
Bone marrow neoplastic
Bone marrow - neoplastic myeloid
MDS / MPN
MDS / MPN with SF3B1 and thrombocytosis
Author: Patricia Tsang, M.D., M.B.A.
Editorial Board Member: Genevieve M. Crane, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.
Last author update: 14 March 2019
Last staff update: 22 September 2023
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Peripheral smear description | Peripheral smear images | Positive stains | Flow cytometry description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Tsang P. MDS / MPN with SF3B1 and thrombocytosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/myeloproliferativemdsmpnrst.html. Accessed April 1st, 2025.
Definition / general
- Clonal myeloid disorder with mixed myelodysplastic and myeloproliferative features
- Ring sideroblasts ≥ 15% of erythroblasts (Cancer Biol Med 2016;13:360)
- Persistent thrombocytosis ≥ 450 x 109/L (Blood Cancer J 2018;8:15)
- No increase in blast count, < 1% in blood and < 5% in bone marrow (Blood Cancer J 2018;8:15)
- Lacking BCR-ABL1, isolated del(5q), t(3;3)(q21.3;q26.2) and inv(3)(q21.3;q26.2) (Cancer Biol Med 2016;13:360)
- No previous history of myelodysplastic syndrome (MDS) or myeloproliferative neoplasm (MPN), except for MDS with ring sideroblasts
- New distinct entity in 2016 WHO classification; related to 2008 WHO provisional entity, refractory anemia with ring sideroblasts associated with marked thrombocytosis (RARS-T) (Blood Cancer J 2018;8:15, Haematologica 2015;100:1117)
Essential features
- Mixed myelodysplastic and myeloproliferative features with ring sideroblasts (≥ 15% of marrow erythroblasts), persistent thrombocytosis (≥ 450 x 109/L), anemia and normal blast count (Blood Cancer J 2018;8:15)
- Strong association with SF3B1 mutation; if absent, there should be no history of recent cytotoxic or growth factor therapy that could explain the MDS / MPN overlap features
- Often seen in conjunction with JAK2 V617F (and less often CALR or MPL gene mutations), which support but are not required for diagnosis (Haematologica 2015;100:1117, Blood 2016;127:2391)
- In contrast to MDS with ring sideroblasts, at least 15% ring sideroblasts are required even if an SF3B1 mutation is present (Blood 2016;127:2391)
Terminology
- Myelodysplastic and myeloproliferative neoplasm with ring sideroblasts and thrombocytosis (MDS / MPN-RS-T)
- Previously, refractory anemia with ring sideroblasts associated with marked thrombocytosis (RARS-T)
ICD coding
- ICD-10: D46.9 - myelodysplastic syndrome, unspecified
Epidemiology
- Median age mid 70s, range 18 - 95 years (Cancer Biol Med 2016;13:360)
- About equal gender distribution (Cancer Biol Med 2016;13:360)
Sites
- Myeloid cells primarily in bone marrow and blood
- Splenomegaly 40%
- Occasional hepatomegaly
Pathophysiology
- Probable multistep genetic and epigenetic changes, leading to signaling deregulation, impaired DNA damage response and other cellular abnormalities (Int J Hematol 2015;101:229)
Etiology
- Unclear
Clinical features
- Anemia due to ineffective erythropoiesis
- Thrombosis more likely than MDS with ring sideroblasts (Cancer Biol Med 2016;13:360)
Diagnosis
- Anemia with dyserythropoietic changes (Haematologica 2015;100:1117)
- Ring sideroblasts ≥ 15% of erythroblasts (Blood Cancer J 2018;8:15)
- Persistent thrombocytosis ≥ 450 x 109/L (Blood Cancer J 2018;8:15)
- Blast count < 1% in blood and < 5% in bone marrow (Blood Cancer J 2018;8:15)
- SF3B1 mutation or in absence of SF3B1 mutation, no history of recent cytotoxic or growth factor therapy (Haematologica 2015;100:1117)
- No BCR-ABL1 fusion; no rearrangement of PDGFRA, PDGFRB or FGFR1; no PCM1-JAK2, t(3;3)(q21.3;q26.2), inv(3)(q21.3;q26.2) or del(5q) (Cancer Biol Med 2016;13:360)
- No history of MPN, MDS (except for MDS with ring sideroblasts) or MDS / MPN neoplasm (Blood Cancer J 2018;8:15)
Laboratory
- Macrocytic or normocytic anemia
- Thrombocytosis, ≥ 450 x 109/L
- White blood cell (WBC) absolute and differential counts usually normal but mild leukocytosis can occur
Prognostic factors
- Median survival 76 - 128 months (Am J Hematol 2016;91:492)
- Worse outcome than essential thrombocythemia (Am J Hematol 2019;94:475)
- Low risk of acute leukemic transformation (Am J Hematol 2017;92:297, Am J Hematol 2016;91:492)
- SF3B1 mutation longer survival (6.9 years) than wild type (3.3 years) (Leukemia 2013;27:1826)
- JAK2 V617F mutation more favorable than wild type (Leukemia 2013;27:1826, Am J Hematol 2016;91:492)
- ASXL1 or SETBP1 mutation shorter survival (Am J Hematol 2017;92:297, Am J Hematol 2016;91:492)
- Hemoglobin < 10 g/dL or abnormal karyotype shorter survival (Am J Hematol 2016;91:492)
Case reports
- 58 year old man with transfusion dependent anemia, markedly elevated platelet count and marrow changes (Blood Res 2017;52:8)
- 69 year old man with progressive thrombocytosis and suspicion of essential thrombocythemia (Blood 2013;121:4256)
- 75 year old woman presenting with chronic anemia (Blood 2014;123:314)
- 75 year old man with prefibrotic / early primary myelofibrosis (Blood 2017;129:657)
- 80 year old man with history of radiotherapy treated prostate cancer (Rev Bras Hematol Hemoter 2014;36:69)
Treatment
- No specific therapy, only general treatment for lower risk MDS and MPN (Haematologica 2015;100:1117)
- Aspirin may be used (Am J Hematol 2017;92:297)
- Luspatercept may improve anemia (Am J Hematol 2019;94:475)
- Anecdotal reports of response with single agent lenalidomide (Blood 2010;116:180, Am J Hematol 2018;93:E27)
Microscopic (histologic) description
- Hypercellularity of bone marrow with < 5% blasts
- Erythroid hyperplasia with dyserythropoiesis, including megaloblastic change, common in marrow
- Ring sideroblasts ≥ 15% of normoblasts on iron stain (Blood Cancer J 2018;8:15)
- Multilineage dysplasia possible
- Atypical megakaryocytic hyperplasia and cluster formation with large, hyperlobated megakaryocytes, reminiscent of BCR-ABL negative MPN (Haematologica 2015;100:1117)
- Marrow fibrosis can occur
Microscopic (histologic) images
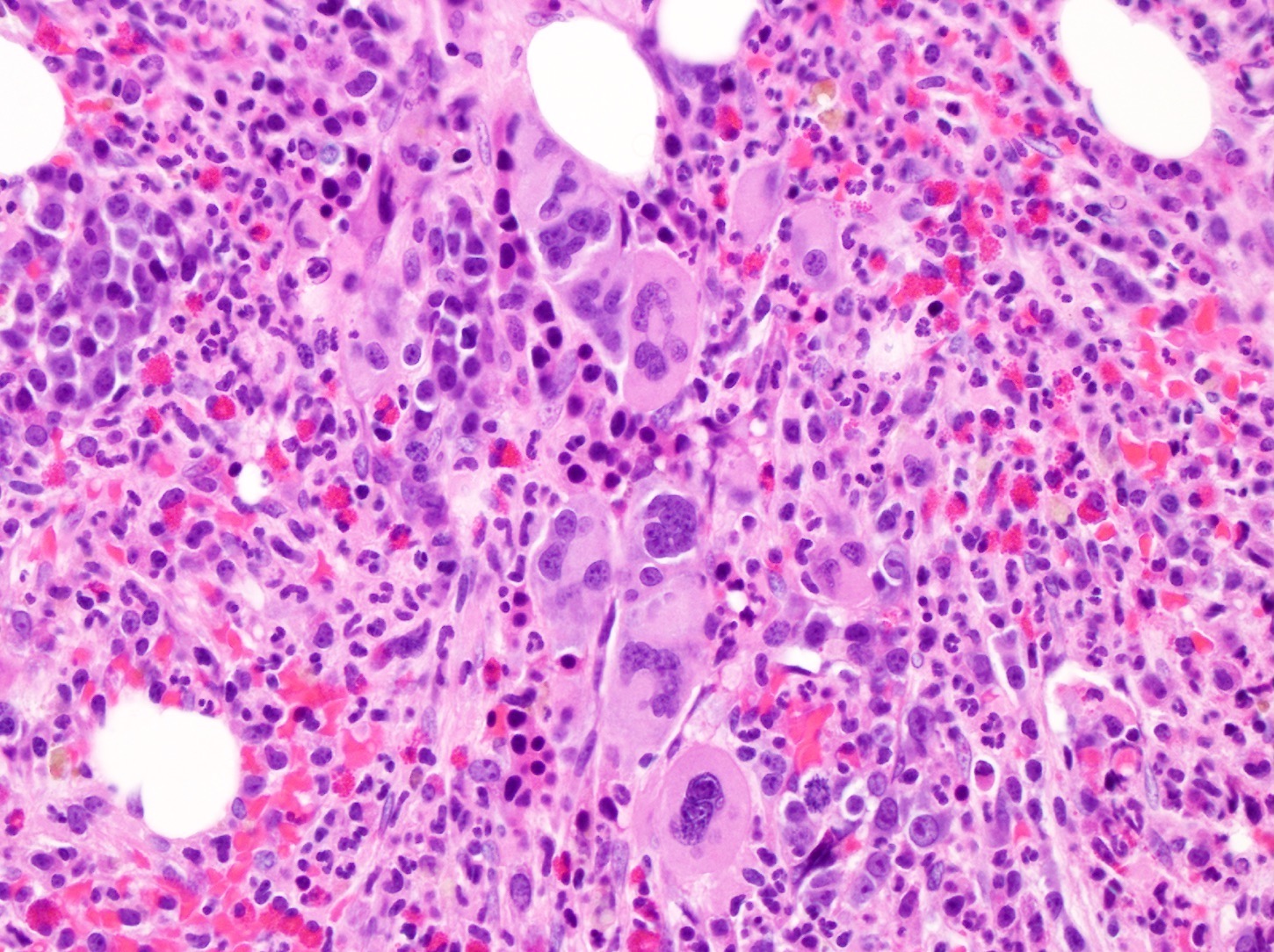
Contributed by Patricia Tsang, M.D., M.B.A.
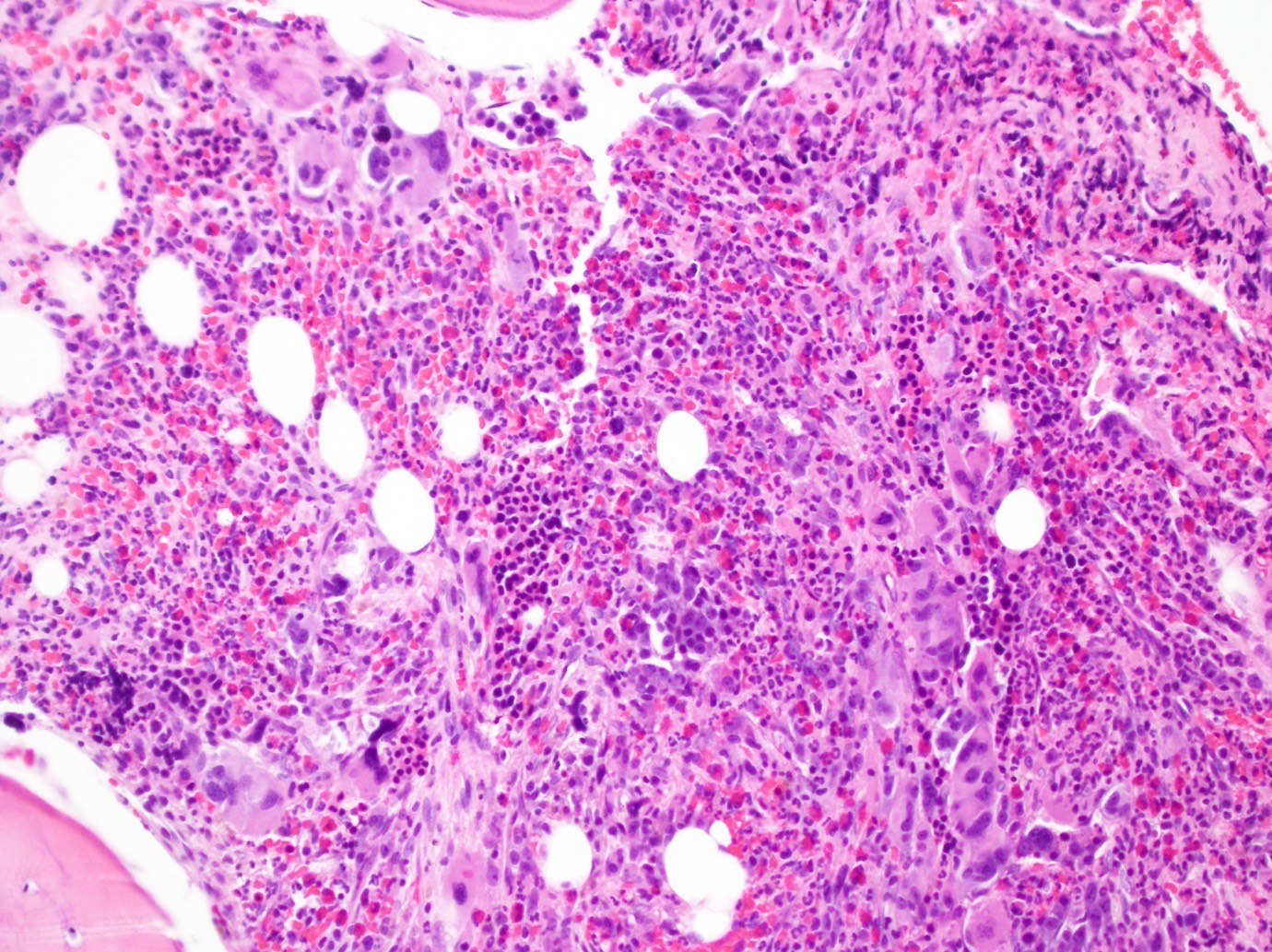
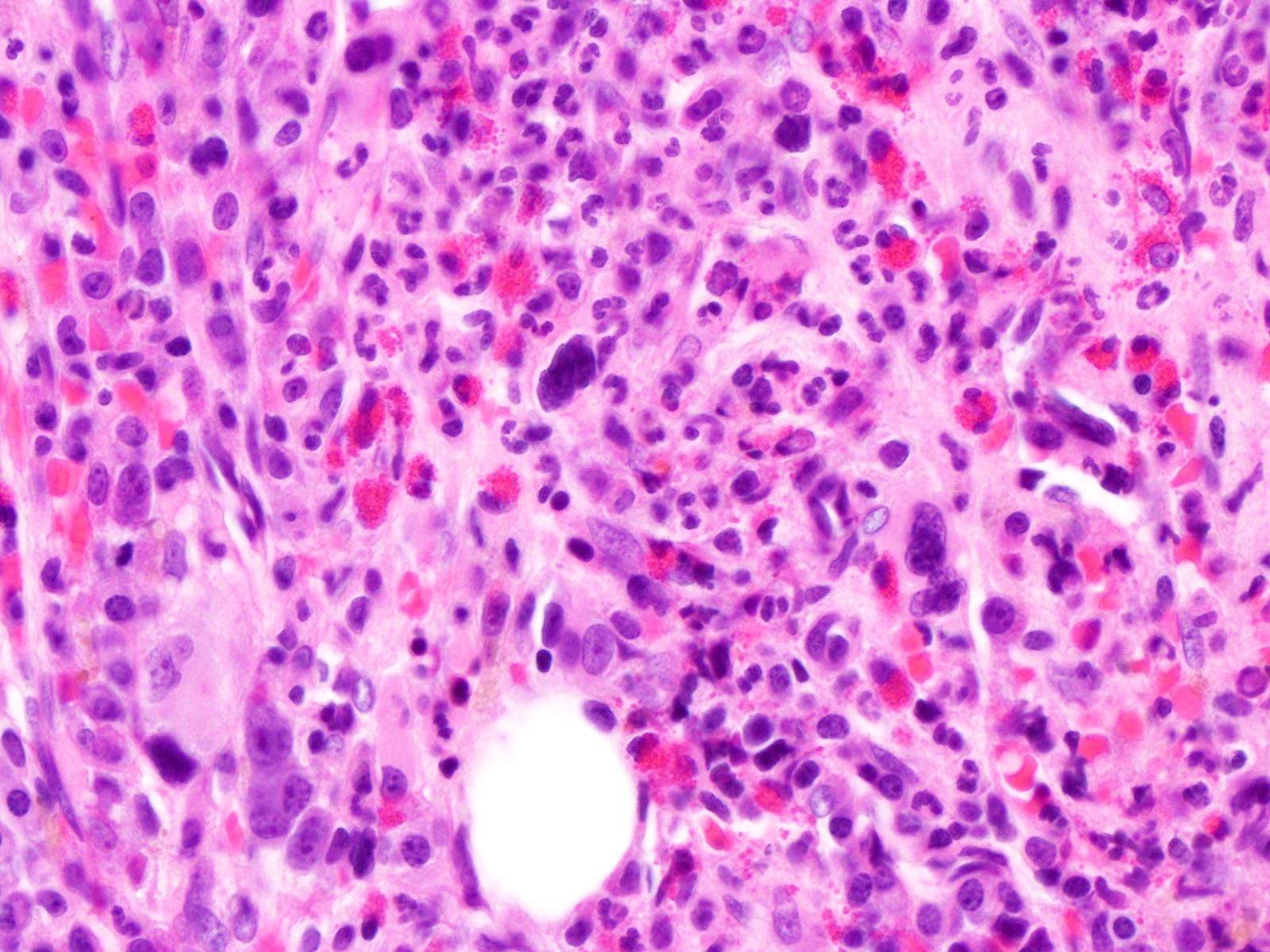
Hypercellular marrow
Megakaryocyte proliferation

Iron stain with ring sideroblast
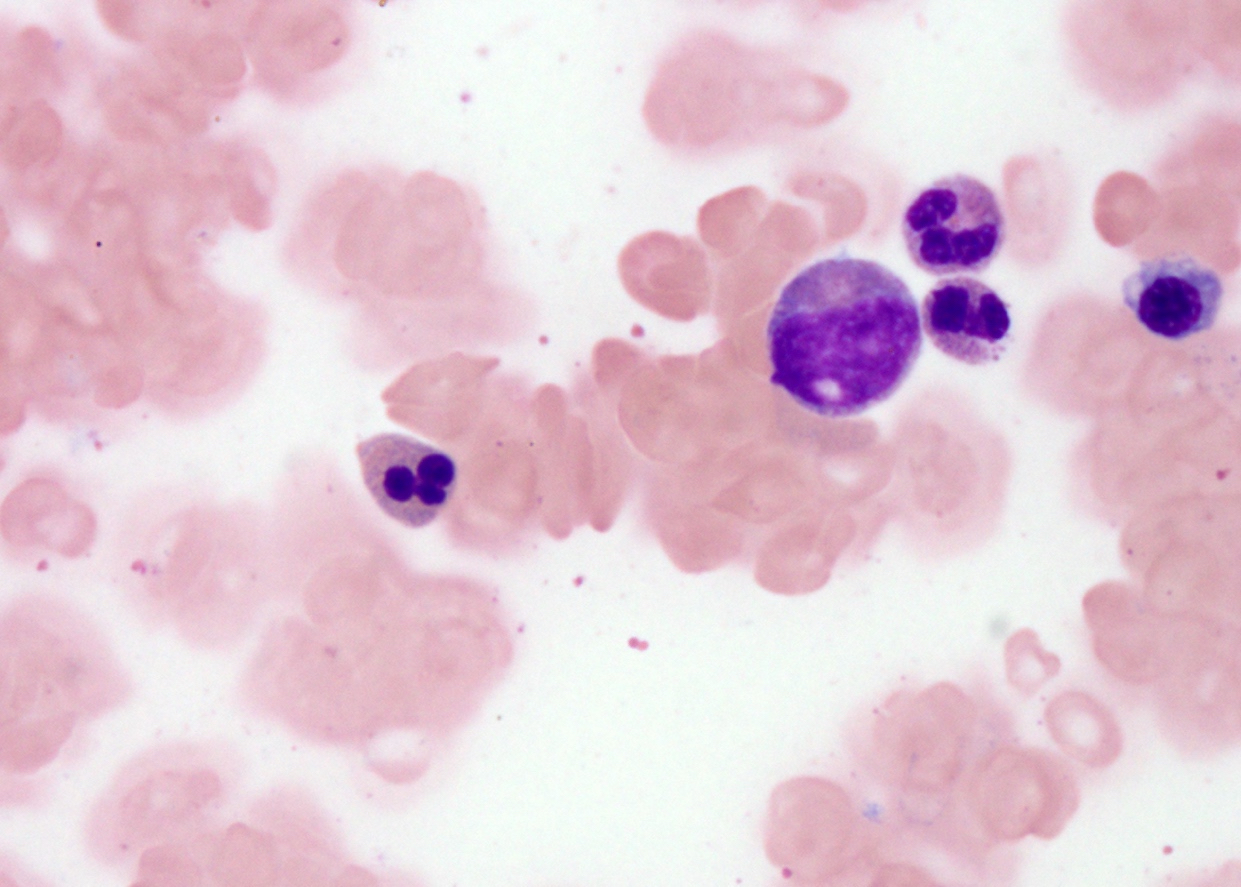

Dyserythropoiesis
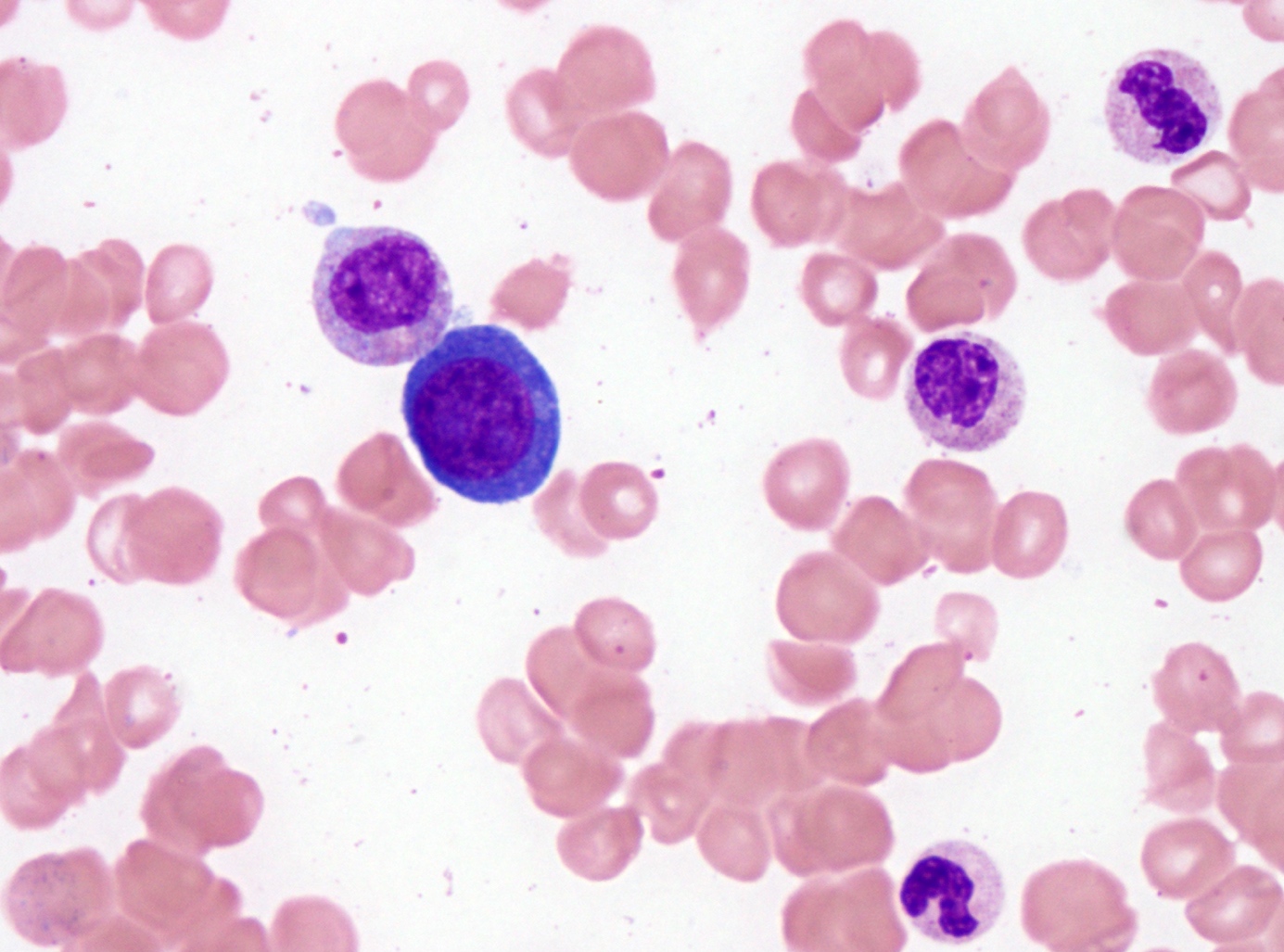
Normoblast with megaloblastic change
Peripheral smear description
- Normocytic to macrocytic, normochromic red blood cells
- Thrombocytosis, sometimes with large, giant or atypical platelets
- No or rare blasts, < 1% (Blood Cancer J 2018;8:15)
Peripheral smear images
Contributed by Patricia Tsang, M.D., M.B.A.
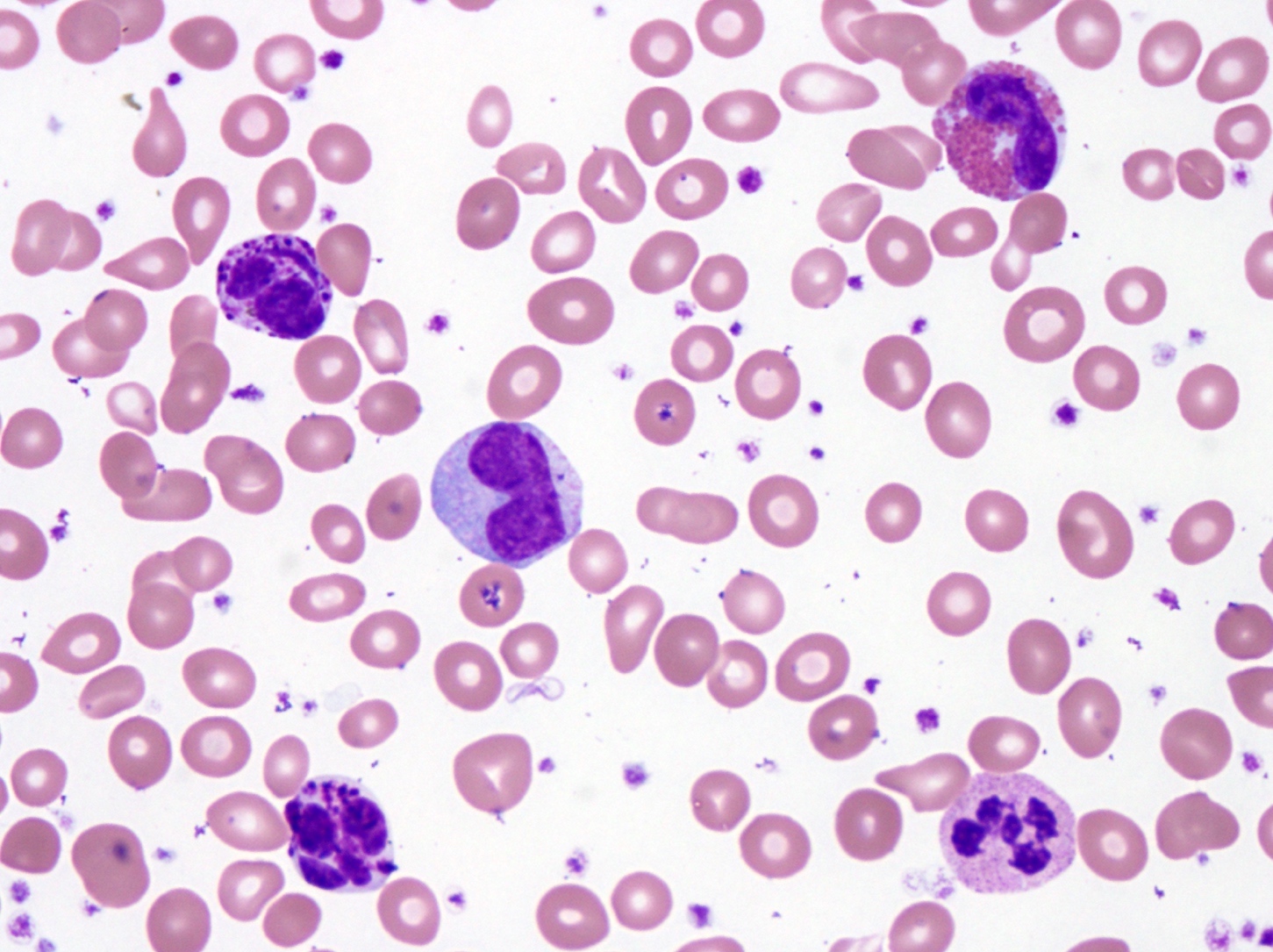
Thrombocytosis
Positive stains
- Iron stain on aspirate smear shows ring sideroblasts
- Immunostains generally not needed for diagnosis
Flow cytometry description
- No increase in blasts detected
- Aberrant CD56 on myeloid cells sometimes seen
Molecular / cytogenetics description
- SF3B1 mutation (60 - 90%), often in conjunction with JAK2 V617F mutation (> 60%), infrequently with MPL or CALR gene mutation (< 10%) (Am J Hematol 2018;93:E27, Am J Hematol 2016;91:492)
- ASXL1 (20%), DNMT3A (15%), SETBP1 (10%) and TET2 (25%) mutations (Am J Hematol 2017;92:297, Am J Hematol 2018;93:E27)
- Abnormal cytogenetics (~20%) (Am J Hematol 2018;93:E27)
Sample pathology report
- Bone marrow biopsy and aspirate smears, left posterior iliac crest:
- Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis, formerly refractory anemia with ring sideroblasts and thrombocytosis
- Cytogenetics, next generation sequencing for myeloid disorders, reticulin and trichrome stains are pending for further evaluation
- Peripheral blood smear:
- Macrocytic anemia with occasional teardrop RBCs
- Mild neutrophilia and marked thrombocytosis with some giant platelets
- Microscopic description:
- The peripheral blood smear shows leukocytosis with mild neutrophilia (8,400/mcL) and no circulating blasts. Anisopoikilocytosis with macrocytic RBCs and occasional teardrop cells are seen. Platelet count is elevated (610,000/mcL).
- The bone marrow aspirate (dry tap) is aspicular and hypocellular with evidence of maturing granulopoiesis and erythropoiesis. Some of the normoblasts show megaloblastic change and nuclear lobation, consistent with dyserythropoietic changes. The iron stain on aspirate reveals adequate storage iron. Ring sideroblasts constitute about 35% of the erythroid precursors.
- The bone marrow biopsy is hypercellular (about 80%) with trilineage hyperplasia. There is focal crush cell artifact, suggestive of marrow fibrosis. Myeloid:erythroid ratio appears unremarkable. No increase in myeloblasts is seen histologically. Proliferation of atypical megakaryocytes with cluster formation is present. Megakaryocytes are characteristically enlarged and hyperlobated. No abnormal lymphoid or plasma cell infiltrate is noted.
Differential diagnosis
- Myelodysplastic syndrome with ring sideroblasts (MDS-RS): lower platelet count, lacking myeloproliferative morphologic features, lacking JAK2 / CALR / MPL gene mutation
- Essential thrombocythemia: typically higher white blood cell count, higher hemoglobin levels, lacking ring sideroblasts, lacking dysplastic features, lacking SF3B1 mutation
- Myelodysplastic syndrome with isolated del(5q): unilobated or hypolobated megakaryocytes, del(5q) occurring singly or with one other cytogenetic abnormality, often del(7q) or monosomy 7
Additional references
Board review style question #1
Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis is most frequently associated with alterations of which pair of genes?
- ABL1 and CALR
- ASXL1 and KRAS
- SETBP1 and TP53
- SF3B1 and JAK2
- TET2 and FLT3
Board review style answer #1
D. SF3B1 and JAK2 are the two most frequently altered genes in myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis
Comment Here
Reference: Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis
Comment Here
Reference: Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis
Board review style question #2
Which of the following features is characteristic of myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis?
- Blasts < 1% in the blood and < 5% in the bone marrow
- Circulating ring sideroblasts > 15% in the peripheral blood
- Deletion 5q or monosomy 5
- Persistent monocytosis with no secondary etiology
- Proliferation of hypolobated megakaryocytes in the bone marrow
Board review style answer #2
A. Blasts < 1% in the blood and < 5% in the bone marrow. No increase in blasts is seen in the blood or bone marrow in myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis.
Comment Here
Reference: Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis
Comment Here
Reference: Myelodysplastic / myeloproliferative neoplasm with ring sideroblasts and thrombocytosis
