
Muscle & peripheral nerve nontumor
Inflammatory myopathies
Dermatomyositis
Last author update: 1 April 2016
Last staff update: 21 September 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Muscle dermatomyositis
See Also: Skin nontumor - Dermatomyositis



Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Clinical images | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Walsh M, Kresak J. Dermatomyositis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/muscledermatomyositis.html. Accessed April 2nd, 2025.
Definition / general
- Idiopathic process that leads to an inflammatory myopathy with skin manifestations
Essential features
- Myositis with perifascicular muscle fiber atrophy and generally inflammatory infiltrates around intramuscular vessels
- Clinical history can be supportive, with the classic skin finding being a heliotrope rash of the eyelids, face, neck and MCP joints
Terminology
- Dermatomyositis, DM
- Dermatomyositis sine myositis or amyopathic myositis: without muscle involvement
- Dermatomyositis sine dermatitis: either no skin findings or skin findings not noted in darker skin individuals:
Epidemiology
- There are two forms, adult and juvenile
- Adult dermatomyositis peaks ~ age 50; twice as common in women than men
- Juvenile dermatomyositis tends to occur between 5-10 years
- Dermatomyositis is the most common form of inflammatory myopathy in children (as opposed to polymyositis and inclusion body myositis)
Sites
- Symmetric weakness that affects the proximal limb muscles
- This weakness is progressive and occurs over weeks to months
- There are rare acute cases of weakness
- Patients describe difficulty rising from a seated position or chair, lifting objects or climbing stairs
- Distal weakness, in general, is not a presenting symptom
Pathophysiology
- The primary process is attack on the endothelium of the capillaries of myofibers, with deposition of complement on the vessel walls and eventual formation of membrane attack complex (N Engl J Med 1986;314:329)
- This causes perivascular inflammation and can eventually reduce the number of intramuscular small vessels
- This causes hypoxic change in the muscle, characterized by perifascicular atrophy, since these fibers are more distal to the vessels (N Engl J Med 1991;325:1487)
- In chronic disease, the number of capillaries can be significantly reduced in a biopsy
- There is up regulation of MHC-1 in myofibers and also increased expression of ICAM1 (N Engl J Med 1993;329:1993)
- No viral etiology has been associated with dermatomyositis
Etiology
- The exact etiology is idiopathic; however, juvenile dermatomyositis is associated with HLA DQA1 0501
- In adult forms, there is a 15% chance of an underlying malignancy (N Engl J Med 1992;326:363)
- There is also an association with other connective tissue diseases such as SLE, systemic sclerosis and mixed connective tissue disease (Yachnis: Neuropathology: A Volume in the High Yield Pathology Series, 2012)
Clinical features
- The classic symptoms are a rash followed by mild to severe myopathy
- Some cases have no rash or an unrecognized rash in darker skinned individuals (dermatomyositis sine dermatitis)
- Some cases lack muscle involvement (dermatomyositis sine myositis or amyopathic myositis)
- The skin rash is helicotrophic (violaceous, purple-blue) with edema over the upper eyelids; it can also involve the face, neck, anterior chest, back, shoulders, elbow and knees
- The rash is called the "V sign" when it occurs on the chest, and the "shawl sign" when it occurs on the back / shoulders (N Engl J Med 1991;325:1487)
- Classic findings also include Gottron's papules (elevated, purple rash on MCP joints), dilated capillaries at the base of the nails, skin calcinosis in chronic cases and a tiptoe gait from contractures in children when chronic (N Engl J Med 1991;325:1487)
- Occasionally patients have idiopathic interstitial lung disease (Clin Rheumatol 2007;26:1647)
Clinical images
Images hosted on other servers:

Heliotrope rash: the "classic" violaceous rash over the eyes and the malar region of the face

Gottron's papules: erythematous papules on the dorsum of MCP or interphalangeal joints; biopsy shows acanthosis and hyperkeratosis with vacuolar change and a scattered perivascular inflammatory infiltrate

Calcinosis: subcutaneous cases occur in long term, intractable cases, usually of juvenile type
Diagnosis
- A clinical-pathologic diagnosis
- Skin and muscle biopsies can be performed at the same time, although a clinical history of skin rash may override the need for a skin biopsy
- EMG/NCS [nerve conduction studies] findings may show increased membrane irritability (Up To Date)
Laboratory
- Elevated sedimentation rate, CK level (generally 5-50x normal, Yachnis: Neuropathology: A Volume in the High Yield Pathology Series, 2012), aldolase
- Antibodies may be found, but also associated with other connective tissue diseases
- ANA antibodies are more common in juvenile forms and anti-Jo antibodies are more common in adult forms
Radiology description
- MRI of musculature using T2 and STIR sequences can be helpful to establish a muscle group for biopsy (Rheumatology (Oxford) 2004;43:603, Arch Dermatol 1999;135:721)
Prognostic factors
- Response to therapy and presence of an underlying malignancy are useful factors
Case reports
- 24 year old woman with severe abdominal symptoms 3 months after diagnosis of dermatomyositis (Surgery 1998;123:356)
- 25 year old woman with spontaneous abortion after prednisone treatment for dermatomyositis (Scand J Rheumatol 1999;28:192)
- 32 year old man with osteosarcoma arising in heterotopic bone from dermatomyositis treated at age 3 (Cancer 1981;48:1256)
- 42 year old man with pneumomediastinum from interstitial lung disease with dermatomyositis (Clin Rheumatol 2001;20:359)
- 52 year old man with dermatomyositis and Lyme disease (Clin Infect Dis 1994;18:166)
- Patient with Lafora disease with phenytoin-induced dermatomyositis (J Child Neurol 1998;13:577)
Treatment
- Corticosteroids and other immunomodulators
- Rituximab for refractory cases (Reumatol Clin 2013;9:117)
- Newer therapies include high dose immunoglobulins (Int J Inflam 2016;2016:3523057)
Gross description
- The skeletal muscle gross findings are non-specific
Microscopic (histologic) description
- Perifascicular atrophy is the hallmark of dermatomyositis
- Muscle may have altered muscle fiber sizes, but there is less of a tendency to hypertrophy muscle fibers (more common in dystrophy)
- May be increased internal nuclei and basophilic myofibers
Microscopic (histologic) images
Contributed by Meggen Walsh, D.O., M.S., P.A. and Jesse L. Kresak, M.D.

Perifascicular atrophy
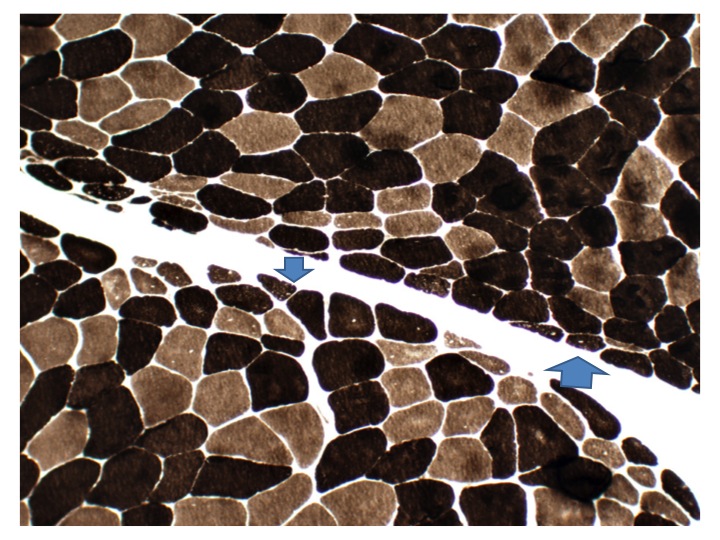
Perifascicular atrophy stain
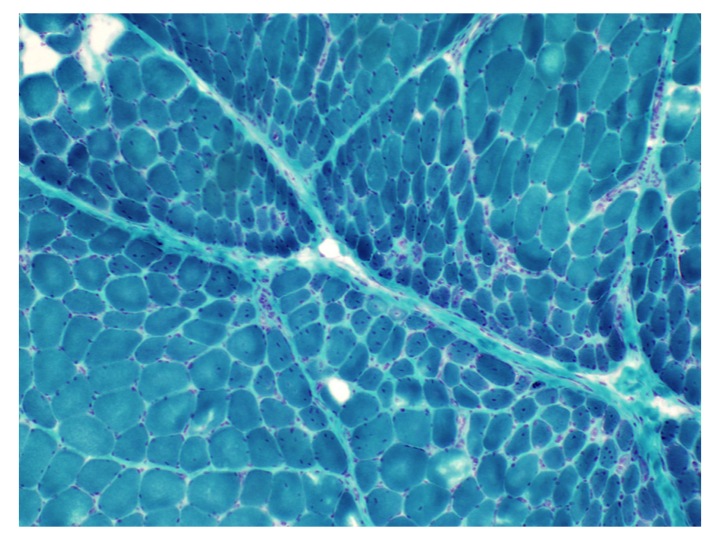
GMS


Myosin I/II immunostain
Cytology description
- Cytology is of no benefit since the main feature is atrophy in the perifascicular region
Positive stains
- Biopsy shows increased CD4+ T cells
- H&E cross sections are best to examine perifascicular atrophy
Negative stains
- Dystrophy panel is normal
- No loss of enzyme histochemical stains
Electron microscopy description
- Intramuscular vessels will occasionally show tubuloreticular inclusions
Differential diagnosis
- Myasthenia gravis: also causes muscle weakness, but has ophthalmologic muscular fatigue (DM does not)
- Polymyositis: Similar inflammatory myopathy, but no prominent perifascicular atrophy
Additional references
