinal type adenocarcinoma (ITAC) is an epithelial tumor of the nasal cavity and the paranasal sinuses, often related to professional exposure to organic dust (such as wood or leather) and histologically resembling intestinal adenocarcinoma (Head Neck 2016;38:1564)
- ITACs can be present in 5 morphologic patterns: colonic, papillary, solid, mucinous and mixed (Head Neck Pathol 2017;11:295)
Essential features
- Incidence is correlated with organic dust exposure (Cancers (Basel) 2021;13:5245)
- ITAC is usually located in the olfactory mucosa of the ethmoid sinus (Cancers (Basel) 2021;13:5022)
- A characteristic feature of this tumor is an increased production of intracellular or extracellular mucin, similar to mucinous adenocarcinoma of the intestinal tract (Cancers (Basel) 2021;13:5022)
Terminology
- Colloid type adenocarcinoma, colonic type adenocarcinoma, enteric type adenocarcinoma (these terms are not recommended for use by WHO)
ICD coding
- ICD-O: 8144/3 - intestinal type adenocarcinoma
- ICD-11:
- 2C20.0 & XH0349 - adenocarcinoma of nasal cavity & adenocarcinoma, intestinal type
- 2C22.0 & XH0349 - adenocarcinoma of accessory sinuses & adenocarcinoma, intestinal type
Epidemiology
- Male predominance (M:F ratio can vary from 4:1 to 21:1 in different geographical regions) with a median age of 60 - 65 years (Cancers (Basel) 2021;13:5245, Head Neck 2016;38:1564)
- Strong correlation to professional exposure to organic dust, such as wood or leather (Head Neck 2016;38:1564)
- Incidence of ITAC varies between geographical regions, presumably due to differences in dust exposure (Cancers (Basel) 2021;13:5245)
- Reported average exposure period is ~40 years
- In contrast to squamous cell carcinoma of a similar region, alcohol, smoking and human papillomavirus do not seem to be risk factors for the development of ITAC (Head Neck 2016;38:1564)
Sites
- Most common location is the olfactory mucosa of the ethmoid sinus but can occur in the nasal cavity and maxillary antrum (Cancers (Basel) 2021;13:5022)
- Cases related to industrial wood dust exposure show predilection for ethmoid sinus
- Sporadic tumors are more common in maxillary antrum
Pathophysiology
- ITAC is considered to develop through intestinal metaplasia of the sinonasal epithelium (Patholog Res Int 2011;2011:230147)
- Wood dust does not seem to have direct mutagenic properties of its own but prolonged exposure to and irritation by wood dust particles can stimulate cellular turnover by inflammatory pathways
- Chronic inflammation is recognized as an important mechanism in tumor initiation and progression (Head Neck 2016;38:1564)
Etiology
- Exposure to organic dust (such as wood or leather) for several decades is the major risk factor (Head Neck 2016;38:1564)
Clinical features
- Unilateral nasal obstruction, rhinorrhea, epistaxis are common presentations (Arch Craniofac Surg 2018;19:210)
- Tumor tends to be very locally aggressive but rarely metastasizes (Arch Craniofac Surg 2018;19:210, Pathol Res Pract 2019;215:152432)
- Advanced tumors may cause pain, neurologic disturbances, exophthalmos, visual impairment
Diagnosis
- CT and MRI are used for diagnosing early lesions, defining disease extent and detecting early recurrences
- Ultrasound guided fine needle aspiration plays an important role in confirming the diagnosis before treatment because it is frequently misdiagnosed as a salivary gland tumor (Arch Craniofac Surg 2018;19:210)
Radiology description
- CT or MRI may reveal soft tissue mass in the ethmoid sinus, frontal sinus or other locations (Arch Craniofac Surg 2018;19:210)
Radiology images
Images hosted on other servers:

Frontoethmoidal sinus mass

Frontal sinus mass
Prognostic factors
- Locally aggressive with ~50% local recurrence
- Locoregional / distant metastasis occurs in 10 - 20% cases
- Mean disease free survival is 32 months (Cancers (Basel) 2021;13:5022)
- Papillary subtype is associated with better prognosis, while mucinous and solid subtypes carry poor prognosis (Cancers (Basel) 2021;13:5022)
- Prognosis and response to the chemotherapy can be associated with genotoxic agents, such as TP53 mutations
- Significantly higher complete response rate and disease free survival rate were reported in patients carrying tumors with wild type TP53 compared to patients bearing mutated TP53 (Head Neck 2016;38:1564)
- There is no significant prognostic difference between occupational and sporadic tumors
Case reports
- 36 year old man with ITAC that developed from inverted papilloma (J Clin Diagn Res 2016;10:ED12)
- 50 year old man with right nasal block, mass in right nose and frontal headache (J Clin Diagn Res 2014;8:149)
- 63 year old man with a rapidly growing soft mass on his glabellar region for 4 months (Arch Craniofac Surg 2018;19:210)
Treatment
- Standard treatment is surgical resection, with a minimally invasive endoscopic approach when possible (Cancers (Basel) 2021;13:5022)
- Due to the high recurrence rate of ITAC, postoperative radiation is commonly administered
- Neoadjuvant chemotherapy is used in advanced stage tumors (Cancers (Basel) 2021;13:5022)
- Because local recurrences and metastases of these tumors occur frequently, palliative treatment is most often the only option (Head Neck 2016;38:1564)
Clinical images
Images hosted on other servers:

Mass on glabellar region

Wide excision of mass

76 days after surgery

Endoscopic resection
Gross description
- Irregular exophytic tan-pink mass bulging into nasal cavity or paranasal sinuses, often with necrotic and friable appearance
- Some lesions are gelatinous
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
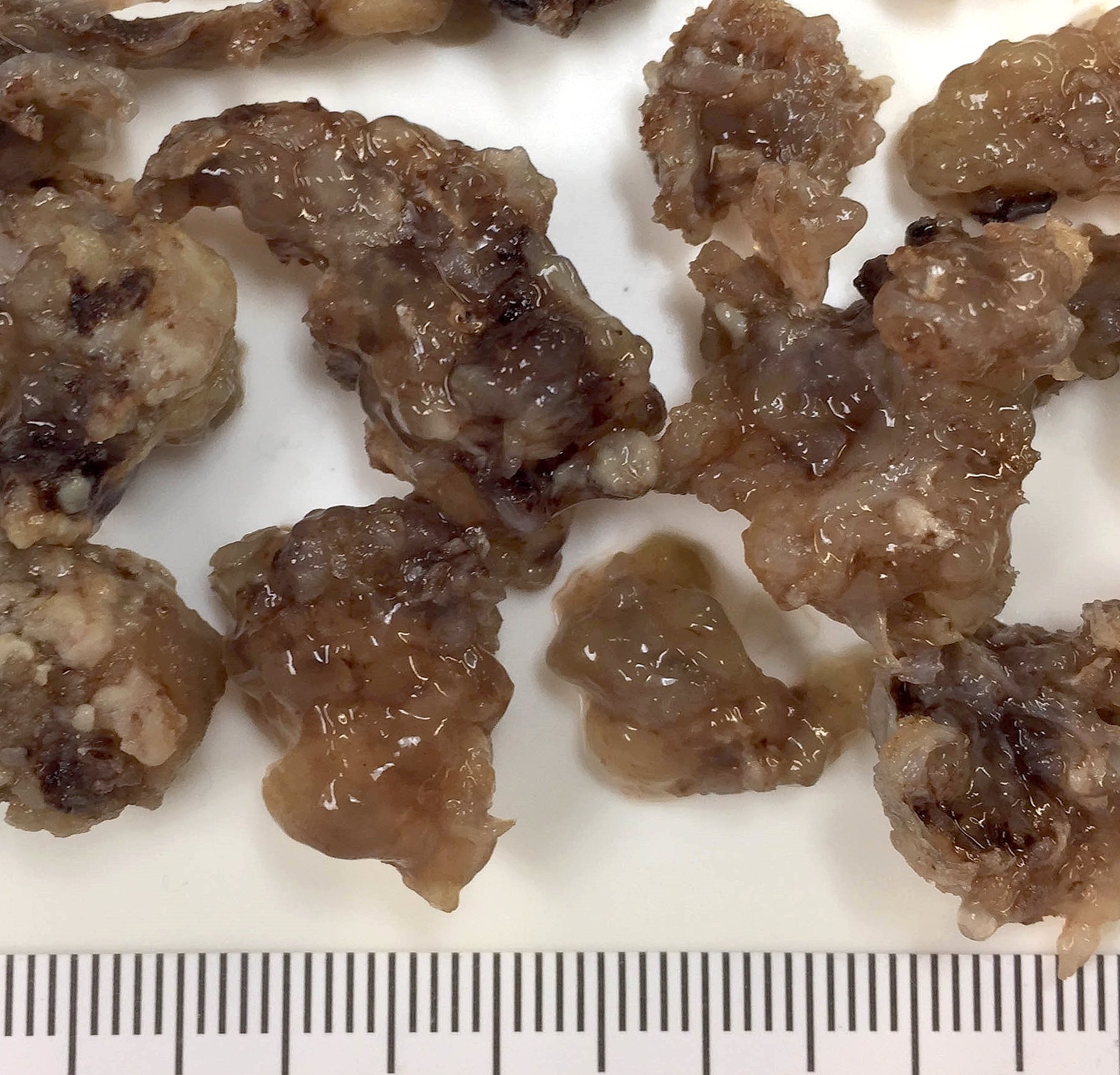
Macroscopic appearance
Images hosted on other servers:

Open biopsy masses
Microscopic (histologic) description
- ITACs can be present in 5 morphologic patterns: colonic, papillary, solid, mucinous and mixed (Head Neck Pathol 2017;11:295)
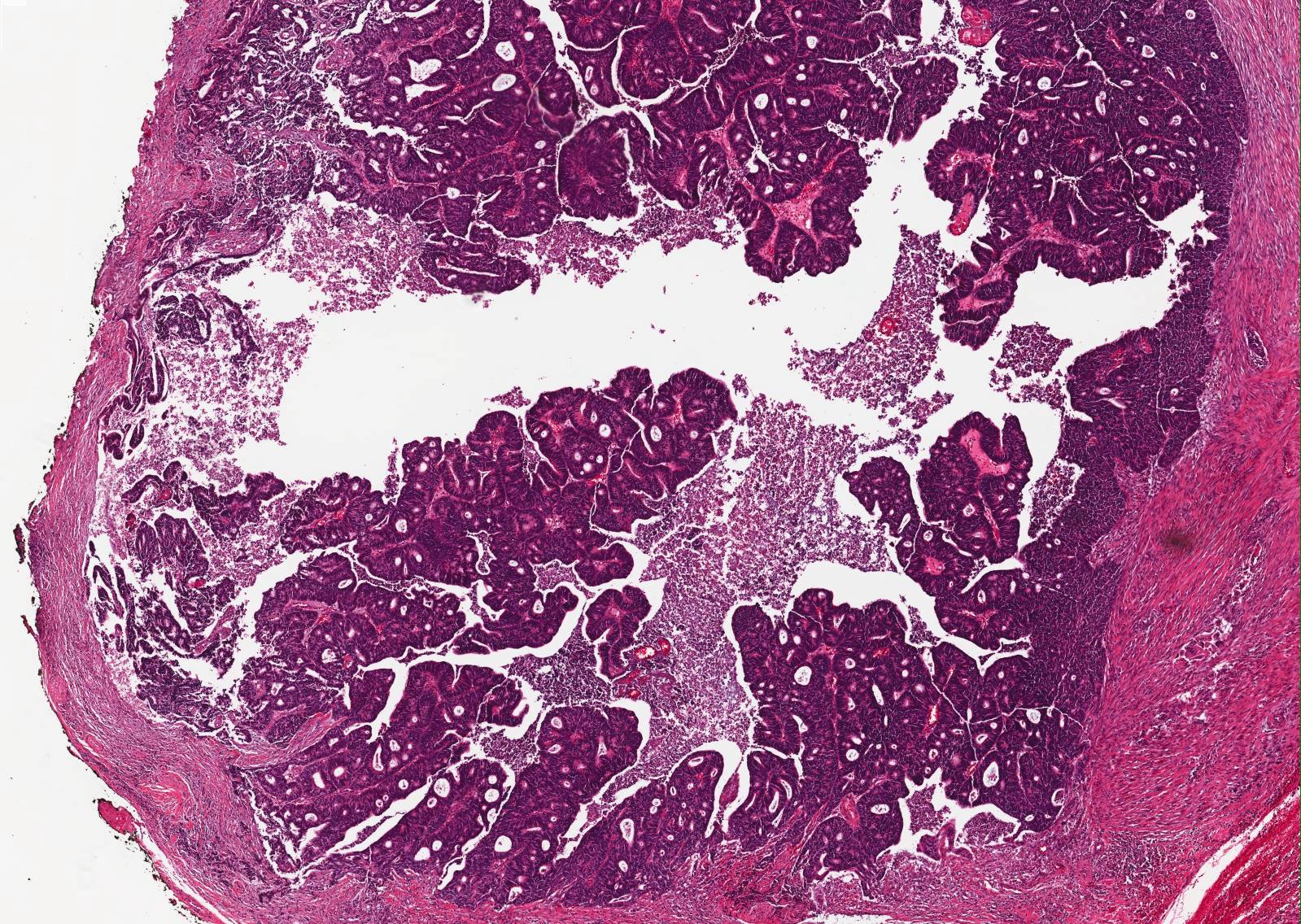
- Papillary pattern: predominantly papillary growth with tubular elements
- Colonic pattern: tubuloglandular architecture with minor papillary elements; neoplastic cells have palisaded hyperchromatic nuclei and a few goblet cells
- Solid pattern: poorly differentiated; trabecular and solid proliferation of neoplastic cells
- Mucinous pattern: mucin laden neoplastic glands or tumor cell clusters within pools of extracellular mucin
- Mixed pattern: variable admixture of 2 or more subtypes
- Goblet cells, Paneth cells and argentaffin cells may be found in all patterns
- Exceptionally well differentiated ITAC may resemble normal small intestinal mucosa with well formed villi and muscularis mucosae
Microscopic (histologic) images
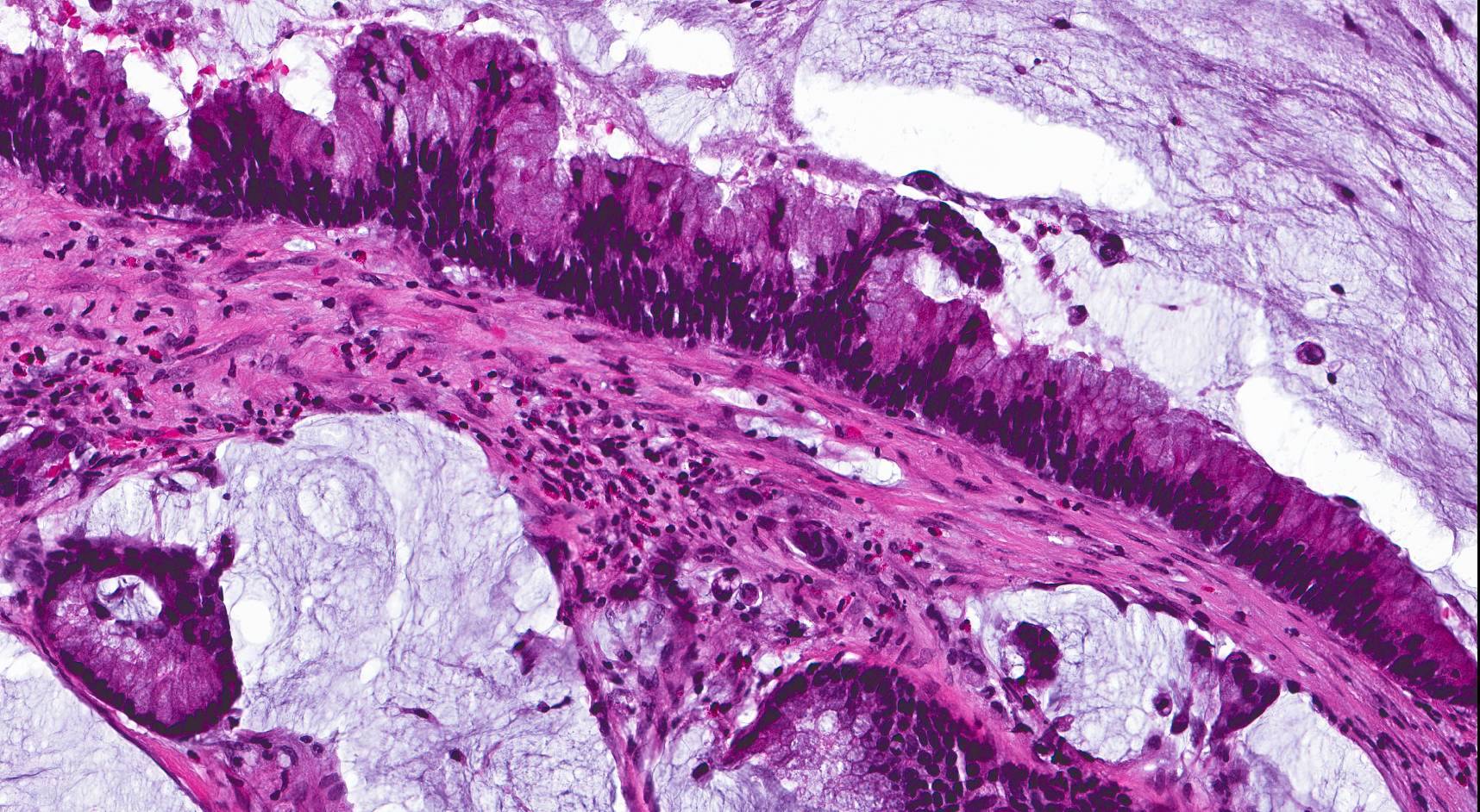
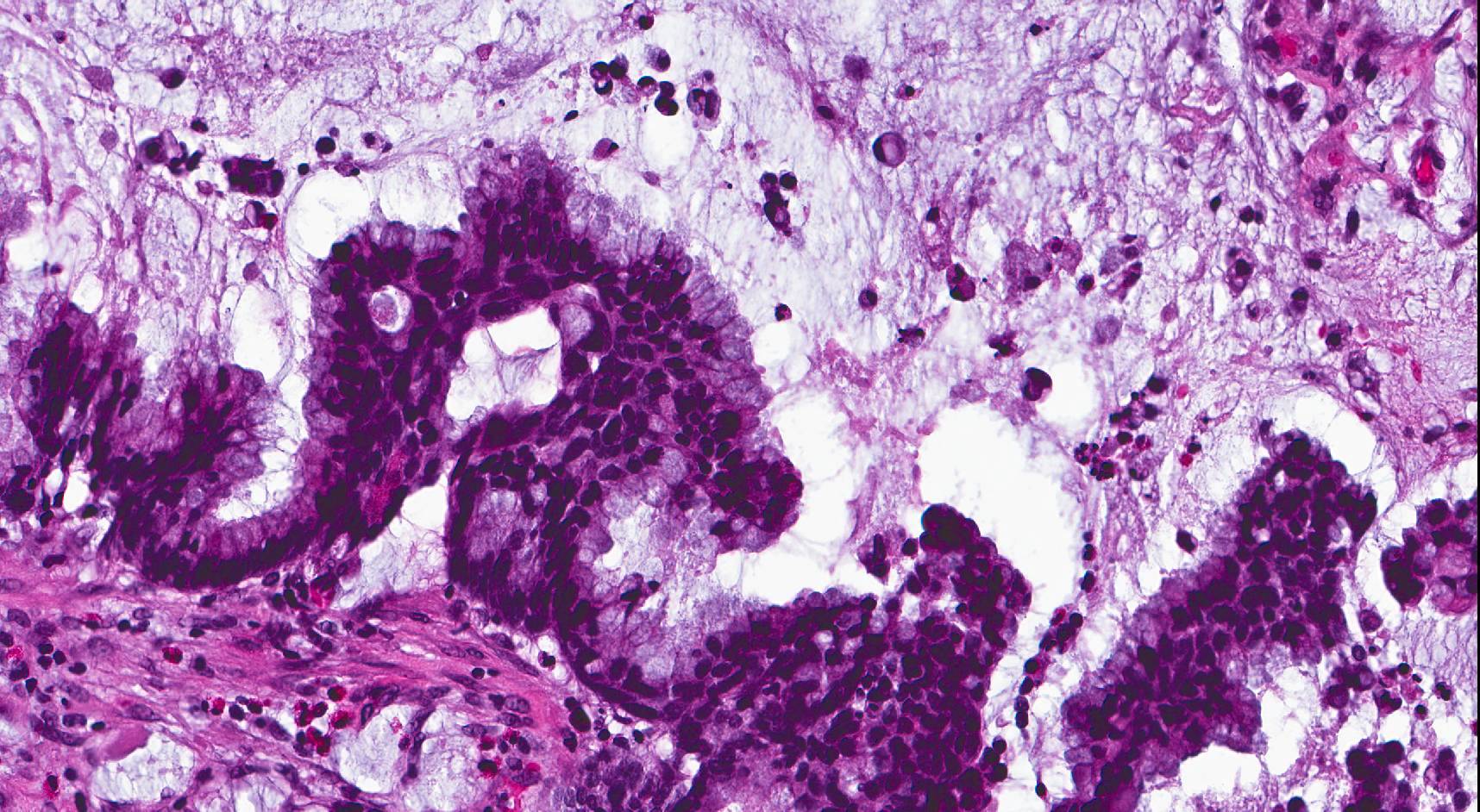
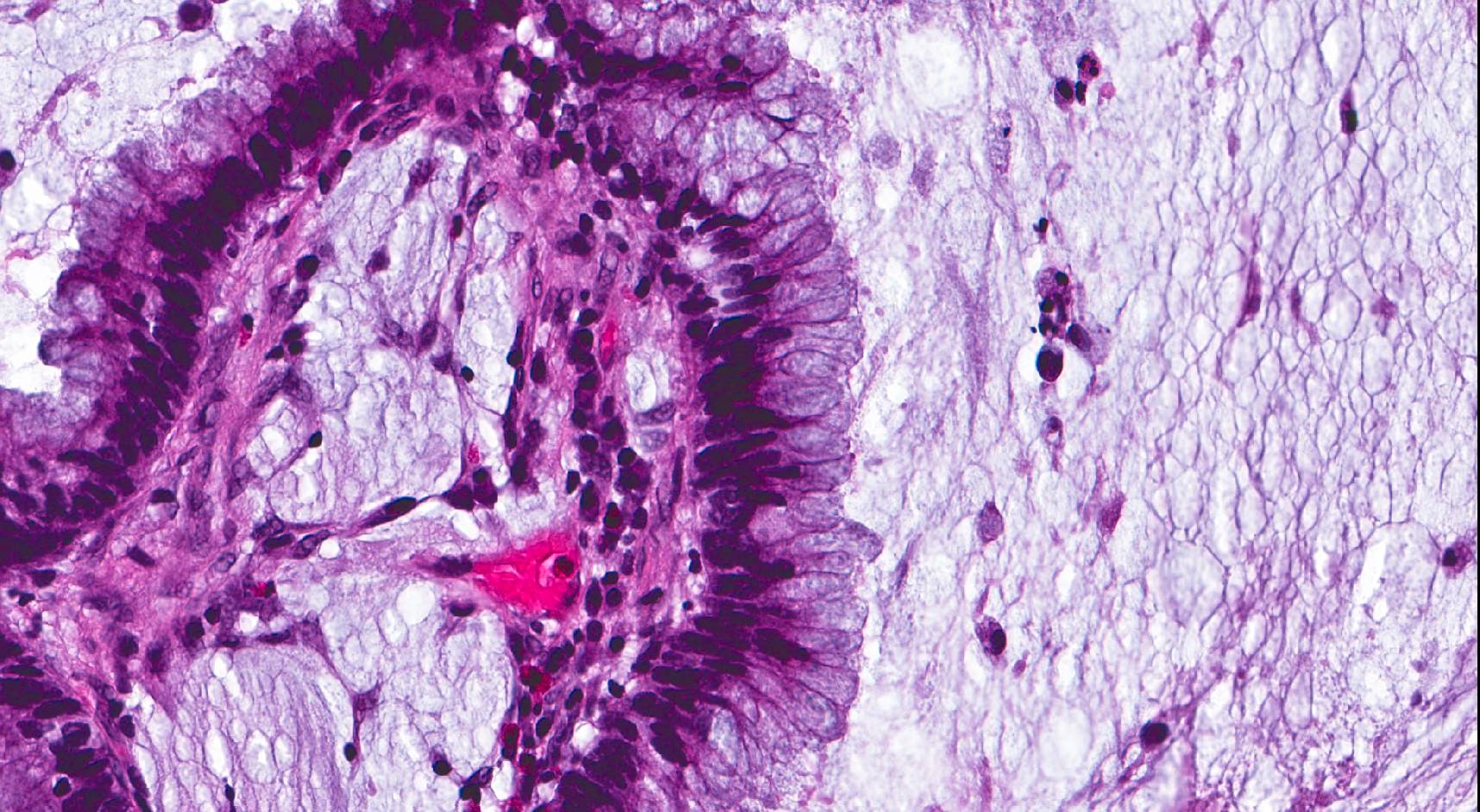
Contributed by Vladyslav Ilchenko, M.D., Diana Bell, M.D. and Kelly Magliocca, D.D.S., M.P.H.
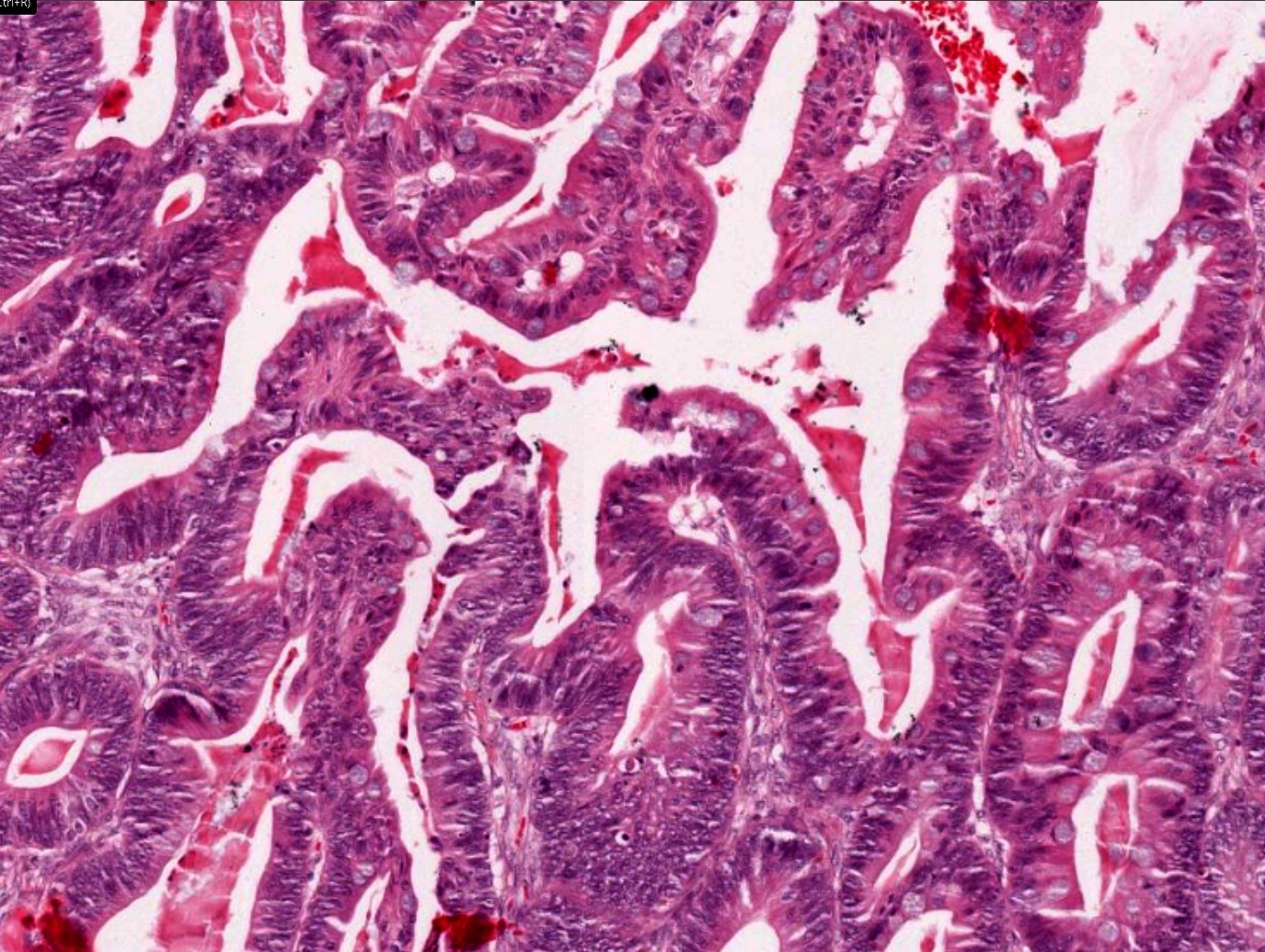
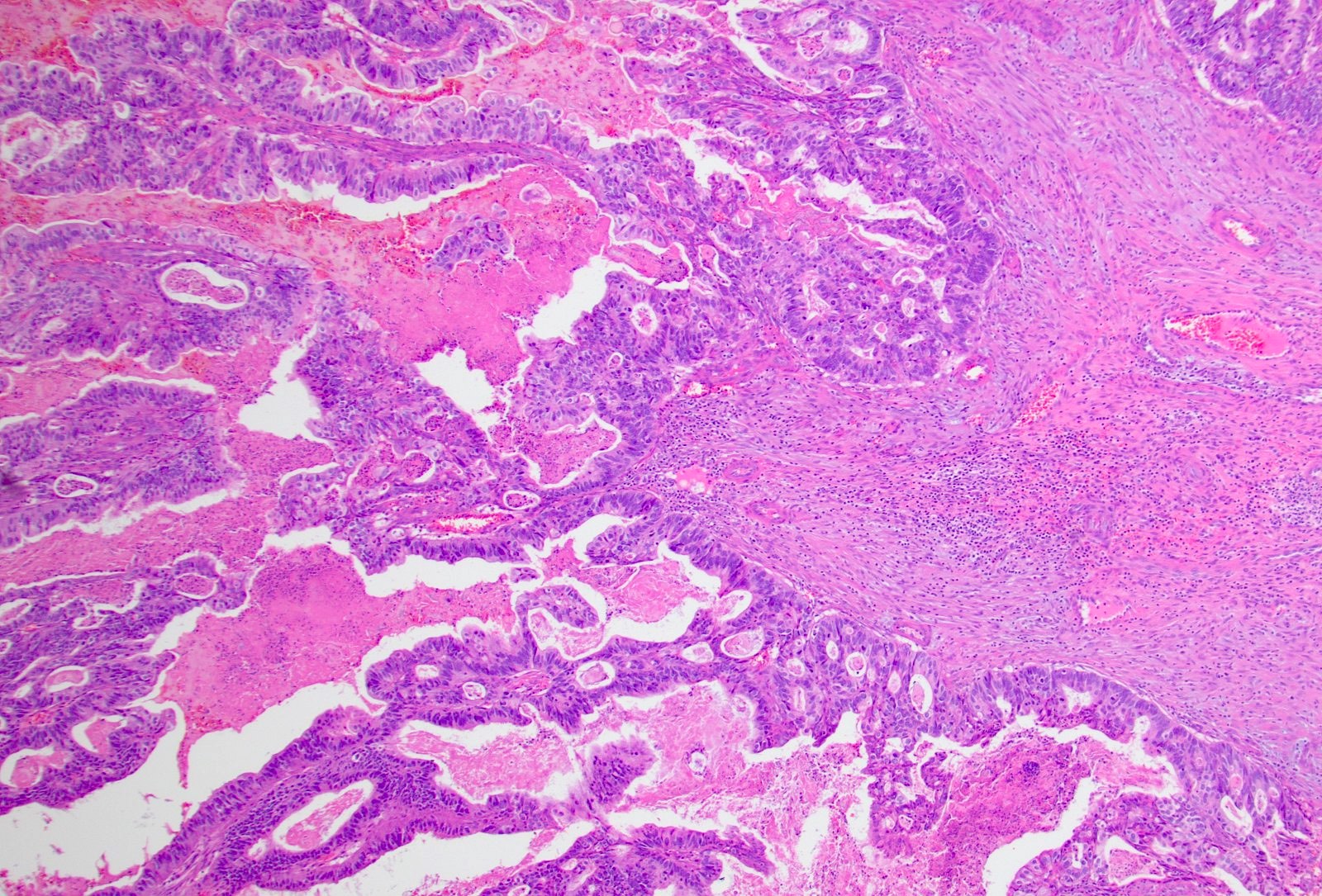
Complex glands
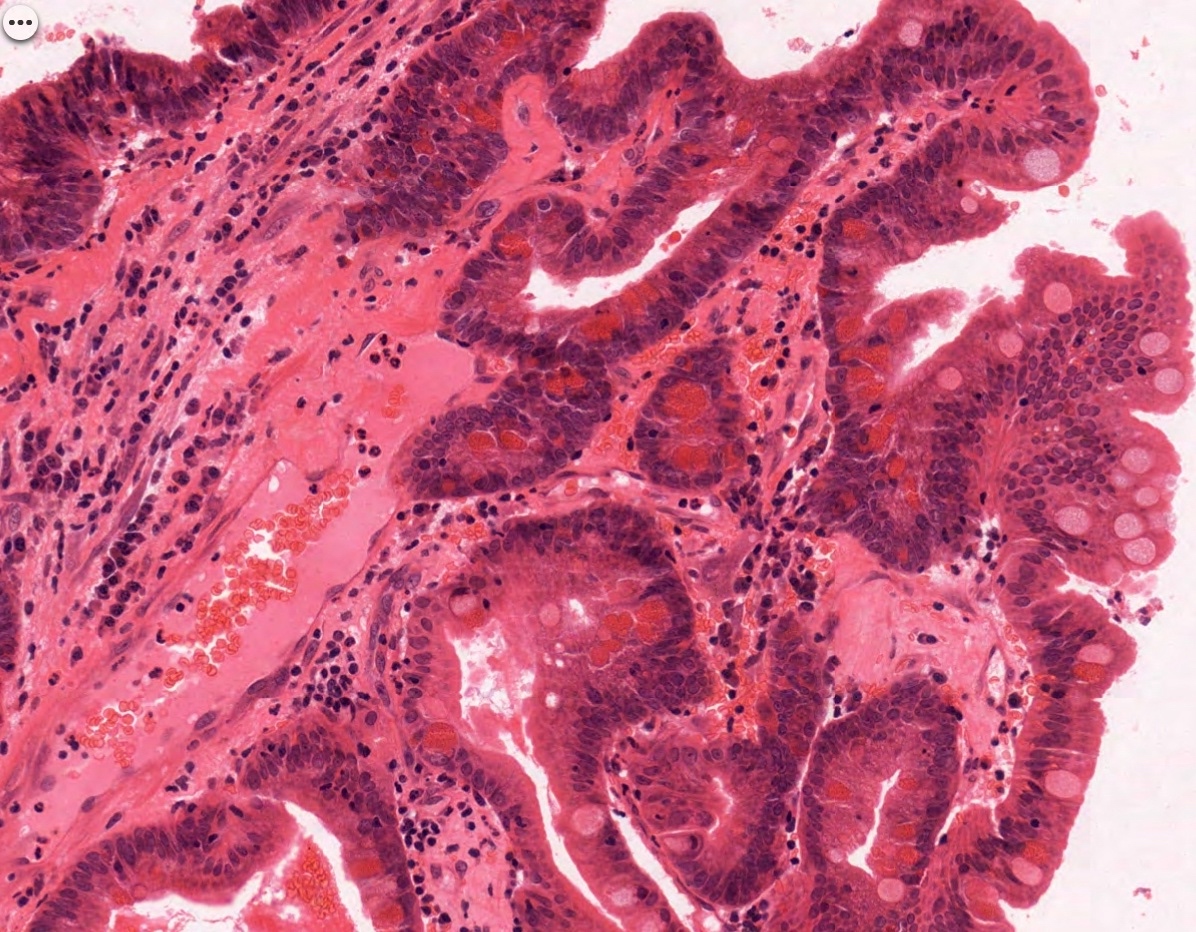
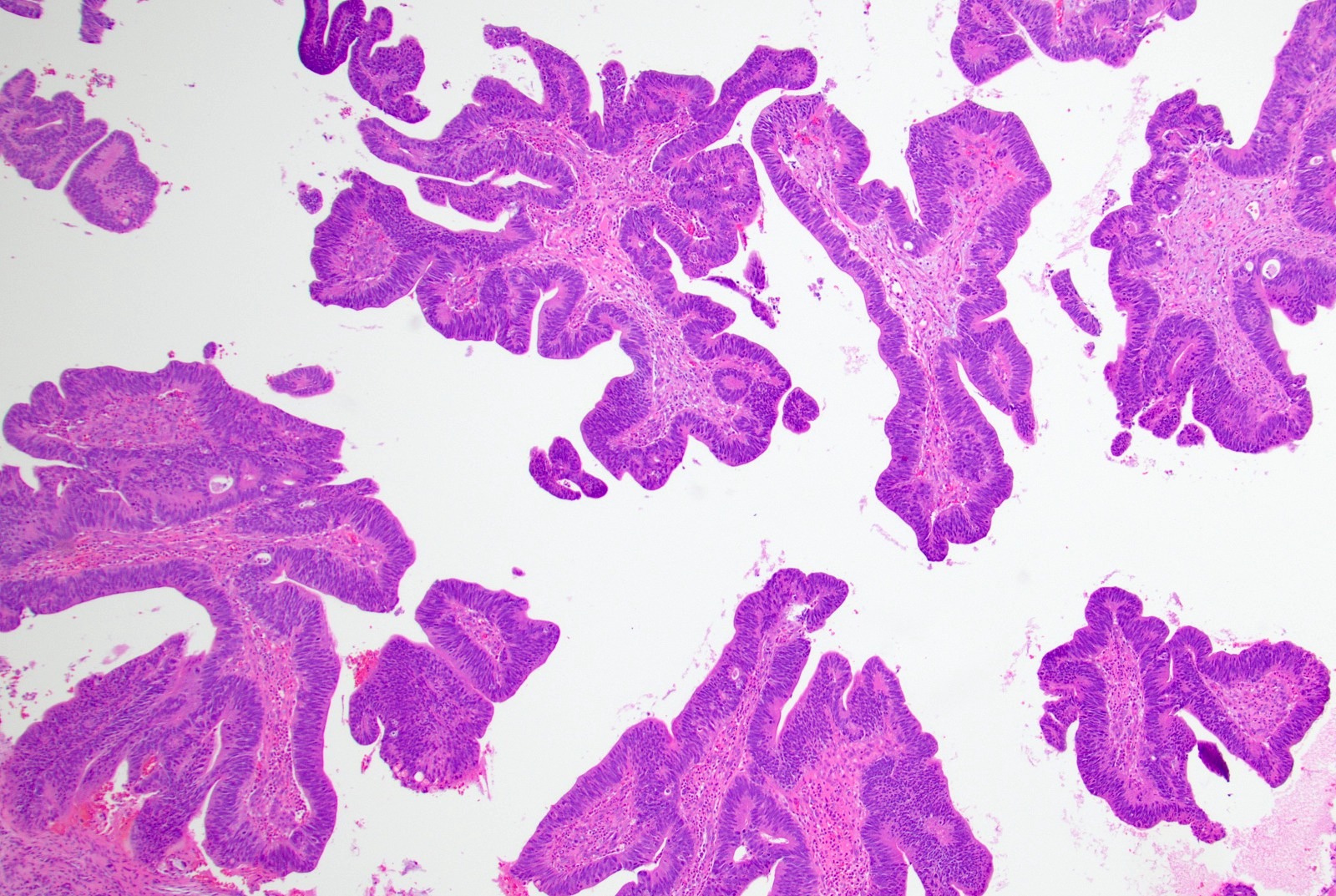
Papillary pattern with goblet cells
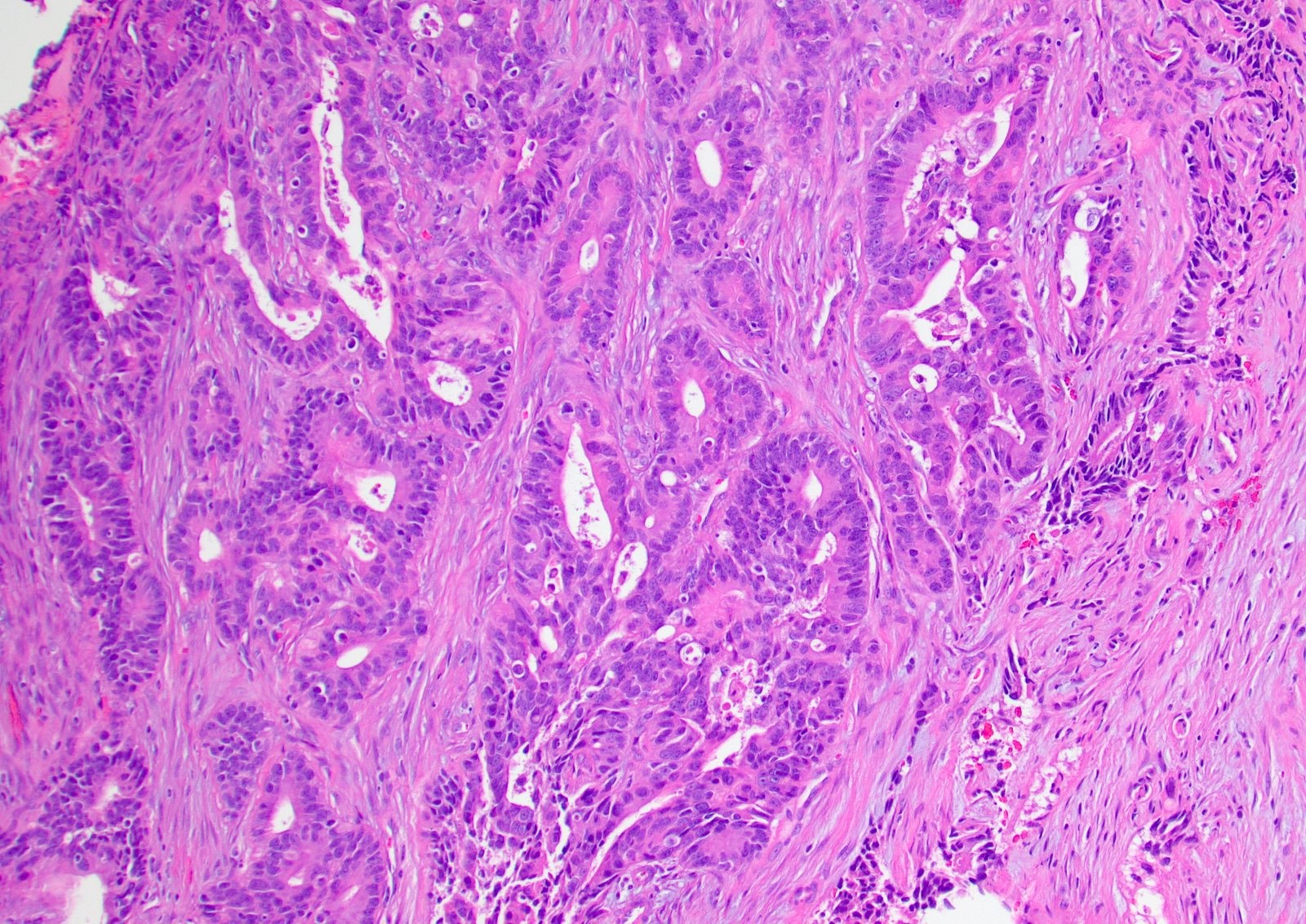
Tubuloglandular architecture
Complex colonic type glands and stroma
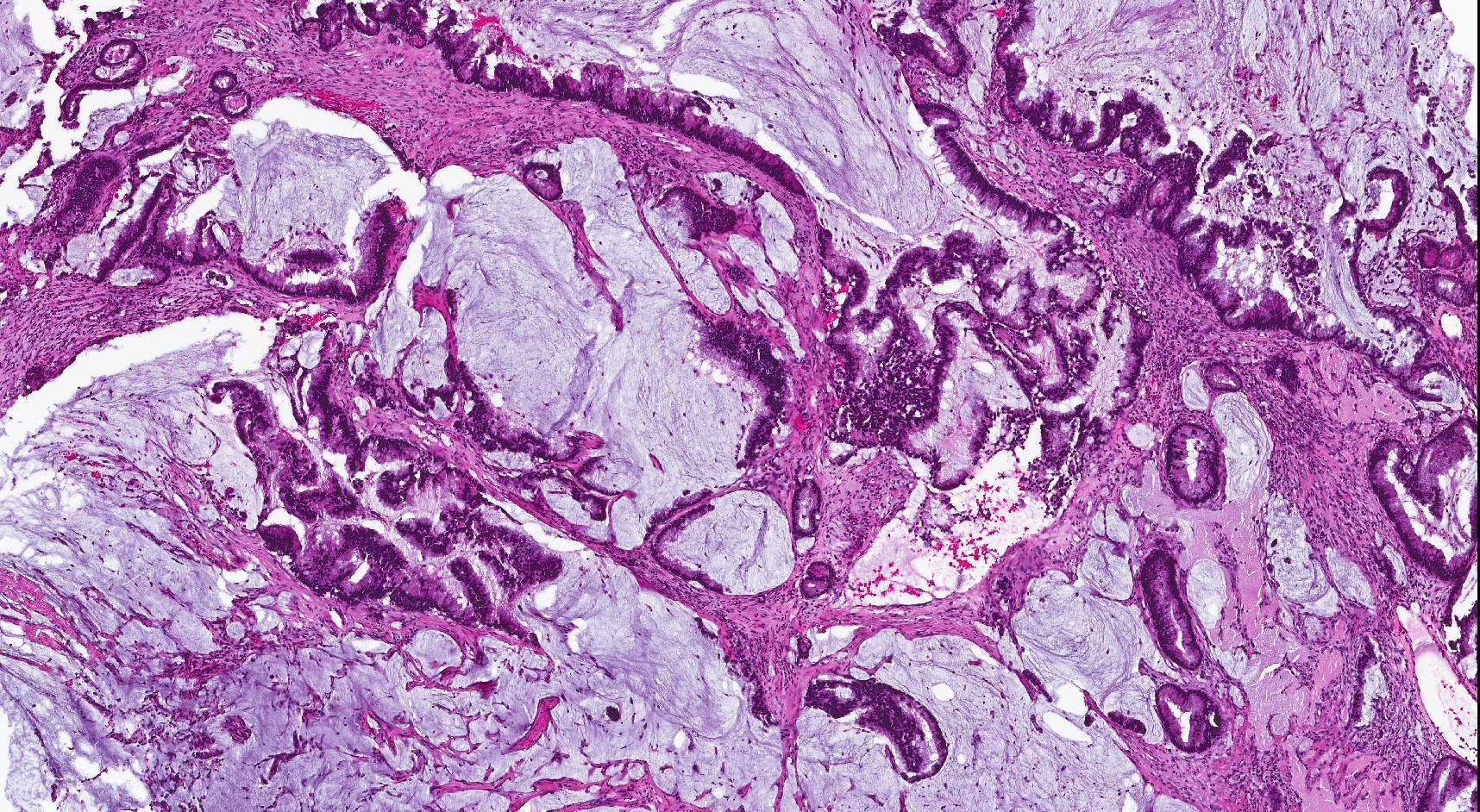
Mucinous type
Mucinous type
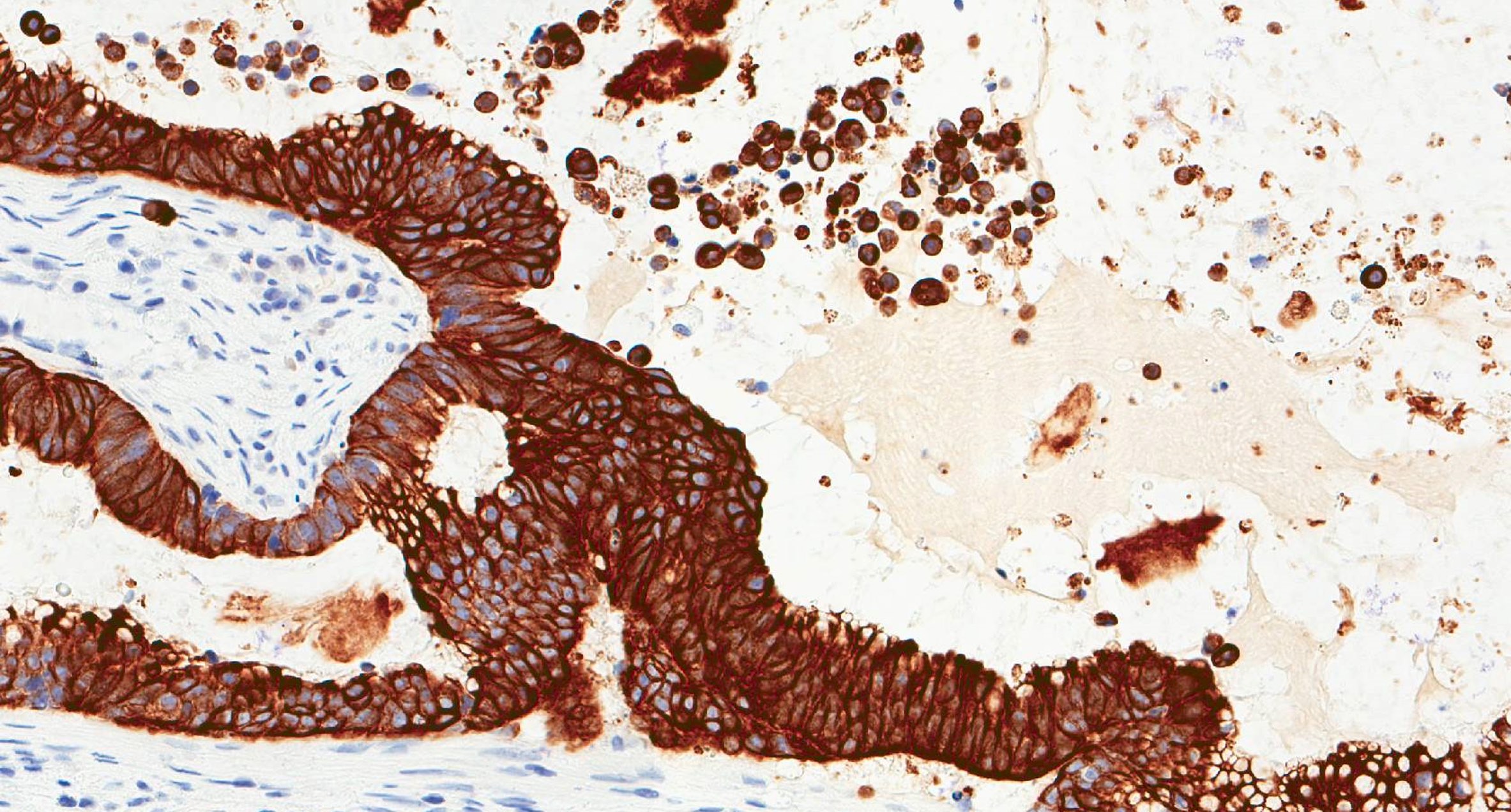
CK20
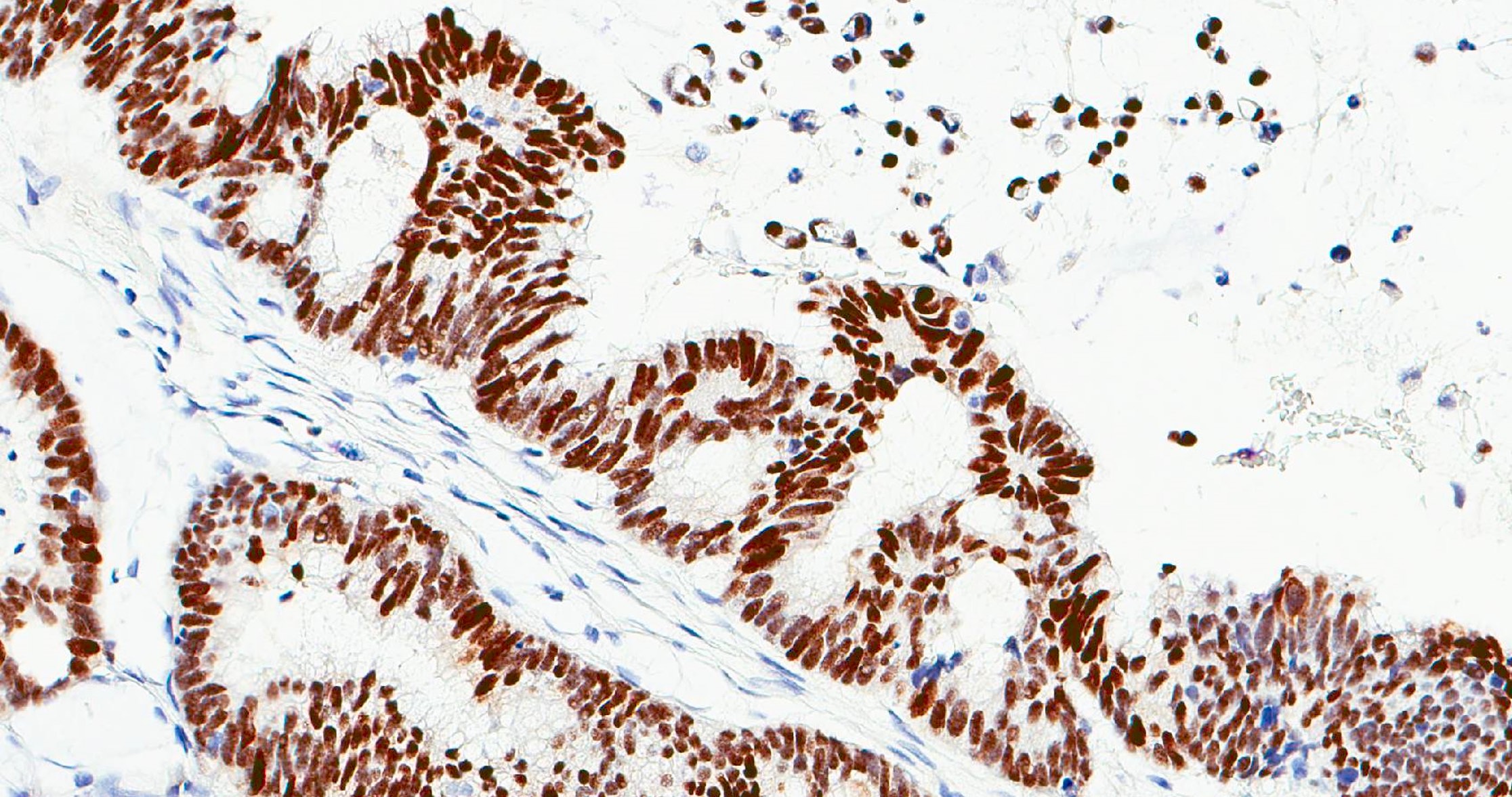
CDX2
Positive stains
- Consistently positive for CK20, CDX2, villin, MUC2, SATB2 (Head Neck Pathol 2022;16:670)
- Variably positive for CK7 and CEA
- Chromogranin+ cells may be present, scattered or in clusters
Molecular / cytogenetics description
- Frequent KRAS and p53 mutations (Head Neck Pathol 2022;16:670, Head Neck 2016;38:1564)
- Tumors with occupational exposure to wood dust show p53, p14 ARF, p16 INK4a gene deregulation
- EGFR alterations also reported (Cancers (Basel) 2021;13:5022)
- Mutations in the genes in Wnt, MAPK and PI3K pathways were reported in 20%, 20% and 24% of cases, respectively (Cancers (Basel) 2021;13:5022)
Videos
Update on sinonasal carcinoma
Malignant tumors of the paranasal sinuses
Sample pathology report
- Ethmoid sinus, biopsy:
- Invasive adenocarcinoma, intestinal type (see comment)
- Comment: The patient's clinical history of a mass in the right ethmoid sinus is noted. Morphology and immunophenotypic features (positive for CK7, CK20, villin and MUC2) are most consistent with intestinal type sinonasal adenocarcinoma. However, a metastasis from elsewhere, particularly the digestive tract, cannot be absolutely ruled out. Clinical and imaging correlation is suggested.
Differential diagnosis
- Nonintestinal sinonasal adenocarcinoma:
- Metastasis from colonic adenocarcinoma:
- Rare but most important differential
- Usually CEA+, CK7-, chromogranin-
- Clinical features and colonoscopy are helpful
- Papillary sinusitis:
- May have abundant mucinous material but has short and blunt papillae with clean background
- Thick and hyalinized basement membrane
- Ciliated surface cells
- Prominent eosinophils and no significant cytological atypia
Board review style question #1
A 70 year old man presented with a mass in the right nose and a frontal headache. A representative image of the mass is shown in the image above. Which of the following statements is true?
- Chemotherapy is the standard treatment
- Cigarette smoking is the number one risk factor for this tumor
- The tumor can be locally aggressive but rarely metastasizes
- The tumor is most commonly located in the nasal cavity
Board review style answer #1
C. The tumor can be locally aggressive but rarely metastasizes.
The image depicts intestinal type adenocarcinoma, with colonic type morphology. These tumors are known to be locally aggressive but metastasis is very uncommon (answer C). Ethmoid sinus is the most common location, not nasal cavity (answer D). Exposure to organic wood dust is considered as a strong risk factor. Unlike squamous cell carcinoma, cigarette smoking or human papillomavirus is not etiologically linked to ITAC (answer B). Surgical resection is the standard treatment, not chemotherapy (answer A).
Comment Here
Reference: Intestinal type adenocarcinoma
Comment Here
Reference: Intestinal type adenocarcinoma
Board review style question #2
Which of the following statements is true for intestinal type sinonasal adenocarcinoma?
- Signet ring cell morphology is the most common histologic pattern
- Tumor cells have uniform nuclei with salt and pepper chromatin
- Tumor may be positive for EBV
- Tumor usually demonstrates positive staining for CK20, villin or SATB2
Board review style answer #2
D. Tumor usually demonstrates positive staining for CK20, villin or SATB2. ITAC shows intestinal phenotype and shows immunoreactivity for CK20, villin and SATB2 (answer D). There is no association with EBV (answer C). Common histologic subtypes include colonic, papillary, solid, mucinous and mixed patterns. Signet ring cell morphology is uncommon (answer A). Salt and pepper nuclear chromatin is characteristically observed in neuroendocrine tumors and not in ITAC (answer B).
Comment Here
Reference: Intestinal type adenocarcinoma
Comment Here
Reference: Intestinal type adenocarcinoma

