
Muscle & peripheral nerve nontumor
Congenital myopathies
Central core disease
Authors: Wesley Hiser, M.D., Jesse L. Kresak, M.D.


Last author update: 1 September 2017
Last staff update: 12 August 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Central core disease

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Hiser W, Kresak JL. Central core disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/musclecentralcoredisease.html. Accessed April 3rd, 2025.
Definition / general
- First described in 1956 by Magee and Shy (Brain 1956;79:610)
- One of the more common forms of congenital myopathy
- Characterized by the presence of central cores in skeletal muscle histologically in addition to the clinical features of congenital myopathy
Essential features
- Skeletal muscle with areas of reduced to absent staining of enzymes such as NADH, SDH and COX
- Most commonly associated with mutation in RYR1 gene
- Presence of cores in a muscle biopsy without associated clinical symptoms and weakness is insufficient for diagnosis of central core disease
Terminology
- "Central core" refers to areas of reduced oxidative and glycolytic enzymatic activity along the longitudinal axis of skeletal muscle fibers, as seen on enzymatic stains such as NADH
ICD coding
- ICD-10: G71.2 - congenital myopathies
Epidemiology
- One of the more common congenital myopathies but true incidence is unknown
Sites
- Predominantly involves proximal musculature
- Most frequently hip girdle and axial muscles
Pathophysiology
- Two models of mutation induced receptor malfunction:
- Leaky channel hypothesis: depletion of sarcoplasmic reticulum calcium stores and increase in cytoplasmic calcium levels
- EC uncoupling hypothesis: disturbance of excitation contraction coupling (Yachnis: Neuropathology - A Volume in the High Yield Pathology, 1st Edition, 2014)
Etiology
- Typically caused by mutations in the skeletal muscle ryanodine receptor (RYR1)
- Less commonly caused by selenoprotein N (SEPN1) mutations (Semin Pediatr Neurol 2011;18:239)
Clinical features
- Variable presentation
- Static to slowly progressive disease course
- May worsen or progress during or after pregnancy
- Usually presents in infancy or early childhood
- Most common symptoms: myalgias, muscle stiffness, exertional weakness
- Common orthopedic symptoms include congenital hip dislocation, scoliosis and foot deformities (Neurology 2013;80:1584), but most patients can walk independently
- Extraocular, respiratory, cardiac muscle involvement is uncommon
- Precautions with general anesthesia due to risk of malignant hyperthermia (associated with RYR1 mutation)
Diagnosis
- Histologic finding of central cores in skeletal muscle combined with clinical features of congenital myopathy
- Presence of cores in a muscle biopsy without associated clinical symptoms and weakness is insufficient for diagnosis of central core disease
Laboratory
- CK levels are typically within normal range but may be elevated
Radiology description
- Ultrasound shows localized increased echogenicity within quadriceps
- MRI shows pattern of selective muscle involvement with predilection for vasti muscles, sartorius and adductor magnus of thigh, as well as soleus and peroneal group of lower leg
- Relative sparing of gracilis, adductor longus and rectus femoris (Neurology 2013;80:1584)
Prognostic factors
- Autosomal dominant mutations are typically associated with a favorable prognosis
- Autosomal recessive mutations may be associated with more severe complications
Case reports
- Infant boy presenting with motor delay and muscle weakness (Eur J Paediatr Neurol 2011;15:70)
- Infant girl with bilateral congenital lumbar hernias, multiple joint contractures, decreased muscle bulk and symptoms of malignant hyperthermia (Neuromuscul Disord 2016;26:56)
Treatment
- No current treatment
- Supportive care
Microscopic (histologic) description
- Large areas of reduced oxidative and glycolytic enzymatic activity along longitudinal axis of muscle fiber
- Fibers may have multiple cores; cores may be central or eccentrically placed
- Usually involves type 1 fibers, with some degree of hypertrophy or predominance
- Internal nuclei may be seen
- Myofiber necrosis and regeneration are not seen (Yachnis: Neuropathology - A Volume in the High Yield Pathology, 1st Edition, 2014)
Microscopic (histologic) images
Contributed by Jesse L. Kresak, M.D.
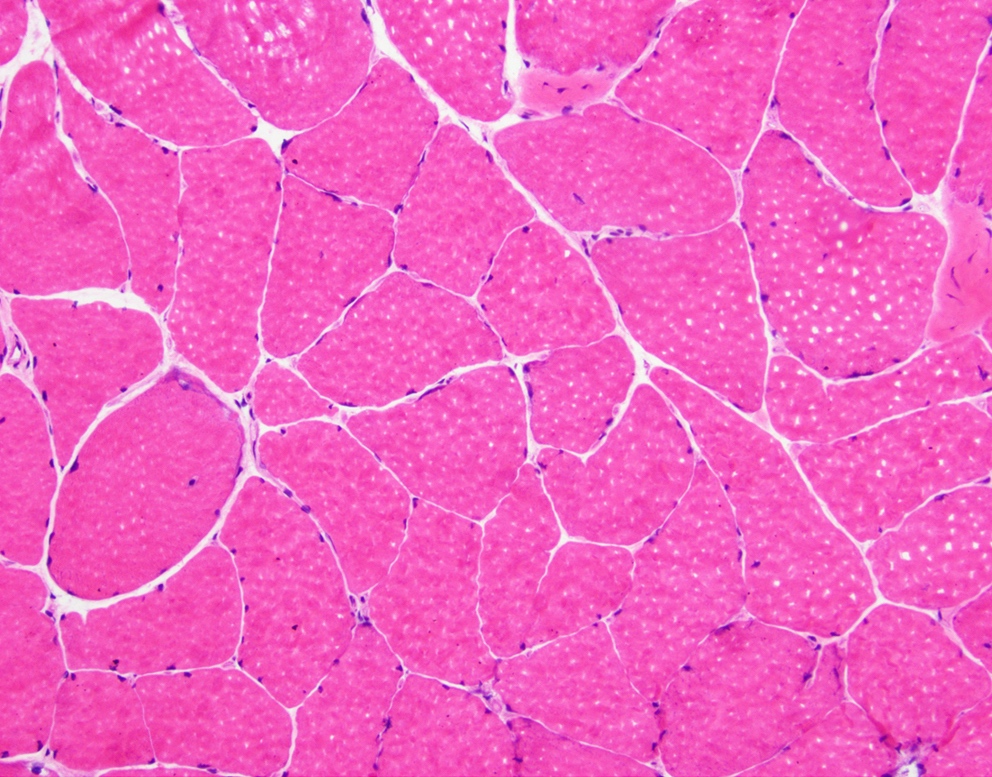
H&E

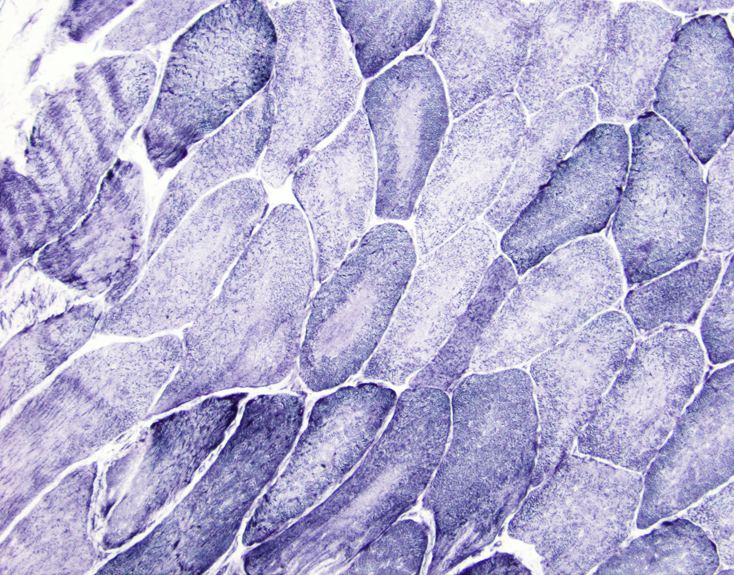
NADH and NADH1
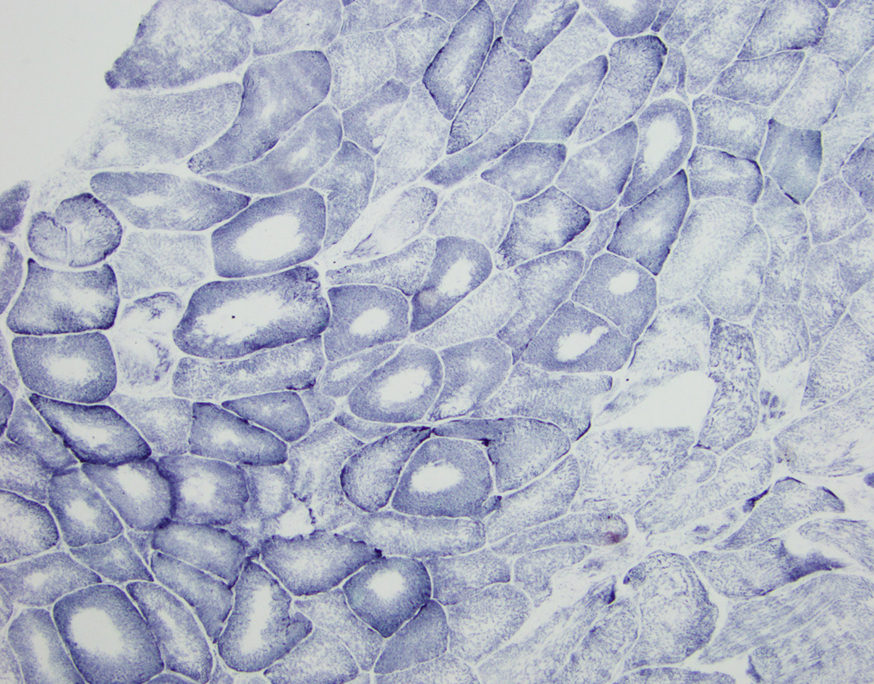
SDH
Positive stains
- Desmin positivity in region of core
- May display nemaline rods with Gömöri trichrome (core rod myopathy)
Negative stains
- NADH stain shows absence of enzyme activity within the cores
- SDH and COX stains may also show absence of enzyme activity within cores
Electron microscopy description
- Reduced or absent mitochondria within cores
- Two types of cores: structured and unstructured
- Structured: preserved myofibrillar architecture and retained ATPase activity
- Unstructured: severe myofibrillar disruption with accumulation of smeared Z line material and absent ATPase activity (Yachnis: Neuropathology - A Volume in the High Yield Pathology, 1st Edition, 2014)
Molecular / cytogenetics description
- Most commonly caused by autosomal dominant mutations in RYR1 gene on chromosome 19q13.1
- Less commonly caused by selenoprotein N (SEPN1) gene mutations (Semin Pediatr Neurol 2011;18:239)
- RYR1 encodes ryanodine receptor, which is ligand gated release channel for calcium stored in terminal cisterna
- RYR1 gene is also implicated in malignant hyperthermia sensitivity (MHS) phenotype
- Dominant mutations affecting N terminal or central domains of RYR protein give rise to MHS phenotype, while those affecting C terminal give rise to central core disease phenotype
- Recessive mutations are uncommon and typically present as multiminicore disease on histology (Yachnis: Neuropathology - A Volume in the High Yield Pathology, 1st Edition, 2014)
Differential diagnosis
- Cores are nonspecific and can be seen in a number of other conditions:
- Denervation – often with "targetoid" fibers
- Following exercise in healthy individuals
- Associated with other gene defects (ACTA1, MYH7) and congenital myopathy (Yachnis: Neuropathology - A Volume in the High Yield Pathology, 1st Edition, 2014)
- Metabolic conditions
- Tenotomy: surgical act which involves the division of a tendon
Additional references
Board review style question #1
The term "central core" refers to which of the following:
- Areas of increased oxidative and glycolytic enzymatic activity along the longitudinal axis of skeletal muscle fibers, as seen on enzymatic stains such as NADH
- Areas of reduced oxidative and glycolytic enzymatic activity along the longitudinal axis of skeletal muscle fibers, as seen on enzymatic stains such as NADH
- Centrally located accumulation of red to purple, rod-like inclusions within skeletal muscle fibers, visible with Gömöri trichrome stain
- Centrally placed, rimmed vacuole within skeletal muscle fibers, visible with Gömöri trichrome stain
Board review style answer #1
B. Areas of reduced oxidative and glycolytic enzymatic activity along the longitudinal axis of skeletal muscle fibers, as seen on enzymatic stains such as NADH
Comment Here
Reference: Central core disease
Comment Here
Reference: Central core disease
