

Appendix
Appendicitis
Enterobius vermicularis
Author: Eiman Adel Hasby Saad, M.D.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 27 April 2021
Last staff update: 15 October 2021
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Enterobius vermicularis [TIAB] appendix

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Hasby Saad EA. Enterobius vermicularis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixenterobius.html. Accessed December 26th, 2024.
Definition / general
- Nematode infection caused by human pinworm Enterobius vermicularis
Essential features
- Enterobiasis is one of the most common worm diseases in humans, occurring predominantly in children via fecal - oral transmission and also by inhalation of dust containing eggs
- Pruritis ani is the main symptom; also can present with intestinal or less commonly extraintestinal manifestations
- Affection of appendix varies from asymptomatic to various inflammatory patterns
- Diagnosis is by detection of adult worms or eggs clinically or microscopically
Terminology
- Synonyms include threadworm and seatworm
- Symptomatic pinworm infection is referred to as enterobiasis (older term: oxyuriasis) (Acta Vet Hung 2013;61:147)
Epidemiology
- More common in children and adolescents; F > M (5 - 14 year age group) but overall M:F = 2:1
- Highest prevalence in Africa, especially Nigeria
- More common in countries with lower levels of income and lower Human Development Index (HDI) (PLoS One 2020;15:e0232143)
Sites
- Worms live and reproduce in the ileum, cecum, colon and appendix
- Nematode female migrates to the anus to deposit its eggs and die, usually at nighttime
- Extraintestinal presentation is very rare (J Clin Microbiol 2011;49:4369)
- Most common extraintestinal site is the female reproductive tract (vagina, uterus, ovaries and fallopian tubes) due to migration of the female worm from the anus
- Female worm can also enter the urinary tract, kidneys, biliary tract and liver
- Isolated case reports of infection involving the salivary glands, nasal mucosa, skin and lungs, presumably due to autoinoculation of these sites with eggs or adult worms from the intestinal tract
Pathophysiology
- Following ingestion, the embryonated eggs hatch in the small intestine and develop into adult worms that reside in the cecum, appendix, colon and rectum
- Male and female worms mate in the human intestinal tract and the gravid female worm migrates to the anus to lay partially embryonated eggs on the perianal and perineal surfaces
- Migration of the female worm to the anus causes pruritus, which is the most common symptom of pinworm infection
- See diagram
- Reference: J Clin Microbiol 2011;49:4369
Etiology
- Caused by ingestion and inhalation of the worm oocysts / eggs (fecal - oral route and autoinfection)
- Strictly human - pathogenic parasite

Clinical features
- Most patients are asymptomatic
- In symptomatic patients, the most common complaint is perianal pruritus, usually nocturnal or in the early morning
- Other complaints include abdominal pain, irritability and restlessness
- Heavy infection in children may cause anorexia, behavioral changes (sleep disturbance, nausea, nail biting, grinding teeth at night)
- Also has been reported to present with manifestations of urinary tract infection, salpingitis, eosinophilic ileocolitis and pelvic abscess
- In the case of appendicitis, release and accumulation of eggs from female Enterobius vermicularis may lead to the obstruction and inflammation of the appendix (PLoS One 2020;15:e0232143)
- People infected with pinworm can transfer the parasite to others for as long as there is a female pinworm depositing eggs on the perianal skin
- A person can also reinfect themselves or be reinfected by eggs from another person
- Good personal hygiene: washing hands with soap and warm water after using the toilet and changing diapers and before handling food is the most successful way to prevent pinworm infection
- Reference: Centers for Disease Control and Prevention: Enterobiasis - Prevention & Control [Accessed 8 March 2021]
Diagnosis
- While diagnosis may be made by histology, it can also be made clinically:
- Look for the worms in the perianal region 2 - 3 hours after the infected person is asleep
- Touch the perianal skin with cellophane tape to collect possible pinworm eggs around the anus first thing in the morning
- This should be conducted on 3 consecutive mornings right after the infected person wakes up and before he / she does any washing
- If a person is infected, the eggs on the tape will be visible under a microscope
- Analyze samples from beneath fingernails of infected person under a microscope; if patient has scratched the anal area, they may have picked up some pinworm eggs under the nails (CDC: Parasites - Enterobiasis - Diagnosis [Accessed 23 February 2021])
- In case of severe infestation, worms may be visibly expelled with the stool
- Occasionally, individual adult worms are visualized on proctoscopy or colonoscopy
Laboratory
- Best diagnosed by microscope detection of adult worms or microscopic detection of eggs on the perineum (Dtsch Arztebl Int 2019;116:213)
- Microscopic demonstration of characteristic eggs in the perianal scrapings is the method of choice for the diagnosis of enterobiasis
- Anal or perianal specimens can be collected by National Institutes of Health (NIH) swab, cellophane swab or cellophane tape
- Since anal itching is a common symptom of pinworm, the third option for diagnosis is analyzing samples from beneath fingernails under microscope
- Pinworm eggs and worms are often sparse in stool; examining stool samples is not recommended
- Serologic tests are not available for diagnosing pinworm infections
Case reports
- 18 year old woman with lower abdominal pain (BMJ Case Rep 2015;2015:bcr2015210464)
- 21 year old Arabic man admitted at emergency department after 2 days of abdominal pain and nausea (BMC Res Notes 2017;10:494)
- 23 year old woman presented to emergency department after 8 hours of right lower abdominal pain with concomitant anorexia, nausea and vomiting (Int J Surg Case Rep 2019;63:153)
- 35 year old woman with a 96 hour history of constant right iliac fossa pain on movement and coughing (BMJ Case Rep 2014;2014:bcr2013202962)
- 40 year old woman with white vaginal discharge for past year (J Nat Sci Biol Med 2015;6:476)
Treatment
- Either mebendazole, pyrantel pamoate or albendazole
- Any of them given in 1 dose initially, then another dose of the same drug 2 weeks later
- Pyrantel pamoate is available without prescription but medication does not reliably kill pinworm eggs, therefore, the second dose is to prevent reinfection by adult worms that hatch from any eggs not killed by the first treatment
- Health practitioners and parents should weigh the health risks and benefits of these drugs for patients under 2 years of age and in pregnant and lactating women
- Repeated infections should be treated by the same method as the first infection
- When multiple members in the same house or institution are infected, simultaneous treatment to all household members or mass treatment to all institution members is recommended and to be repeated after 2 weeks to be effective (CDC: Parasites - Enterobiasis - Treatment [Accessed 25 February 2021])
Clinical images
Images hosted on other servers:

Intraoperative pinworm

Enterobius vermicularis through appendix
Gross description
- If inflamed, appendix shows congested wall, opaque serosal covering with serofibrinous exudate, lumen can be filled by stercolith
- Some authors have reported macroscopically visible parasites (BMC Res Notes 2017;10:494)
- Female worms are 9 - 12 mm long with a diameter of approximately 0.5 mm, while the males are shorter (3 - 5 mm) but visible to the naked eye
- Striking whitish beige in color; they are typically round in shape and move with a vigorous crawling motion
Gross images
Images hosted on other servers:

Inflamed appendix with stercolith

With retrieved worm

Enterobius vermicularis through appendix
Microscopic (histologic) description
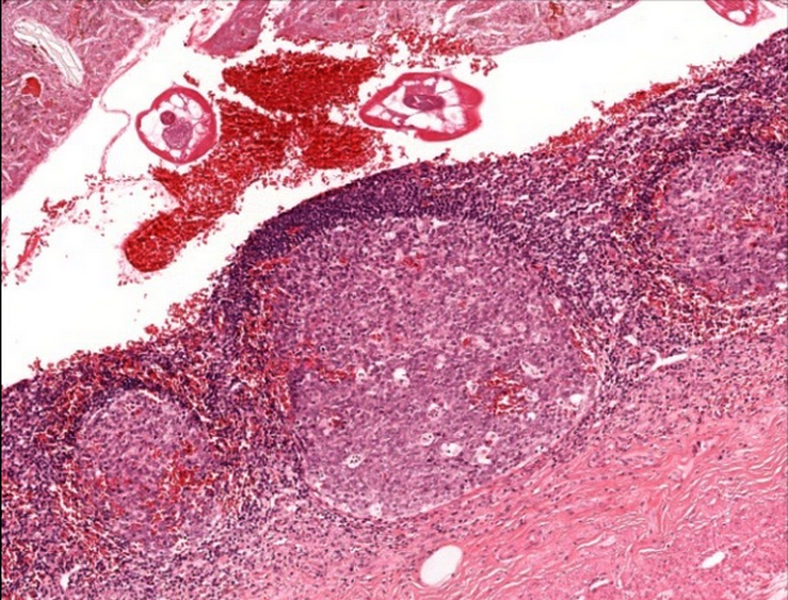
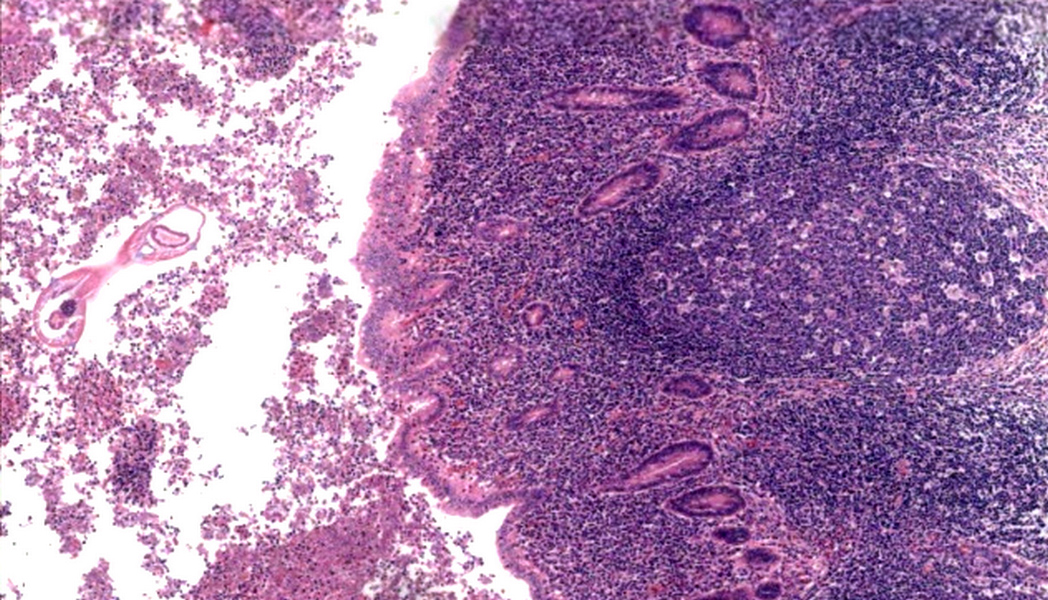
- Appendix can range from normal to various inflammatory patterns, such as mucosal ulceration, suppuration, lymphoid hyperplasia, eosinophilic infiltrate or neutrophilic infiltrate and plasma cells (Diagn Pathol 2007;2:16, Infect Dis Clin North Am 2010;24:995, BMJ Case Rep 2015;2015:bcr2015210464)
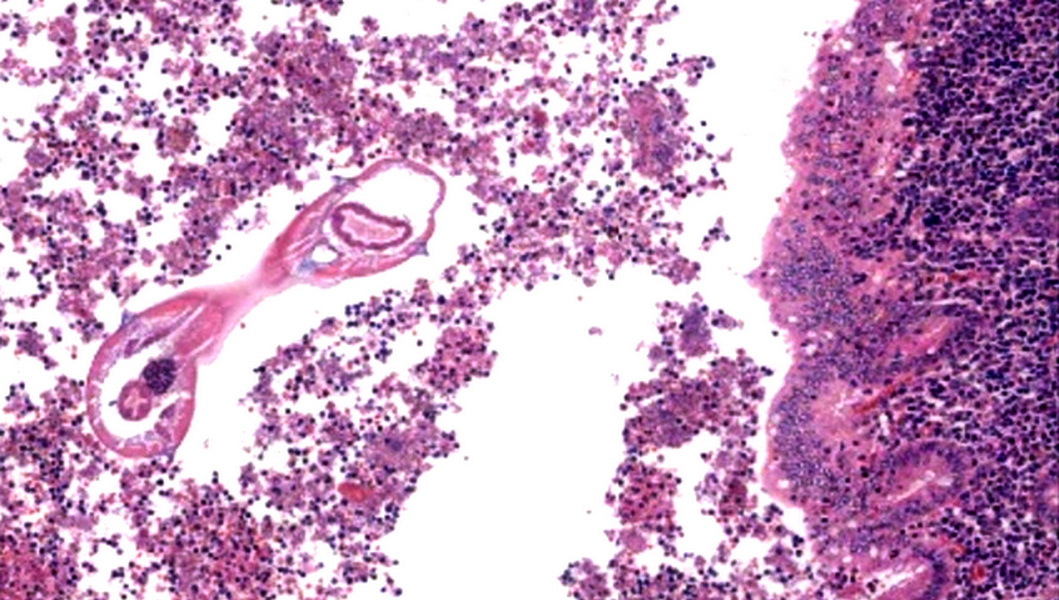
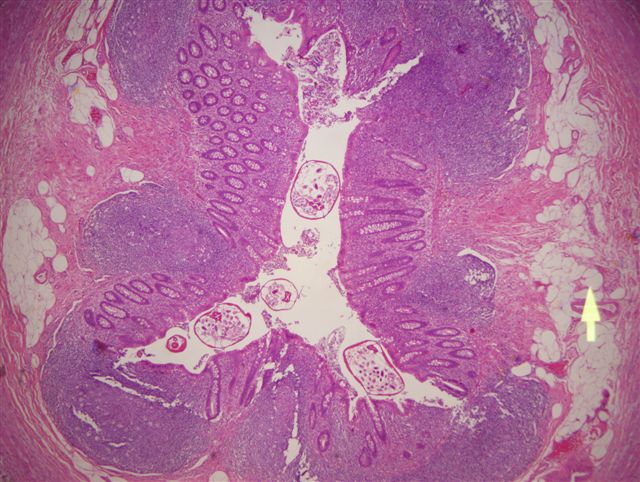
- Worms mostly seen in lumen
- Occasionally, erratic migration of eggs and larvae can elicit granuloma formation
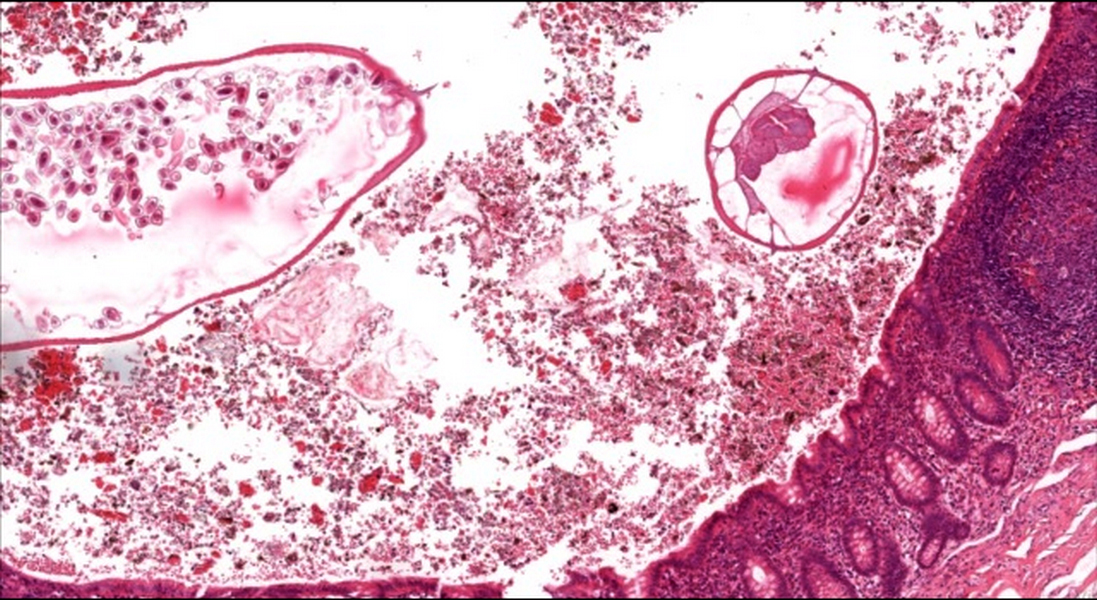
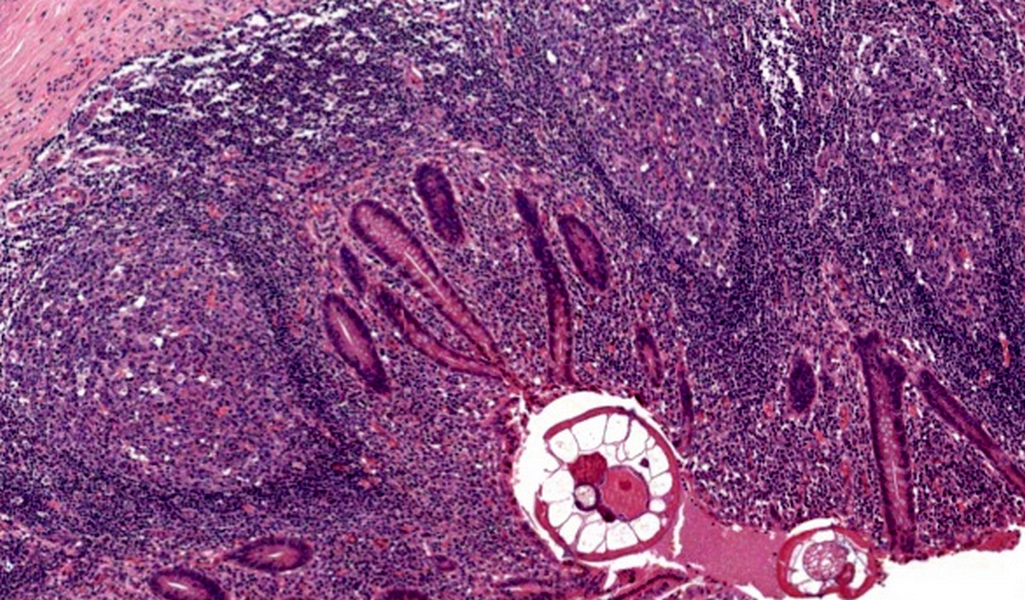
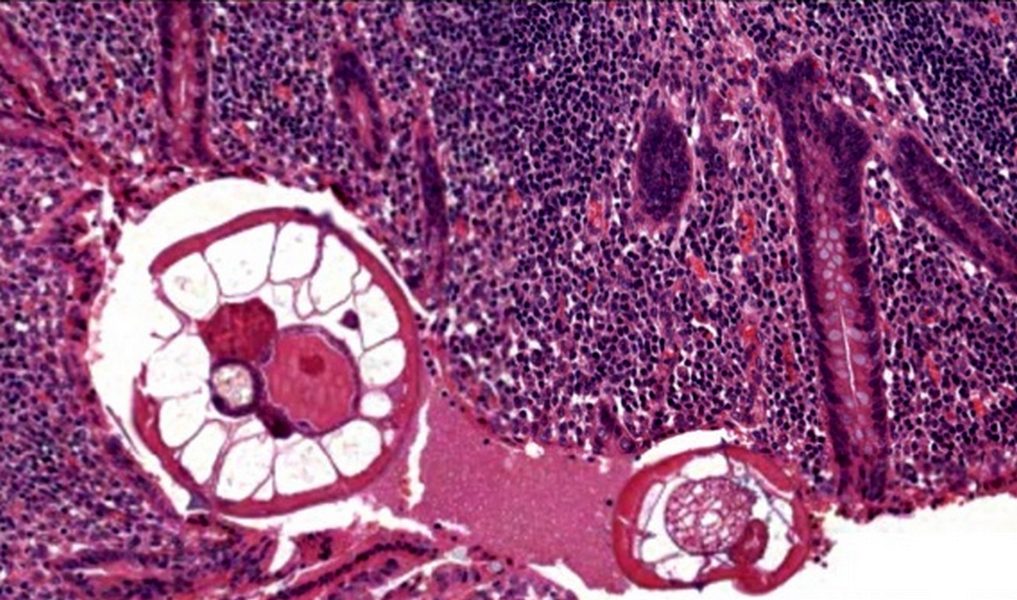
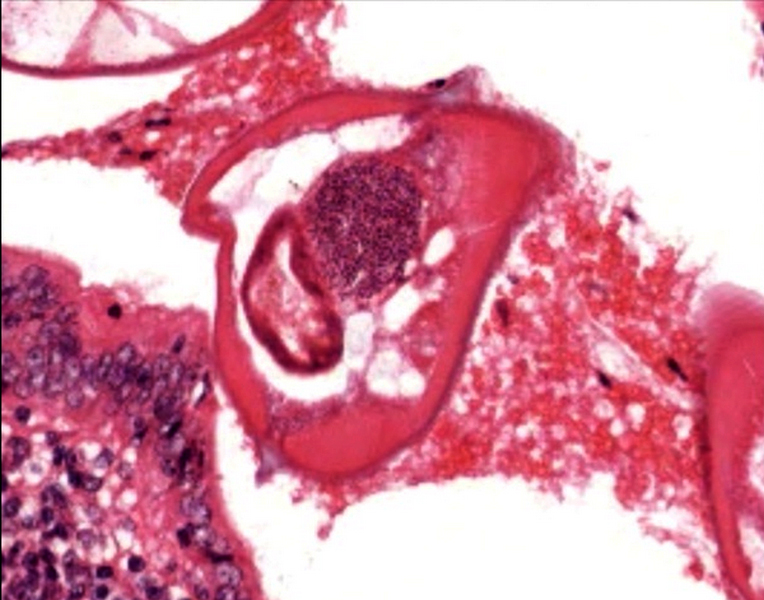
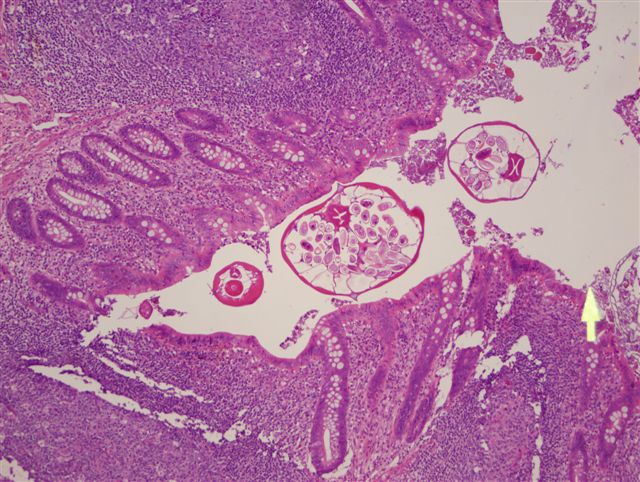
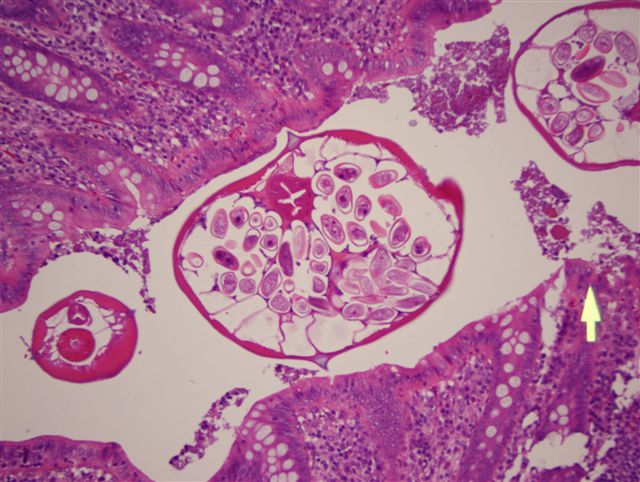
- On cross section, adult worms have a thick cuticle, lateral alae (wings) and visible organs, which may include intestines and ovaries / testes
- Head section is rounded and contains a muscular esophagus and bulb; in females, the tail section is narrow and sharply tapered and the extensive uterine reproductive system of the fertilized female worm is often completely filled with eggs (> 10,000/worm)
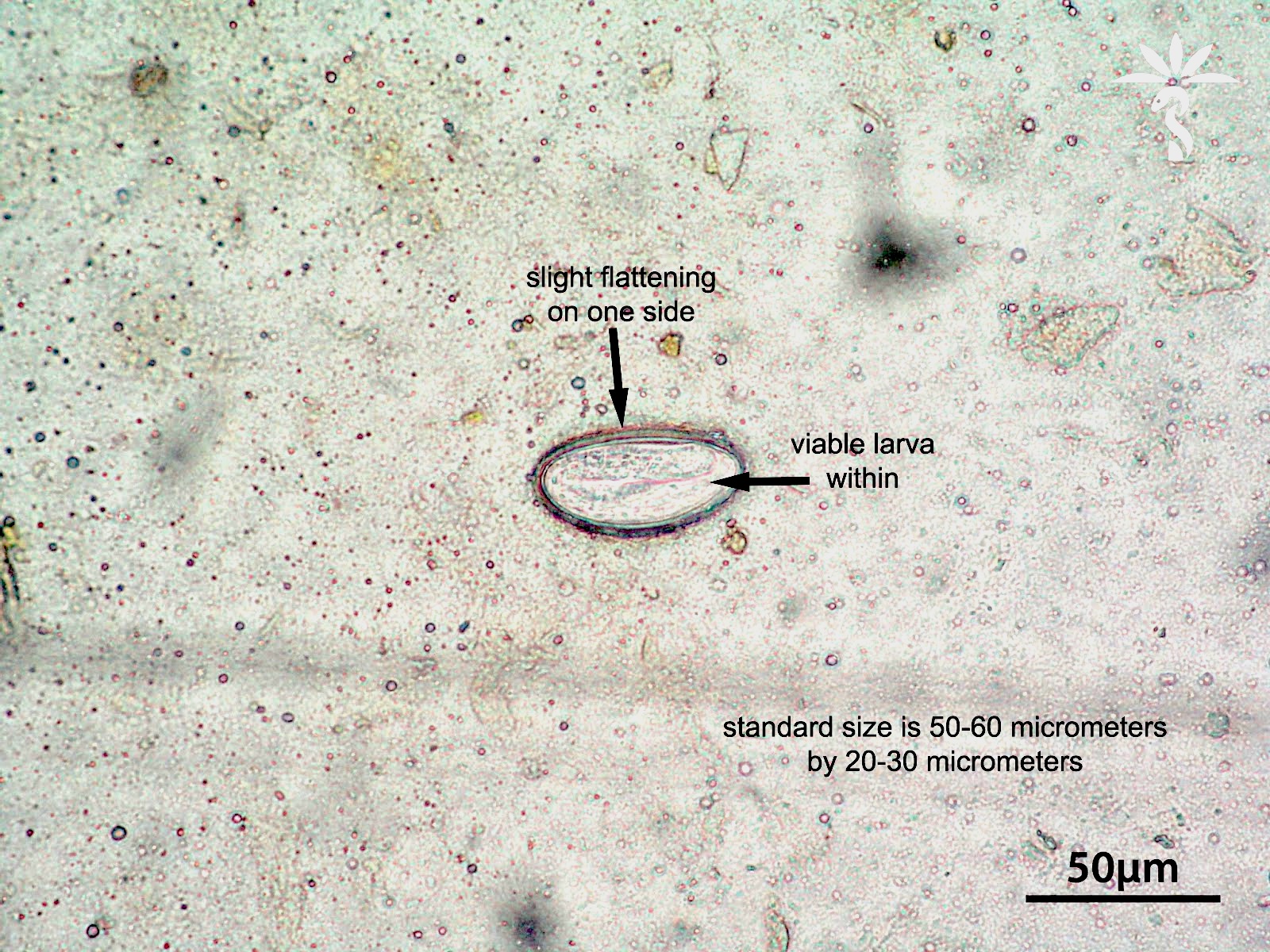
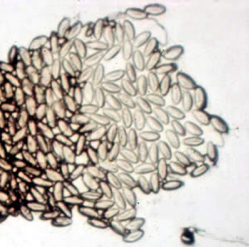
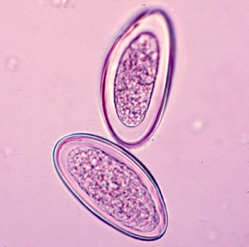
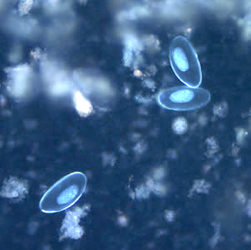
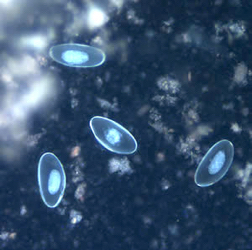
- Eggs are colorless, measuring 50 - 60 μm in length and 20 - 32 μm in breadth
- Typically plane convex, with 1 flattened side and 1 convex side
- They are surrounded by a thin, hyaline, transparent shell composed of 2 layers of chitin
- Egg contains a coiled tadpole-like larva and floats in saturated salt solution (Dtsch Arztebl Int 2019;116:213)
Microscopic (histologic) images
Contributed by Eiman Adel Hasby, M.D. and Case #90
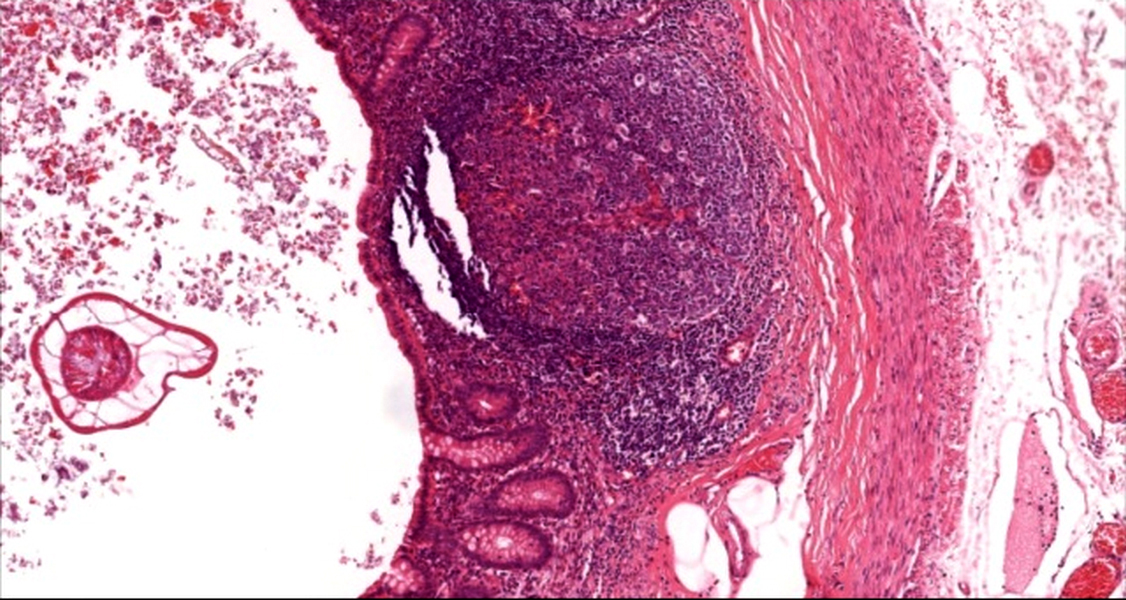
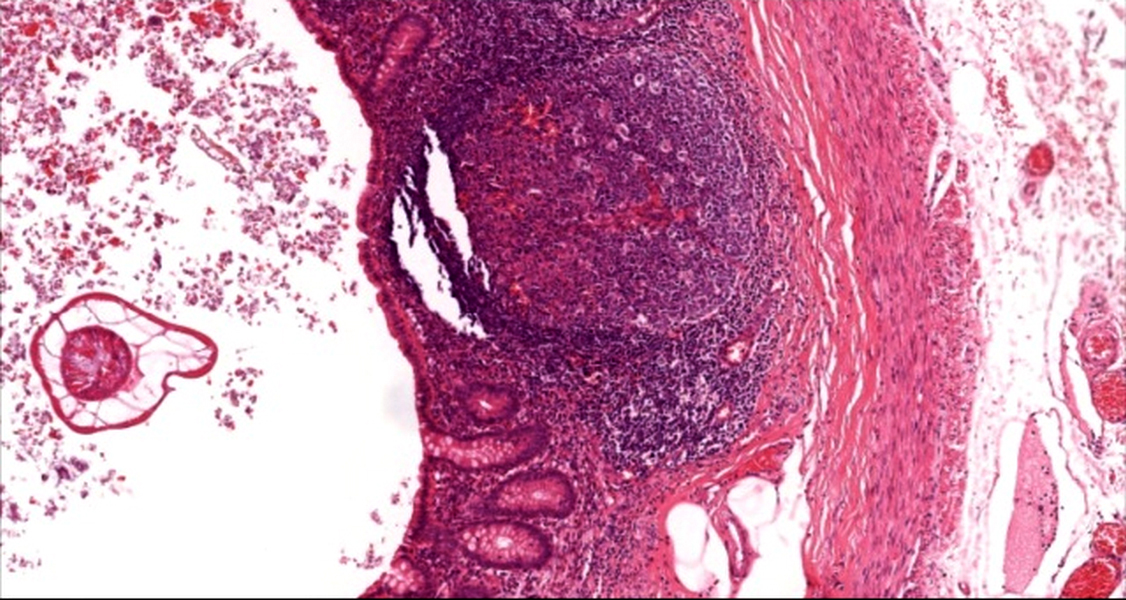
Appendix with luminal Enterobius
Enterobius in acute appenicitis
Appendicitis with luminal Enterobius
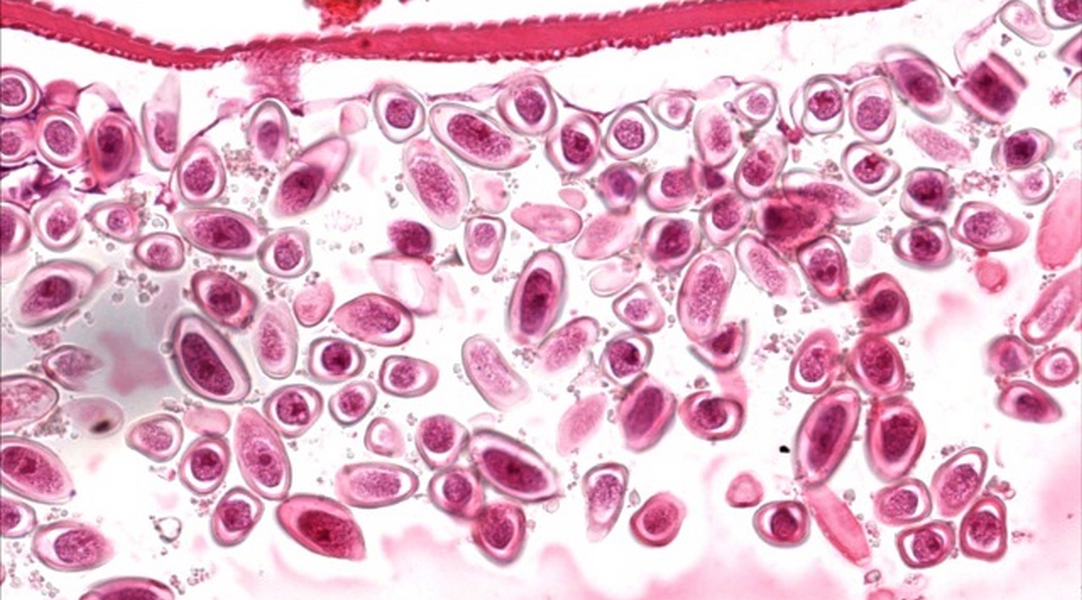
Enterobius eggs
Appendicitis with enterobiasis
Appendicitis with enterobiasis
Male Enterobius adult worm

Female Enterobius adult worm
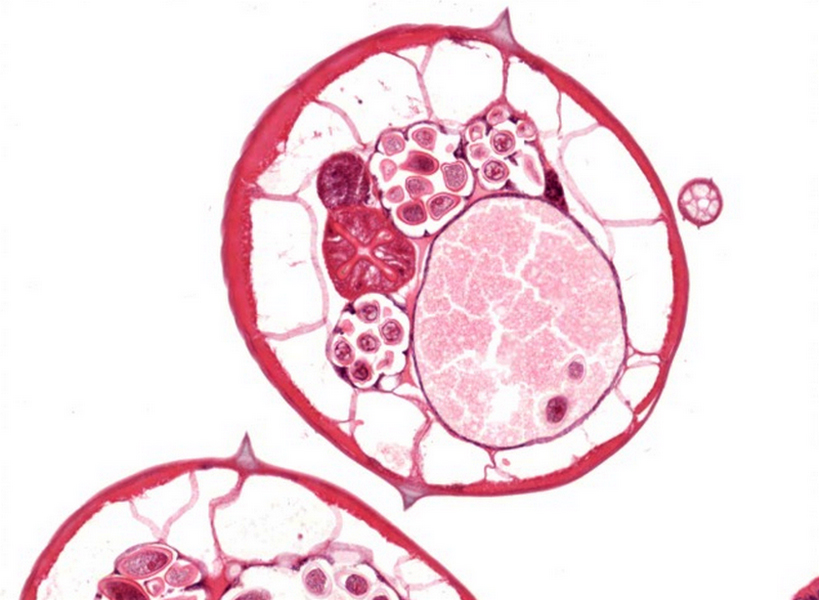
Gravid female Enterobius worm
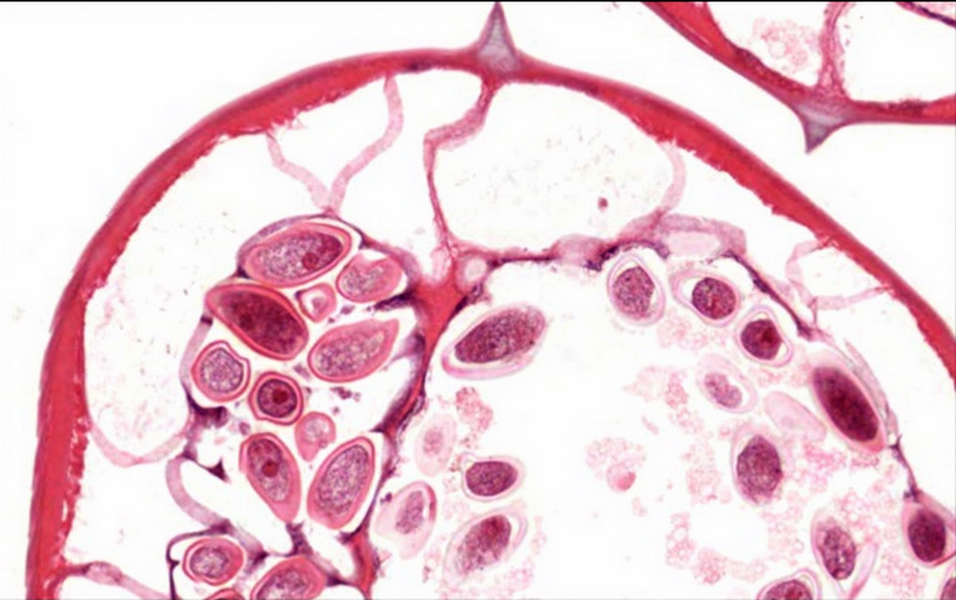
Enterobius eggs
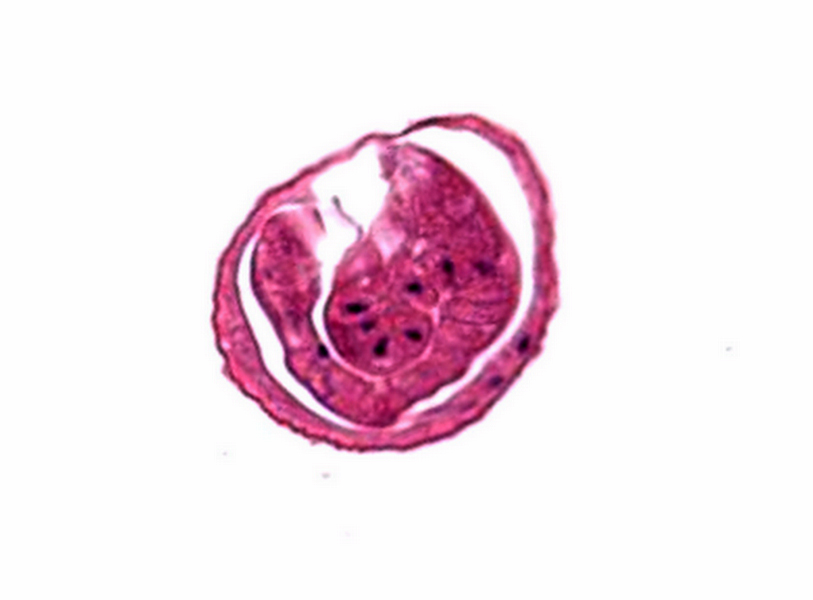
Enterobius egg with larva
Eggs
Virtual slides
Images hosted on other servers:


Appendix, Enterobius vermicularis

PASD, no cuticle staining
Cytology images
Contributed by Bobbi Pritt, M.D. and Chamarajan Shrinivasan, M.D.

Wet mount from stool sample



Ova and larva of Enterobius vermicularis
Contributed by Centers for Disease Control and Prevention
Eggs
Sample pathology report
- Appendix, excision:
- Acute appendicitis with Enterobiasis vermicularis (see comment)
- Comment: There is an inflamed appendix showing congested blood vessels in its wall, hyperplastic lymphoid follicles of variable sizes with prominent mantle zones and reactive germinal centers and a diffuse inflammatory infiltrate formed of lymphoplasmacytic cells, together with neutrophils and eosinophils. There is also focal surface ulceration. Appendicular lumen shows inspissated mucous with fecal matter within which cross sections of Enterobius vermicularis adult worms show an outer eosinophilic cuticle with lateral alae, worm gut and uterus filled with eggs inside.
Differential diagnosis
- On microscopic examination, the worm and eggs should be differentiated from:
- Whipworm (Trichuris trichiura):
- Worms are longer, embedded in surface mucosa by one end, its eggs have polar plugs
- Vegetable material:
- Enterobius vermicularis has cuticle, eggs are distinctly compressed laterally and flattened on one side
- Whipworm (Trichuris trichiura):
Board review style question #1
A 14 year old girl complaining of perianal itching especially at night for 2 weeks came to the emergency department complaining of abdominal pain and underwent appendectomy. On pathologic examination of the resected appendix, structures shown in the micro image were detected in the appendicular lumen. What is the most likely diagnosis?
- Appendicitis with Enterobius vermicularis infestation
- Appendicitis with whipworm infestation
- Crohn's disease
- Granulomatous appendicitis
Board review style answer #1
A. Appendicitis with Enterobius vermicularis infestation
Comment Here
Reference: Enterobius vermicularis
Comment Here
Reference: Enterobius vermicularis
Board review style question #2
What is most likely to be helpful for the diagnosis of enterobiasis?
- Breath test
- Cellophane tape test
- Serological tests
- Stool examination
Board review style answer #2

