

Small intestine & ampulla
Infectious disorders
Infectious disorders-general
Author: Hanni Gulwani, M.B.B.S.

Last author update: 1 August 2012
Last staff update: 20 September 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Infectious disorders small bowel

Table of Contents
Anisakis | Bacterial enterocolitis | Cryptosporidium | Cyclospora (pending) | Entamoeba histolytica | Giardia lamblia | Isospora belli | Microsporidia | Rotavirus | Salmonella | Strongyloides stercoralis | Vibrio cholerae (pending) | Whipple disease | Board review style question #1 | Board review style answer #1Cite this page: Gulwani H. Infectious disorders-general. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/smallbowelinfectiousdisordersgen.html. Accessed December 26th, 2024.
Anisakis
Definition / general
Diagrams / tables
Images hosted on other servers:

Case reports
Clinical images
Images hosted on other servers:



Gross images
Contributed by Bobbi Pritt, M.D.
Microscopic (histologic) description
Microscopic (histologic) description
Contributed by Bobbi Pritt, M.D.

Images hosted on other servers:


Additional references
- Larvae of ascarids (Anisakidae) are found in sea animals
- After ingesting contaminated raw fish or other sea food, larvae attach to mucosa of stomach or small intestine and cause ulceration, penetration or perforation
Diagrams / tables
Images hosted on other servers:

Life cycle
Case reports
- 37 year old woman with epigastric pain two hours after ingesting fried hake and fish ova and 200 larvae obtained by endoscopy (J Investig Allergol Clin Immunol 2010;20:437)
- 50 year old man with abdominal pain and peripheral eosinophilia after eating raw salmon from Pacific Ocean (Am J Surg Pathol 2003;27:1167)
- Worm found in fresh salmon (Pritt: Creepy Dreadful Wonderful Parasites Blog - Case of the Week 557 [Accessed 7 September 2023])
Clinical images
Images hosted on other servers:
Larvae in terminal ileum
Larvae in fish

Larvae in a herring
Gross images
Contributed by Bobbi Pritt, M.D.
Most likely a
type I Anisakis or
Pseudoterranova
Microscopic (histologic) description
- Serositis, mucosal edema, submucosal abscess with eosinophils surrounding parasite with unpaired excretory gland (renette cell), Y shaped lateral epidermal cords, no apparent reproductive system and a ventriculus (glandular esophagus)
- No lateral alae, no ventricular appendage, no intestinal cecum
Microscopic (histologic) description
Contributed by Bobbi Pritt, M.D.
Most likely a type I Anisakis or Pseudoterranova: anterior boring tooth (left); mucron (terminal spicule-like structure) (right)
Images hosted on other servers:

Larva in submucosa with eosinophils and lymphocytes

Larva in jejunum
Additional references
Bacterial enterocolitis
Definition / general
Clinical features
Microscopic (histologic) description
Differential diagnosis
- Bacterial related disease due to either ingestion of preformed toxin (Staphylococcus aureus, Vibrio cholera, Clostridium perfringens), infection by toxigenic organisms or infection by enteroinvasive organisms which invade and destroy mucosal epithelium cells (eMedicine: Bacterial Gastroenteritis [Accessed 7 September 2023])
- Bacterial adhere to mucosal epithelial cells, elaborate enterotoxins, have capacity to invade
- Adhere by plasmid mediated adhesins (E. coli, V. cholera), fimbriae or pili
- Adhesion destroys microvilli brush border
Clinical features
- Complications due to massive fluid loss and loss of mucosal barrier include dehydration, sepsis, perforation
- Salmonella: invades via transcytosis with minimal epithelial damage
- Yersinia enterocolitica: penetrates ileal mucosa, multiplies in Peyer patches and regional lymph nodes
- Insidious infection: Yersinia and Mycobacterium tuberculosis
- Cytotoxins: Shiga toxin, enterohemorrhagic E. coli
- Enterotoxins:
- Bind to cell membrane, enter cell, activates massive electrolyte secretion (cholera toxin, E. coli heat labile and heat stable toxins produce traveler's diarrhea)
- No white blood cells in stool
- Bacterial invasion:
- Enteroinvasive E. coli and Shigella have plasmid that mediates epithelial cell invasion via microbe simulated endocytosis; then intracellular proliferation, cell lysis, cell to cell spread
- Patients ingest preformed toxins:
- Symptoms within hours
- Explosive diarrhea and acute abdominal distress
- 1 - 2 days
- C. botulinum may produce rapid, fatal respiratory failure
- Infection with enteric pathogens:
- Incubation of hours - days
- Diarrhea and dehydration (secretory enterotoxin) or dysentery (cytotoxin or enteroinvasive)
- Traveler's diarrhea:
- Fecally contaminated water / food
- Begins abruptly, subsides in 2 - 3 days
Microscopic (histologic) description
- Decreased epithelial cell maturation, increased mitotic figures, hyperemia and edema of lamina propria, variable neutrophils, modest villus blunting of small bowel
- Late: lymphocytes, plasma cells, regenerative change
Differential diagnosis
Cryptosporidium
Definition / general
Diagnosis
Microscopic (histologic) description
Microscopic (histologic) images
Images hosted on other servers:


Positive stains
Differential diagnosis
- Acid fast protozoa which causes self limited disease in immunocompetent but severe watery diarrhea resistant to most therapy in immunocompromised (J Biomed Res 2012;25:1)
Diagnosis
- Acid fast infective oocyst in stool
Microscopic (histologic) description
- 2 - 5 micron basophilic spherical structures attached to microvillus surface of epithelium
- Variable villus abnormality, may have eosinophils infiltrating mucosa
Microscopic (histologic) images
Images hosted on other servers:
Small round blue organisms at the luminal border

Cryptosporidium
Positive stains
Differential diagnosis
- Cellular debris
- Mucin
Entamoeba histolytica
Definition / general
Pathophysiology
Diagrams / tables
Images hosted on other servers:

Microscopic (histologic) images
Contributed by Hanni Gulwani, M.D.
Images hosted on other servers:


- Dysentery causing protozoa that can also cause fulminant colitis; causes up to 100,000 deaths per year (Trop Biomed 2011;28:194)
- Increased incidence in homosexual men and AIDS patients
Pathophysiology
- Fecal oral spread
- Amoeba invade colonic crypts, burrow into lamina propria, create flask shaped ulcer with broad base
- 40% invade portal vessels, embolize to liver and cause abscesses up to 10 cm
- May activate apoptosis in target cells (Trends Parasitol 2011;27:254)
- Rare abscesses in lung, heart, kidneys, brain
Diagrams / tables
Images hosted on other servers:

Life cycle
Microscopic (histologic) images
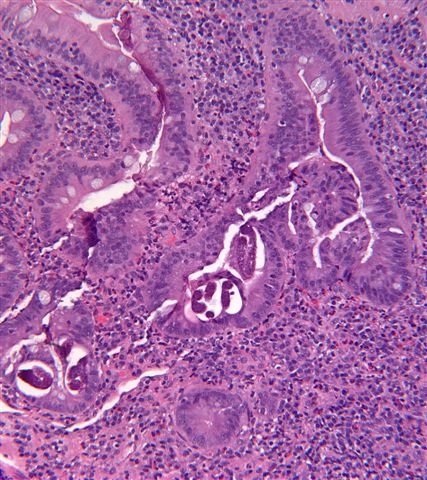
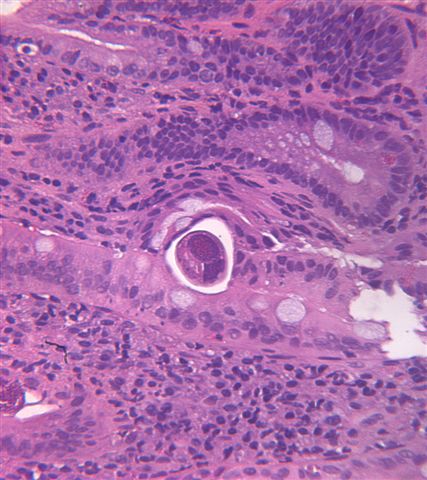
Contributed by Hanni Gulwani, M.D.
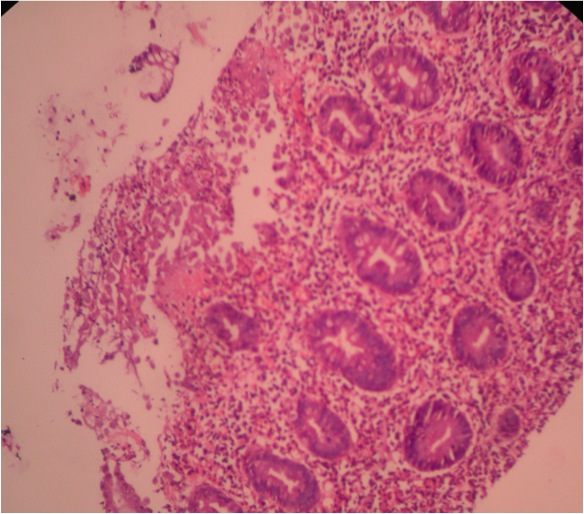
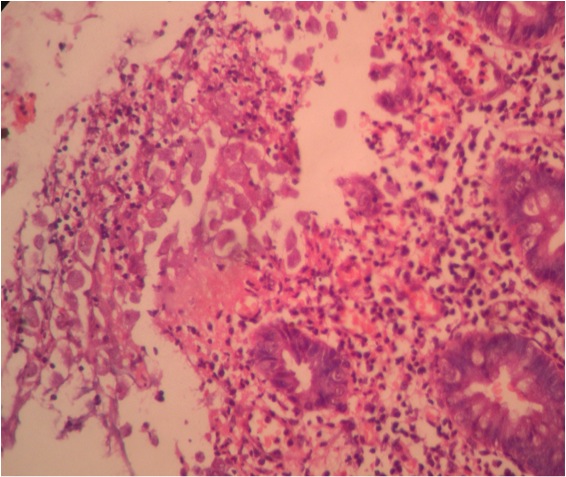
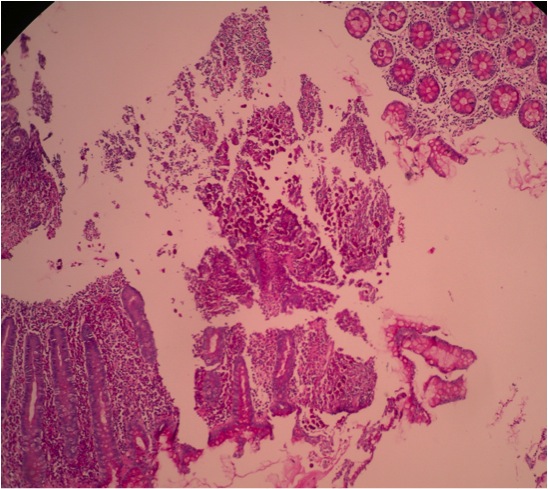
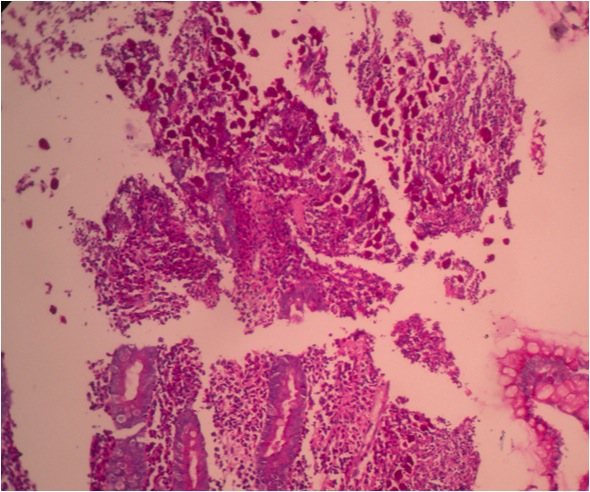
Amoebic colitis, numerous trophozoites of amoeba are noted
Amoebic colitis, PAS stain
Images hosted on other servers:
Ulcer seen in amebic colitis
Mice deficient for leptin or the functional leptin receptor
Giardia lamblia
- See Giardia lamblia
Isospora belli
Definition / general
Diagnosis
Case reports
Microscopic (histologic) description
Microscopic (histologic) images
Images hosted on other servers:

Positive stains
- Coccidian parasite that infects epithelial cells of small intestine
- Causes chronic diarrhea and acalculous cholecystitis in AIDS patients (Indian J Med Res 2011;134:878)
Diagnosis
- Cysts in stool, biopsy (H&E or EM)
Case reports
- 35 year old HIV+ man (Indian J Pathol Microbiol 2010;53:824)
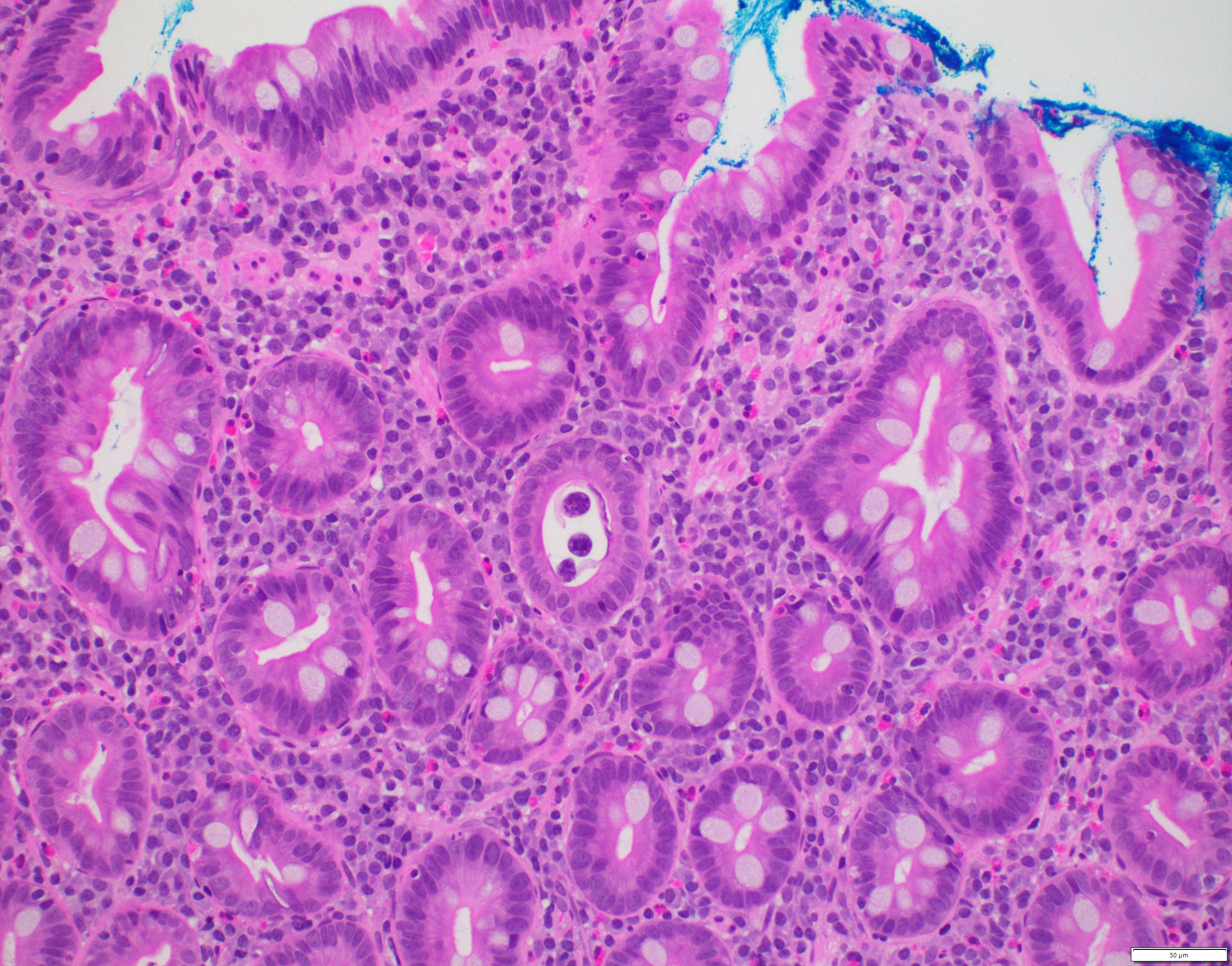
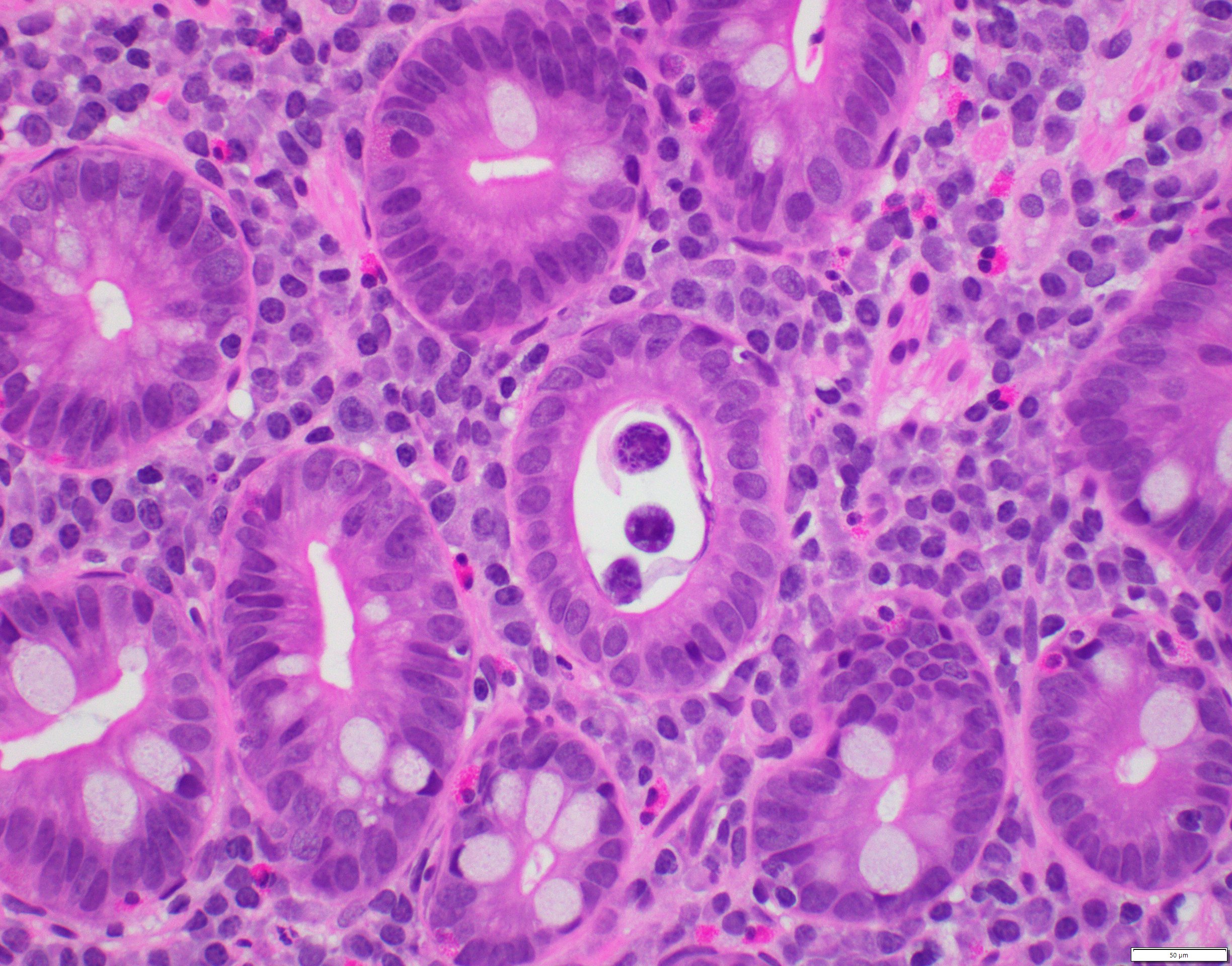
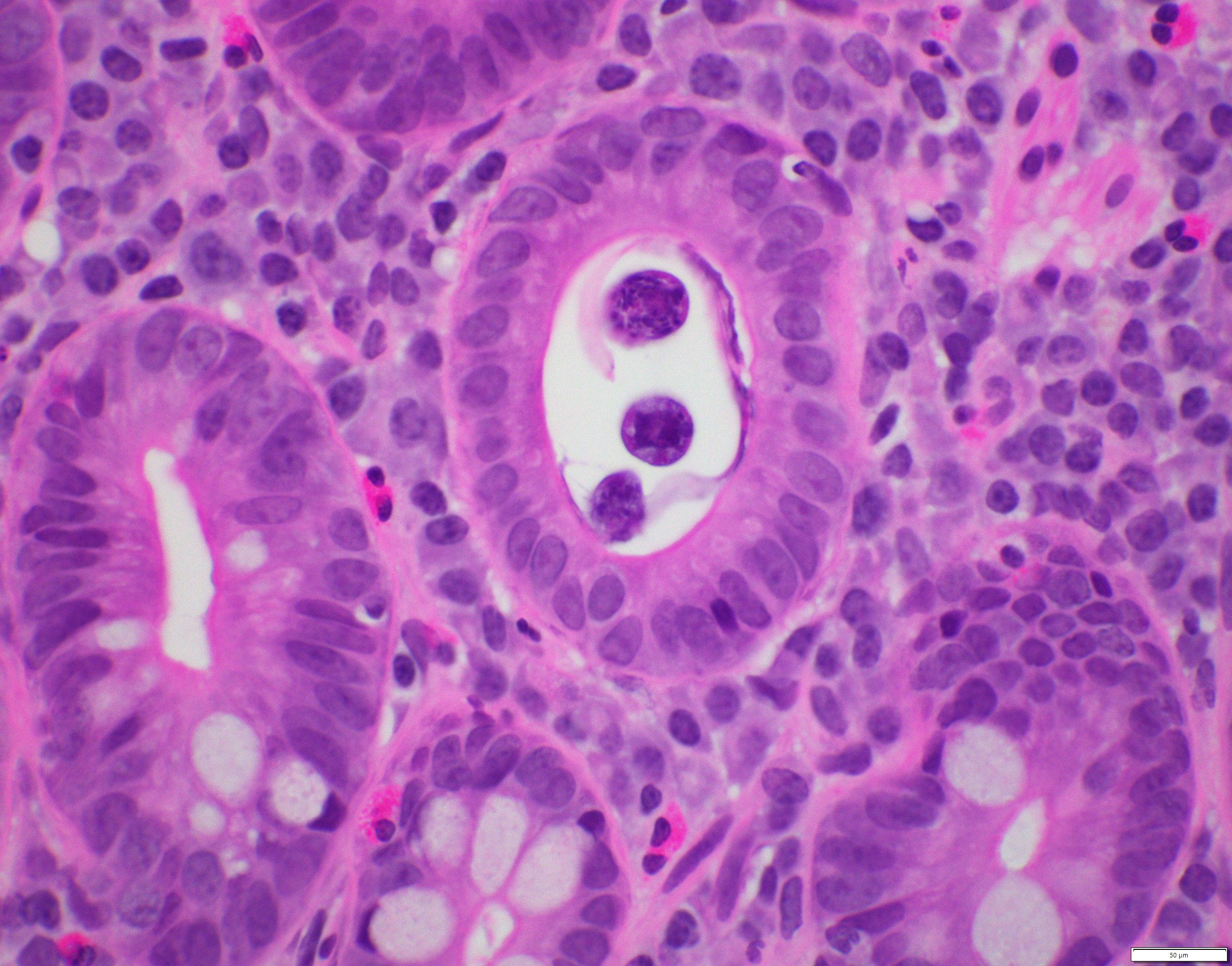
Microscopic (histologic) description
- Cysts present in parasitophorous vacuole in lamina propria (Hum Pathol 2001;32:500)
- Ovoid developmental forms are identified in and beneath epithelial cells near villus tip
Microscopic (histologic) images
Images hosted on other servers:

Oocyst of C. belli in epithelial cells of mammalian host
Positive stains
Microsporidia
Definition / general
Diagnosis
Case reports
Treatment
Microscopic (histologic) description
Microscopic (histologic) images
Images hosted on other servers:


Positive stains
Electron microscopy description
- Caused by Enterocytozoon bieneusi, an obligate intracellular protozoan that affects only enterocytes and Encephalitozoon intestinalis, which infects macrophages, fibroblasts, endothelial cells, enterocytes
- Both cause chronic diarrhea in patients with immunosuppression, HIV
Diagnosis
- Stool examination, PCR
Case reports
- 33 year old woman with myeloma, postautologous stem cell transplant and chemotherapy for relapse (Emerg Infect Dis 2012;18:1155)
- 43 year old man with pancreas / kidney transplant recipient and multiorgan system dissemination (Arch Pathol Lab Med 2004;128:e41)
Treatment
- Albendozole for E. intestinalis, nothing for E. bieneusi
Microscopic (histologic) description
- Minimal / no changes in mucosa but can find development spores as 1.5 mm dots in enterocytes
- May be surrounded by halos
- Also nucleated sporont present as 3 - 5 micron, rounded, basophilic structure often surrounded by a halo
Microscopic (histologic) images
Images hosted on other servers:
Various images
Positive stains
Electron microscopy description
- Often helpful for diagnosis
Rotavirus
Definition / general
Essential features
Terminology
ICD coding
Epidemiology
Sites
Pathophysiology
Clinical features
Diagnosis
Laboratory
Prognostic factors
Case reports
Treatment
Microscopic (histologic) description
Electron microscopy images
Images hosted on other servers:

Differential diagnosis
Additional references
- Primarily diarrheal illness caused by infection with rotavirus
Essential features
- Rotavirus is a segmented, nonenveloped double stranded RNA virus
- It is ubiquitous and infection is essentially universal first occurring in early childhood
- Transmission is fecal oral either via direct contact with stool or via fomites
- In the developed world, the vast majority of infections cause self limited diarrheal illness or in subsequent infections and vaccinated populations, are asymptomatic
- Most cases in the developing world are similar; however, the World Health Organization estimates that in 2013 ~215,000 children under 5 years old died from rotavirus infection (WHO: Rotavirus [Accessed 7 September 2023])
- Live attenuated vaccines are available and their use has resulted in a dramatic worldwide decrease of severe disease
- Intestinal intussusception is a rare but well recognized potential complication of vaccination
Terminology
- Rotavirus is a genus of the Reoviridae family
ICD coding
- ICD-10: A08.0 - rotaviral enteritis
Epidemiology
- Rotavirus is ubiquitous and infection is essentially universal in childhood in all socioeconomic groups
- Transmission is fecal oral either via direct contact with stool or via fomites
- Infection generally first occurs around 6 months of age as the gastrointestinal tract matures and passive immunity from breast milk wanes
- Infection may occur earlier in infants fed formula and in parts of India, Asia and sub-Saharan Africa where protection from maternal antibodies appears to be less effective
- Reinfection occurs throughout life and in most children older than 2 years and adults infection is minimally symptomatic or asymptomatic due to immunity either from prior infections or vaccination
- In the developed world, disease was more common in winter and spring; however, whether this pattern is still valid with widespread vaccination is unclear
- Transmission in the daycare and hospital setting is common
- Viral particles are hardy and resistant to chlorinated drinking water although they are vulnerable to alcohol based hand sanitizer and spray disinfectants
- The World Health Organization estimates that in 2013 ~215,000 children under 5 years old died from rotavirus infection, overwhelmingly in the developing world compared to 528,000 in 2000 (WHO: Global Illness and Deaths Caused by Rotavirus Disease in Children [Accessed 7 September 2023])
- According to the CDC in the United States rotavirus causes over 400,000 doctor visits, 200,000 emergency room visits, 55,000 to 70,000 hospitalizations and from 20 to 60 deaths each year (CDC: Rotavirus in the U.S. [Accessed 7 September 2023])
- Serologically rotavirus is classified into serogroups, subgroups and G and P serotypes
- Genotypically, it is classified into electropherotypes, genogroups and G and P genotypes
- There is a substantial geographic and temporal variation in strain distribution and antigenic drift as well as introduction and reassortment with animal viruses which increases genetic diversity
- Epidemiologically nucleic acid testing is increasingly replacing serologic testing
- Further information is available from the Rotavirus Classification Working Group's database (RotaC v2.0: Classification Tool for Rotaviruses Group A [Accessed 7 September 2023])
Sites
- Infection occurs in the small intestine
Pathophysiology
- Pathophysiology is complex and not fully understood
- Enterocytes at villous tips are initially infected; the virus binds surface carbohydrates and penetrates the cell membrane leading to transcription of viral RNA
- Damage to the mucosa leads to malabsorption
- Activity of disaccharidases and peptidases in the brush border is decreased and osmosis from unabsorbed nutrients contributes to the diarrhea
- Glucose cotransport of electrolytes is decreased but oral rehydration solutions are still affective (see Treatment below)
- Mature enterocytes are lost and initially replaced by immature secretory cells
- There is net secretion of water in part mediated by the enteric nervous system
- Clearance of infection is complex and involves overlapping elements of innate, cellular and humoral immunity
- Virus is usually shed for 6 to 10 days after patients become symptomatic
Clinical features
- There is an incubation period of 1 - 3 days
- Illness in infants and young children usually starts with vomiting and fever lasting 2 - 3 days, progressing to 4 - 5 days of profuse watery diarrhea
- In symptomatic older children and adults there is 1 - 4 days of diarrhea with anorexia, crampy abdominal pain and low grade fever
- Chronic infections may occur in immunosuppressed patients excepting HIV; isotonic dehydration and metabolic acidosis occur in severe cases
- Viremia is uncommon; extraintestinal manifestations are rare and described in the liver and kidney
- Intestinal intussusception is a rare but well recognized potential complication of vaccination
- Prior intussusception is a contraindication to vaccination
- Patient deaths are due to dehydration and electrolyte abnormalities that lead to cardiac failure or less commonly seizures or aspiration pneumonia
Diagnosis
- Enzyme immunoassay and PCR are the mainstays
- Latex agglutination is often used in resource poor areas
- Viral culture and electron microscopy are largely of historical interest
- Microbiologic diagnosis is rarely required
Laboratory
- Severe disease may cause metabolic acidosis and high urine specific gravity
- Mild elevation of transaminases and uric acid may occur
- Leukocytosis is rare and stool is usually negative for white blood cells and blood
Prognostic factors
- Disease is most severe in infants and young children
- Immunosuppressed patients often suffer from more severe disease and cannot receive the live attenuated vaccine although patients infected with HIV do not suffer more severe disease and should be vaccinated
- Infection in the developing world is more likely to lead to severe illness or death; this is related to less access to health care, malnutrition, the presence of other infections and possibly larger inoculums
Case reports
- 5 month old boy, 51, 54 and 71 year old men in a multiorgan transplant unit (Transpl Int 2005;18:470)
- 22 month old girl with opsoclonus myoclonus syndrome after rotavirus gastroenteritis (Pediatr Int 2014;56:e86)
- 8 year old Japanese girl with mild encephalopathy (BMJ Case Rep 2016;2016:bcr2016216895)
- 73 year old man with Henoch-Schönlein purpura (Am J Case Rep 2017;18:136)
Treatment
- Mild to moderate disease: oral rehydration
- Severe disease: intravenous lactated ringers or normal saline until oral rehydration can be tolerated
- Infants: return to breast feeding or formula as soon as it can be tolerated
- In the developing world, zinc supplementation and some probiotics in children older than 6 months may reduce disease duration
- Diosmectite, a type of aluminum magnesium clay silica, is available in parts of Europe and controls gastroenteritis
- Oral immunoglobulins have a possible role in chronic disease and for high risk patients where vaccination is unlikely to be effective (premature infants) or is contraindicated
- Antibiotics are not indicated
- Vaccination is recommended to commence at 2 months of age
Microscopic (histologic) description
- Biopsy is rarely performed
- Findings are nonspecific; villi are shortened, blunted and lined by cuboidal cells
- There is crypt hyperplasia and increased mononuclear cells within the lamina propria
- Apoptotic epithelial cells may be present
- Disease may be patchy in distribution
- Viral inclusions are not present
Electron microscopy images
Images hosted on other servers:

Multiple
rotavirus
particles
Differential diagnosis
- Other causes of infectious gastroenteritis and enterocolitis
Additional references
Salmonella
Definition / general
Gross images
Case #362


Microscopic (histologic) description
Microscopic (histologic) images
Case #362
- Bacterial causing food poisoning and typhoid fever (S. typhi)
- Typhoid fever: systemic dissemination with bacteremia, fever, chronic infection of joints, biliary tree, bones and meninges
- From contaminated milk, eggs, beef, poultry
- Usually affects terminal ileum
Gross images
Case #362
Microscopic (histologic) description
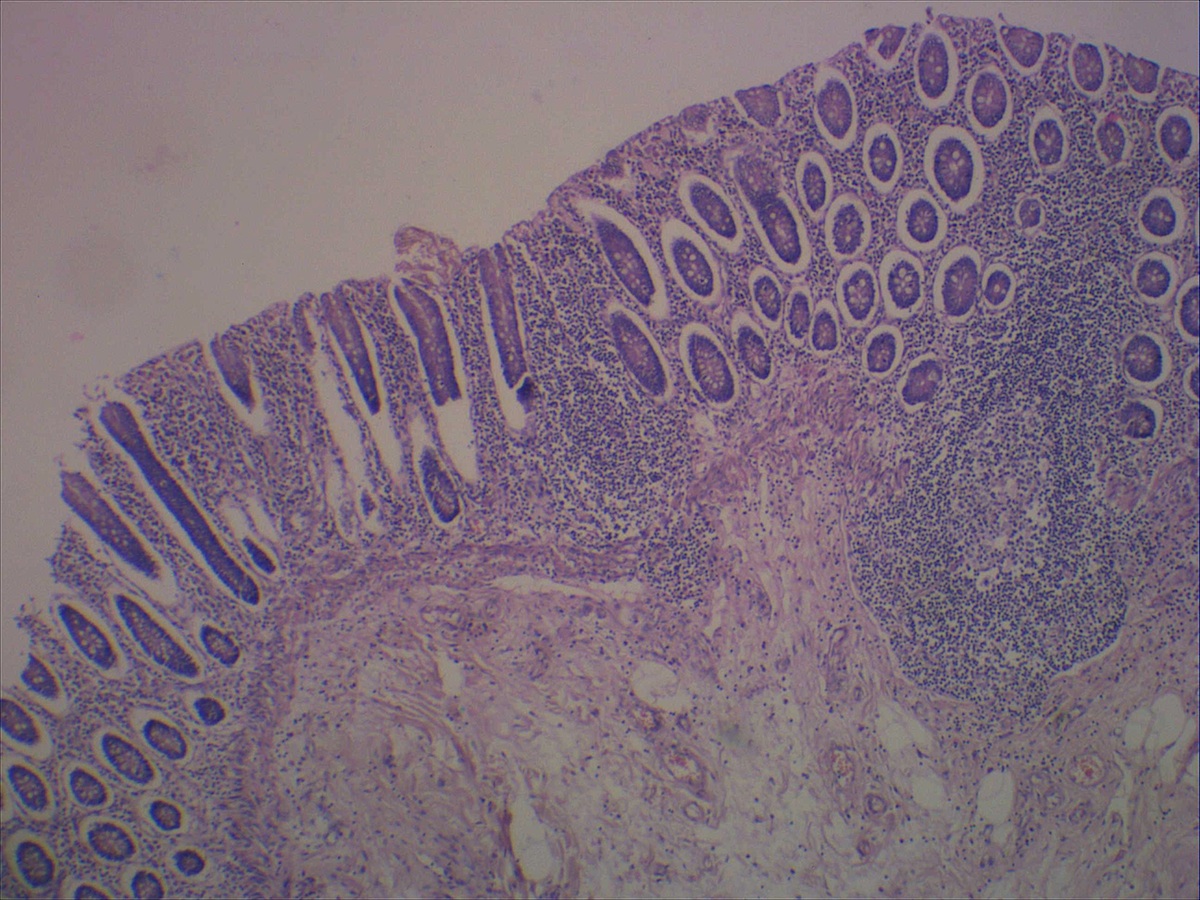
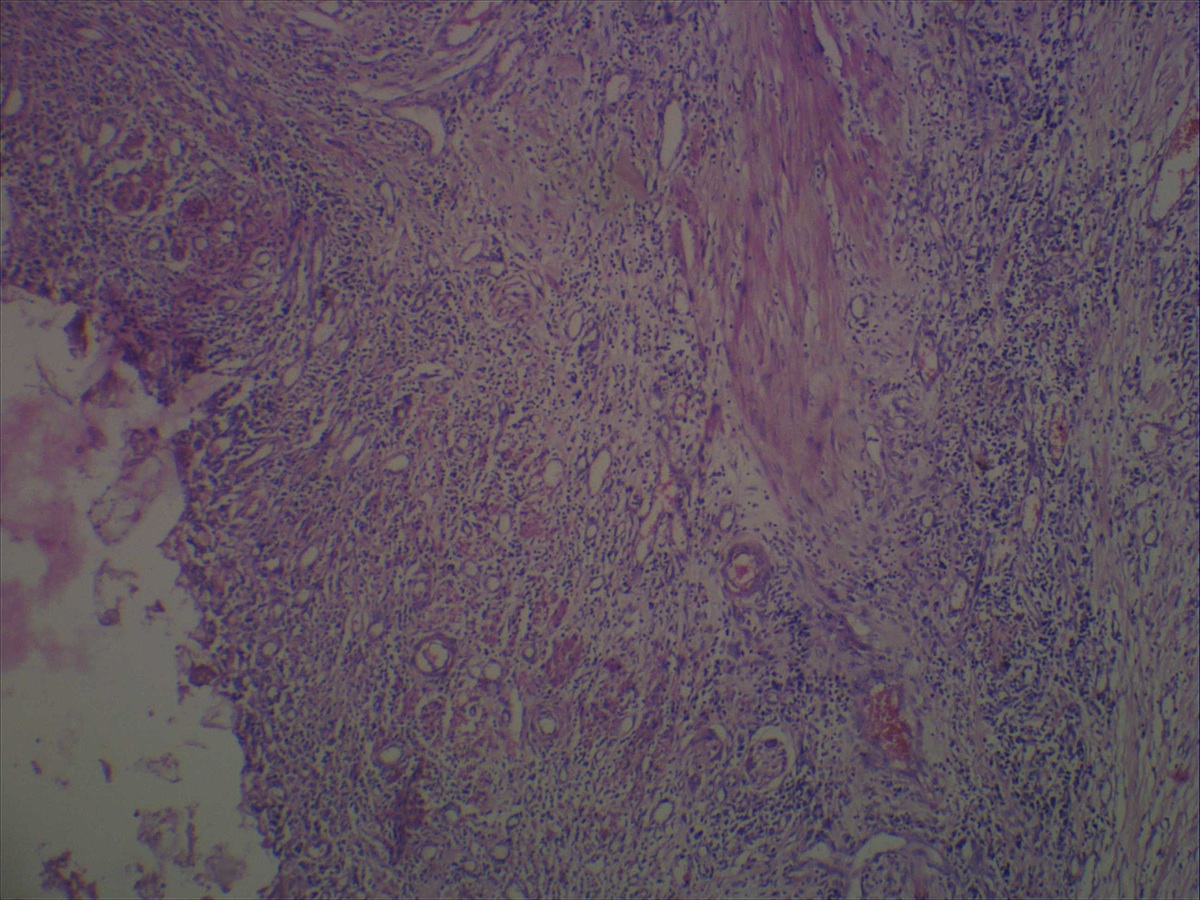
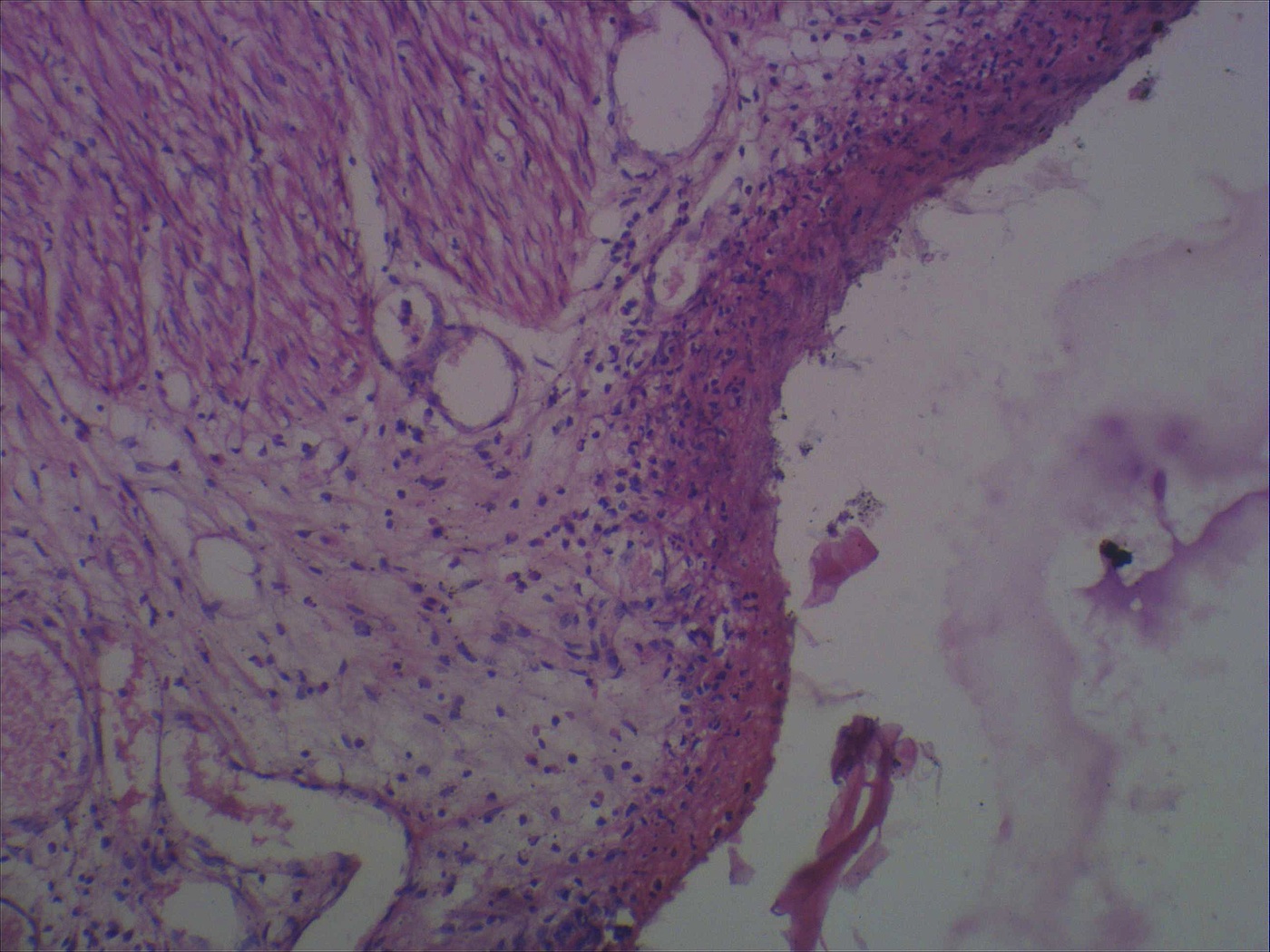
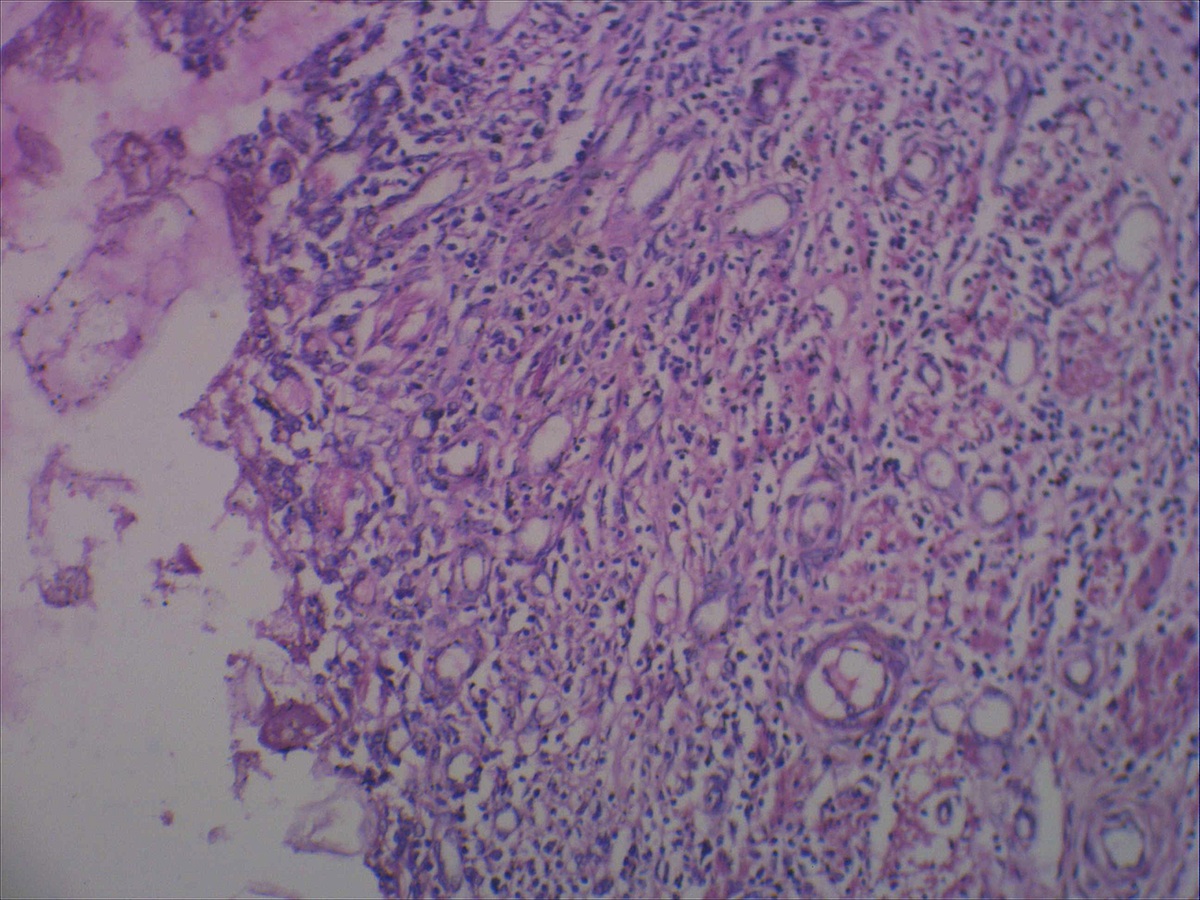
- Ulcers overlying Peyer patches with minimal inflammatory cells, chiefly mononuclear (plasma cells, histiocytes and lymphocytes)
- Often histiocytes with erythrophagocytosis
- May lead to perforation or toxic megacolon
Microscopic (histologic) images
Case #362
Strongyloides stercoralis
Definition / general
Life cycle
Diagrams / tables
Images hosted on other servers:

Clinical features
Diagnosis
Case reports
Treatment
Microscopic (histologic) images
Contributed by Josehp Christopher Castillo, M.D. and Case #133

Contributed by @liverwei on Twitter
Additional references
- Nematode with complex life cycle that alternates between free living and parasitic cycles, with potential for autoinfection and multiplication within host
Life cycle
- Larvae burrow into mucosa of duodenum and jejunum, where they mature into adults
- Females lay eggs, which develop into larvae that pass into stool, where they mature and become infective
- Infective larvae in soil penetrate intact skin, usually through feet
- Larvae enter circulatory system, are transported to lungs, enter alveolar spaces, are carried to trachea and pharynx, are swallowed and enter intestinal tract, where process is repeated
- If larvae become infective before leaving body, they may invade intestinal mucosa or perianal skin, causing autoinfection
Diagrams / tables
Images hosted on other servers:
Life cycle
Clinical features
- Symptoms: none, diarrhea, malabsorption
- Severe / fatal infections in immunocompromised, due to worms moving from GI tract into other organs (WormBook 2007:1)
Diagnosis
- Larvae in stool
- Adult female or eggs in small bowel mucosa, often with eosinophilic or granulomatous inflammation
Case reports
- 43 year old Honduran man with diarrhea and abdominal pain (Case #133)
- 66 year old man with weakness and epigastric pain (Int J Prev Med 2012;3:370)
Treatment
- Antihelminths such as thiabendazole (Ann Pharmacother 2007;41:1992)
- Prevent by wearing shoes in endemic areas
Microscopic (histologic) images
Contributed by Josehp Christopher Castillo, M.D. and Case #133
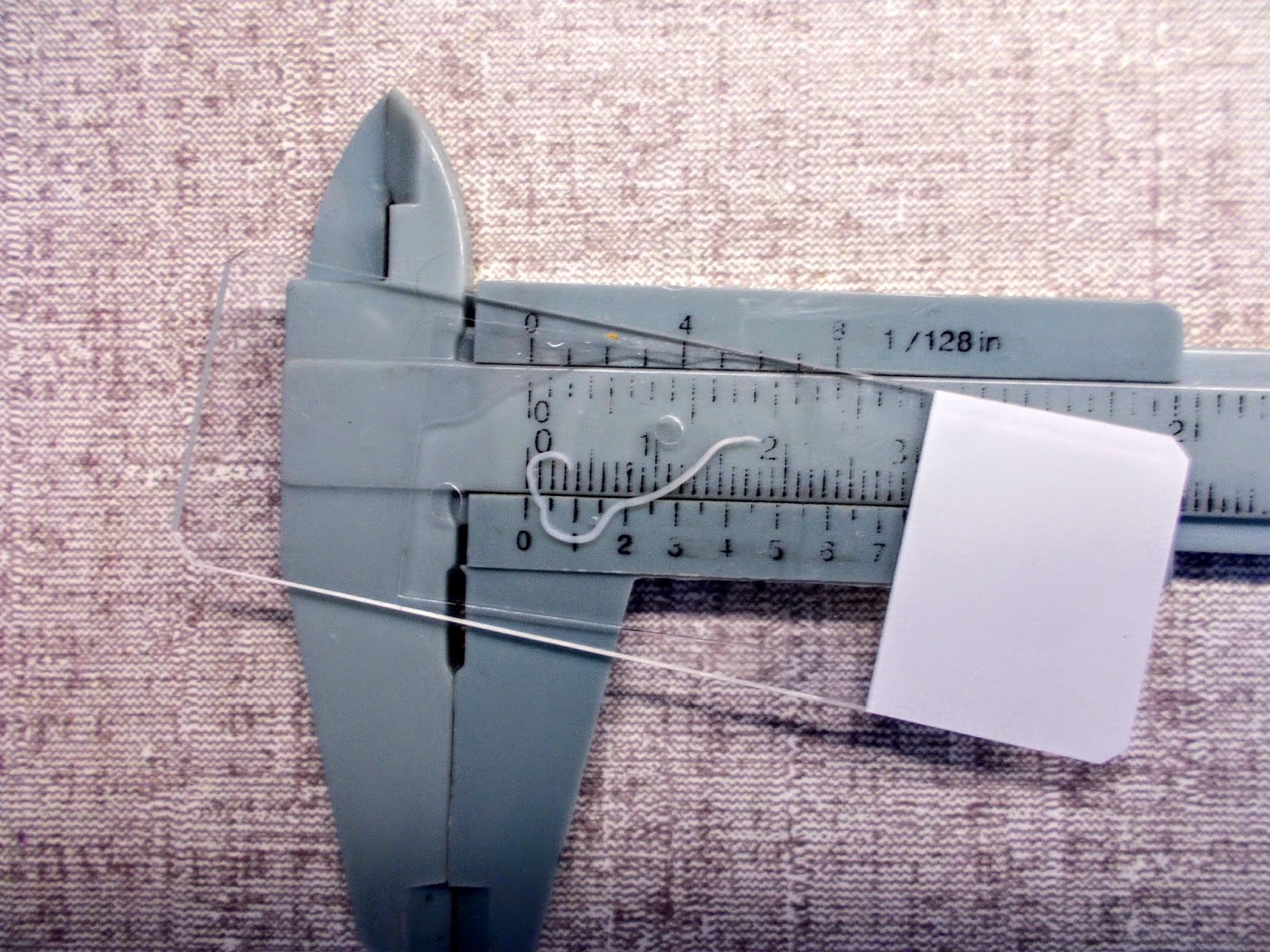
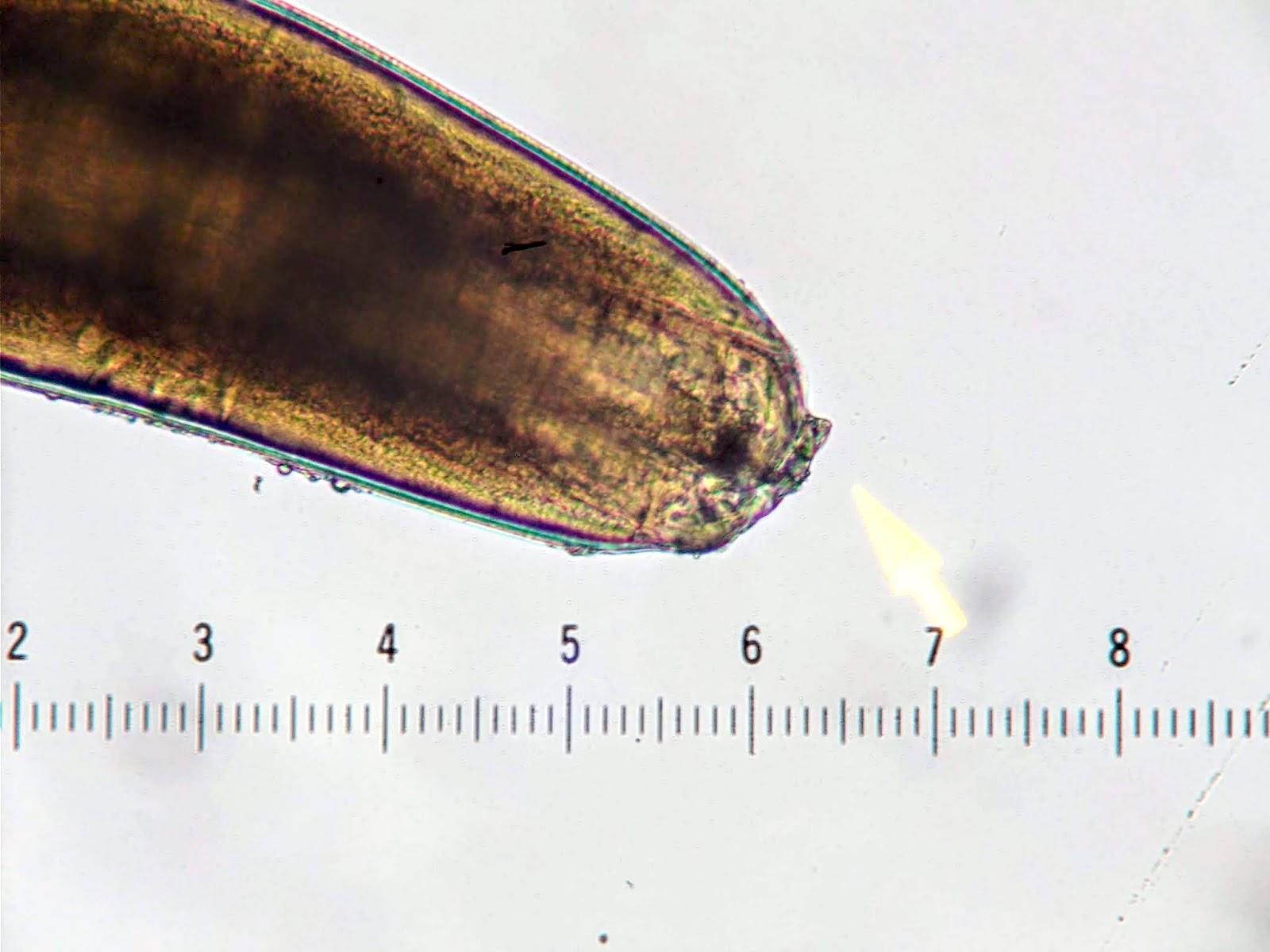
Small intestine
Various images
Contributed by @liverwei on Twitter
Strongyloides stercoralis
Additional references
Vibrio cholerae (pending)
[Pending]
Whipple disease
- See Whipple disease
Board review style question #1
What is true regarding rotavirus?
- Characteristic viral inclusions are diagnostic
- Incidence has increased
- Infection typically affects the sigmoid colon and rectum
- Intussusception is a rare but recognized complication associated with vaccination
- Most deaths occur in the elderly
Board review style answer #1
D. Intussusception is a rare but recognized complication associated with vaccination. However, there is broad agreement that the benefits of vaccination greatly exceed the risk.
Comment Here
Reference: Infectious disorders-general
Comment Here
Reference: Infectious disorders-general

