
Soft tissue
Vascular
Benign
Cystic / cavernous lymphangioma


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Cystic / cavernous lymphangioma

- Benign vascular lesion composed of a collection of dilated lymphatic channels that may be superficial, deep or diffusely involve organ systems
- First described by Rodender in 1828 (Arch Pathol Lab Med 2015;139:278)
- Benign proliferation of lymphatic vessels
- Immunohistochemical expression of CD31 and D2-40
- Lymphatic malformation
- Lymphangioma circumscriptum (superficial cutaneous lymphangioma)
- Cavernous lymphangioma (deep lymphangioma)
- Cystic hygroma (cystic lymphangioma)
- Intra-abdominal cystic lymphangioma
- Hemangiolymphangioma
- Lymphangiomatosis (generalized lymphangioma, systemic angiomatosis)
- ICD-O:
- ICD-11:
- LA90.12 & XH9MR8 - lymphatic malformations of certain specified sites & lymphangioma, NOS
- 2E81.10 - disseminated lymphangiomatosis
- Primarily occurs in children and young adults
- Majority presents at birth or within first couple of years (~90%) (J Pediatr Surg 1999;34:1164)
- Intra-abdominal lesions have a slight male predominance
- Cystic hygroma may occur in association with Turner syndrome (Hum Pathol 1984;15:61)
- Splenic lymphangiomas may occur with Klippel-Trenaunay syndrome (J Vasc Surg 2006;43:848)
- Associated with variant of Maffucci syndrome (J Pediatr Orthop B 2003;12:147)
- Associated with trisomies 13, 18 and 21 and other genetic syndromes (e.g., Noonan)
- Rare cases can occur in older adults, often mesenteric lesions (Arch Surg 1985;120:1266, Pathol Oncol Res 2000;6:146, BMJ Case Rep 2011;2011:bcr0320114022)
- Superficial lesions frequently involve the skin of proximal extremities / limb girdles (Br J Dermatol 1976;94:473)
- Deep lesions frequently involve the head and neck (primarily tongue and floor of mouth), followed by the extremities, axilla, groin and abdominal region (J Pediatr Surg 1999;34:1164, Virchows Arch 2008;453:1, Hum Pathol 2005;36:426)
- Cystic hygroma commonly involves head and neck, usually posterior triangle of neck
- Intra-abdominal lesions involve mesentery, omentum and retroperitoneum
- Lymphangiomatosis can involve multiple sites (e.g., liver, lungs and bone) (Am J Surg Pathol 1995;19:125, J Bone Joint Surg Am 2005;87:162, J Pediatr Hematol Oncol 2004;26:136)
- Arises from abnormal lymphatic system development
- PIK3CA and other mutations thought to drive the process through endothelial growth receptor pathways (J Pediatr 2015;166:1048, Int J Clin Exp Pathol 2015;8:5924)
- Early or congenital lesions are favored to be developmental malformations
- Sequestered lymphatics fail to communicate with normal lymphovascular system
- Most are considered to be malformations / hamartomas (not true neoplasms)
- Genetic abnormalities play a role (Virchows Arch 2008;453:1)
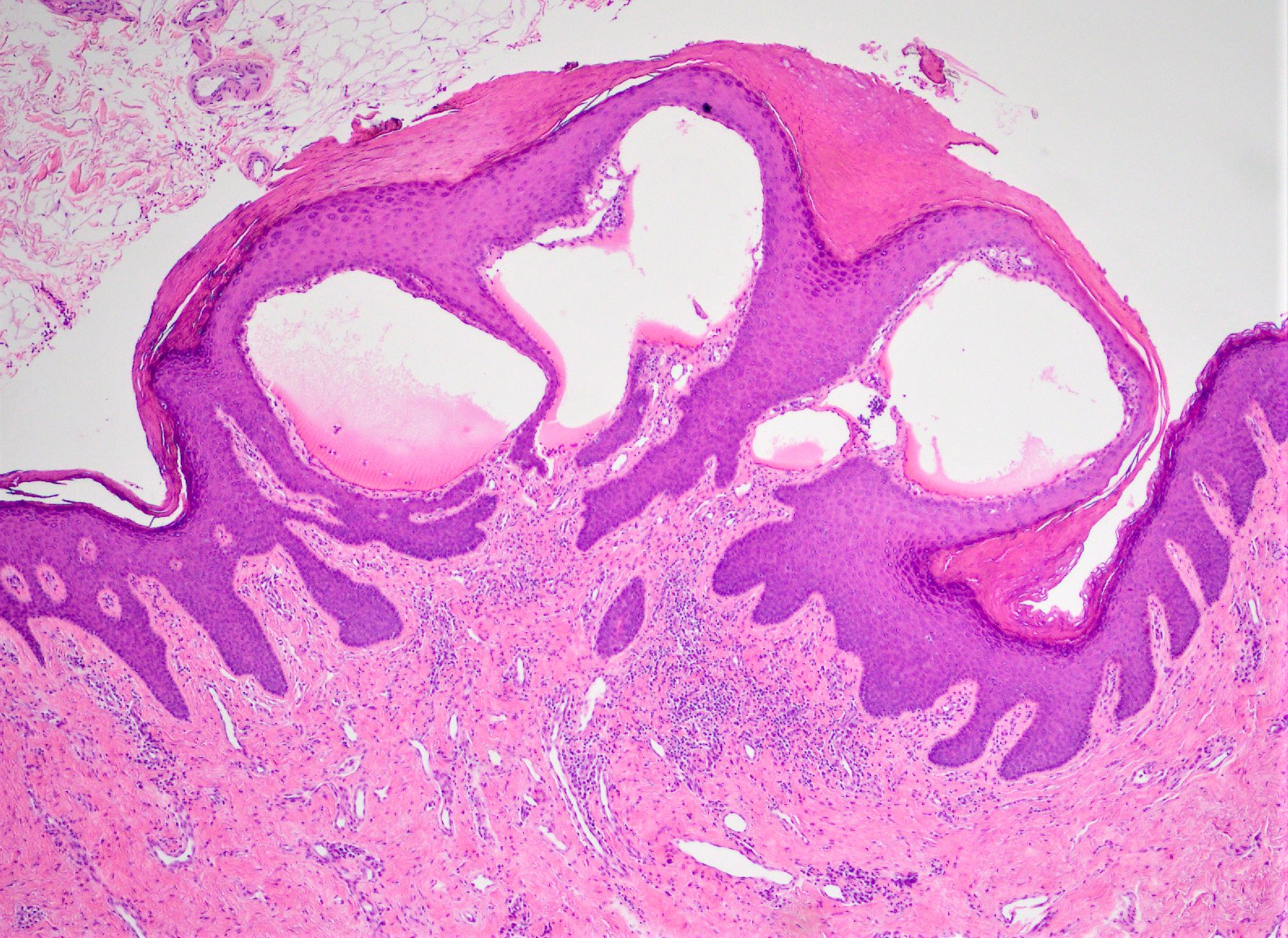
- Superficial lesions may present as multiple small, grouped vesicular lesions involving the skin
- Tongue lesions present as a mass surfaced by pebbly, vesicle-like nodules said to resemble frog eggs (Head Neck Pathol 2020;14:512)
- Cystic hygroma usually presents as a unilateral, diffuse, nonpulsatile, painless swelling of the posterior cervical triangle
- Deeper lesions may present as a large, slow growing painless mass
- Intra-abdominal lesions can displace organs and cause intestinal obstruction
- Swollen soft tissue mass with positive transillumination test
- Ultrasound can confirm cystic or multicystic lesion
- Diagnosing these lesions may be very challenging in small biopsies given their cystic nature and bland cytologic features
- Xray:
- Abdominal lesions commonly present as a soft tissue mass with displacement of bowel loops (Pediatr Radiol 2002;32:88)
- Ultrasound:
- Unilocular or multilocular anechoic mass
- Sharply defined cystic of multicystic mass with internal septations
- May be diagnosed on prenatal ultrasound (Prenat Diagn 1988;8:405)
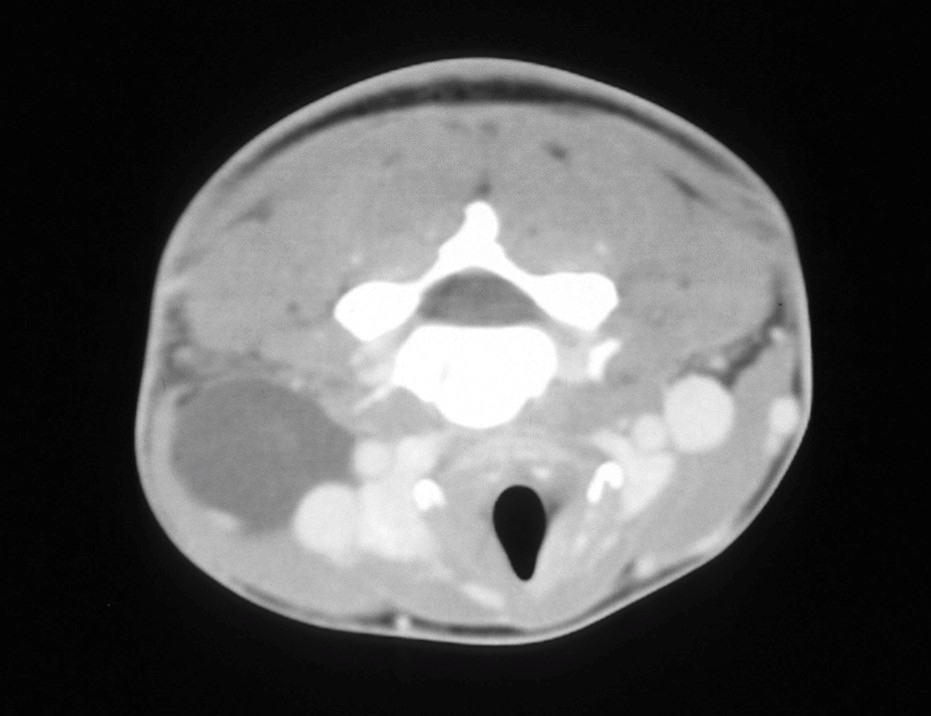
- CT findings:
- Nonenhancing cystic lesions
- Septated cystic mass of variable size (Pediatr Radiol 2002;32:88)
- Contains fluid of homogeneous density
- May displace adjacent organs
- MRI findings:
- T1 weighted image may be hypointense or hyperintense when filled with hemorrhage or proteinaceous material (Magn Reson Imaging 2003;21:81)
- T2 weighted image shows a multiloculated mass with hyperintense areas
Contributed by Jeanne Meis, M.D.
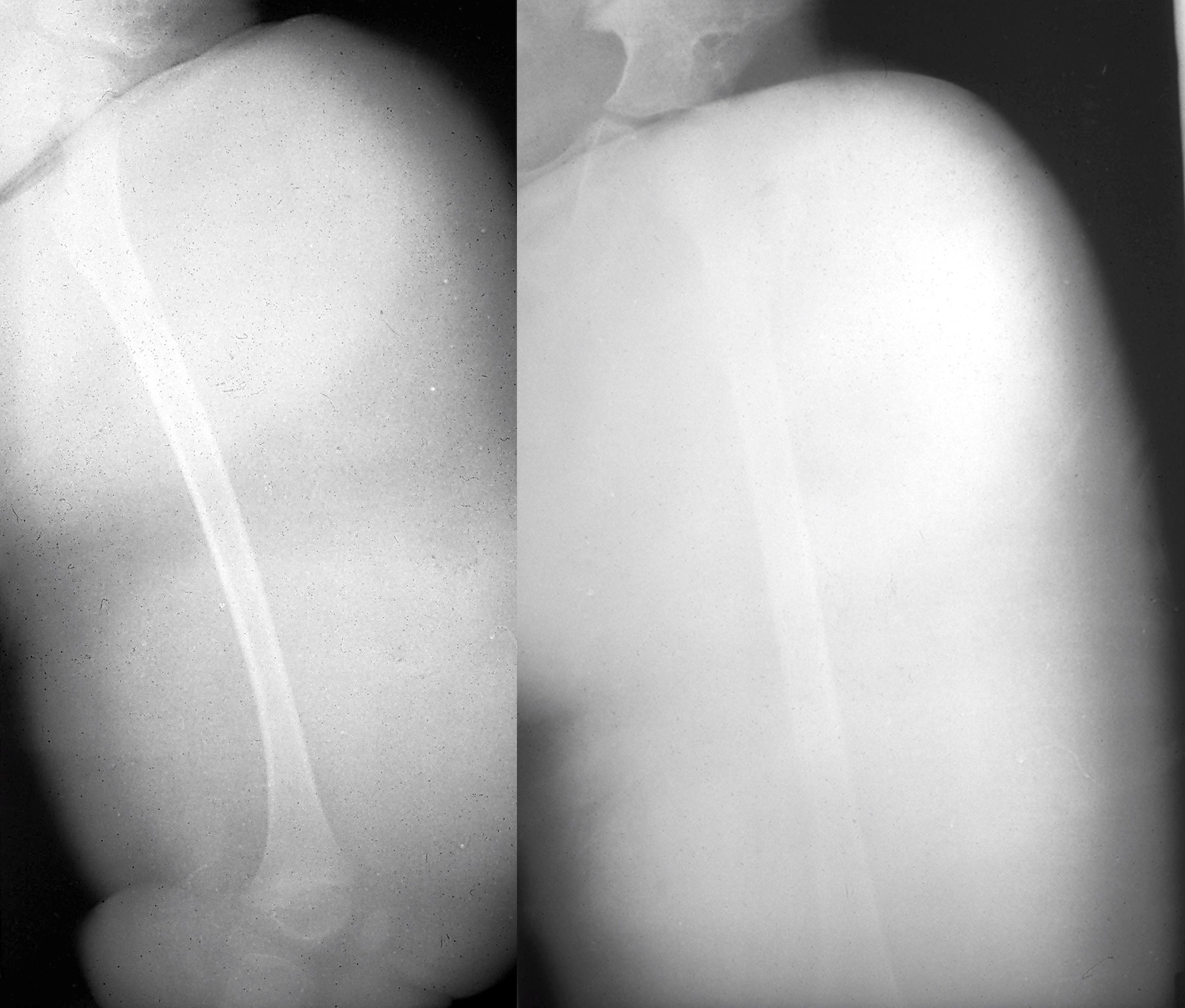
Radiograph of left lower extremity
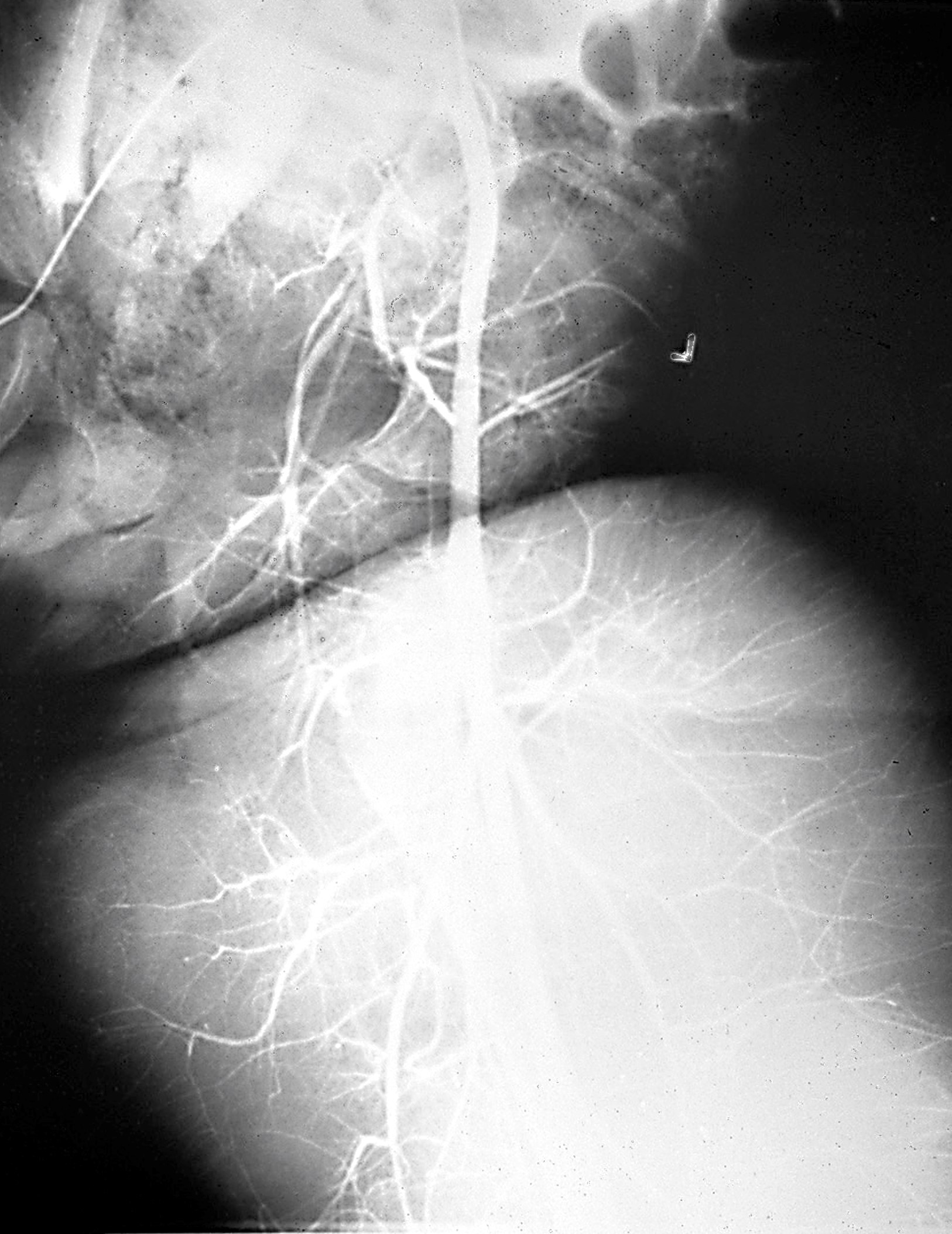
Angiogram of
lymphangiomatosis
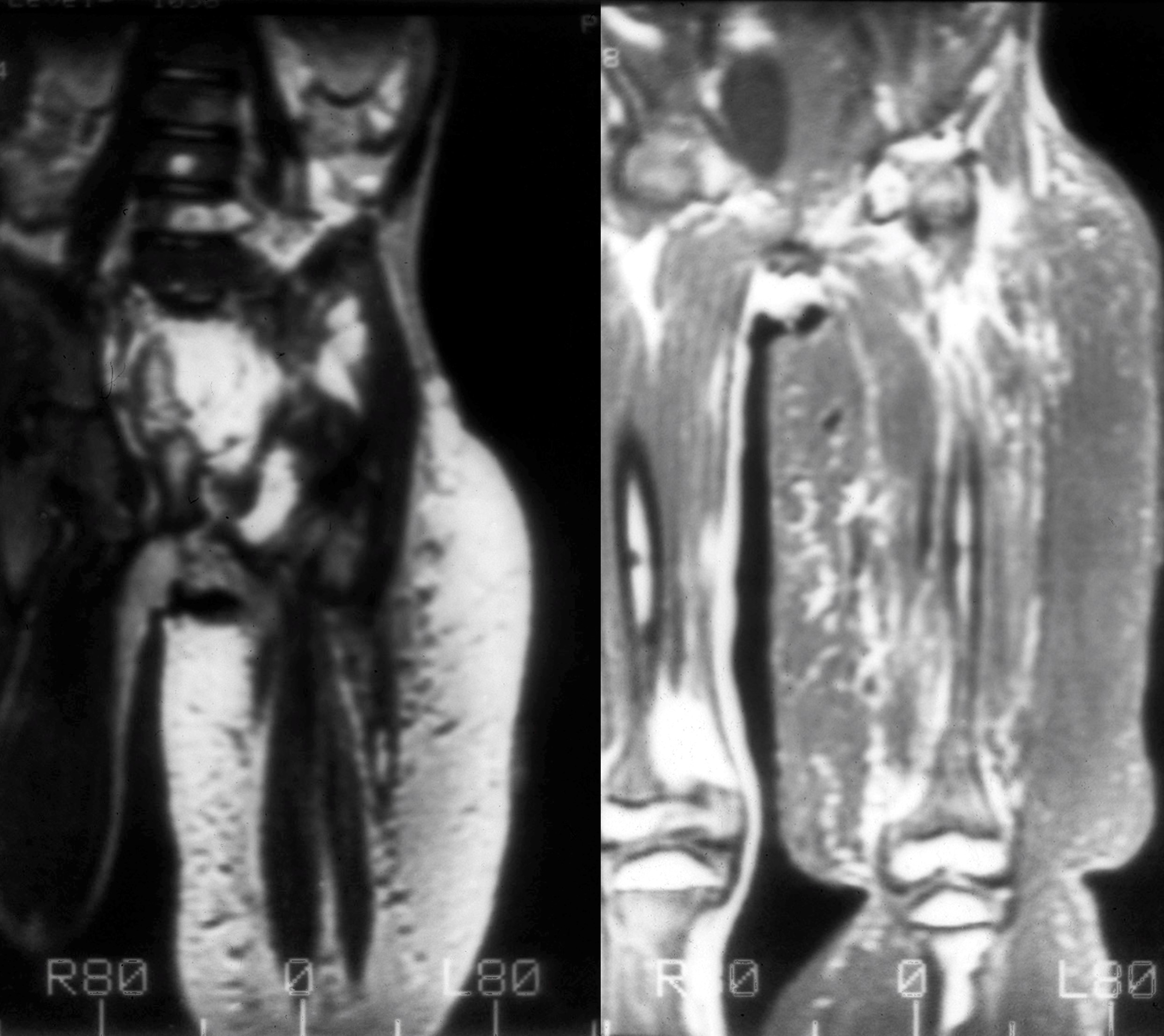
MRI of left extremity

MRI of lower abdomen
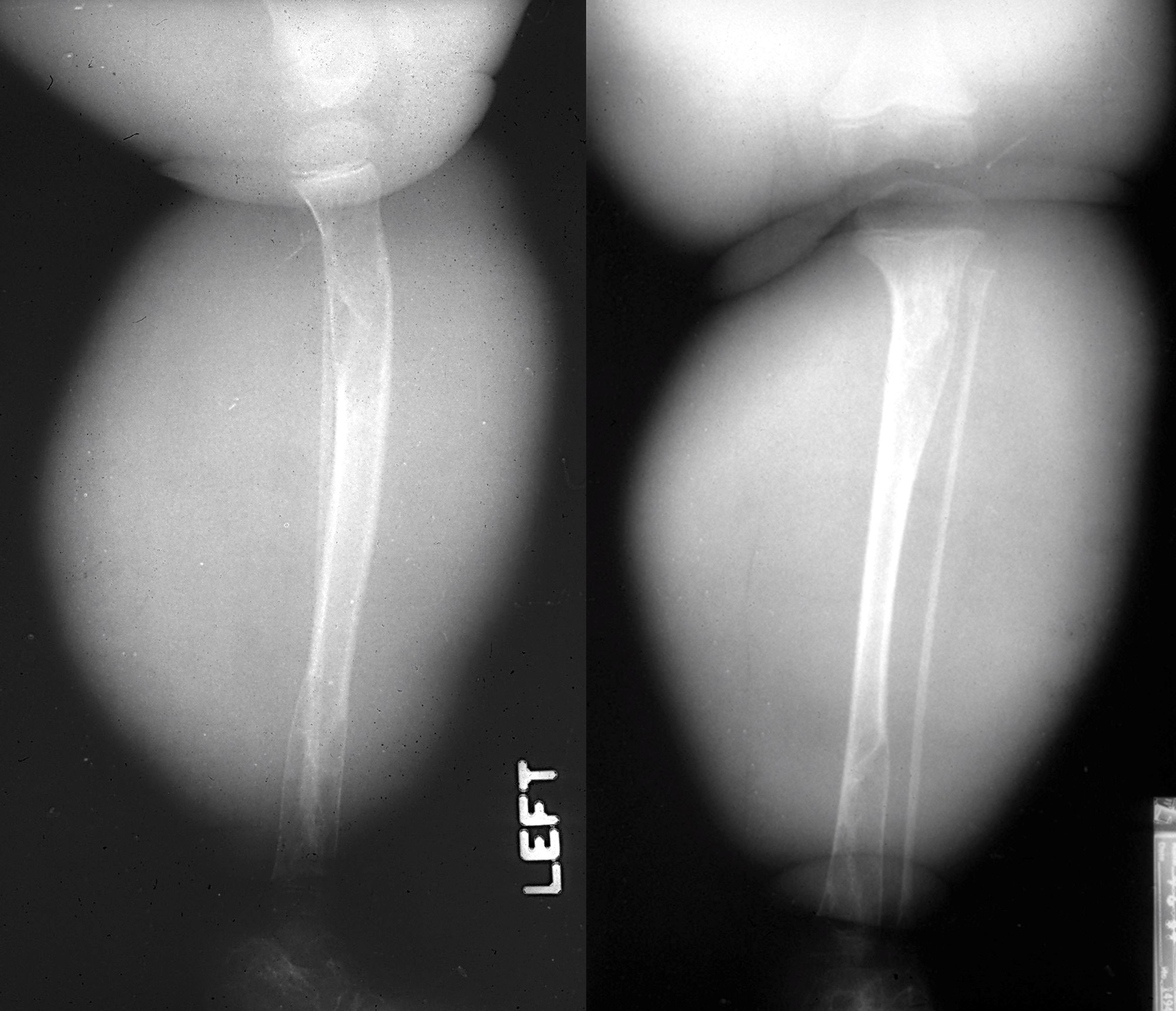
Radiograph of lower extremity
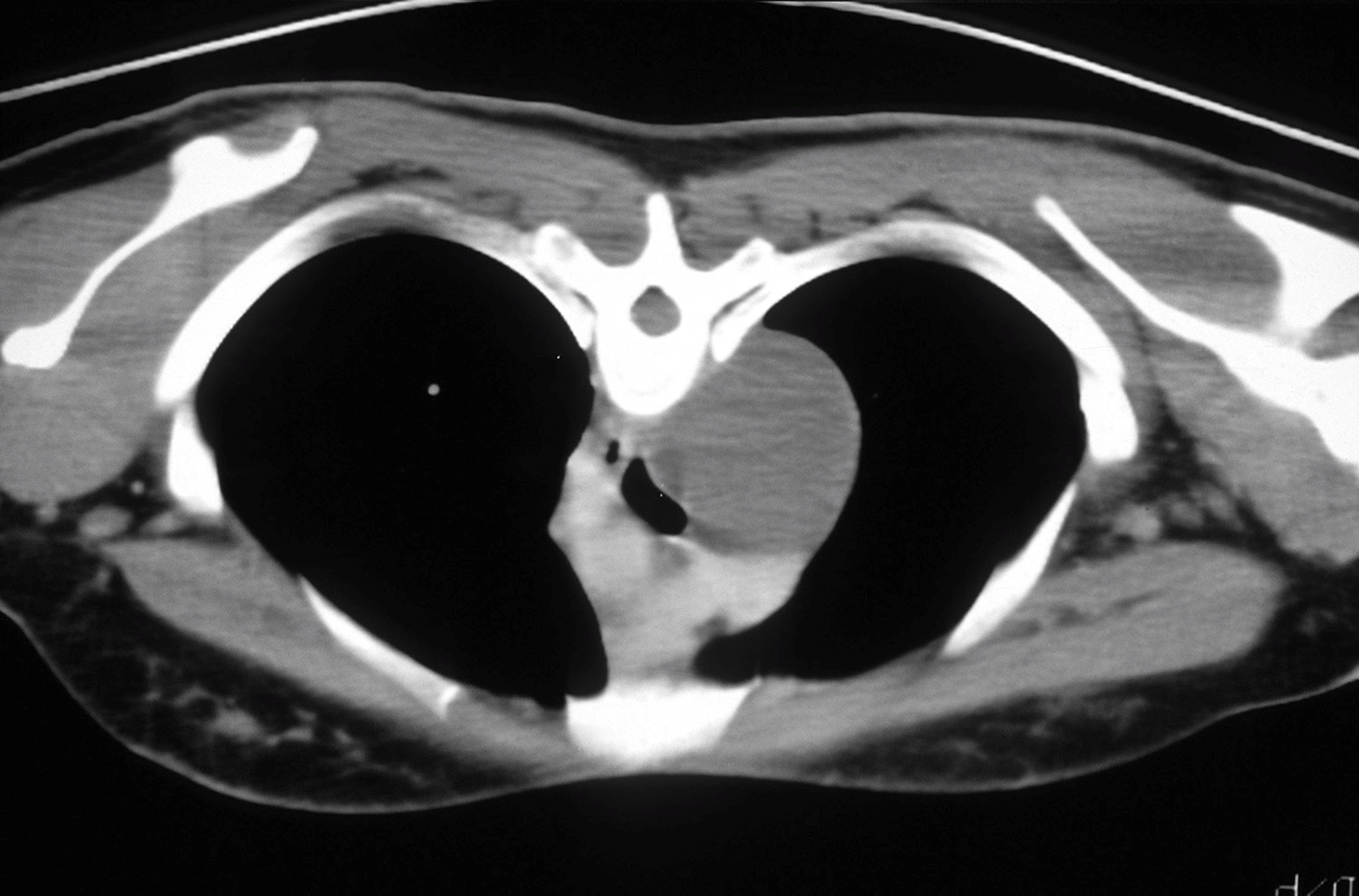
MRI of mediastinal lymphangioma

Radiograph of mediastinal lymphangioma
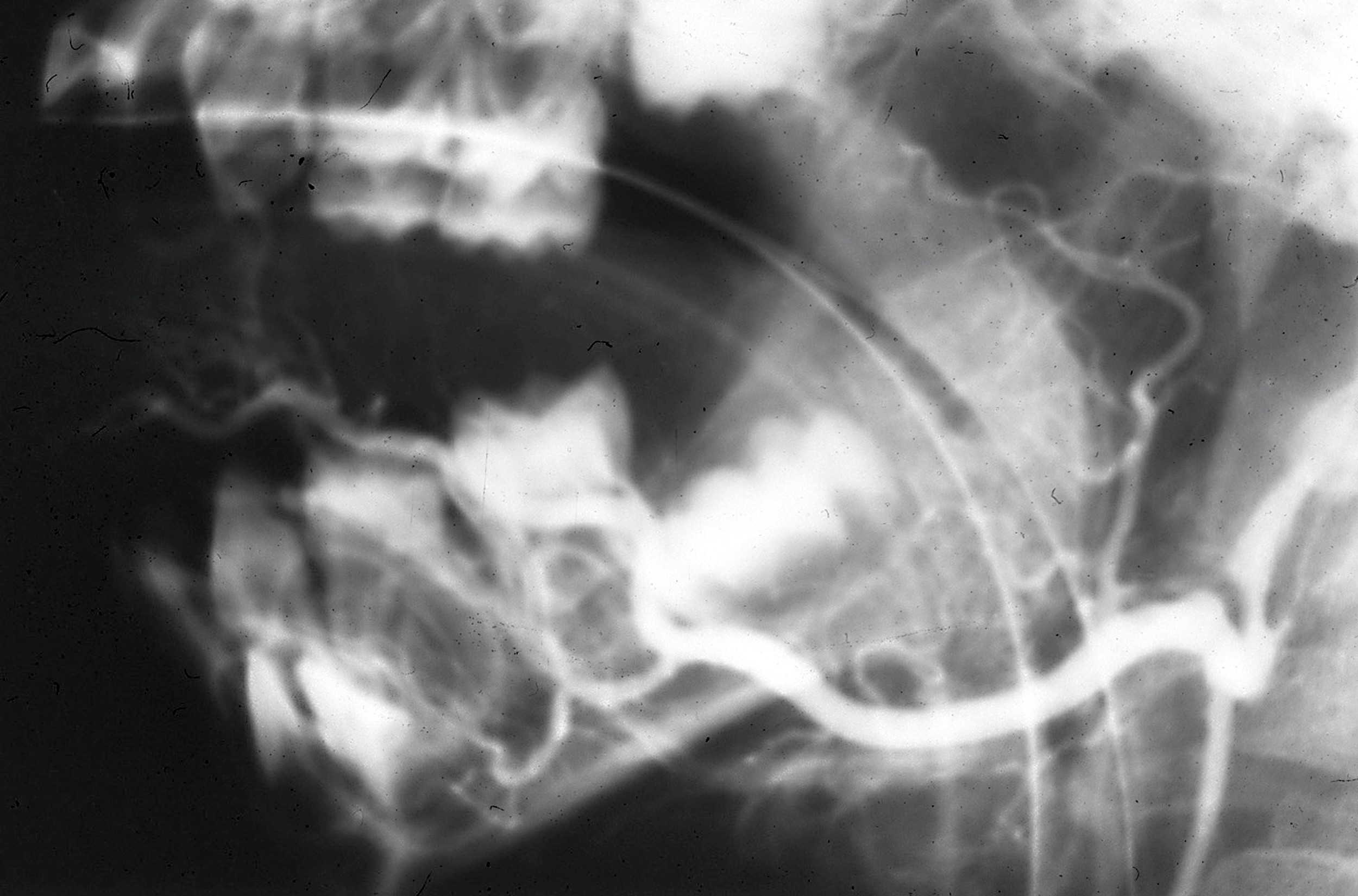
Arteriogram of lymphangioma
Images hosted on other servers:

CT of splenic lymphangioma

CT of orbital lymphangioma

Ultrasound of mesenteric lymphangioma
- Benign lesions with excellent prognosis
- Recurrence is high with incomplete removal
- When involving deeper tissue planes, lesions can recur in up to 20% of patients (J Pediatr Surg 1992;27:220)
- Complications include infection, hemorrhage, rupture and intestinal obstruction
- Diffuse lymphangiomatosis with mediastinal or visceral organ involvement can be fatal
- No malignant transformation has been reported
- 13 year old boy with cystic hygroma of the neck (Rom J Morphol Embryol 2021;62:845)
- 24 year old woman with lymphangioma of the dorsal tongue (Head Neck Pathol 2020;14:512)
- 34 year old woman with jejunal cavernous lymphangioma (BMJ Case Rep 2011;2011:bcr0320114022)
- Surgical resection may be indicated for large, symptomatic lesions
- Intralesional injection of sclerosing agents, including bleomycin and OK-432
- Radiofrequency ablation (Int J Pediatr Otorhinolaryngol 2008;72:953)
Contributed by Jeanne Meis, M.D.

Lower extremity
Images hosted on other servers:

Cystic hygroma of neck


Lymphangioma of dorsal tongue



Omentum: 30 cm tumor in 4 year old girl



Scrotal tumor with hemorrhage in 3 year old boy

Abdominal cyst: 25 cm

Broad ligament: 19 kg tumor in 70 year old woman

Mesentery: 1 year old boy

Thigh tumor


Mesenteric tumor: 12 year old girl


Mesenteric tumors


Mesenteric tumors
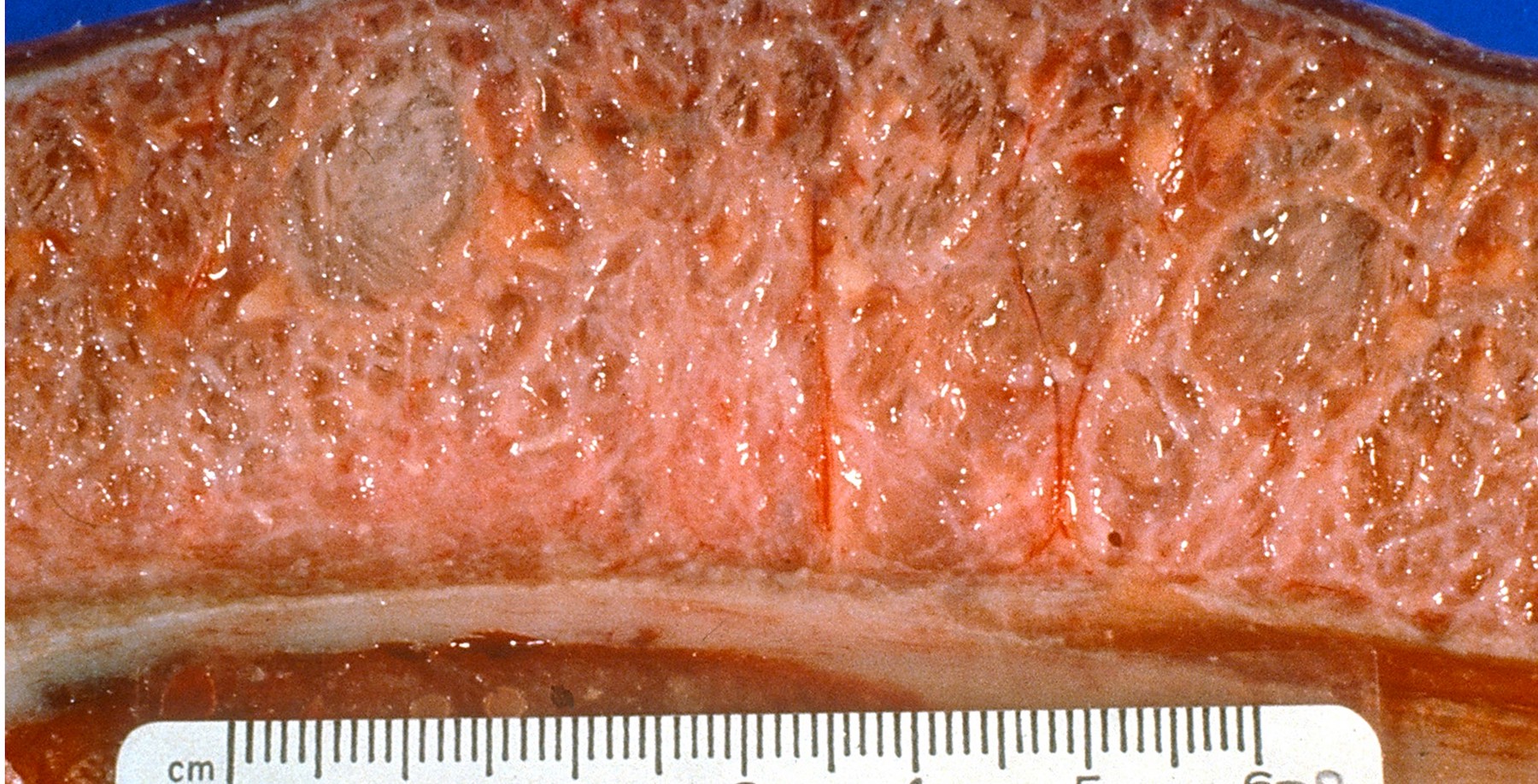
- Multicystic and spongy lesions
- Reddish / brown translucent cystic mass
- Cystic spaces often contain watery, thick or milky fluid (Hum Pathol 2005;36:426)
Contributed by Jeanne Meis, M.D.
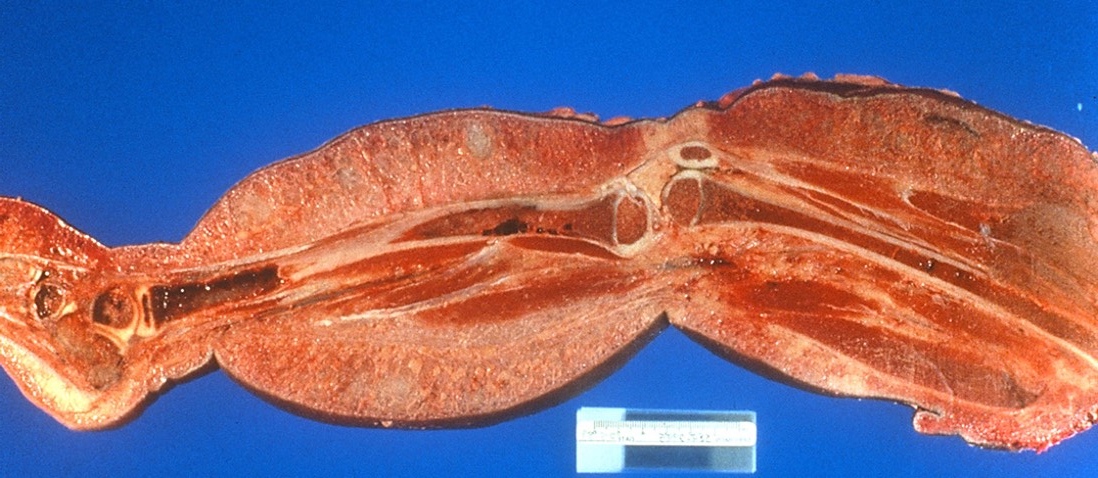
Resection of lymphangiomatosis

Mediastinal lymphangioma
Images hosted on other servers:

Splenic lymphangioma
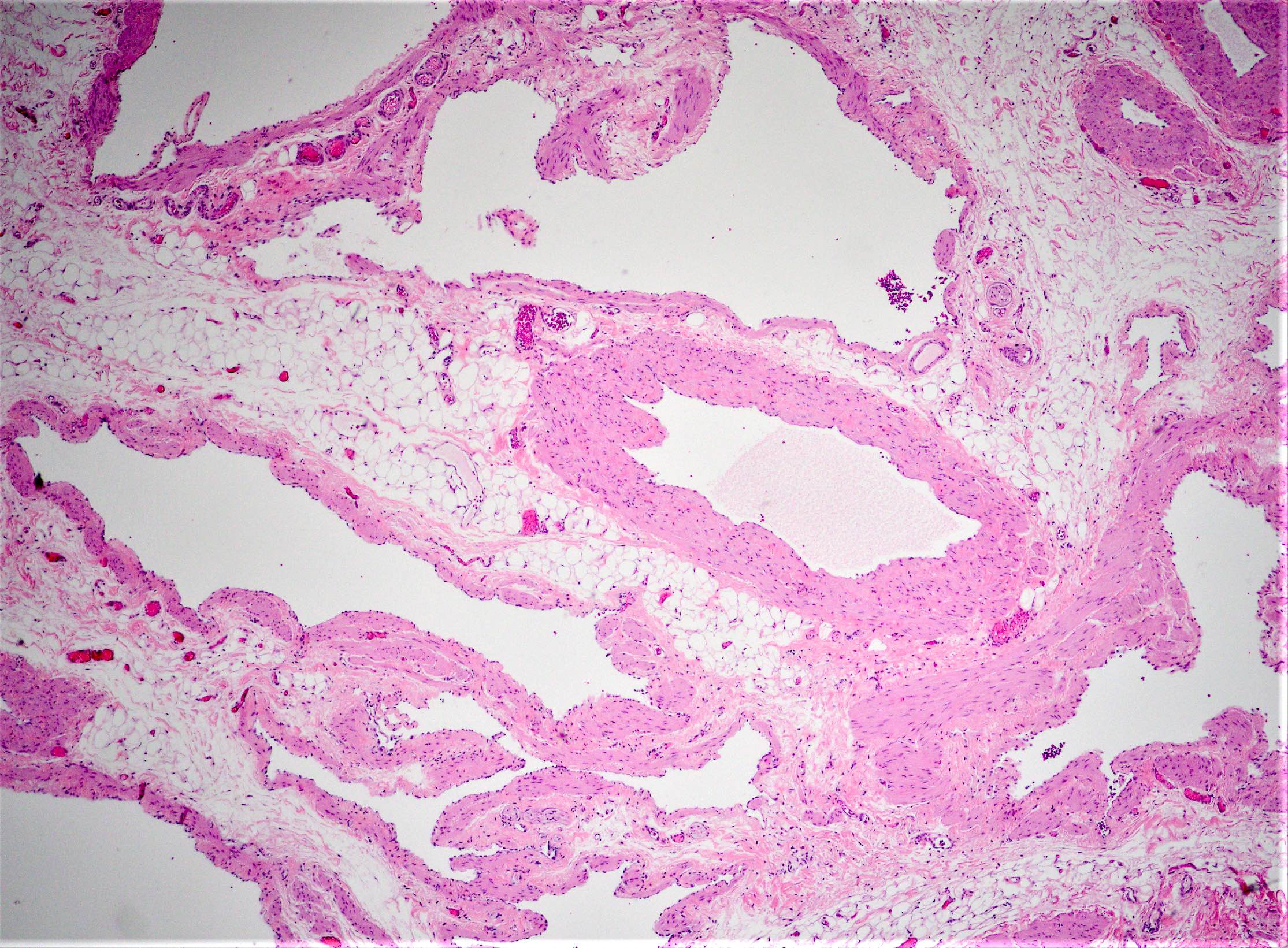
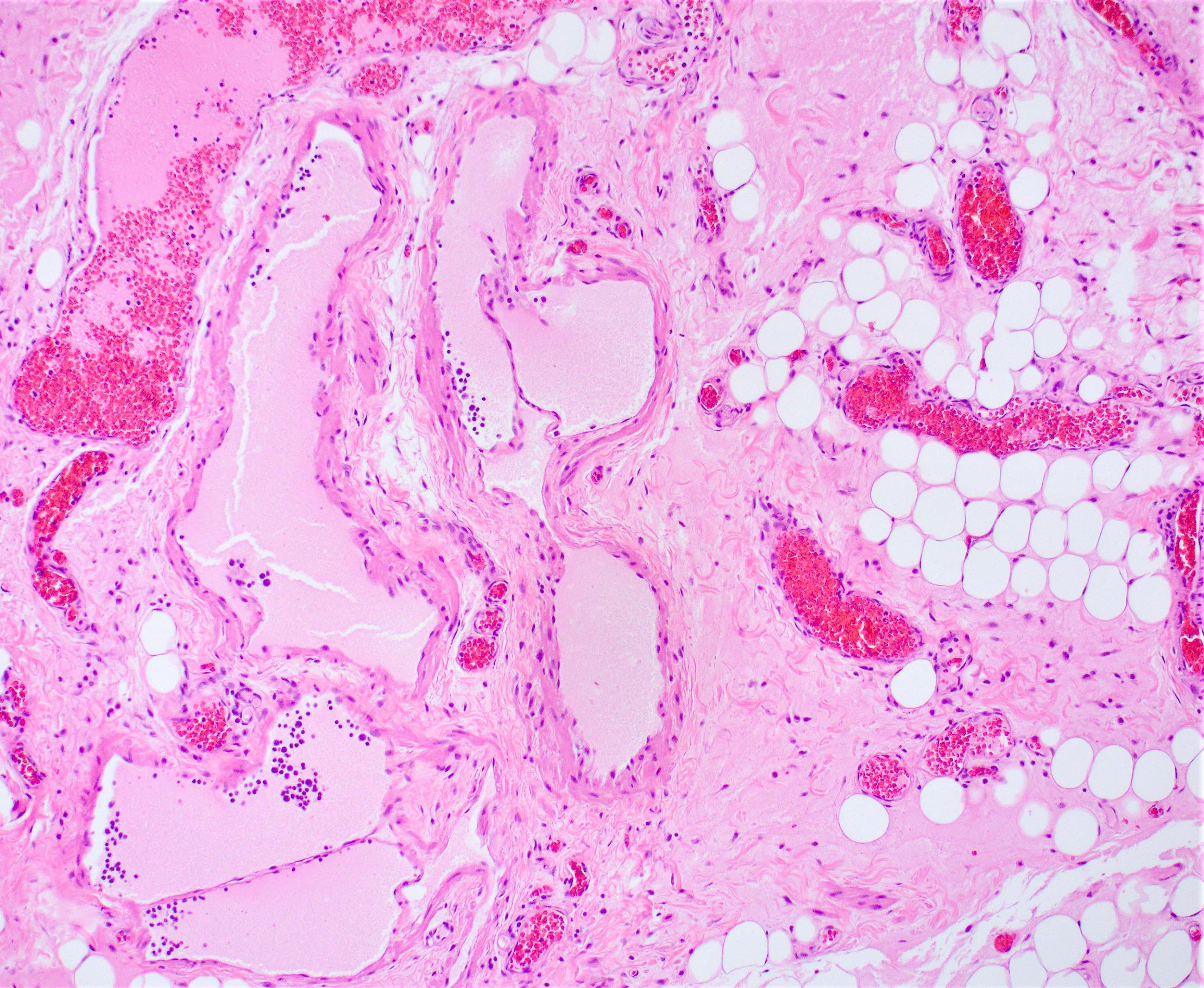
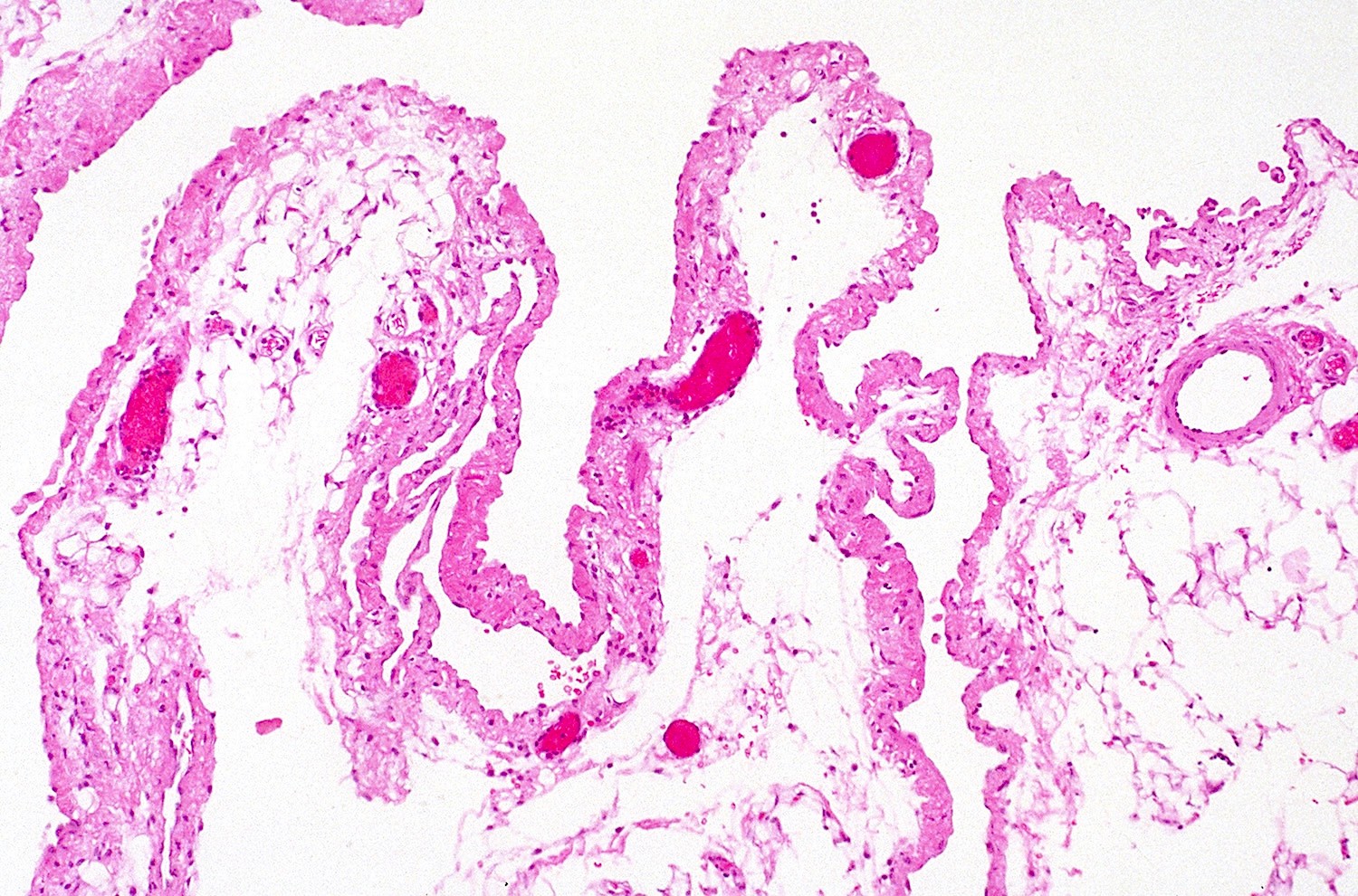
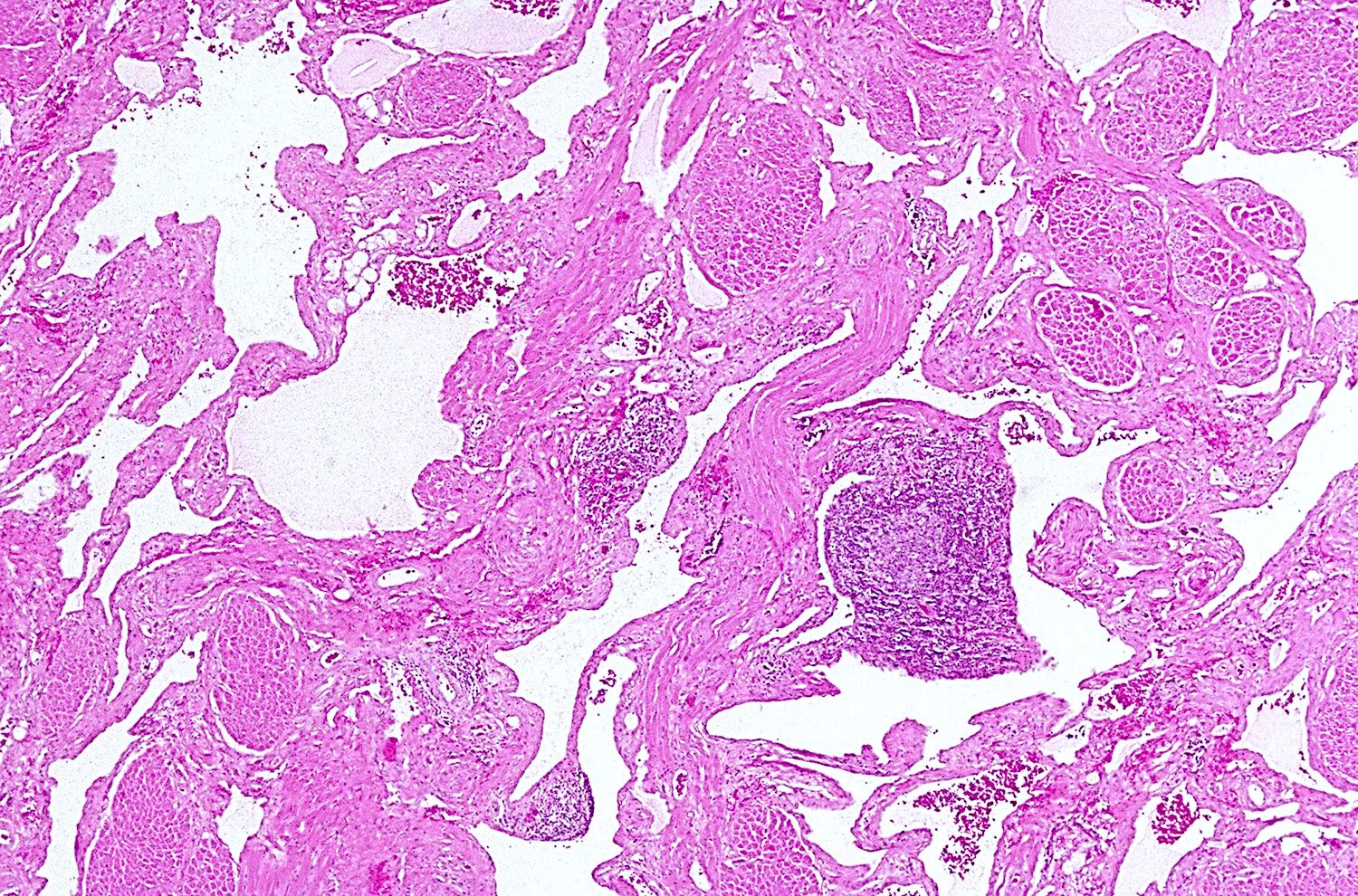
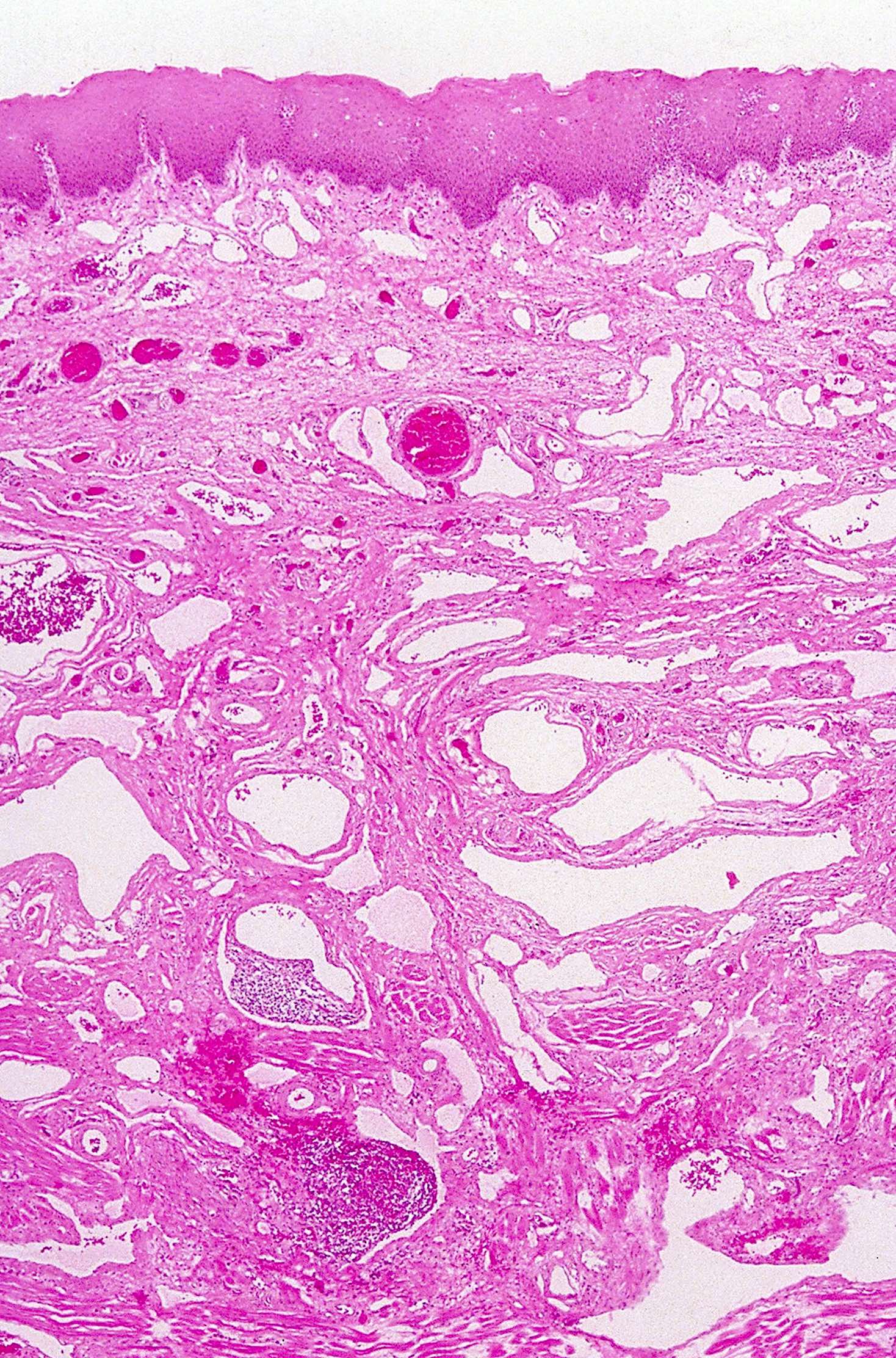
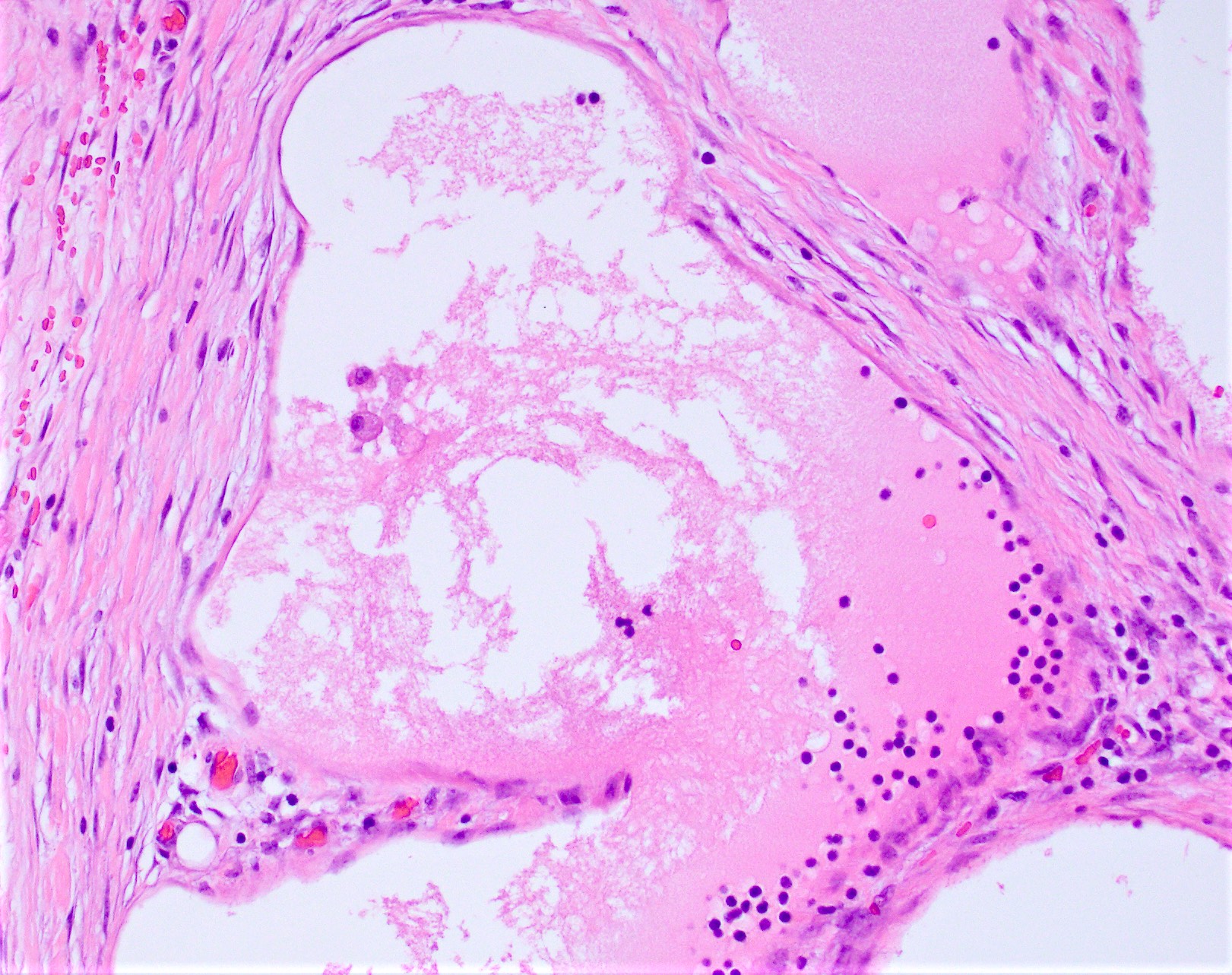
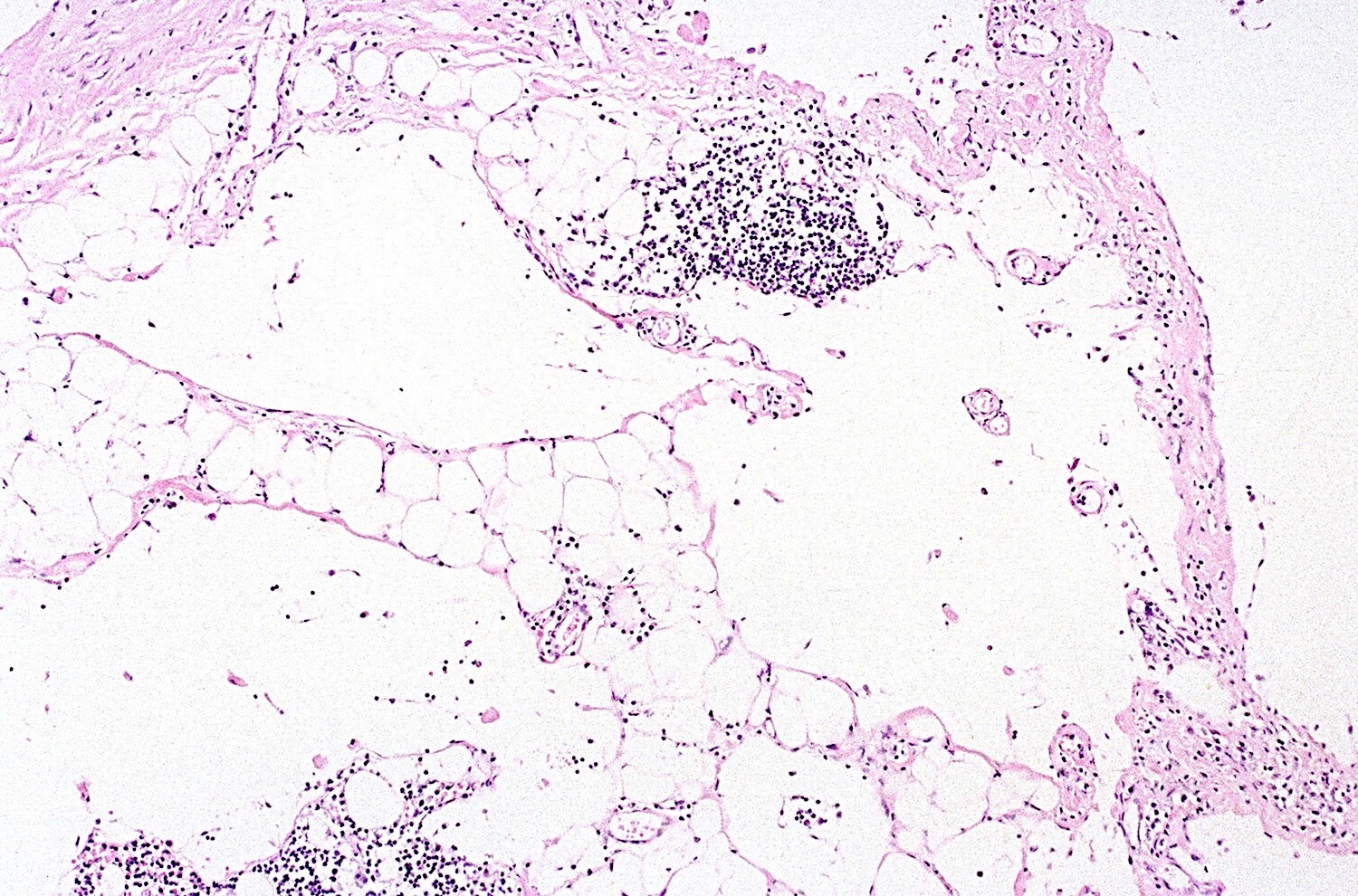
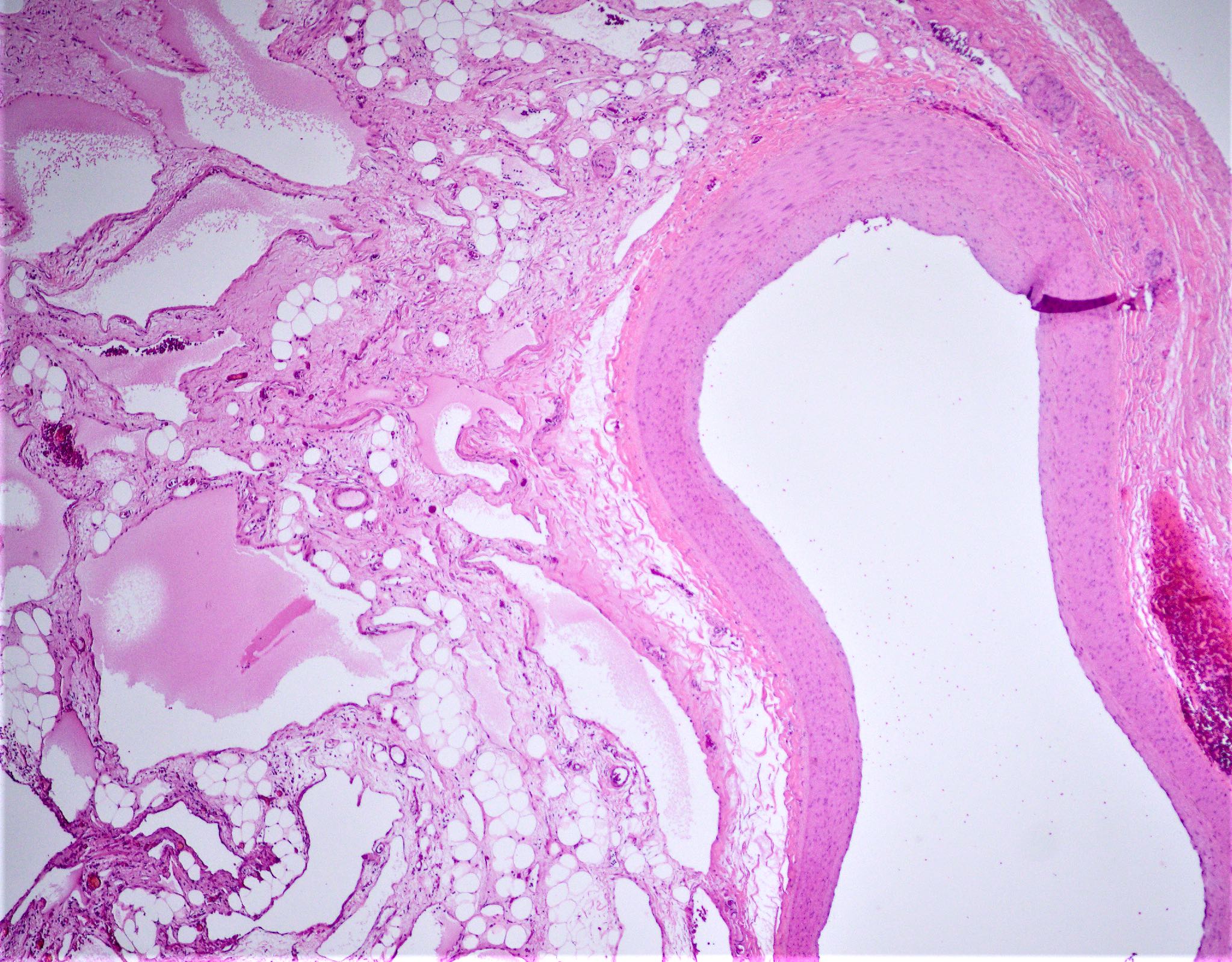
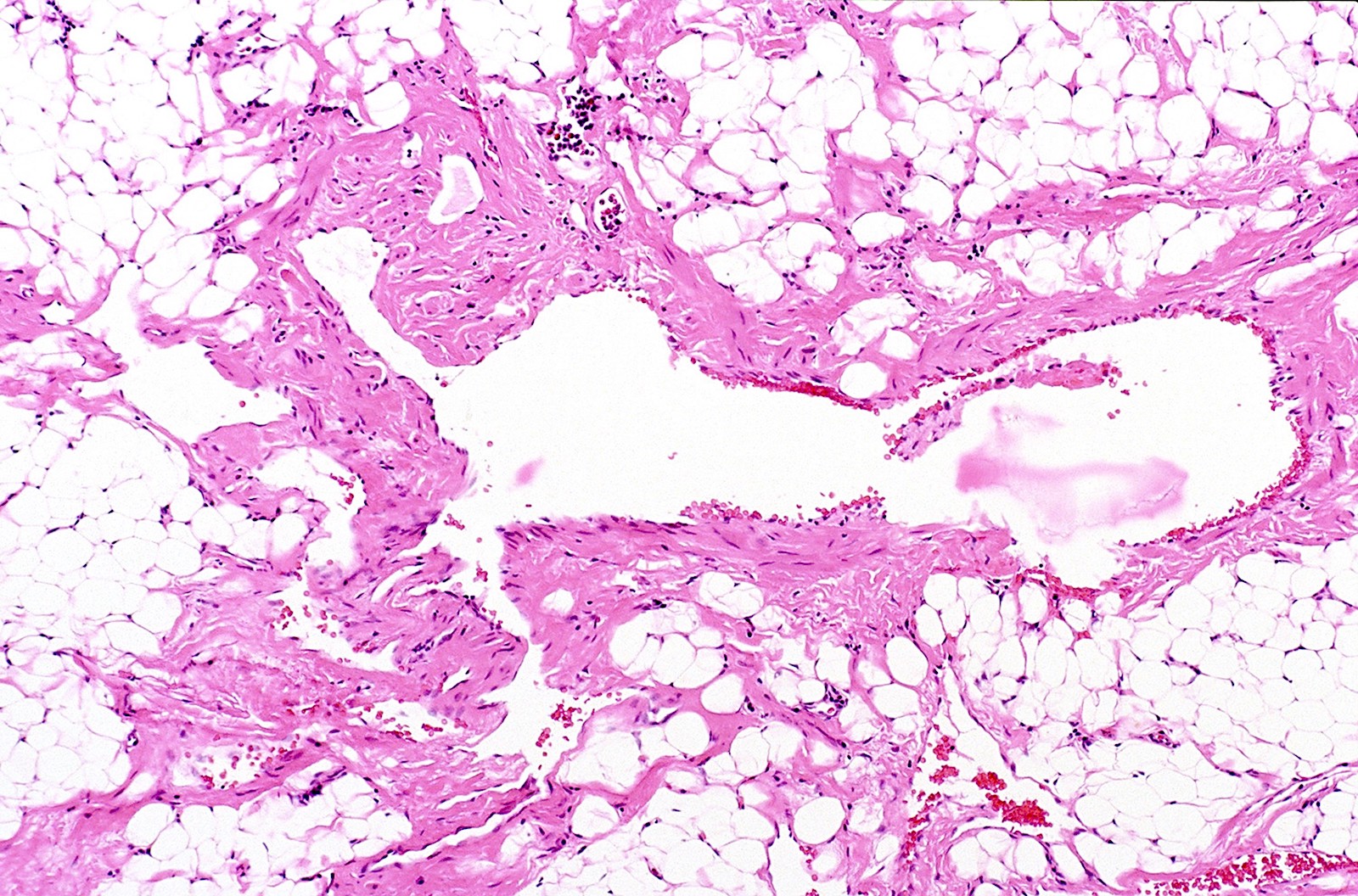
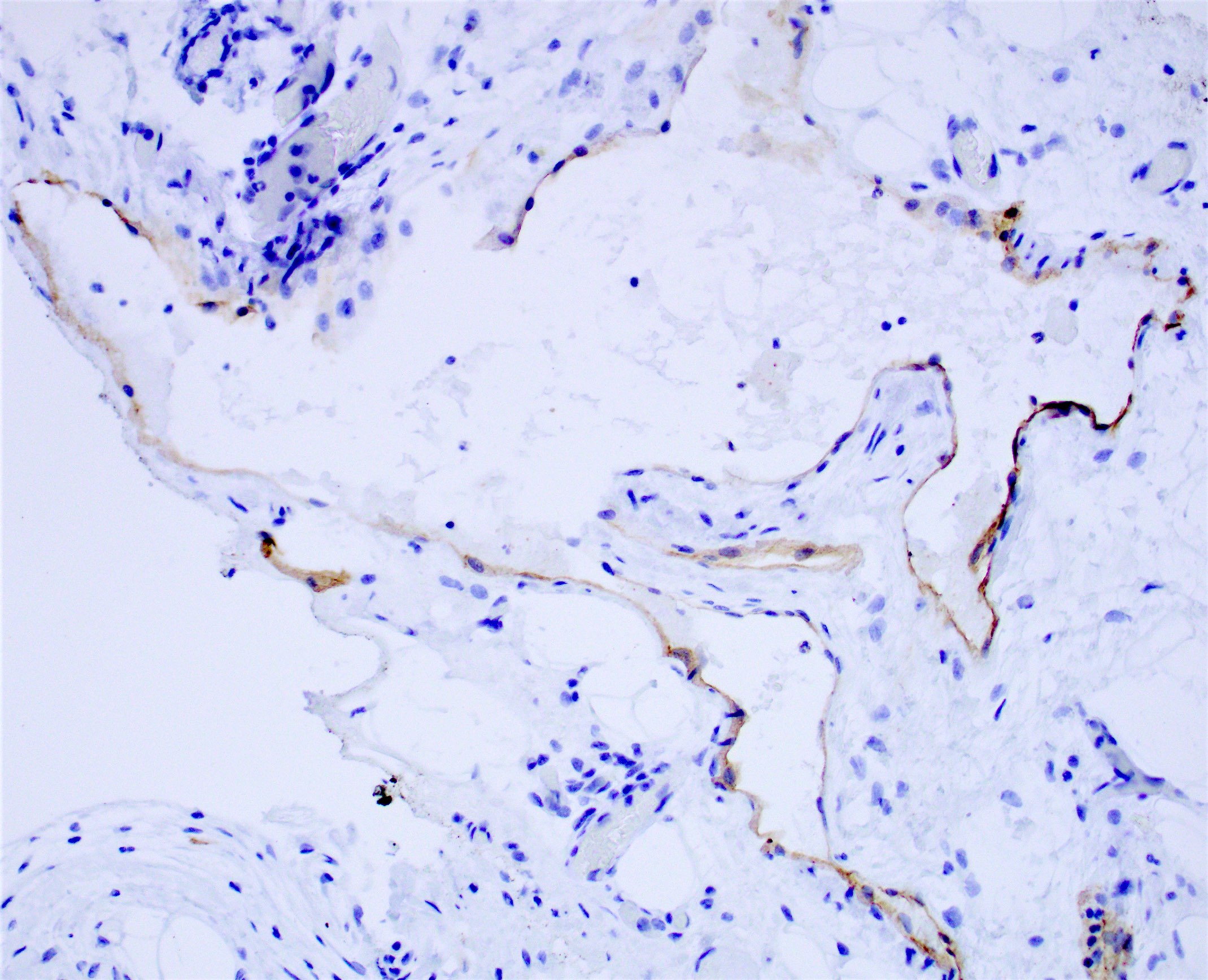
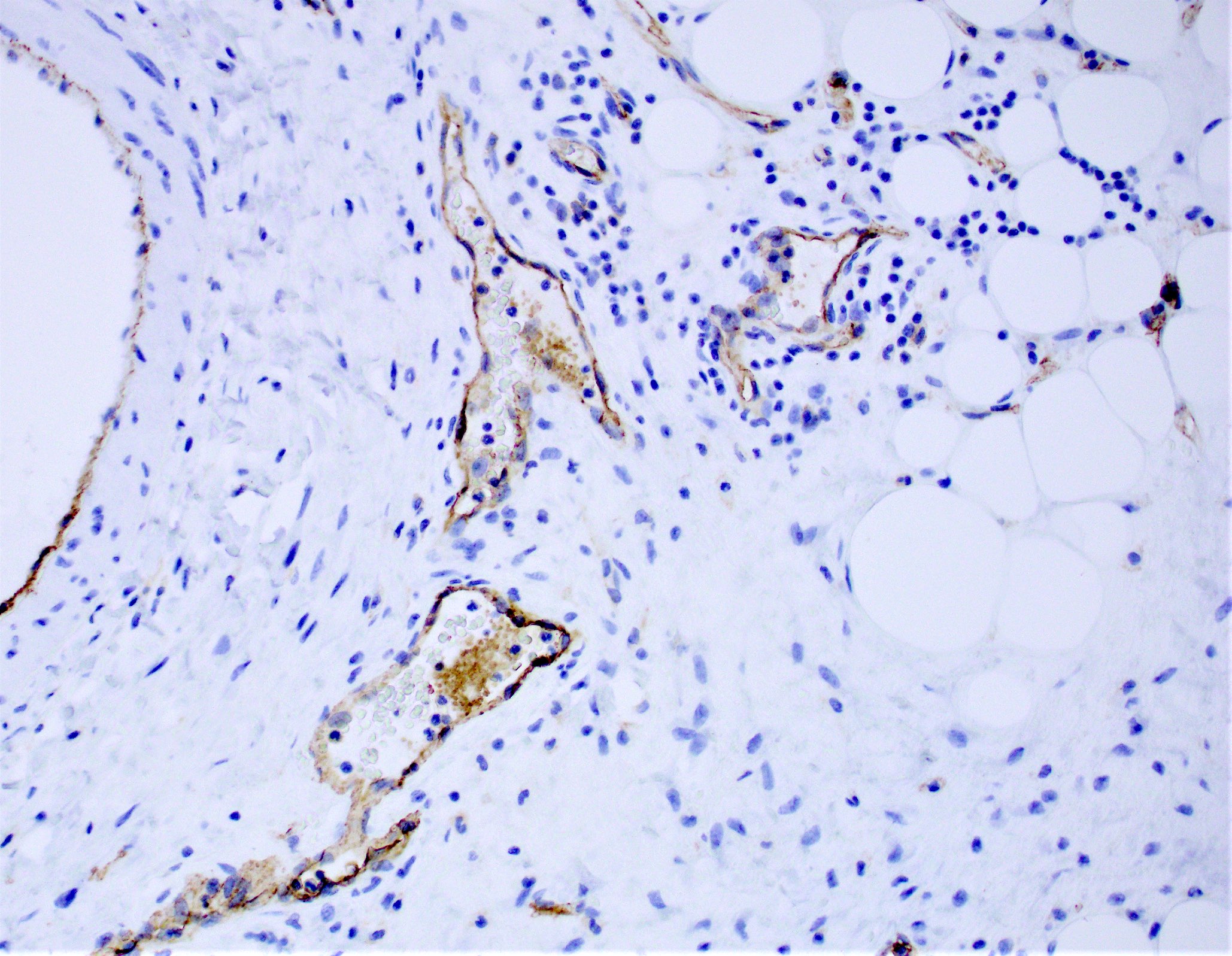
- Variably sized, thin walled, dilated lymphatic vessels lined by flattened endothelium
- Frequently surrounded by lymphoid aggregates, sometimes with reactive germinal centers
- Lumina may contain eosinophilic and amorphous proteinaceous fluid with occasional lipid laden macrophages and lymphocytes
- Longstanding lesions may show interstitial fibrosis
- Walls of larger vessels may contain smooth muscle
- Stromal mast cells and hemosiderin deposits are frequently seen
- Lining of the cysts may rarely form papillary projections
- Lymphangiomatosis frequently shows an anastomosing growth pattern, dissecting around normal structures
- Extensive granulation tissue and inflammation may obscure lymphatic nature (Hum Pathol 2005;36:426)
Contributed by Laura Warmke, M.D. and Jeanne Meis, M.D.
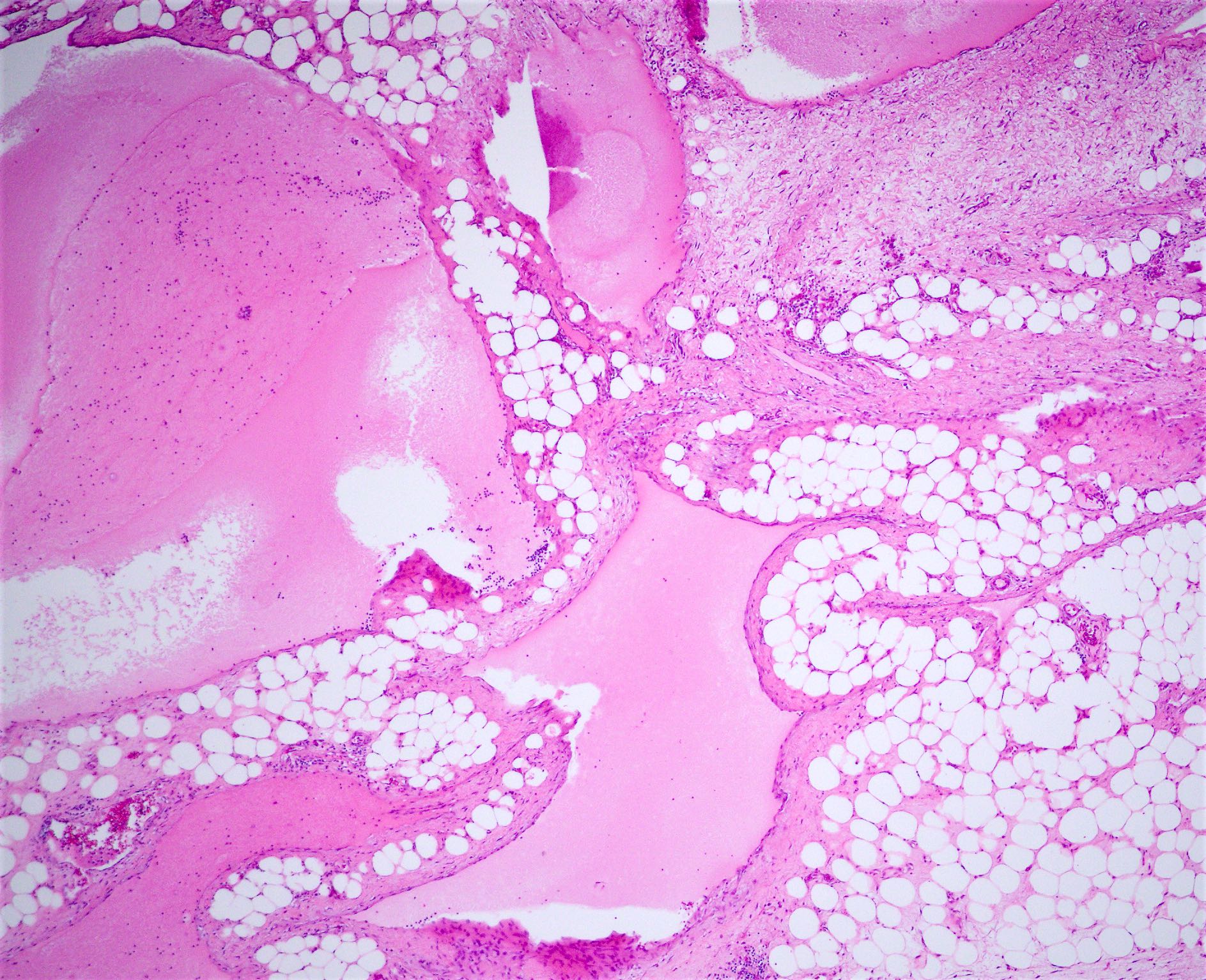
Dilated lymphatic spaces

Focal areas of fibrosis

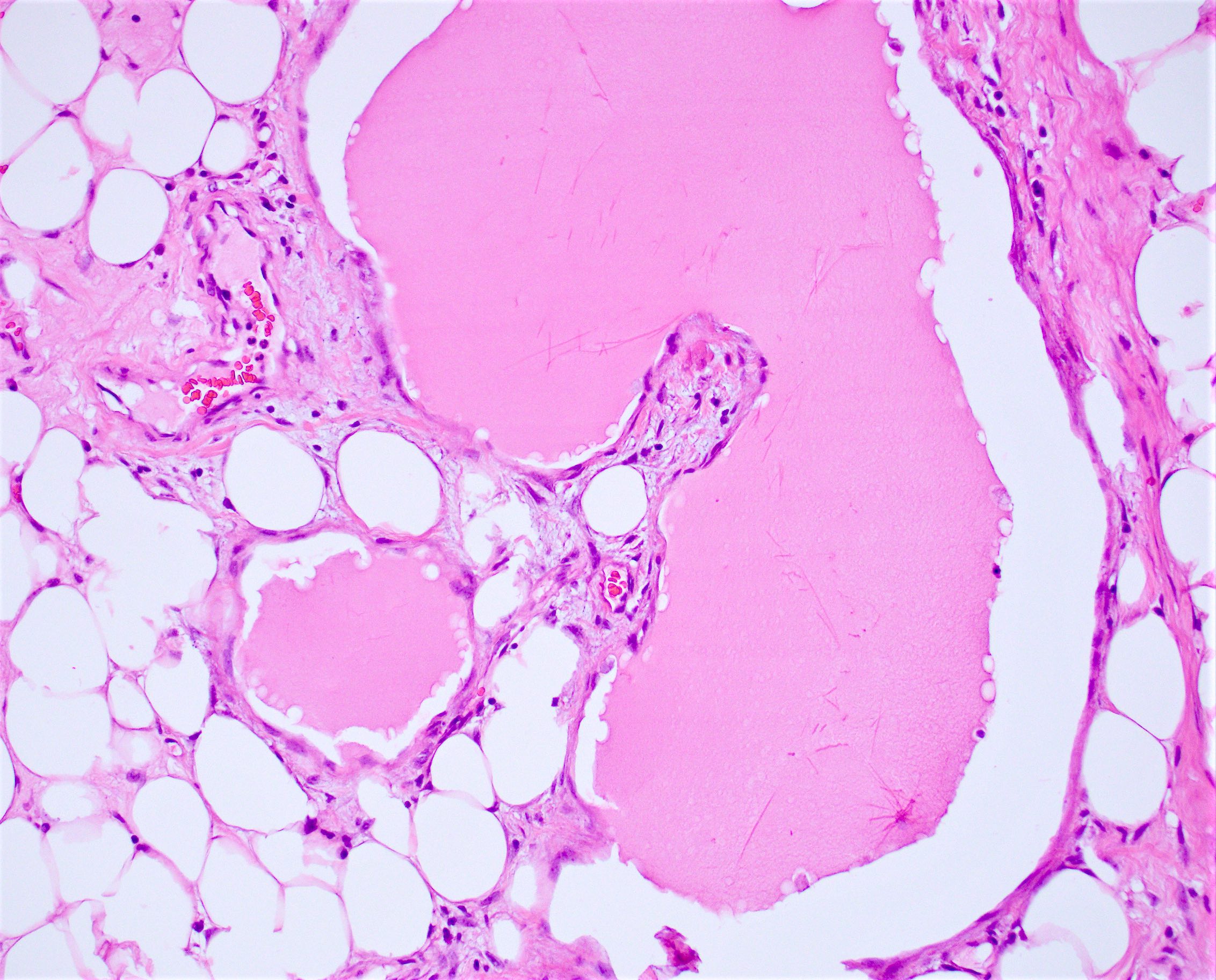
Proteinaceous fluid
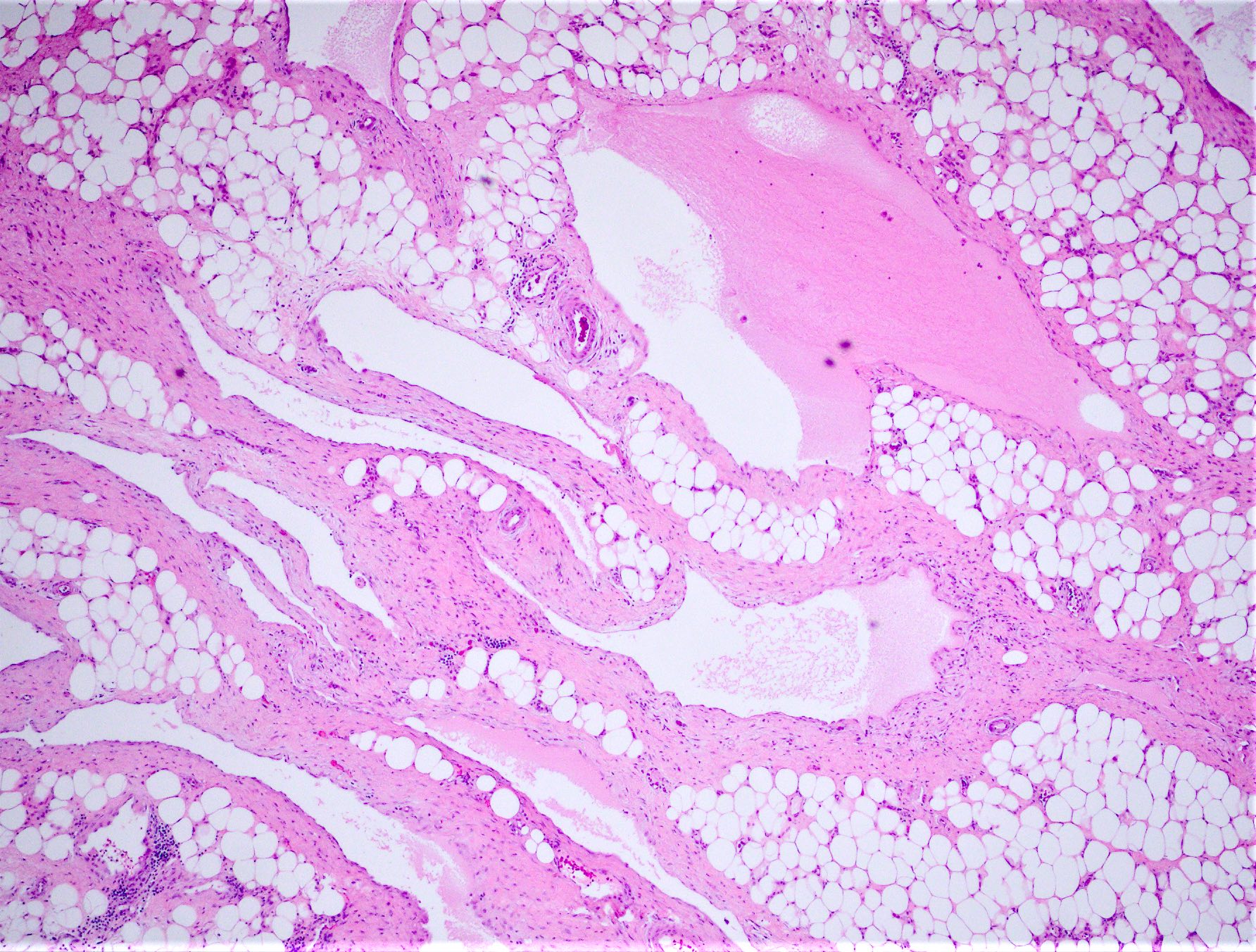
Lymphatic channels
Retroperitoneal lymphanagioma
Retroperitoneal lymphanagioma
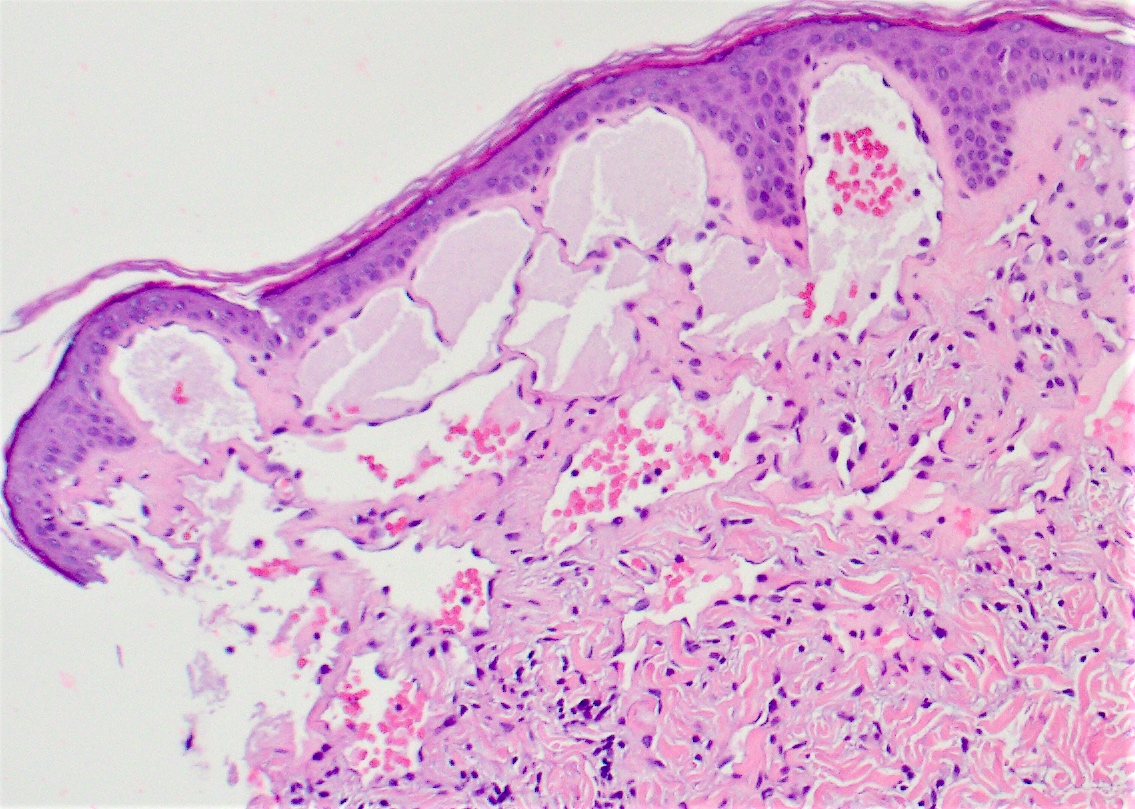
Lymphangioma circumscriptum
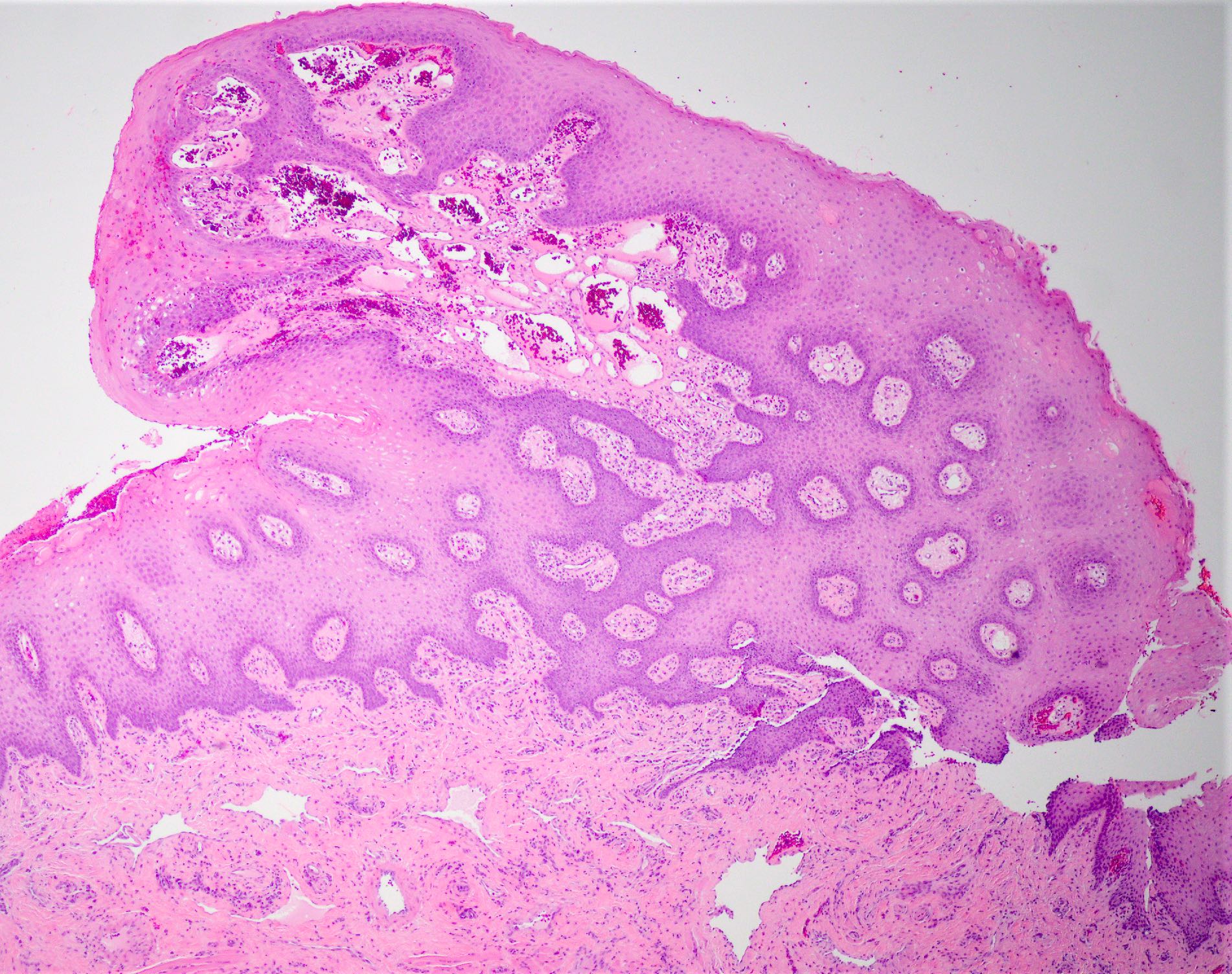
Lymphangioma of tongue
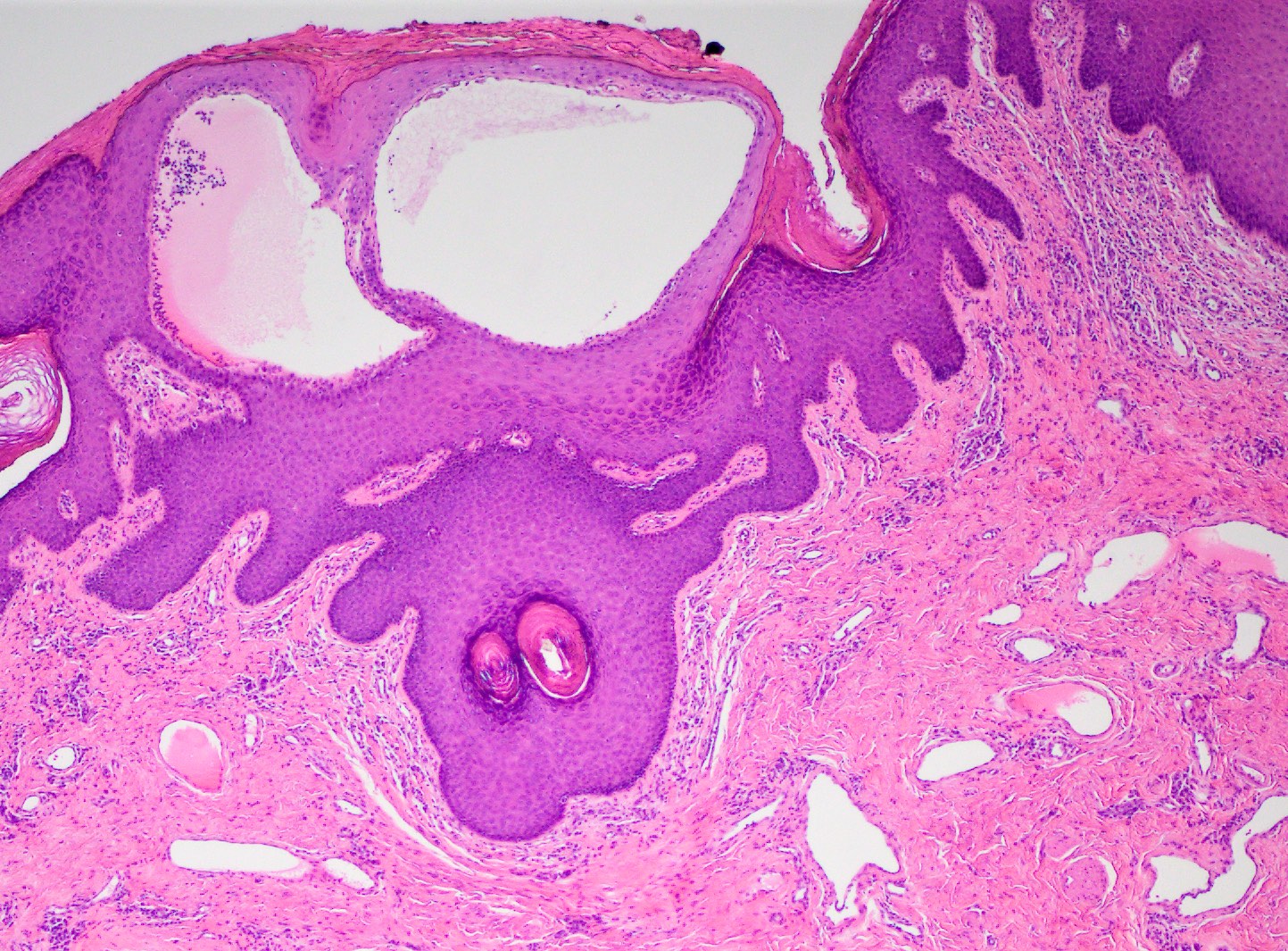
Superficial lymphangioma of vulva
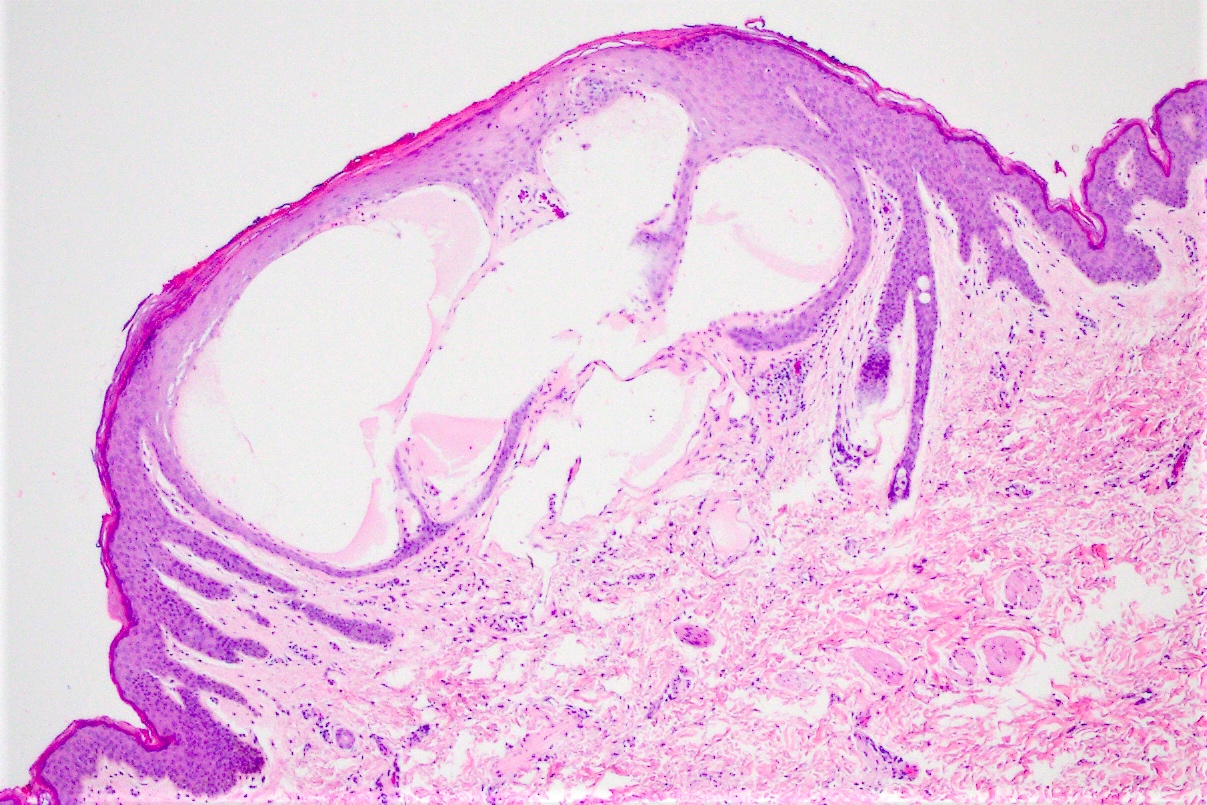
Superficial lymphangioma
Scattered macrophages
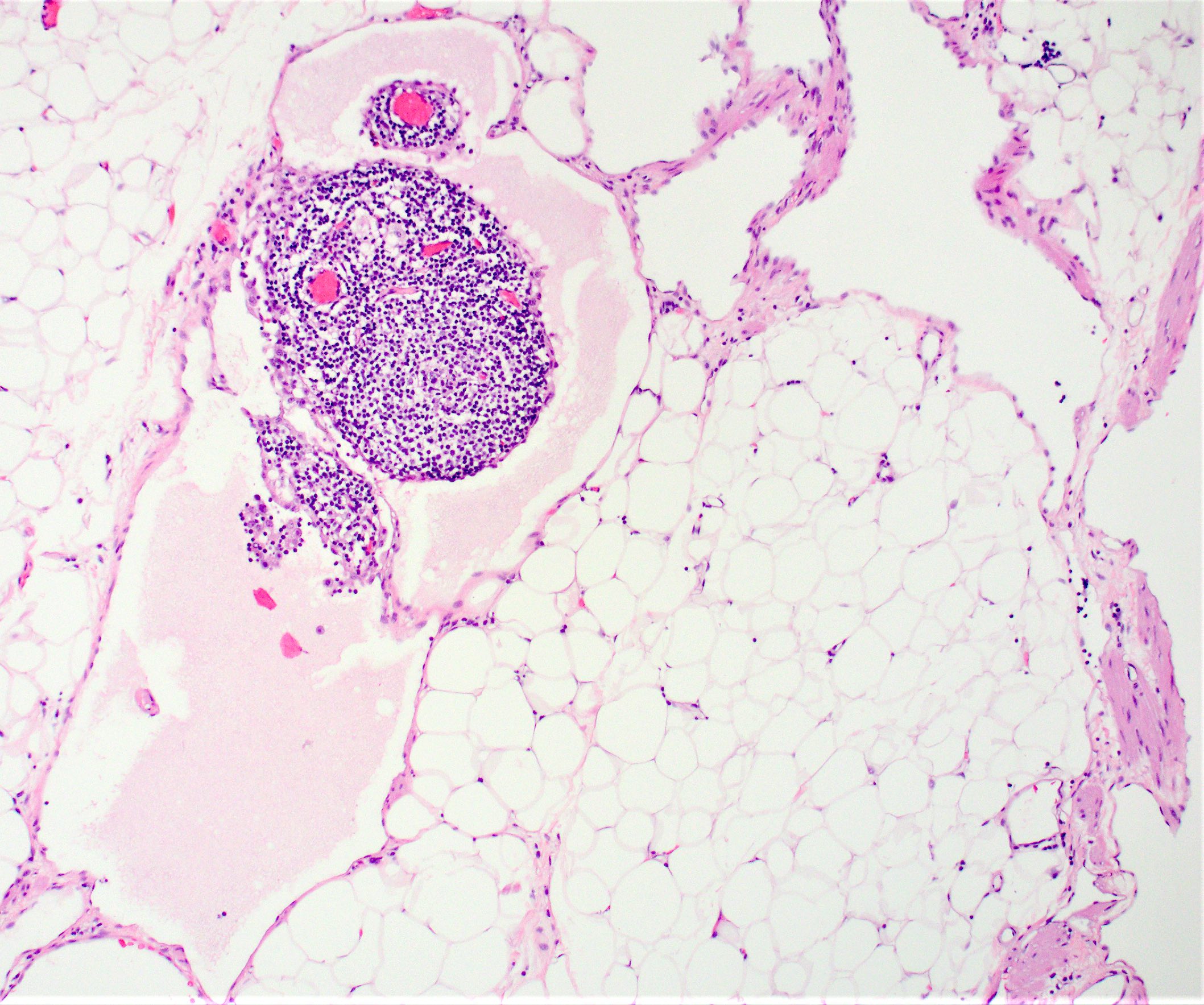
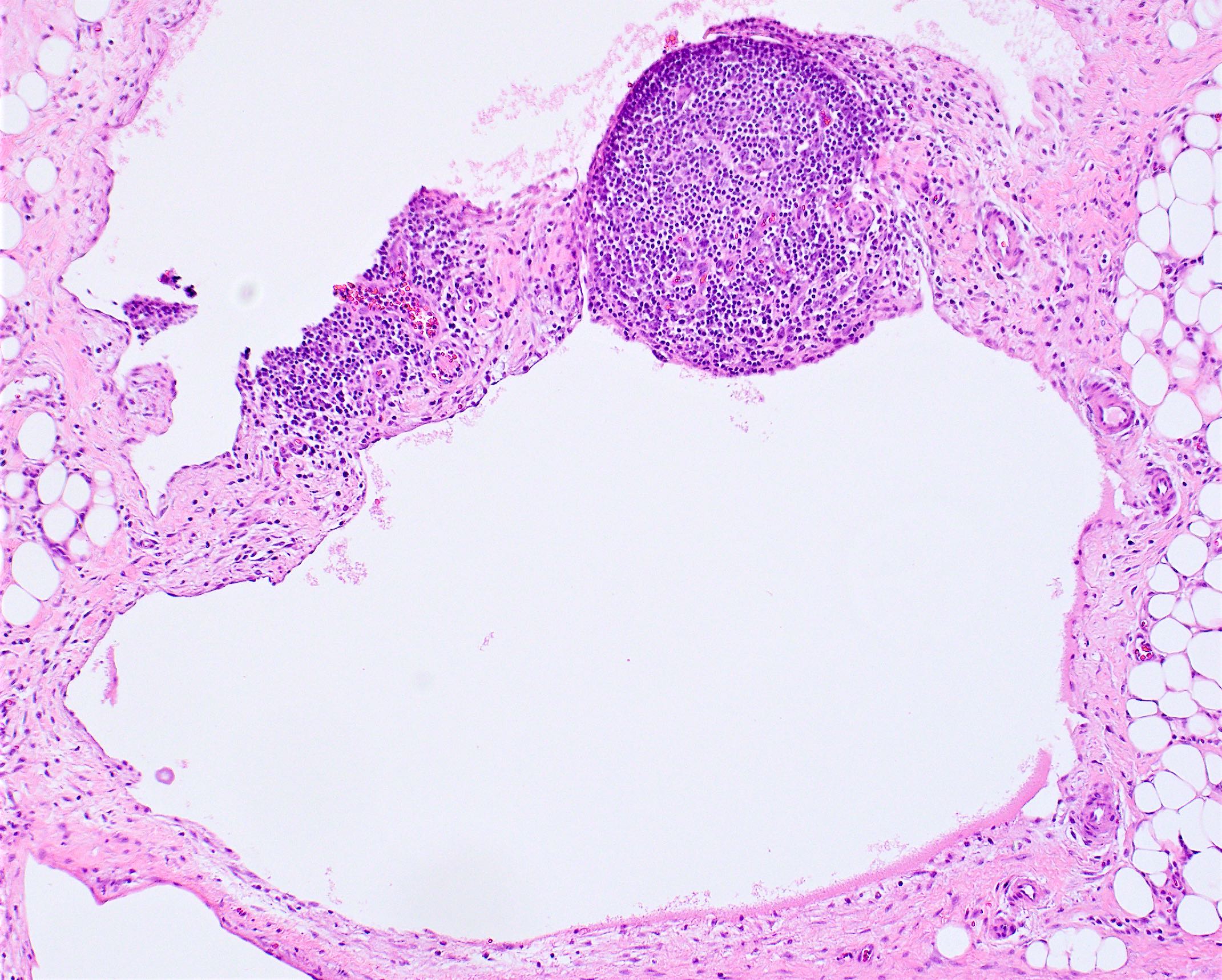
Lymphoid aggregate
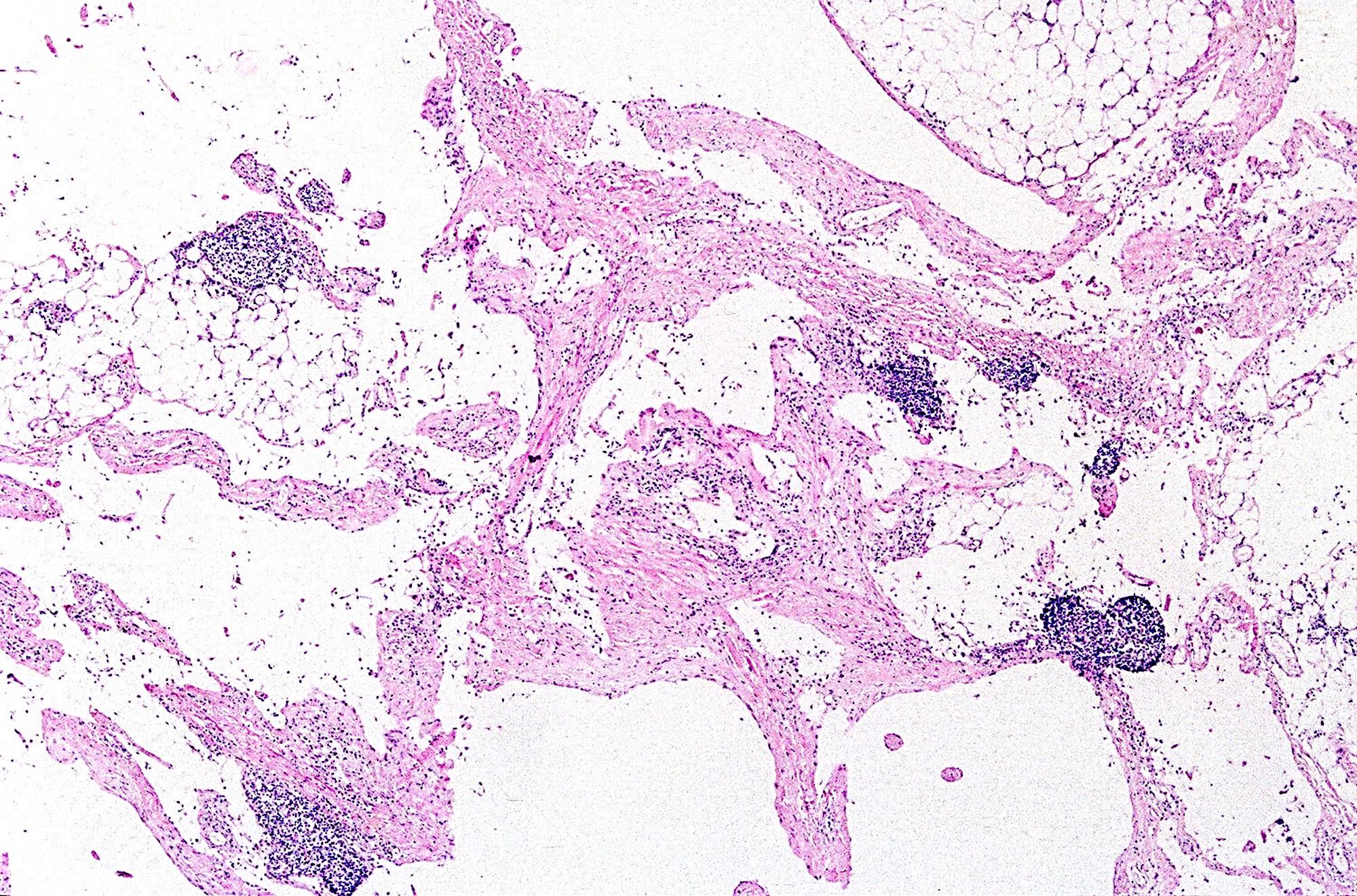
Lymphoid aggregates
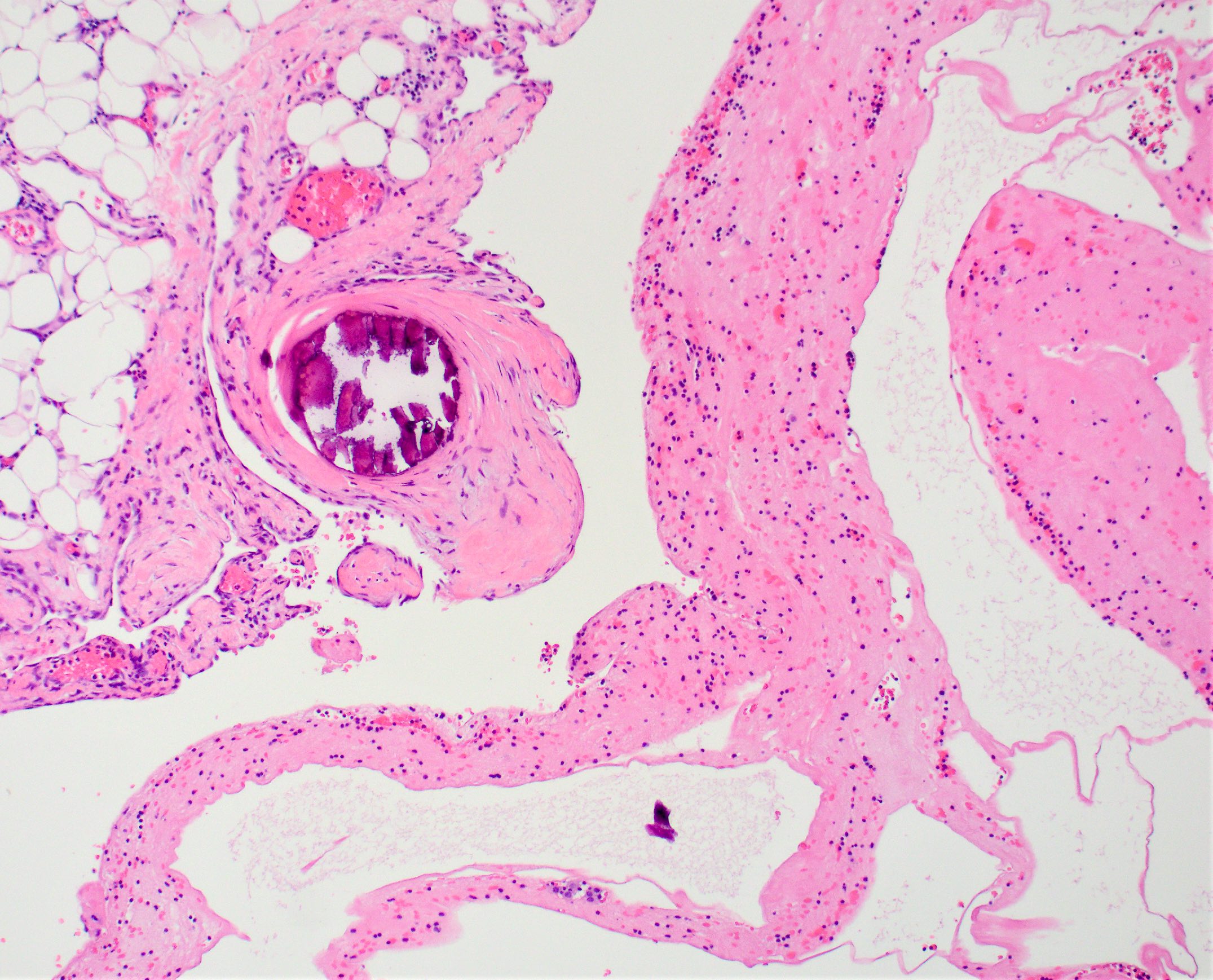
Calcification
Thick wall
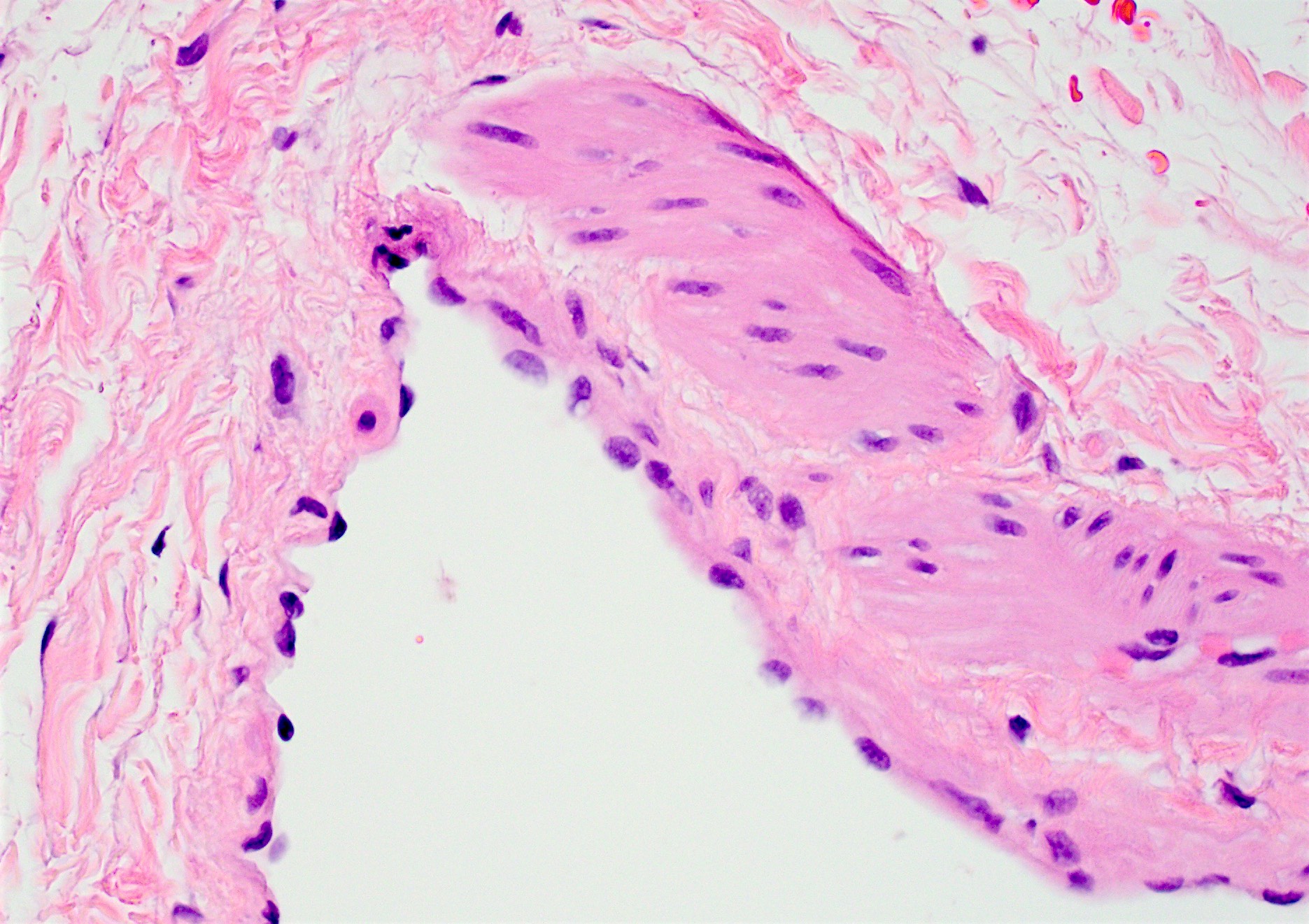
Endothelial lining
Irregular vascular channels
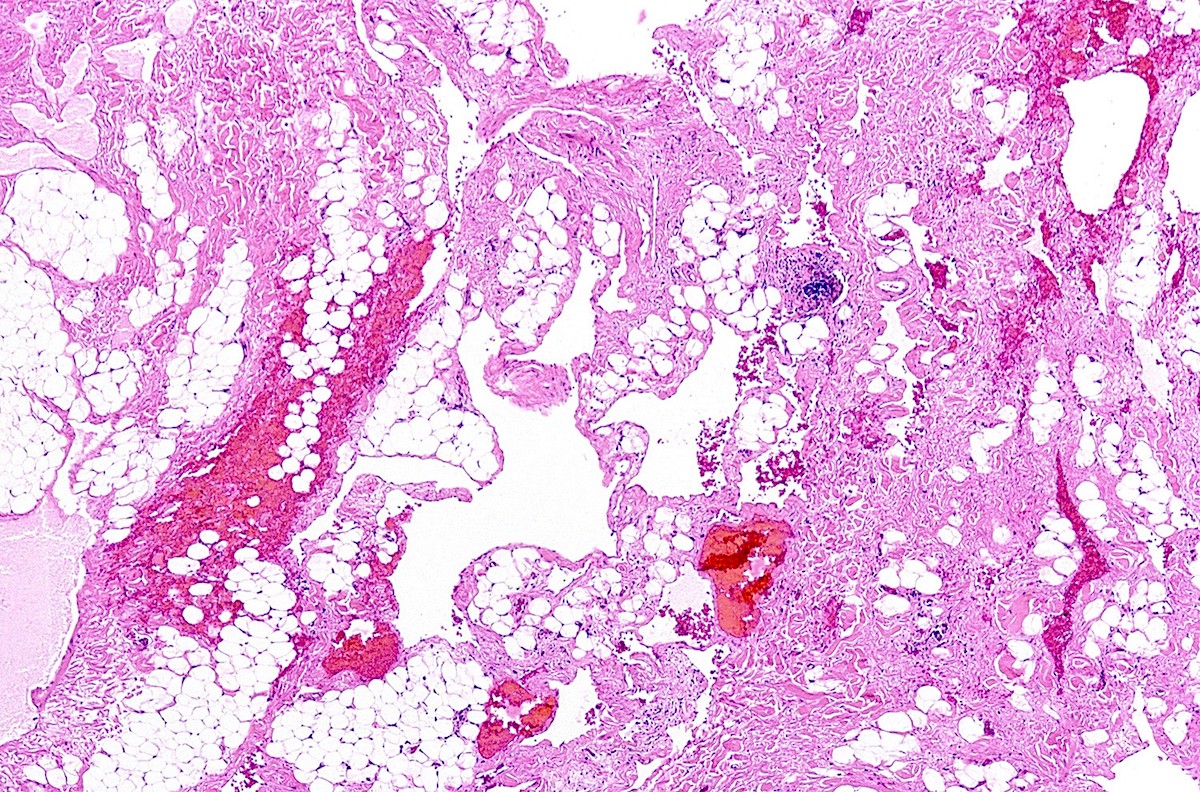
Irregular vascular channels
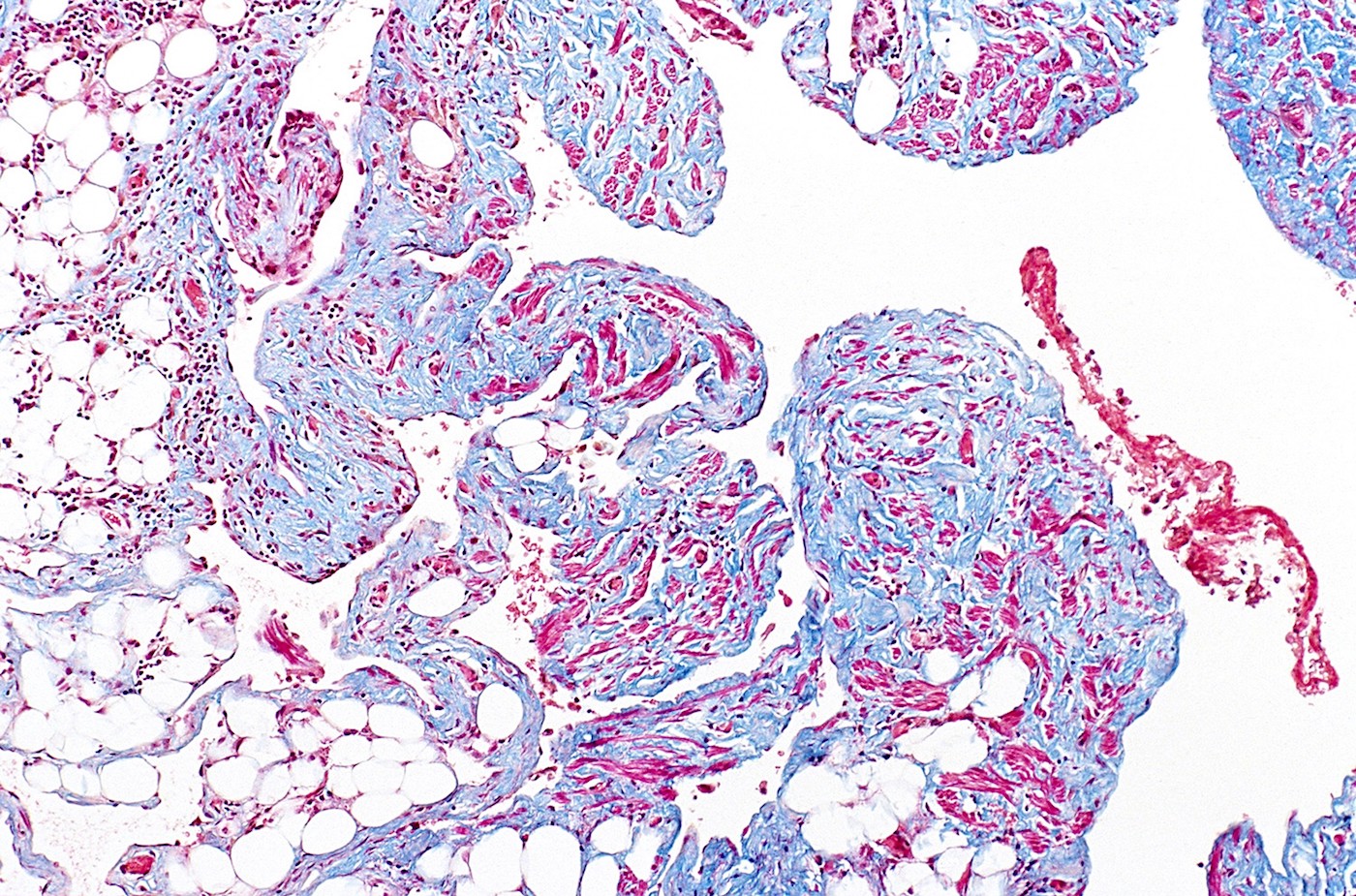
Trichrome stain
D2-40
CD31
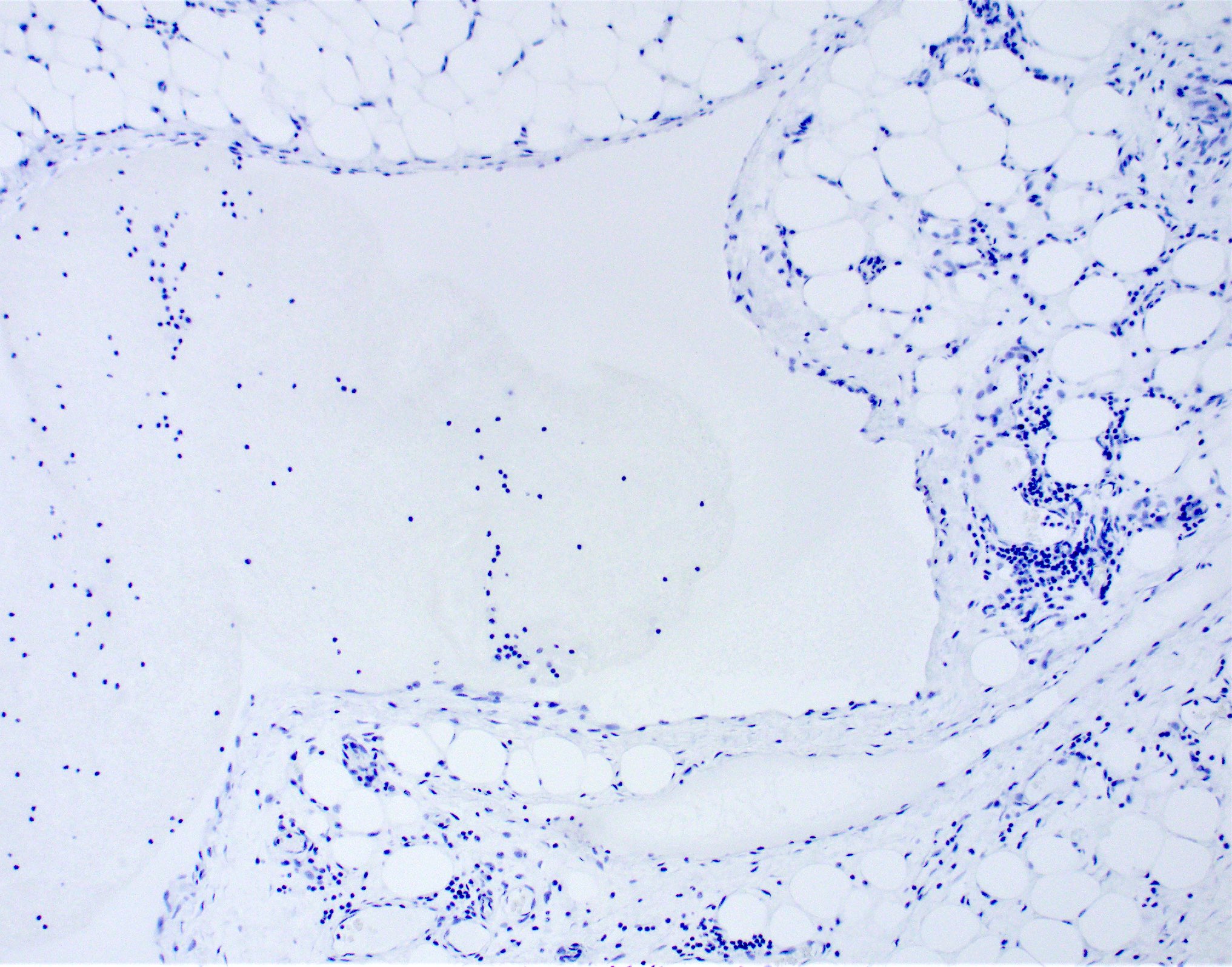
Cytokeratin
- Podoplanin (D2-40)
- PROX1 (Am J Surg Pathol 2012;36:351)
- Vascular endothelial growth factor receptor 3 (VEGFR3)
- Lymphatic endothelial hyaluron receptor 1 (LYVE1)
- CD31 and FVIII variable
- CD34 variable (Hum Pathol 2005;36:426)
- SMA positive in smooth muscle in larger vessels
- May assist in determining endothelial origin of cells lining the cysts
- Presence of Weibel-Palade bodies, storage granules of endothelial cells
- Increased expression of VEGFR3 (Virchows Arch 2008;453:1)
- Mutations in VEGFR3, FLT4, PROX1, FOXC2 and SOX18 may play a role
- Somatic mutations in PIK3CA have been reported (J Pediatr 2015;166:1048)
Lymphangioma (cystic hygroma)
- Soft tissue, retroperitoneal mass, resection:
- Cavernous lymphangioma (see comment)
- Comment: Sections show a lesion composed of dilated lymphatic spaces lined by flattened endothelium without cytologic atypia. Immunohistochemical stains show that the endothelial cells are positive for D2-40 and CD31, supporting a lymphatic nature, while they are negative for cytokeratin. These results, along with the morphologic features, support the above diagnosis.
- Hemangioma:
- Well circumscribed lesion
- Smaller vascular spaces extensively filled with red blood cells
- Vascular malformation:
- Often compressible
- May demonstrate a thrill or bruit
- Atypical vascular lesion:
- Radiation associated
- Frequently occurs in the breast
- Dilated vascular spaces with atypical endothelial cells
- Acquired progressive lymphangioma:
- Cutaneous vascular neoplasm
- Vessels dissect between collagen fibers
- Slow growing reddish brown patch or plaque
- Secondary lymphangiectasia:
- Secondary to lymphatic obstruction
- May be due to tumor, scarring or radiation
- Clinical history is helpful
- Cystic lymphangioma-like adenomatoid tumor (Adv Anat Pathol 2009;16:424):
- Mesothelial in origin
- Positive for cytokeratin and calretinin
- Ultrastructural finding of abundant long, slender microvilli
- Parasitic cyst (echinococcal cyst):
- No true epithelial / endothelial / mesothelial lining
- Protoscolices and refractile hooklets are often present
- Serologic test for Echinococcus are frequently positive
- Mesothelial cyst:
- Positive for cytokeratin and calretinin
- Negative for CD31
Cystic hygroma (cystic lymphangioma), which frequently involves the posterior triangle of the neck, is associated with which of the following syndromes?
- Down syndrome
- Klippel-Trenaunay syndrome
- Maffucci syndrome
- Turner syndrome
Which of the following immunohistochemical stains, when positive, is the most helpful in making the diagnosis of lymphangioma?
- Calretinin
- Cytokeratin
- D2-40
- GLUT1
