
Nasal cavity, paranasal sinuses, nasopharynx
Infectious lesions
Fungal ball
Author: Bin Xu, M.D., Ph.D.
Editorial Board Member: Ruta Gupta, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 14 August 2024
Last staff update: 12 February 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Fungal ball nasal

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Xu B. Fungal ball. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalfungalball.html. Accessed March 27th, 2025.
Definition / general
- 1 of the 3 forms of noninvasive fungal infection of the sinonasal tract, the other 2 being saprophytic fungal infestation (localized colonization) and eosinophil related fungal rhinosinusitis, including allergic fungal rhinosinusitis (Laryngoscope 2009;119:1809)
- Noninvasive conglomeration of dense fungal hyphae in the sinonasal cavity, most frequently maxillary sinus
Essential features
- Dense concretion of fungal hyphae that is detached from the mucosa in the nasal cavity
- Absence of histopathologic evidence of tissue invasion
- Occurs in immunocompetent patients
- Fruiting heads (sexual reproduction, also called fruiting bodies, conidial heads) may be seen and are indicative of Aspergillus sp.
- Most common causal fungi are Aspergillus sp.
- May also coexist with other forms of fungal rhinosinusitis, most often allergic fungal rhinosinusitis (J Allergy Clin Immunol 1997;99:475)
Terminology
- Mycetoma (Laryngoscope 2009;119:1809)
- Aspergilloma
- Chronic noninvasive granuloma
ICD coding
Epidemiology
- ~4% of patients operated for chronic inflammatory conditions in nasal cavity and paranasal sinus (Head Neck 1997;19:481)
- 13 - 29% of chronic maxillary sinusitis (Eur Arch Otorhinolaryngol 2007;264:461)
- Mean age of presentation is 64 years, although a wide age range (14 - 90 years) can be affected (Rhinology 2005;43:34)
- Female predominance; F:M = 2:1
Sites
- Maxillary sinus is most commonly affected, followed by sphenoid sinus (Rhinology 2005;43:34)
- Usually affects just one sinus but bilateral or multisinus involvement has been reported
Etiology
- Aspergillus fumigatus is the most common causal fungus
- Other fungal organisms occasionally cultured include Scedosporium apiospermum, Aspergillus flavus, Aspergillus niger, Aspergillus terreus and Pleurophomopsis lignicola (Eur Arch Otorhinolaryngol 2007;264:461)
Clinical features
- Most with nonspecific complaints such as headache, facial pain, postnasal drip, cough and cacosmia (Rhinology 2005;43:34)
- 15 - 20% may be asymptomatic
Diagnosis
- Diagnostic clinicopathologic criteria proposed by DeShazo et al. include the following (J Allergy Clin Immunol 1997;99:475)
- Radiologically: sinus opacification with or without calcification
- Clinical / macroscopically: mucopurulent cheesy or clay-like material in the sinus
- Microscopically: a dense conglomeration of fungal hyphae separate from the sinus mucosa and a nonspecific chronic inflammation of the mucosa
- No histologic evidence of tissue invasion
Radiology description
- Unilateral partial or complete opacification with or without calcification of a single sinus (Can Assoc Radiol J 2017;68:178, Rhinology 2005;43:34)
- Metallic dense spot or iron-like signaling on CT reflects the iron, manganese and calcium content of fungal hyphae or calcification
- Adjacent bone shows sclerosis, thickening, bony erosion or remodeling
- Low signal on both T1 and T2 weighted MR
Radiology images
Images hosted on other servers:

CT: maxillary sinus opacity

MR: hypointensity of left maxilla

Maxillary opacity with calcification
Prognostic factors
- Surgical treatment frequently results in definitive cure
- Recurrent and persistent disease is rare and is most likely to occur in cases without adequate removal or with a major inflammatory reaction (Rhinology 2005;43:34)
Case reports
- 38 year old man with concurrent antrochoanal polyp and fungal ball in the maxillary sinus (Cureus 2021;13:e19844)
- 62 year old woman with fungal ball of sphenoid sinus (BJR Case Rep 2018;4:20170081)
- 70 and 78 year old women with fungus ball of the paranasal sinuses (Int Arch Otorhinolaryngol 2012;16:286)
Treatment
- Surgical treatment is indicated for symptomatic patients with opacified sinus confirmed by imaging studies (Eur Arch Otorhinolaryngol 2007;264:461)
- Systemic antimycotic treatment is not indicated
- Short term use of topical steroid and irrigation with saline may be used
Clinical images
Images hosted on other servers:

Brown mass on endoscope

Mass with cheesy material
Gross description
- Grumous, friable, gray-brown-black mass, often with clotted blood or a cheesy appearance
- No involvement of the underlying mucous membrane
Gross images
Contributed by @Andrew_Fltv on Twitter

Yellow friable mass
Images hosted on other servers:

Mucoid white-beige mass
Frozen section description
- Dense collection of fungal hyphae
- No evidence of tissue invasion
Frozen section images
Contributed by Bin Xu, M.D., Ph.D.
Dense collection of hyphae
Microscopic (histologic) description
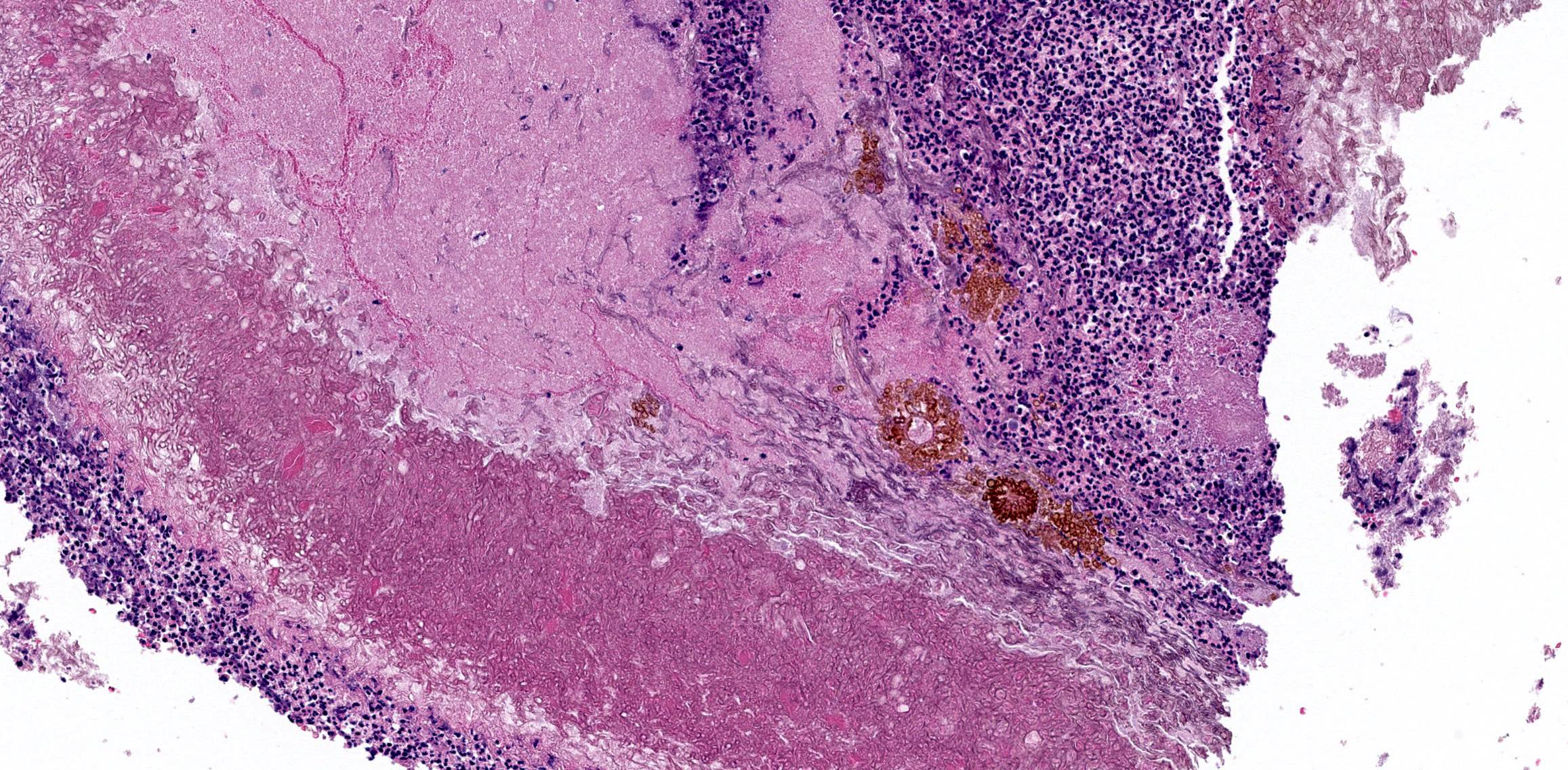
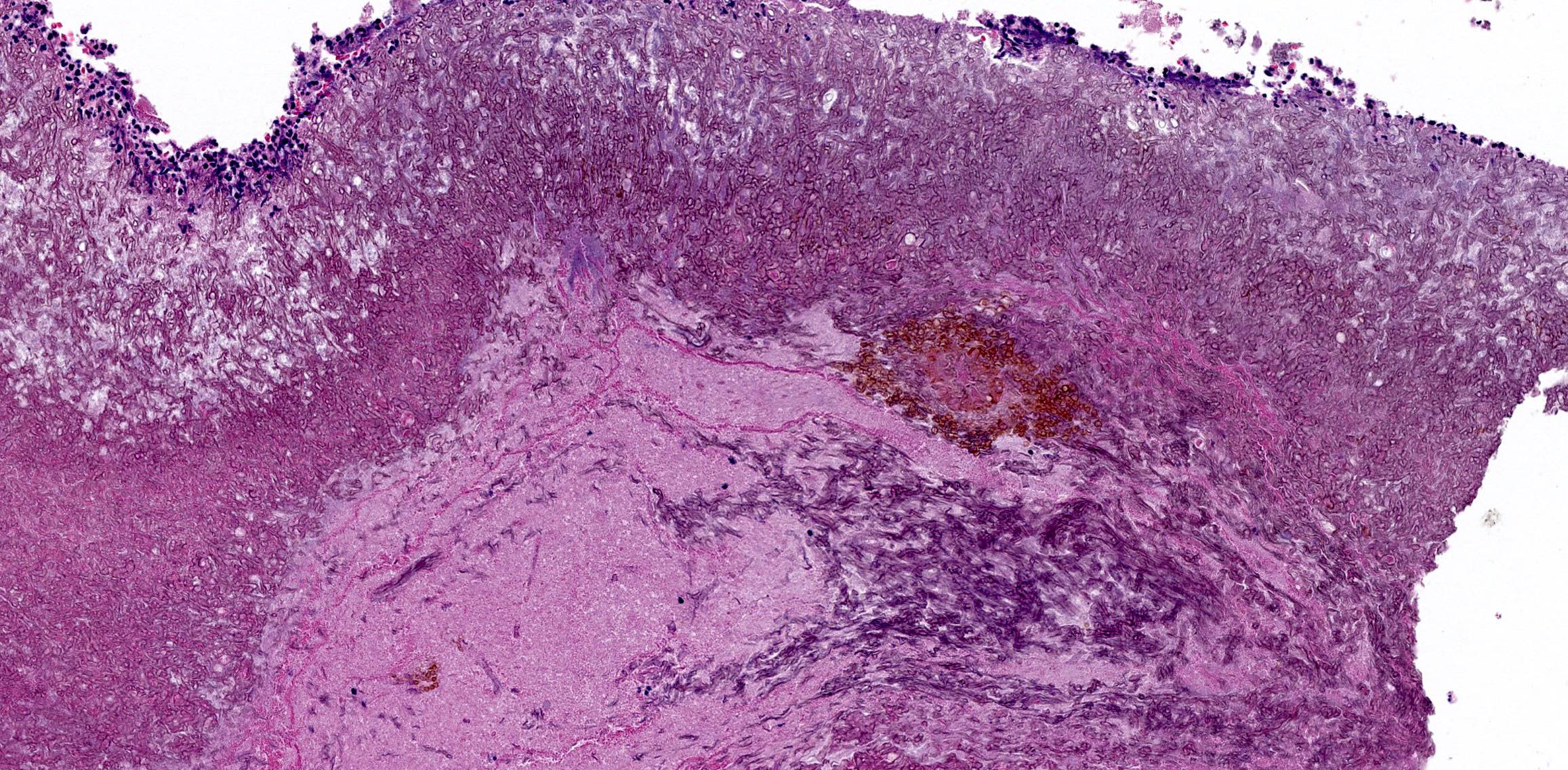
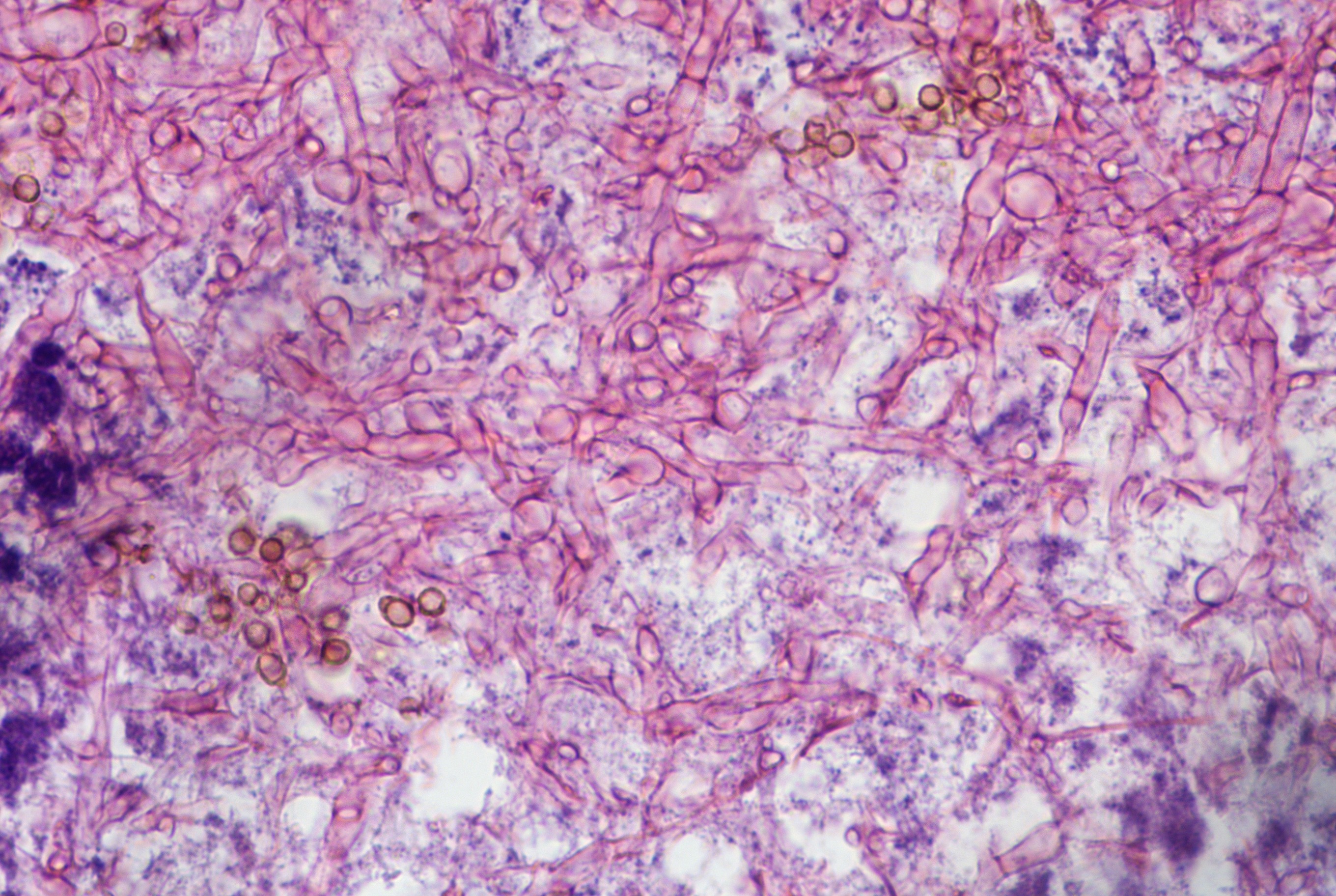
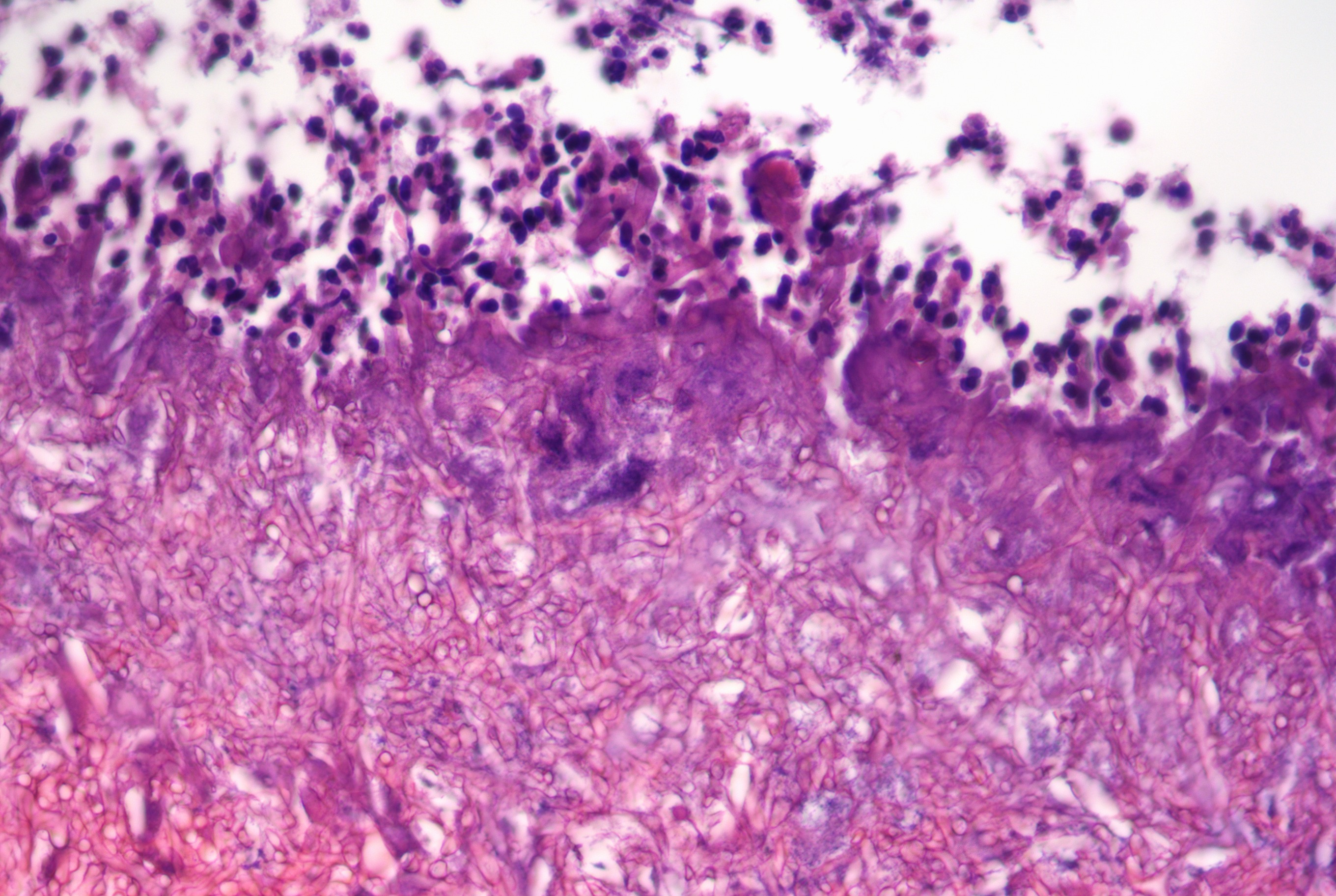
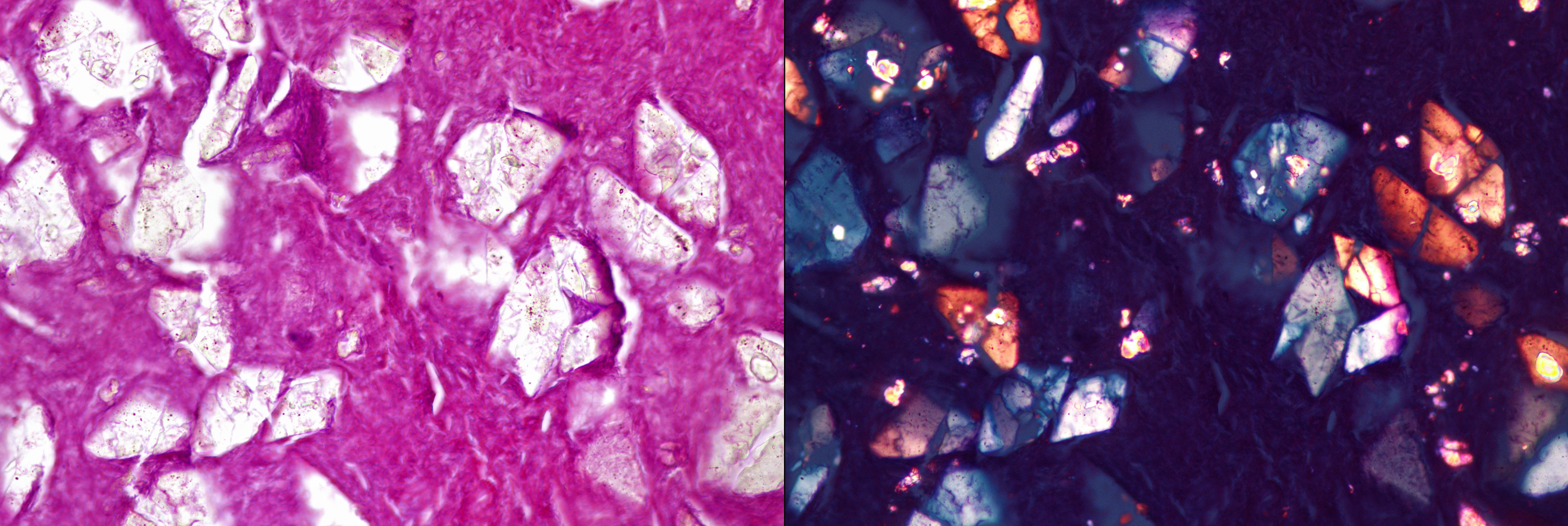
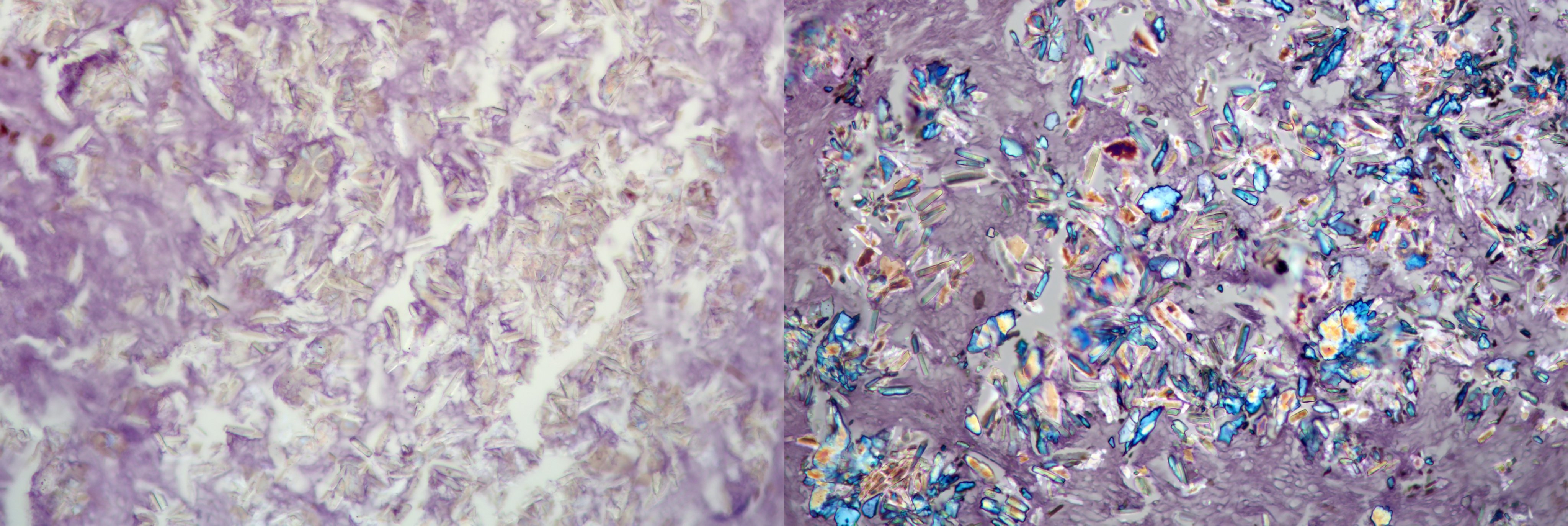
- Tightly packed fungal hyphae detached from the sinonasal mucosa (Head Neck Pathol 2016;10:40)
- May be associated with acute inflammatory exudates
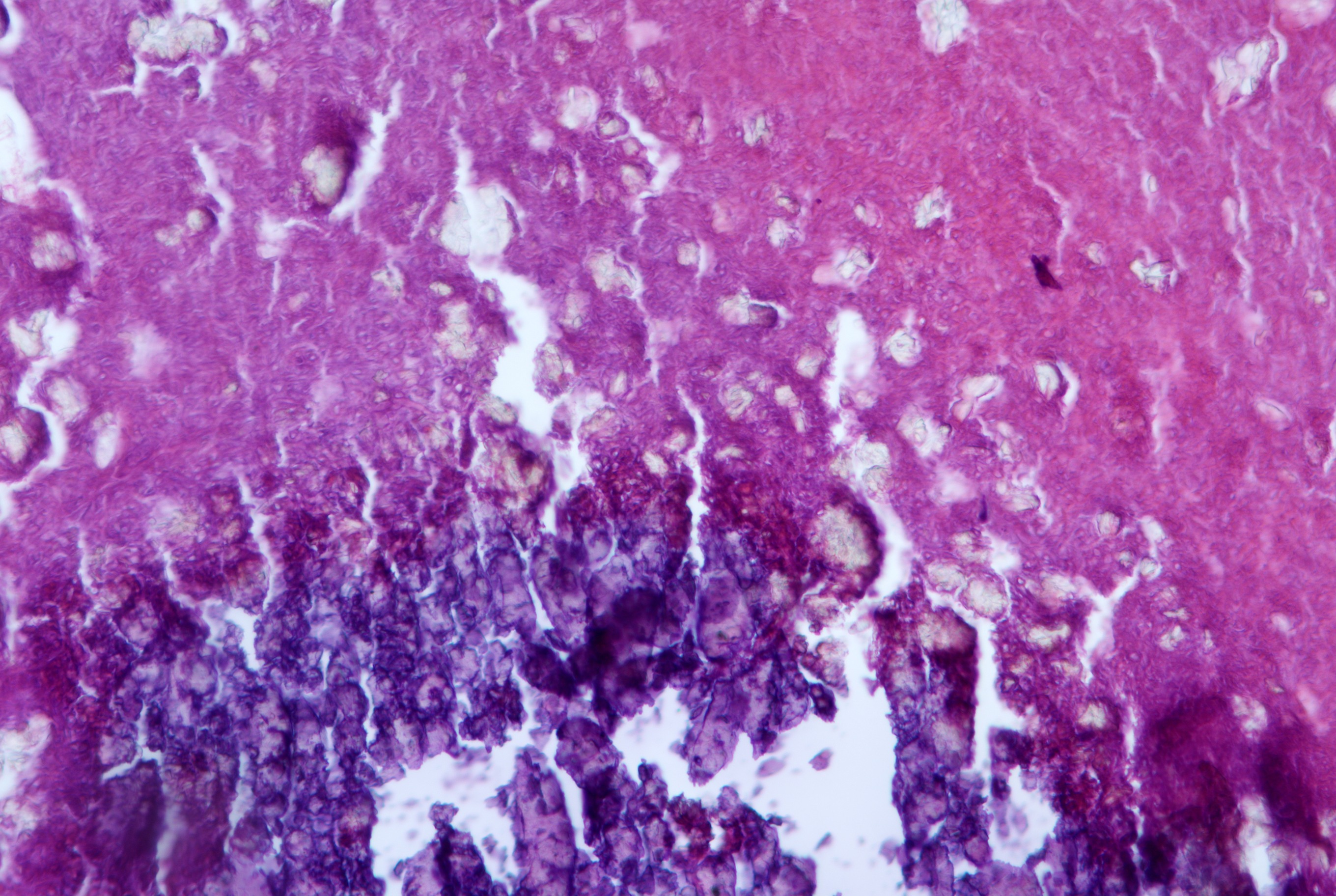
- Presence of characteristic fruiting heads is diagnostic for Aspergillus sp.
- Absence of tissue invasion
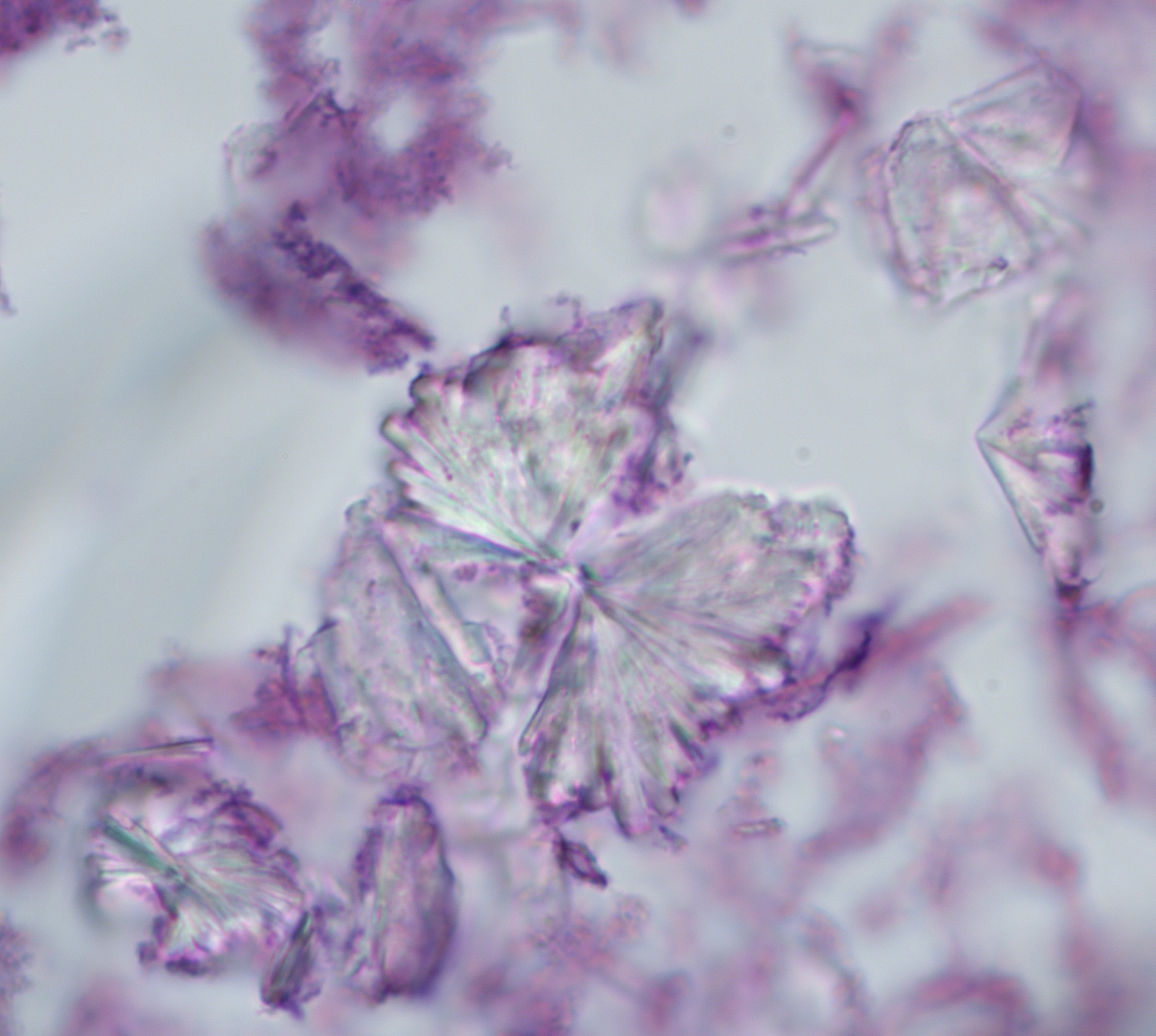
- Splendore-Hoeppli phenomenon: amorphous eosinophilic material surrounding fungal ball as a result of deposition of antigen antibody complexes and debris from host inflammatory cells (J Oral Maxillofac Pathol 2018;22:161)
Microscopic (histologic) images
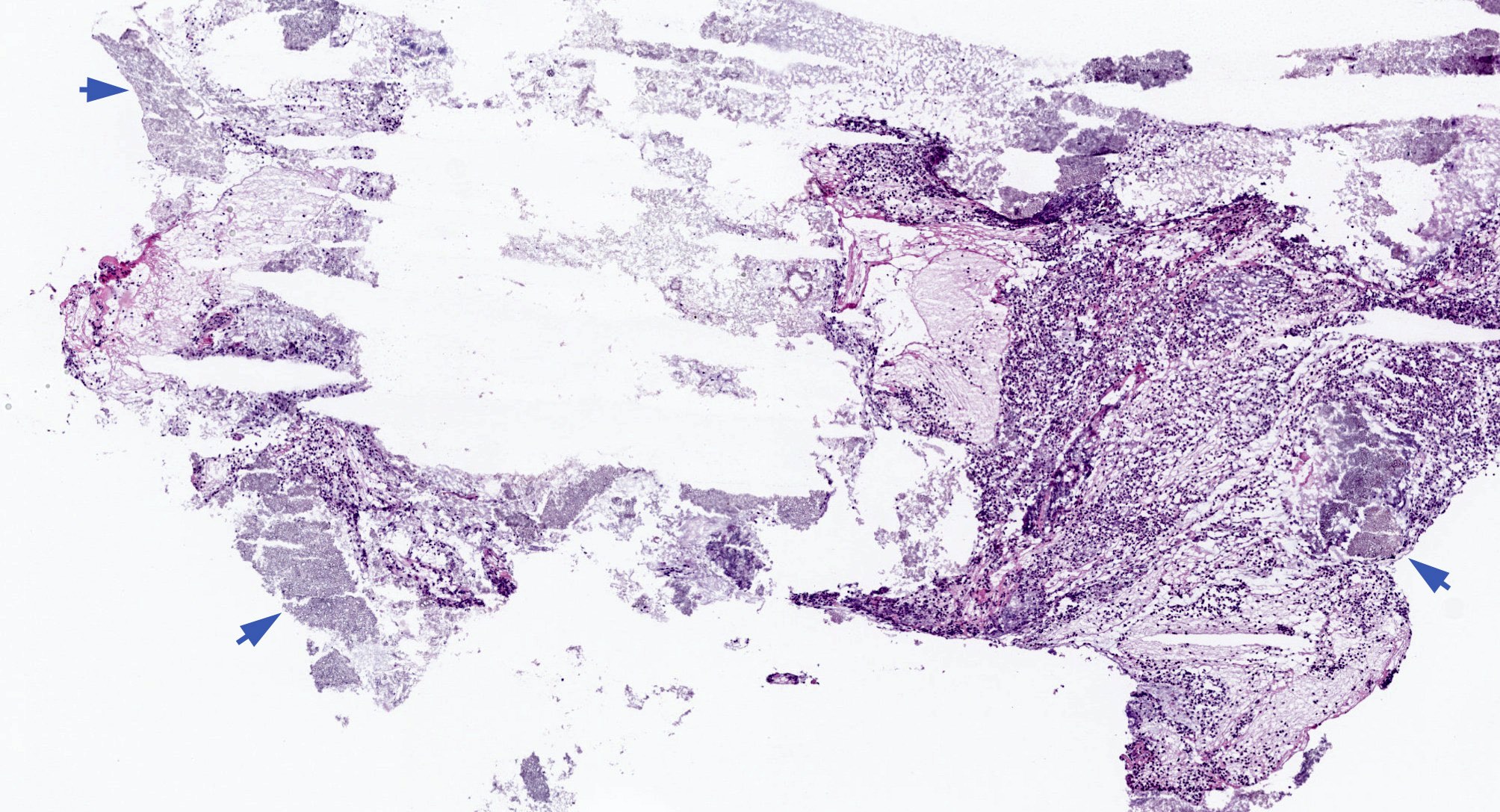
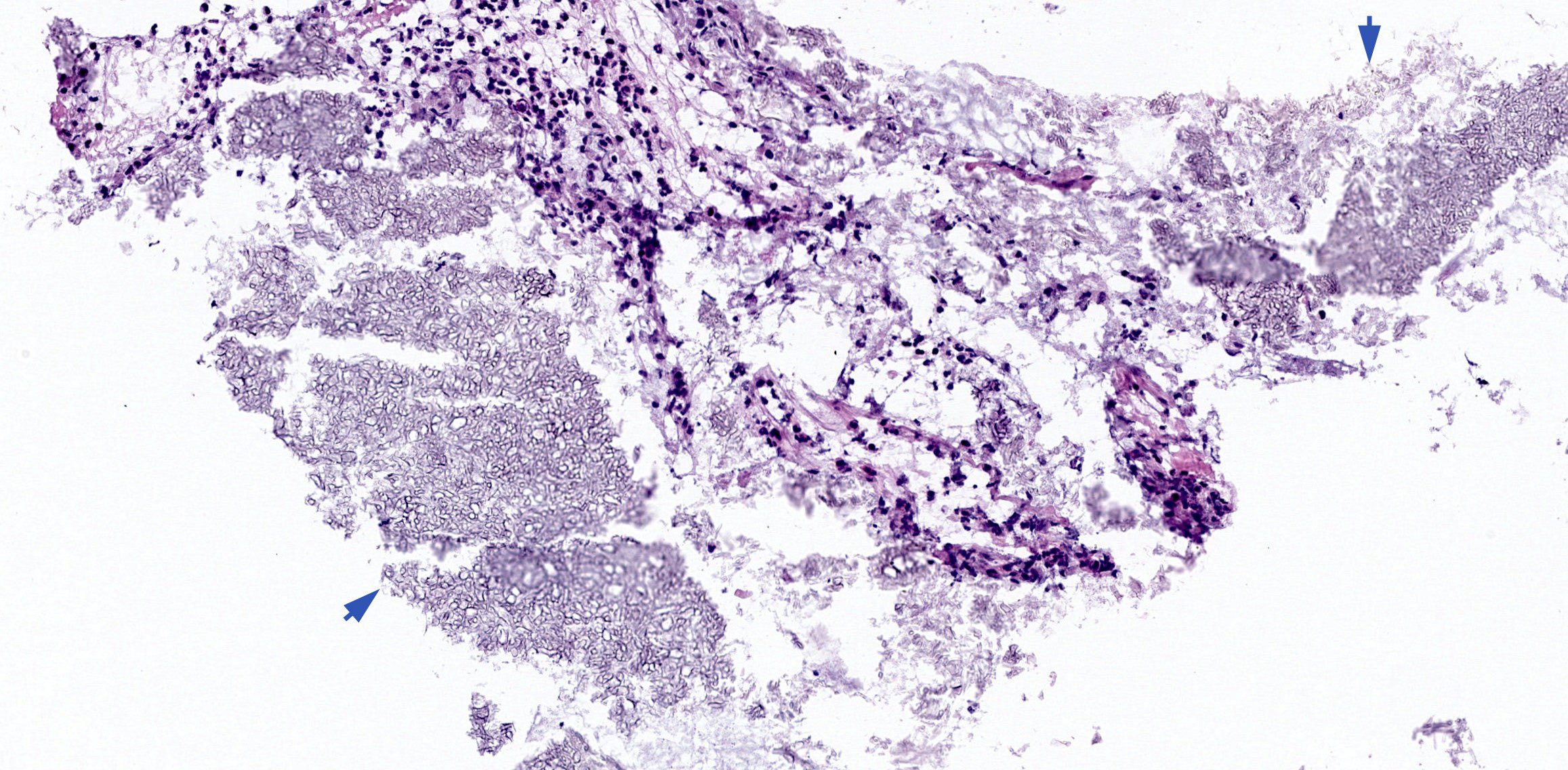
Contributed by Bin Xu, M.D., Ph.D. and @Andrew_Fltv on Twitter


Densely packed fungal hyphae
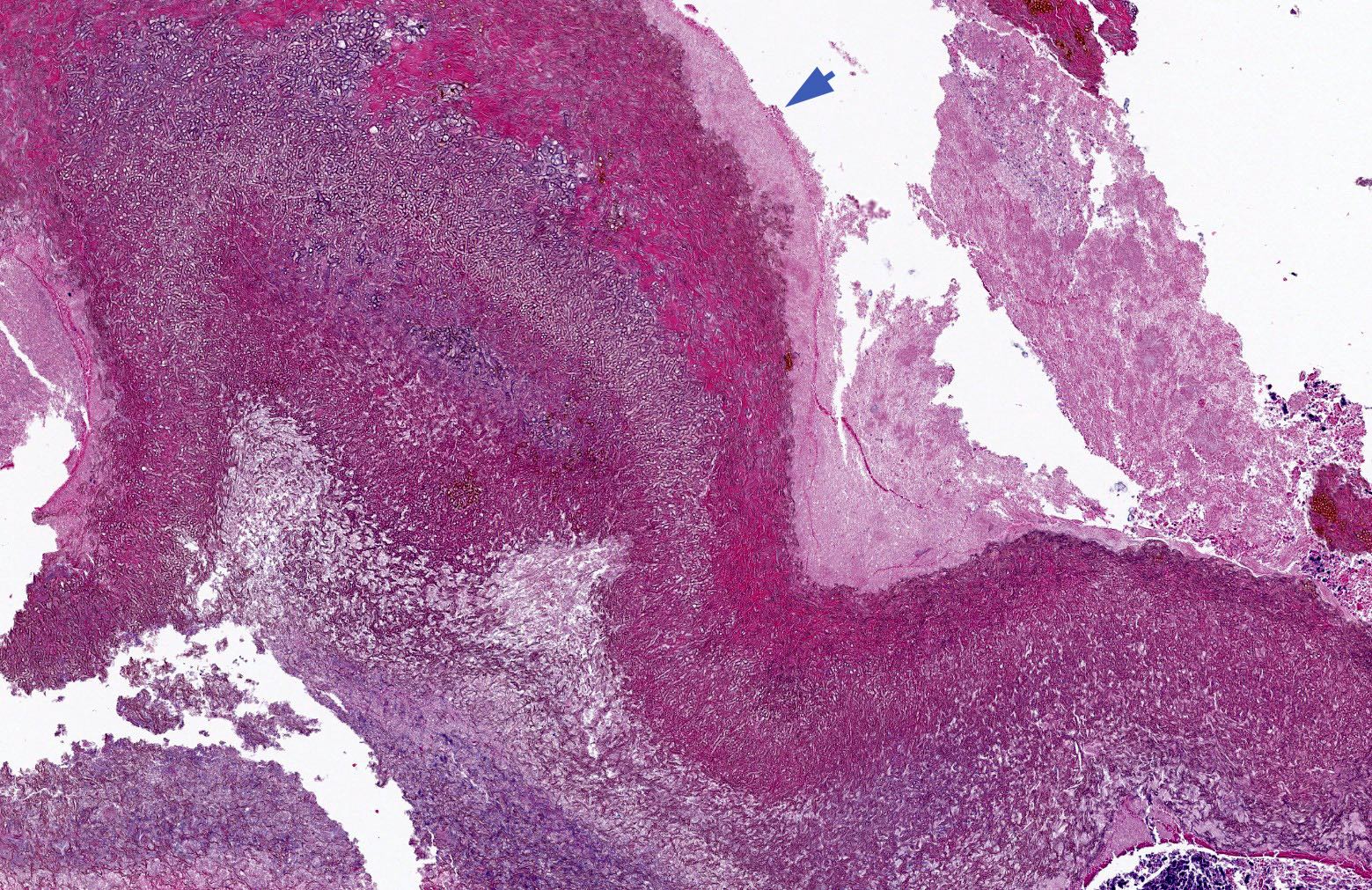
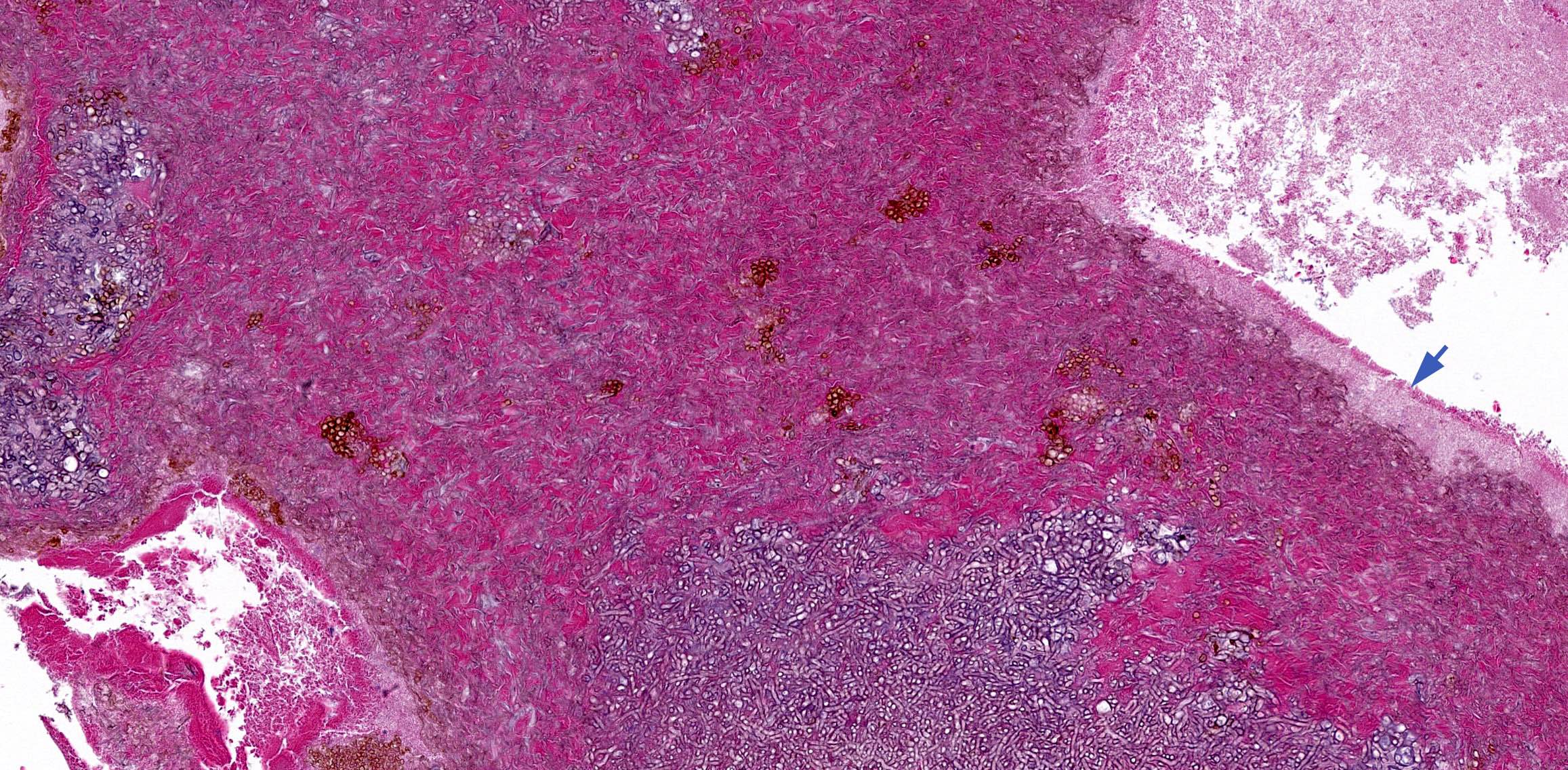
Splendore-Hoeppli phenomenon
Fruiting heads
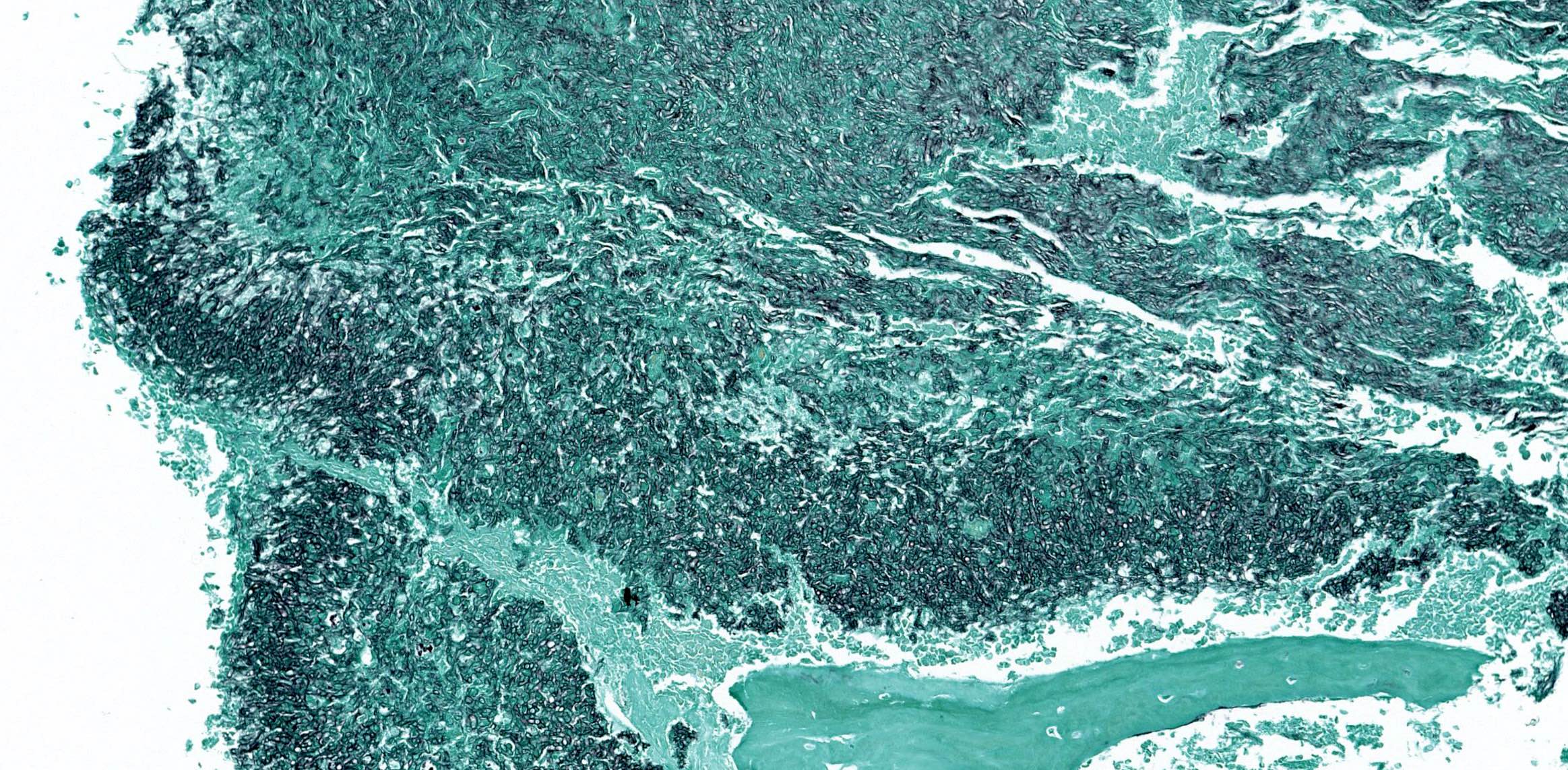

GMS stain shows hyphae
Fungal ball
Fungal ball
Aspergillus lesions of the sinuses
Sample pathology report
- Maxillary sinus content, right, excision:
- Fungal ball (see comment)
- Comment: The fungal ball is composed of sharp angled branching fungal hyphae and fruiting bodies, morphologically consistent with Aspergillus sp. No evidence of invasive fungal sinusitis is seen.
Differential diagnosis
- Invasive fungal rhinosinusitis:
- Shows evidence of tissue invasion or angioinvasion
- Most commonly caused by zygomycetes
- Fungal ball has no tissue invasion and is most commonly caused by Aspergillus sp.
- Allergic fungal rhinosinusitis:
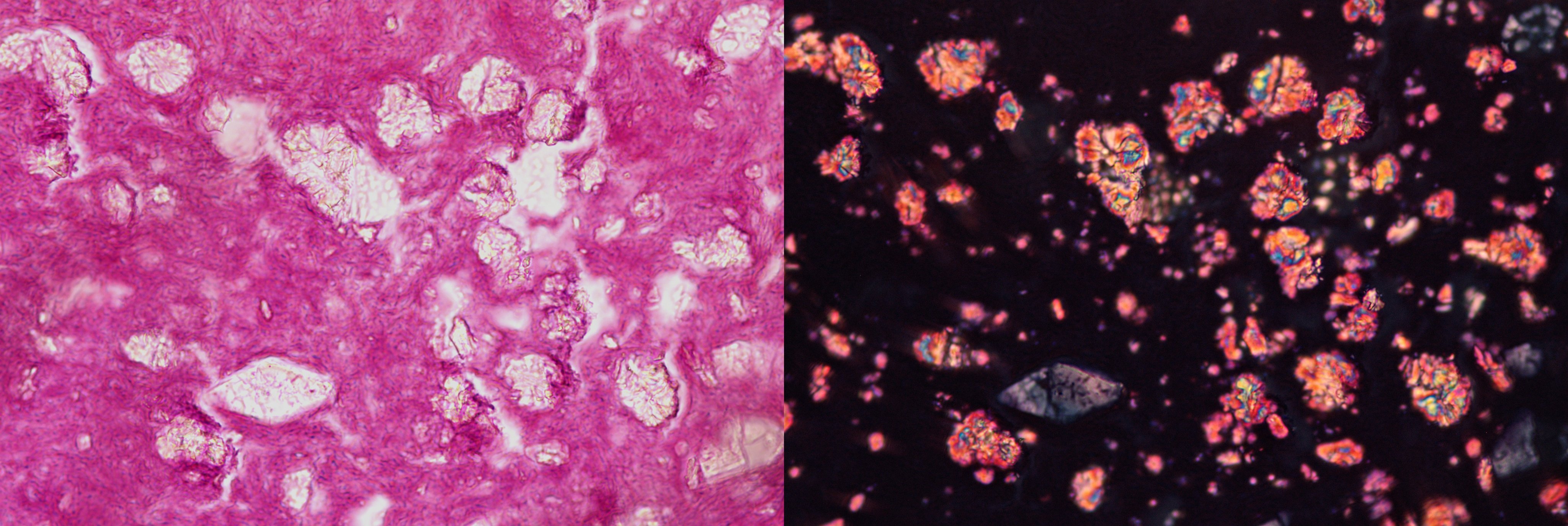
- Characterized by allergic mucin (eosinophilic mucin) defined as layered mucin with abundant eosinophils and Charcot-Leyden crystals
- Fungal hyphae may be absent and when present are sparse
- Lacks densely packed mass forming hyphae of fungal ball
- Occasionally can coexist with a fungal ball (Laryngoscope 2009;119:1809)
Board review style question #1
A 50 year old man presents with opacity of right maxillary sinus. A friable mass lesion is excised and is shown in the images above. What is the diagnosis?
- Allergic fungal rhinosinusitis
- Fungal ball
- Invasive fungal rhinosinusitis
- Rhinosporidiosis
Board review style answer #1
B. Fungal ball. The microscopic images show densely packed fungal hyphae forming a mass, which is characteristic for fungal ball. Answer A is incorrect because no allergic mucin is seen. Answer C is incorrect because the pictures show no evidence of tissue invasion. Answer D is incorrect because rhinosporidiosis contains sporangium of Rhinosporidium seeberi, whereas the pictures show fungal hyphae.
Comment Here
Reference: Fungal ball
Comment Here
Reference: Fungal ball
Board review style question #2
What is the most common fungal organism forming fungal balls in the sinonasal tract?
- Aspergillus sp.
- Candida albicans
- Mucor sp.
- Scedosporium apiospermum
Board review style answer #2
A. Aspergillus sp. The most common fungus identified in sinonasal fungal balls is Aspergillus sp., particularly Aspergillus flavus. Answers B - D are incorrect because they are fungi but not the most common cause of fungal ball.
Comment Here
Reference: Fungal ball
Comment Here
Reference: Fungal ball
