
Mediastinum
Other tumors
Germ cell tumors


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Germ cell tumors mediastinum

- Account for 1 - 15% of all mediastinal neoplasms in adults and 11 - 20% in children (J Thorac Oncol 2020;15:568, Ann Surg Oncol 1994;1:121)
- Classified as seminomas and nonseminomatous germ cell tumors (yolk sac tumor, embryonal carcinoma, choriocarcinoma, teratoma and mixed germ cell tumor)
- A seminoma with any component of a nonseminomatous tumor is considered a nonseminomatous germ cell tumor
- Mature teratomas and yolk sac tumors are almost exclusively the tumor types in very young patients
- Seminomas are almost always diagnosed in patients ≥ 10 years old
- Mixed mediastinal germ cell tumors more common in adults
- Majority occur in anterior mediastinum
- On CT, presence of fat is suggestive of their presence; however, fat fluid level or bone is pathognomonic of teratoma
- Immunoprofile of primary mediastinal germ cell tumors is similar to their gonadal counterparts
- Seminoma
- Nonseminomatous germ cell tumors (NSGCT) include yolk sac tumor, embryonal carcinoma, choriocarcinoma, teratoma and mixed germ cell tumor
- ICD-O:
- 9061/3 - seminoma
- 9070/3 - embryonal carcinoma
- 9071/3 - yolk sac tumor
- 9100/3 - choriocarcinoma
- 9080/0 - mature teratoma
- 9080/1 - immature teratoma of the thymus
- 9085/3 - mixed germ cell tumor
- 9084/3 - teratoma with somatic type malignancies
- 9086/3 - germ cell tumor with associated hematological malignancy
- Median age of mediastinal seminoma is 33 years, while NSGCT is 28 years (J Clin Oncol 2002;20:1864)
- Mature teratomas and yolk sac tumors are almost exclusively the tumor types in very young patients
- Seminomas are almost always diagnosed in patients aged ≥ 10 years (Pediatr Blood Cancer 2004;42:169)
- Mixed mediastinal germ cell tumors more common in adults
- M > F (Front Oncol 2020;10:1137)
- Benign teratomas have equal gender distribution
- Most common site is anterior (prevascular) mediastinum followed by posterior mediastinum (Front Oncol 2020;10:1137)
- Thought to arise from aberrant migration of primitive germ cells during embryonic development or from stem cells in thymus (Int J Androl 2007;30:256)
- Predilection for patients with Klinefelter syndrome (Int J Pediatr Endocrinol 2020;2020:18, Adv Anat Pathol 2021;28:335)
- Presence of chromosome 12p gains and isochromosome i(12p)
- May be metastases from testicular or ovarian primary
Gross, micro, IHC and serum markers of germ cell tumors
| Tumor type | Gross features | Microscopic features | Serum markers | Pankeratin | SALL4 | OCT3/4 | CD30 | Glypican 3 | Beta hCG | CD117 |
| Teratoma | Solid combined with cystic, Rokitansky protuberans contains shiny cartilage, hair and teeth, etc. | Derivatives of all 3 germinal layers | Beta hCG: normal LDH: normal AFP: normal | Positive in epithelial elements | Negative in mature components | Negative in mature components | Negative | Negative | Negative | Negative |
| Embryonal carcinoma | Gray-white with areas of hemorrhage and necrosis | Sheets and aggregates of highly pleomorphic cells | Beta hCG: normal LDH: raised AFP: raised | Positive | Positive | Positive | Positive | Negative | Negative | Negative |
| Yolk sac tumor | Gray-white with variable hemorrhage | Numerous growth patterns, Schiller-Duval bodies, eosinophlic globules | Beta hCG: normal LDH: normal AFP: raised | Positive | Positive | Negative | Negative | Positive | Positive in syncytio-trophoblasts | Negative |
| Chorio-carcinoma | Markedly hemorrhagic | Trimorphic population of trophoblasts with extensive hemorrhage | Beta hCG: raised LDH: normal AFP: normal | Positive | Positive | Negative | Negative | Negative | Positive in syncytio-trophoblasts | Negative |
| Seminoma | Gray-white, shiny cut surface | Islands of pleomorphic cells with prominent nucleoli, separated by thin fibrous septa having lymphocytes | Beta hCG: raised LDH: raised AFP: normal | Negative | Positive | Positive | Negative | Negative | Negative | Positive |
- Chest pain, cough, dyspnea, superior vena cava syndrome, weight loss, cervical mass, chest wall mass
- Lung involvement, liver and bone metastasis (Front Oncol 2020;10:1137)
- Clinical symptoms and elevated serum markers
- Radiological examination indicating a mass most commonly in anterior mediastinum
- Lactate dehydrogenase (LDH)
- Alpha fetoprotein (AFP)
- Beta human chorionic gonoadotropin (hCG)
- If the beta hCG is > 1,000, a nonseminomatous component may be present and should be evaluated (J Magn Reson Imaging 2010;32:1325)
- Highly malignant trophoblastic neoplasm composed of syncytiotrophoblasts, cytotrophoblasts and variable number of intermediate trophoblasts
Essential features
- Atypical and proliferating syncytiotrophoblasts and cytotrophoblasts with areas of hemorrhage and necrosis (J Cutan Pathol 2021;48:81)
- Immunoprofile positive for keratins, SALL4 and GATA3; hCG in syncytiotrophoblasts (Histopathology 2022;80:381)
ICD coding
- ICD-O: 9100/3 - choriocarcinoma
- ICD-11: 2C28.0 & XH8PK7 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & choriocarcinoma, NOS
Epidemiology
- Only 3% of mediastinal germ cell tumors are pure choriocarcinoma (J Thorac Cardiovasc Surg 1999;118:692)
- Almost all reported cases are in males
Sites
- Occurs in anterior mediastinum and posterior mediastinum (Ann Transl Med 2019;7:703)
Etiology
- Increased frequency in patients with Klinefelter syndrome (Ann Intern Med 1981;94:279, Int J Pediatr Endocrinol 2020;2020:18)
Clinical features
- Grow rapidly with early lung invasion
- Cough, shortness of breath, chest pain, superior vena cava syndrome
- Symptoms include gynecomastia due to hCG production
- May develop thyrotoxicosis due to TSH-like effects of hCG
- Extremely rare (Thorac Cancer 2014;5:463, BMJ Case Rep 2010;2010:bcr0220102712)
Diagnosis
- Radiological imaging with serum markers and biopsy or excision
Laboratory
- Elevated serum beta hCG levels
Radiology description
- Multiloculated cystic to solid hypodense masses which are highly vascular (J Taibah Univ Med Sci 2021;16:632)
Radiology images
Images hosted on other servers:

Mediastinal mass & metastatic lung nodules

Mass in posterior mediastinum
Prognostic factors
- Among NSGCTs, choriocarcinoma and embryonal carcinoma have the worst prognosis (J Surg Res 2021;267:25)
Case reports
- 25 year old man presented with cutaneous metastasis of primary mediastinal choriocarcinoma (J Cutan Pathol 2021;48:81)
- 26 year old man with primary mediastinal choriocarcinoma with diffuse metastasis to both lungs and multiple brain metastases (Medicine (Baltimore) 2019;98:e16411)
- 71 year old man on goserelin treatment for metastatic prostatic adenocarcinoma developed mediastinal choriocarcinoma with lung and vertebral metastases (Case Rep Pathol 2019;2019:2734815)
Treatment
- Chemotherapy, radiotherapy and surgery
- Treatment with cisplatin based therapy may improve the outcome
Gross description
- Large, soft, friable, extensively hemorrhagic and with foci of necrosis
Microscopic (histologic) description
- Intermingled syncytiotrophoblasts and cytotrophoblasts in a plexiform pattern or in disordered sheets
- Syncytiotrophoblasts, large multinucleated cells with numerous, pleomorphic, dark staining nuclei, variably distinct nucleoli and abundant densely eosinophilic or amphophilic cytoplasm
- Cytotrophoblasts, uniform, polygonal cells with round nuclei, prominent nucleoli and clear or eosinophilic cytoplasm
- Dilated vascular sinusoids
- Extensive areas of hemorrhage and necrosis
- Atypical mitoses and cellular atypia are common (J Cutan Pathol 2021;48:81, Mediastinum 2019;3:30)
- Mostly choriocarcinoma occurs as a component of mixed germ cell tumors (Arch Pathol Lab Med 2019;143:65)
Microscopic (histologic) images
Contributed by Sarosh Moeen, M.B.B.S.
Intermediate sized cells
Pankeratin (CK AE1 / AE3)
Cytology description
- Abundant necrosis and hemorrhage with clusters or isolated multinucleated syncytiotrophoblasts
Cytology images
Images hosted on other servers:

Transbronchial aspirate: syncytiotrophoblast
Positive stains
- Cytokeratins
- SALL4
- GATA3
- hCG, glypican 3, inhibin A: positive in syncytiotrophoblastic cells (Histopathology 2022;80:381)
Negative stains
Sample pathology report
- Anterior mediastinal mass, core biopsy:
- Germ cell tumor with morphological and immunohistochemical profile favoring choriocarcinoma (see comment)
- Comment: A possibility of mixed germ cell tumor in the vicinity cannot be excluded.
- Sarcomatous carcinoma with giant cells:
- Shows small to medium sized tumor cells with larger giant cells; this is in contrast with choriocarcinomas that show 2 cell populations of cytotrophoblasts and syncytiotrophoblasts
Differential diagnosis
- Malignant nonseminomatous germ cell tumor characterized by embryonal type cells
ICD coding
- ICD-O: 9070/3 - embryonal carcinoma
- ICD-11: 2C28.0 & XH8MB9 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & embryonal carcinoma, NOS
Epidemiology
- Accounts for 2 - 8% of primary mediastinal germ cell tumors (Cancer 2003;97:367)
- Predominantly in young males
Sites
- Occurs in anterior mediastinum
Etiology
- Same as other nonseminomatous germ cell tumors
Clinical features
- Chest pain, dyspnea, cough and superior vena cava syndrome
Diagnosis
- Mediastinal mass on radiology and subsequent biopsy
Laboratory
- Elevated LDH and AFP levels
Radiology description
- Large, lobulated, heterogeneous mass with hemorrhage, necrosis and calcifications on CT scan
- On MRI, cystic or necrotic areas appear hyperintense on T2 weighted images
- FDG PET useful in evaluation of recurrent disease or residual viable tumor after chemotherapy (AJR Am J Roentgenol 2010;195:W274)
Radiology images
Images hosted on other servers:

Expansion of tumor; heterogeneously enhanced
Prognostic factors
- Among NSGCTs, choriocarcinoma and embryonal carcinoma have the worst prognosis (J Surg Res 2021;267:25)
Case reports
- 12 year old boy with large soft tissue mass in mediastinum and left thoracic cavity, diagnosed as malignant mixed germ cell tumor with yolk sac tumor, immature teratoma and embryonal carcinoma components (Open Med (Wars) 2021;16:892)
- 23 year old man with anterior mediastinal mass and right pleural effusion developed pericardial effusion and cardiac tamponade (AJR Am J Roentgenol 1998;170:722)
- 25 year old man with an unresectable embryonal carcinoma of the anterior mediastinum that developed a bronchial fistula after systemic chemotherapy (Case Rep Radiol 2020;2020:7650206)
- 29 year old man with primary mediastinal embryonal carcinoma presented with pulmonary artery stenosis (Pneumonol Alergol Pol 2015;83:151)
Treatment
- Chemotherapy and surgical resection (Nagoya J Med Sci 2014;76:225)
Gross description
- Infiltrating and large with size up to 22 cm
- Hemorrhagic and necrotic cut surface
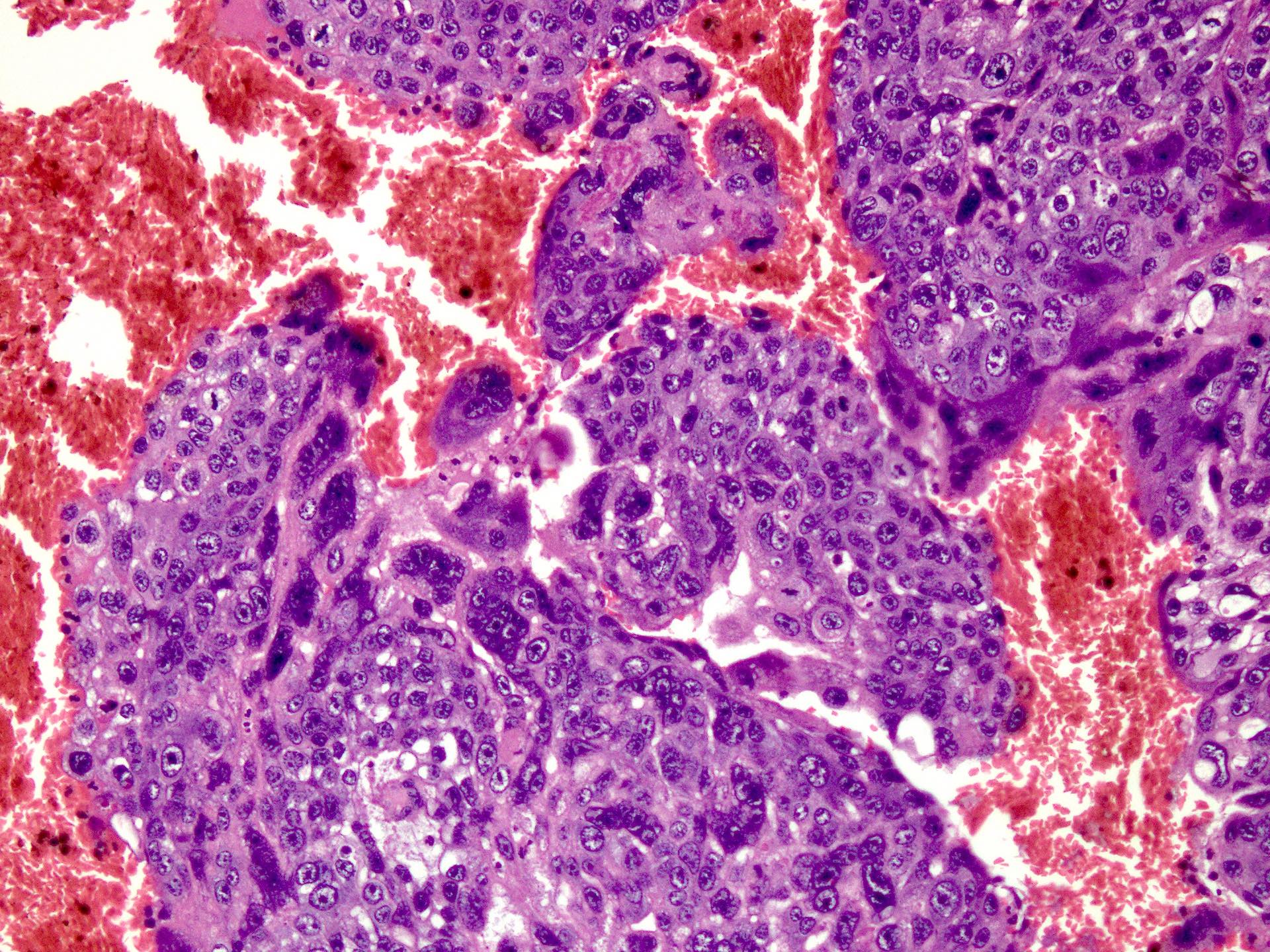
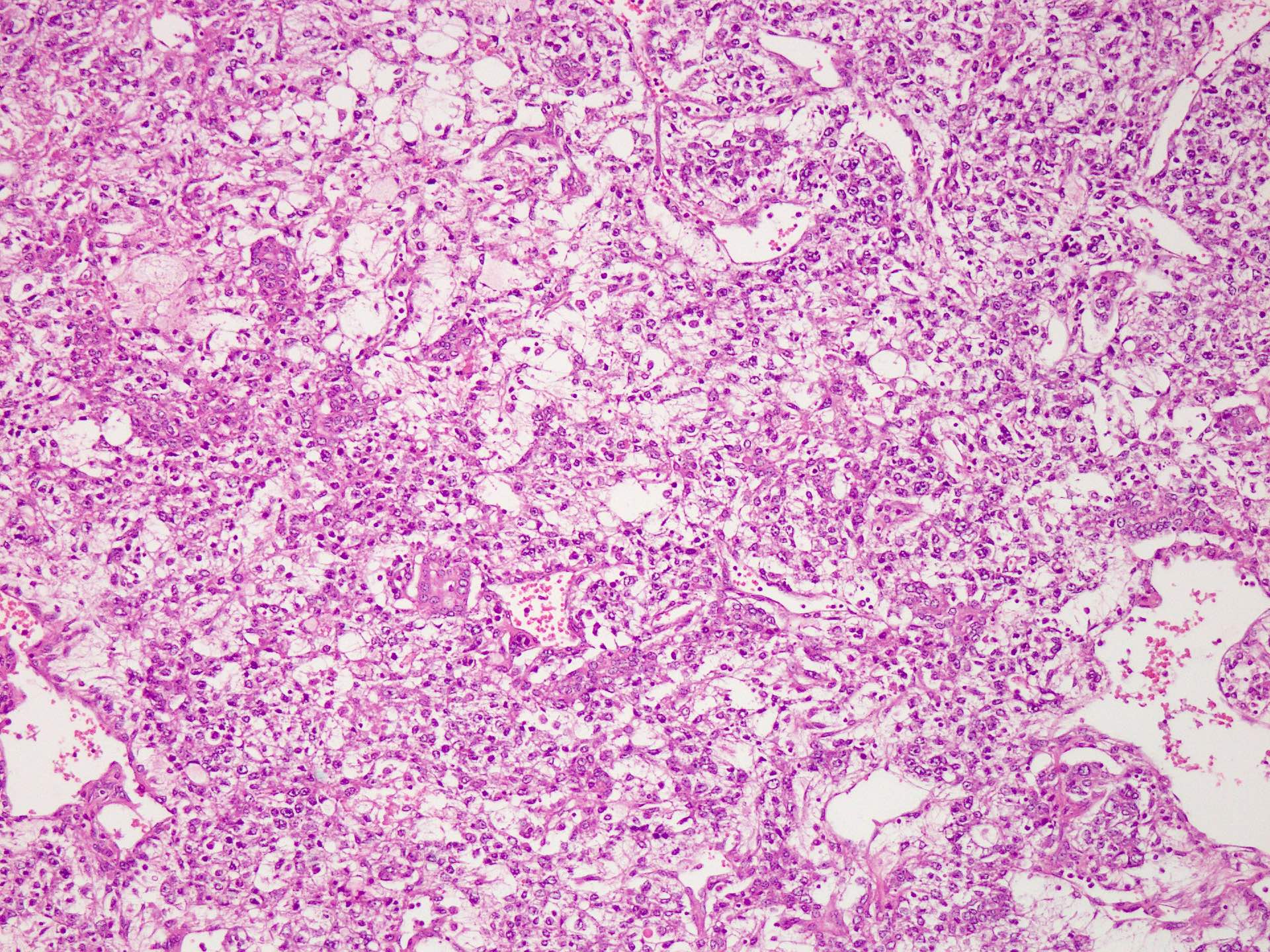
Microscopic (histologic) description
- Large and polygonal cells sometimes columnar with indistinct cell borders
- Eosinophilic, amphophilic, basophilic or clear cytoplasm
- Nuclei have large single or multiple nucleoli (Histopathology 2022;80:381)
- Numerous mitoses, often atypical
- Solid, tubular / glandular or papillary growth patterns
- Tumor necrosis is common (Mediastinum 2019;3:30)
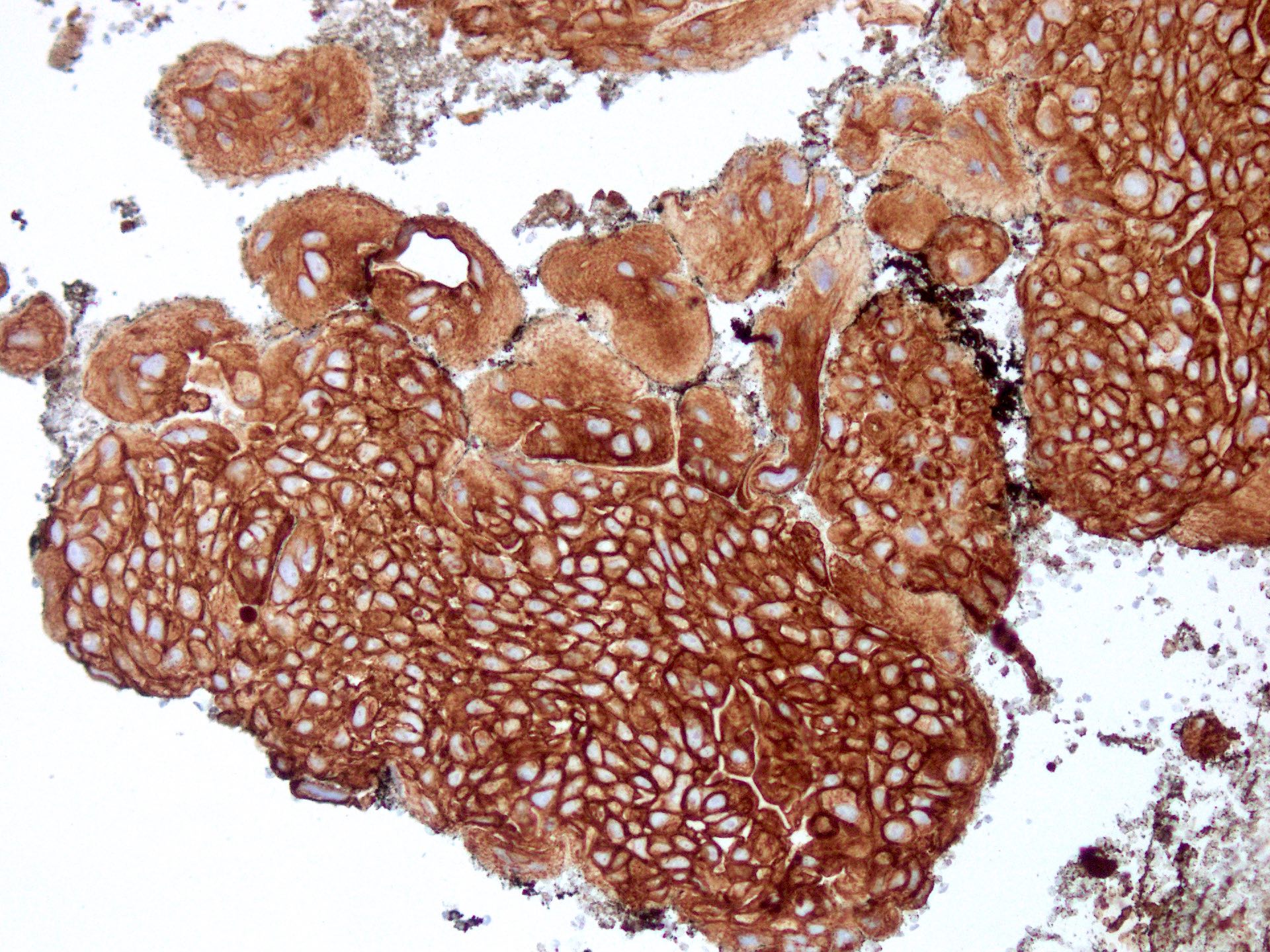
Microscopic (histologic) images
Contributed by Sarosh Moeen, M.B.B.S.
Islands of tumor cells
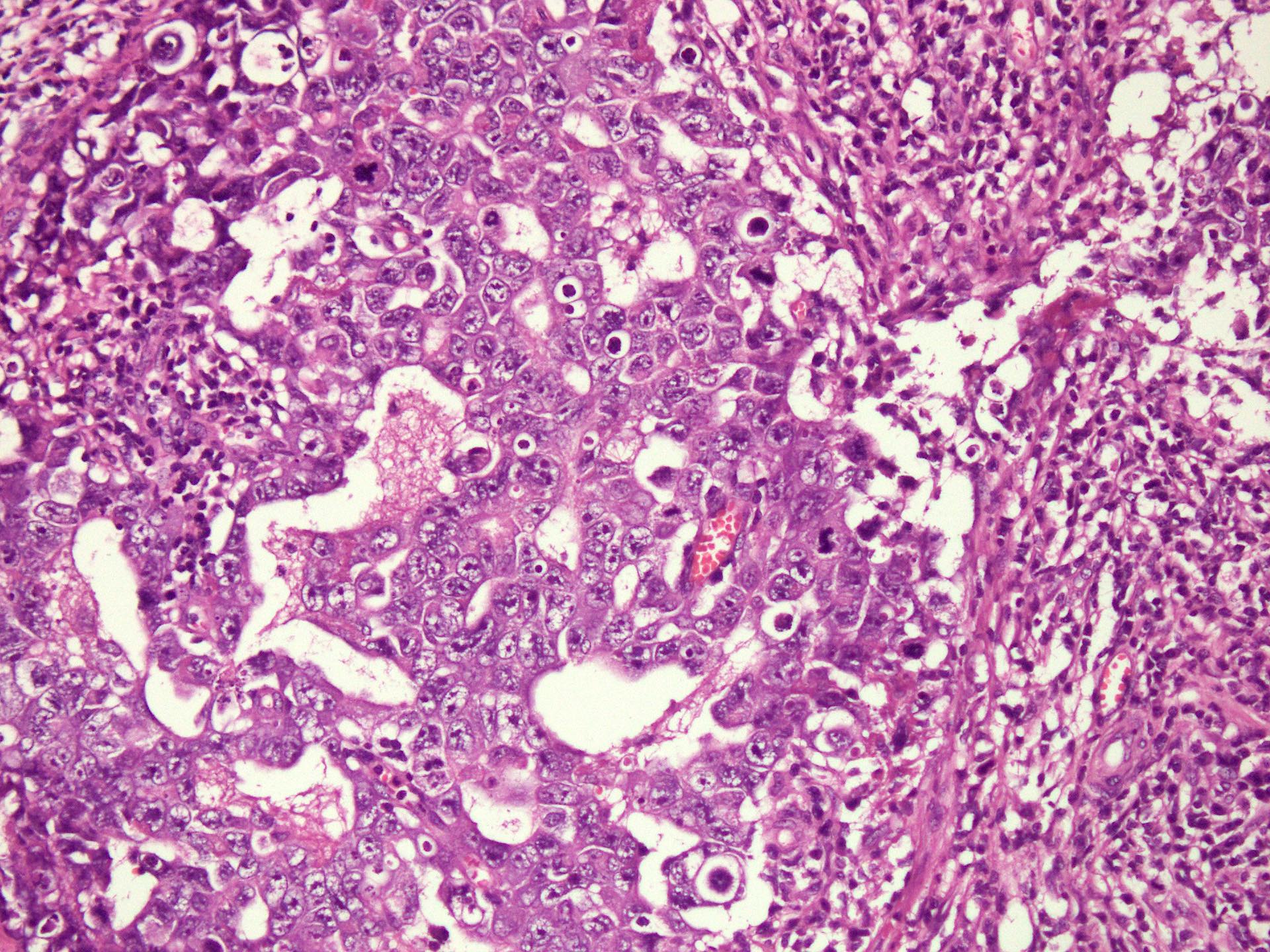
Pleomorphic cells
Pankeratin CK AE1 / AE3
SALL4
OCT3/4
Glypican 3
CD30
Cytology description
- Syncytial cohesive clusters of pleomorphic cells with frequent mitoses
- Necrosis and hemorrhage in many cases (Cancer 2008;114:504)
Cytology images
Images hosted on other servers:

Pleomorphic tumor cells; marked nuclear pleomorphism
Positive stains
Negative stains
Sample pathology report
- Anterior mediastinal mass, core biopsy:
- Germ cell tumor with morphological and immunohistochemical profile favoring embryonal carcinoma (see comment)
- Comment: A possibility of mixed germ cell tumor in the vicinity cannot be excluded.
Differential diagnosis
- Seminoma:
- See Microscopic (histologic) description in seminoma section
- Yolk sac tumor:
- See Microscopic (histologic) description in yolk sac tumor section
- Thymic carcinoma:
- Squamous differentiation and distinct cell borders for squamous subtype
- Glandular architecture and mucin containing cells for adenocarcinoma or mucoepidermoid carcinoma subtypes
- NUT carcinoma:
- Tumor cells with usually monotonous, sometimes abrupt squamous differentiation
- Expresses NUT, t(15;19) in majority of tumors
- SMARCA4 deficient undifferentiated tumor:
- Focal rhabdoid morphology
- Loss of SMARCA4 (BRG1)
- Large B cell lymphoma / primary mediastinal large B cell lymphoma:
- Discohesive tumor cells
- Characteristic immunoprofile
- Neoplasms composed of 2 or more types of germ cells
Essential features
- Presence of more than 1 type of germ cell tumor
Terminology
- Malignant teratoma (not recommended)
ICD coding
- ICD-O: 9085/3 - mixed germ cell tumor
- ICD-11: 2C28.0 & XH2PS1 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & mixed germ cell tumor
Epidemiology
- In adults, M > F and common tumor components are teratoma and embryonal carcinoma
- In children, yolk sac tumor and teratoma (mature or immature) are the most common types
Sites
- Occur in anterior mediastinum
Etiology
- Similar to other types
Clinical features
- Mediastinal mass and elevated serum markers
Diagnosis
- Elevated serum markers
- Mediastinal mass on imaging
- Biopsy showing 2 or more types of germ cell components
Laboratory
- Raised AFP, hCG and LDH (Open Med (Wars) 2021;16:892)
Radiology description
- Large heterogenous mass with necrosis, hemorrhage and often infiltration of adjacent structures
- Presence of cystic spaces or adipose tissue suggests presence of a teratomatous component (AJR Am J Roentgenol 2010;195:W274, Open Med (Wars) 2021;16:892)
Radiology images
Images hosted on other servers:

CT scan of chest with anterior mediastinal mass
Case reports
- 12 year old boy with mixed germ cell tumor of the mediastinum diagnosed on core biopsy (Open Med (Wars) 2021;16:892)
- 16 year old boy with huge mediastinal mass diagnosed as mixed germ cell tumor with possible combination of embryonal carcinoma, yolk sac and teratoma (Case Rep Surg 2016;2016:7615029)
- 26 year old man with mixed germ cell tumor comprising of immature teratoma and seminoma diagnosed due to massive organ displacing tumor in right chest on chest Xray (Pathol Res Pract 2009;205:572)
- 29 year old man with disease progression despite systemic chemotherapy, diagnosed as mixed germ cell tumor on en bloc resection (J Surg Case Rep 2021;2021:rjab416)
Treatment
- Resected after chemotherapy
Gross description
- Heterogeneous cut surface
- Solid, fleshy tumor with areas of hemorrhage and necrosis
- Cystic spaces indicate presence of a teratomatous component
Gross images
Images hosted on other servers:

4.6 kg mediastinal mixed GCT, mostly teratoma
Microscopic (histologic) description
- Morphology identical to pure germ cell component
- Please refer to the sections above for microscopic description of individual components
Cytology description
- Please refer to the sections above for cytological description of individual components
Positive stains
- Please refer to the sections above for individual components
Negative stains
- Please refer to the sections above for individual components
Sample pathology report
- Anterior mediastinal mass, biopsy:
- Malignant mixed germ cell tumor with seminoma (~50%), yolk sac tumor (~30%) and embryonal carcinoma (~20%) components (see comment)
- Comment: The findings show majority of tumor comprised of sheets of polygonal cells with vesicular nuclei and prominent nucleoli. Intervening fibrous septa show lymphocytic infiltration. This component stains positive for immunohistochemical stains SALL4 and OCT3/4 while staining negative for CD30 and glypican 3. Another admixed component shows reticular pattern and Schiller-Duval bodies of cuboidal cells which stain positive for SALL4 and glypican 3 while staining negative for OCT3/4 and CD30. A small component comprised of large polygonal cells with pleomorphic nuclei, prominent nucleoli, numerous mitoses and necrosis is seen. This component stains positive for SALL4 and OCT3/4 and CD30 while staining negative for glypican 3.
- See synoptic reporting for resection specimen.
- Malignant germ cell tumor composed of seminomatous germ cells
- A seminoma with any component of a nonseminomatous tumor is considered a nonseminomatous germ cell tumor (NSGCT)
Essential features
- Seminomas are almost always diagnosed in patients ≥ 10 years old (Pediatr Blood Cancer 2004;42:169)
Terminology
- Germinoma
ICD coding
- ICD-O: 9061/3 - seminoma
- ICD-11: 2C28.0 & XH9FM4 - malignant germ cell neoplasms of heart or mediastinum, or nonmesothelioma of pleura & seminoma, NOS
Epidemiology
- Seminomas are almost always diagnosed in patients aged ≥ 10 years (Pediatr Blood Cancer 2004;42:169)
Sites
- Occurs in anterior mediastinum and rarely in middle mediastinum (Kaohsiung J Med Sci 2005;21:395)
Etiology
- Seminomas are type II germ cell tumors usually arising from thymic gland
- 12p amplification or isochromosome 12p (Int J Clin Exp Pathol 2019;12:3082)
- KIT mutations almost all in exon 7, rarely in exon 9 (Lab Invest 2002;82:1369, Pathology 2009;41:695)
Clinical features
- Most patients are symptomatic
- Dyspnea, chest pain, superior vena cava syndrome, cough with hemoptysis, hoarseness
Diagnosis
- Chest Xray followed by contrast enhanced CT scan or MRI (StatPearls: Mediastinal Seminoma [Accessed 16 March 2023])
Laboratory
- Beta hCG is mildly elevated ≤ 100 IU/L in adults and ≤ 25 IU/L in children (normal range ≤ 5 IU/L)
- LDH is elevated
- AFP is normal (StatPearls: Mediastinal Seminoma [Accessed 16 March 2023])
Radiology description
- Bulky, lobular, homogenous, soft tissue opacity with only slight contrast enhancement (Radiographics 2017;37:413)
Radiology images
Images hosted on other servers:

Mass (M) in prevascular mediastinum
Prognostic factors
- Prognosis is better than nonseminomatous malignant germ cell tumors
- Good prognosis if nonpulmonary visceral metastasis is absent (J Clin Oncol 2002;20:1864)
Case reports
- 18 year old woman with primary mediastinal seminoma mixed with leiomyosarcoma (Cell Mol Biol (Noisy-le-grand) 2022;67:104)
- 19 year old man with primary seminoma of the mediastinum showing local increase in residual tumor after chemotherapy (Hinyokika Kiyo 2020;66:153)
- 48 year old man with primary mediastinal seminoma and florid follicular lymphoid hyperplasia (Diagn Pathol 2021;16:76)
- 52 year old man with primary seminoma of the middle mediastinum (Oncol Lett 2016;12:348)
Treatment
- Cisplatin based combination chemotherapy and radiotherapy
- Surgical excision is reserved for cases not responding to chemotherapy and radiotherapy (Oncol Res Treat 2019;42:95)
Gross description
- Smooth and glistening or lobulated outer surface
- Soft, creamy to light tan nodular cut surfaces (Kaohsiung J Med Sci 2005;21:395)
- May show both solid and cystic areas with necrotic material
Gross images
Images hosted on other servers:

Cystic seminoma with necrotic tissue
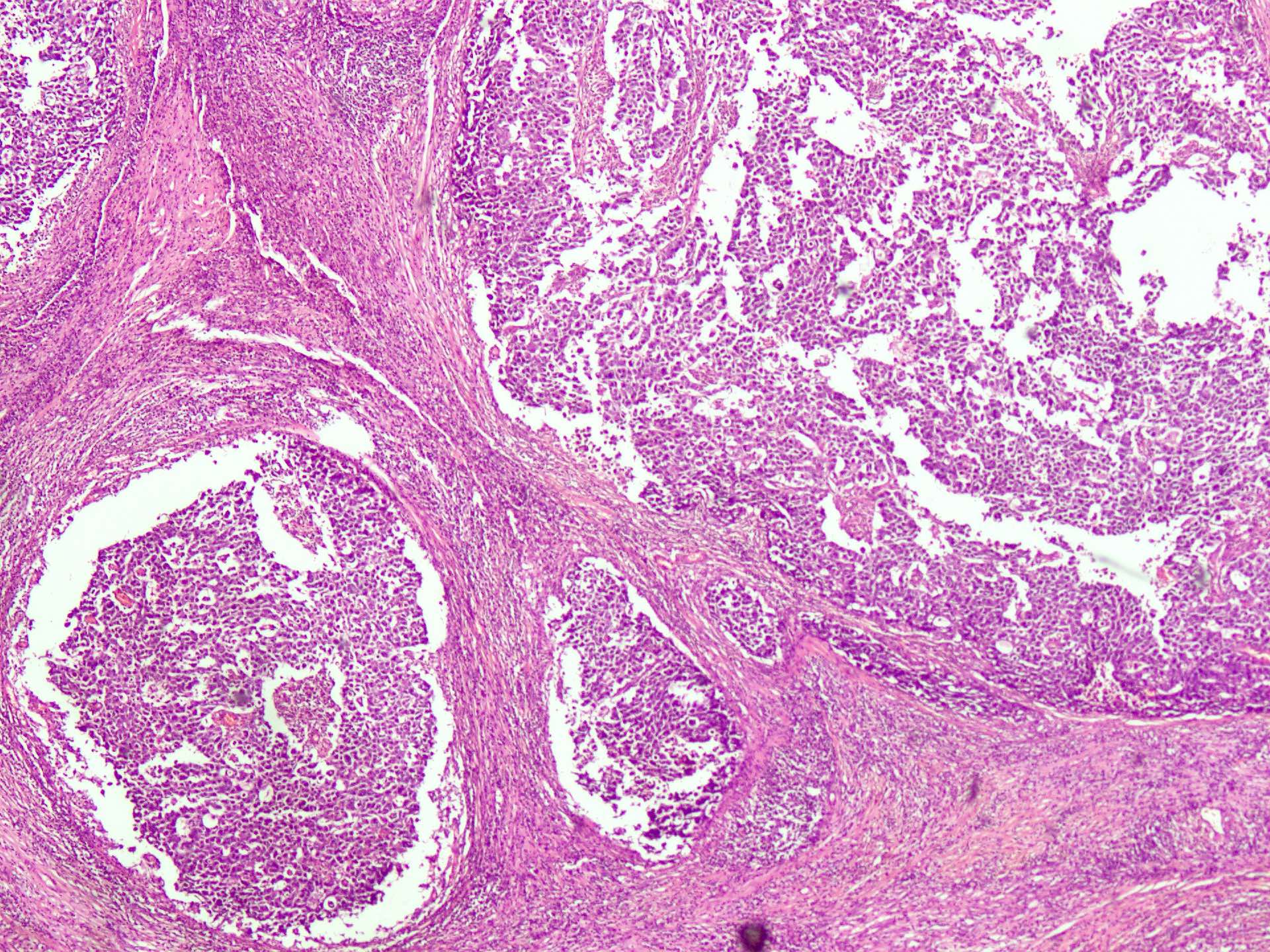
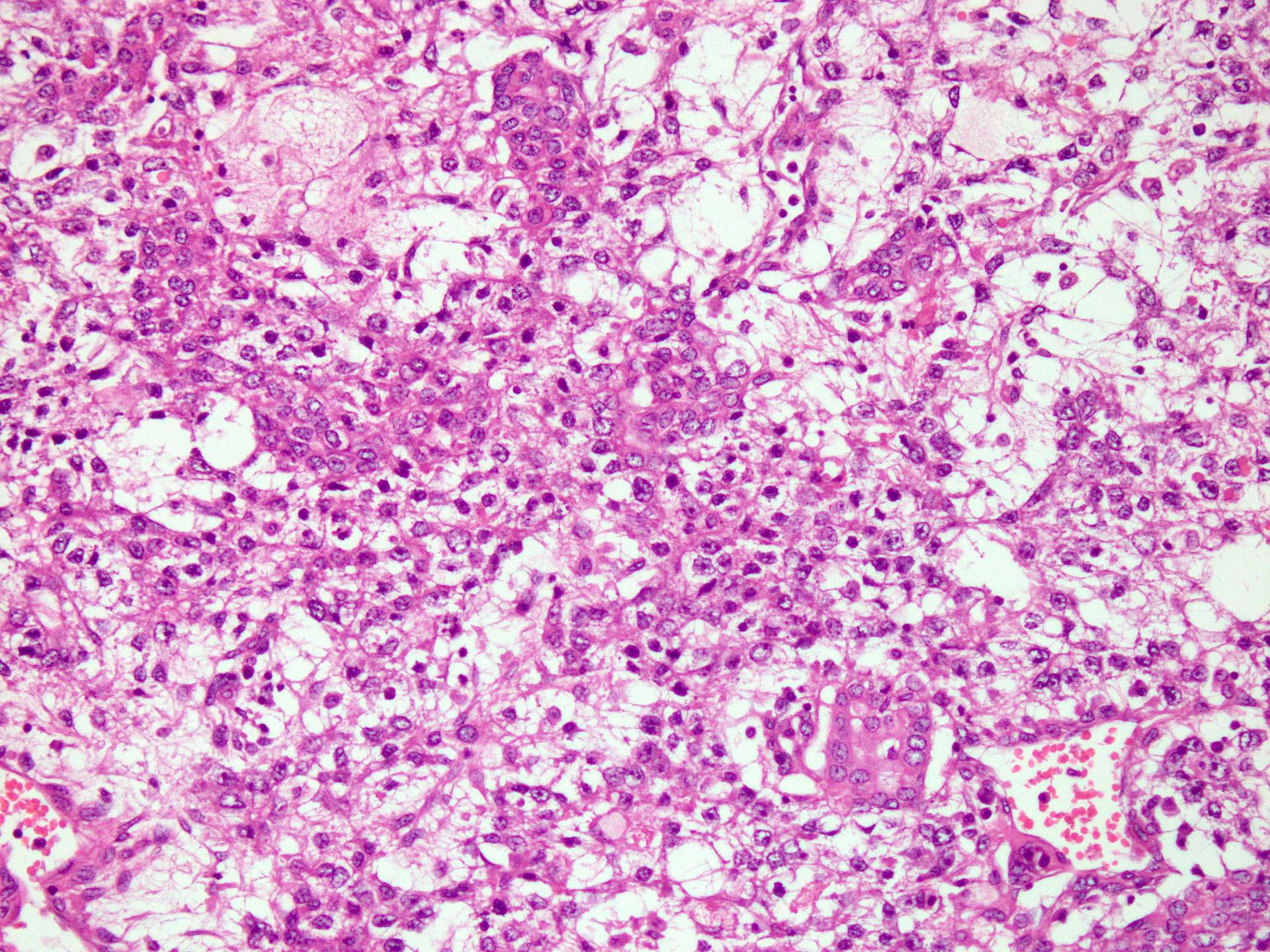
Microscopic (histologic) description
- Round to polygonal, uniform epithelioid cells with round to oval nuclei, vesicular chromatin and large nucleoli
- Abundant, glycogen rich, clear to lightly eosinophilic cytoplasm and distinct cell membranes
- Tumor cells grow in confluent sheets, multinodular clusters, cords or irregular lobules
- Lymphocytic infiltration of fibrous septa / stroma is almost always seen
- Other findings including nonnecrotizing granulomas, cellular pleomorphism, necrosis, intercellular edema, syncytiotrophoblasts (Kaohsiung J Med Sci 2005;21:395, Int J Clin Exp Pathol 2019;12:3082)
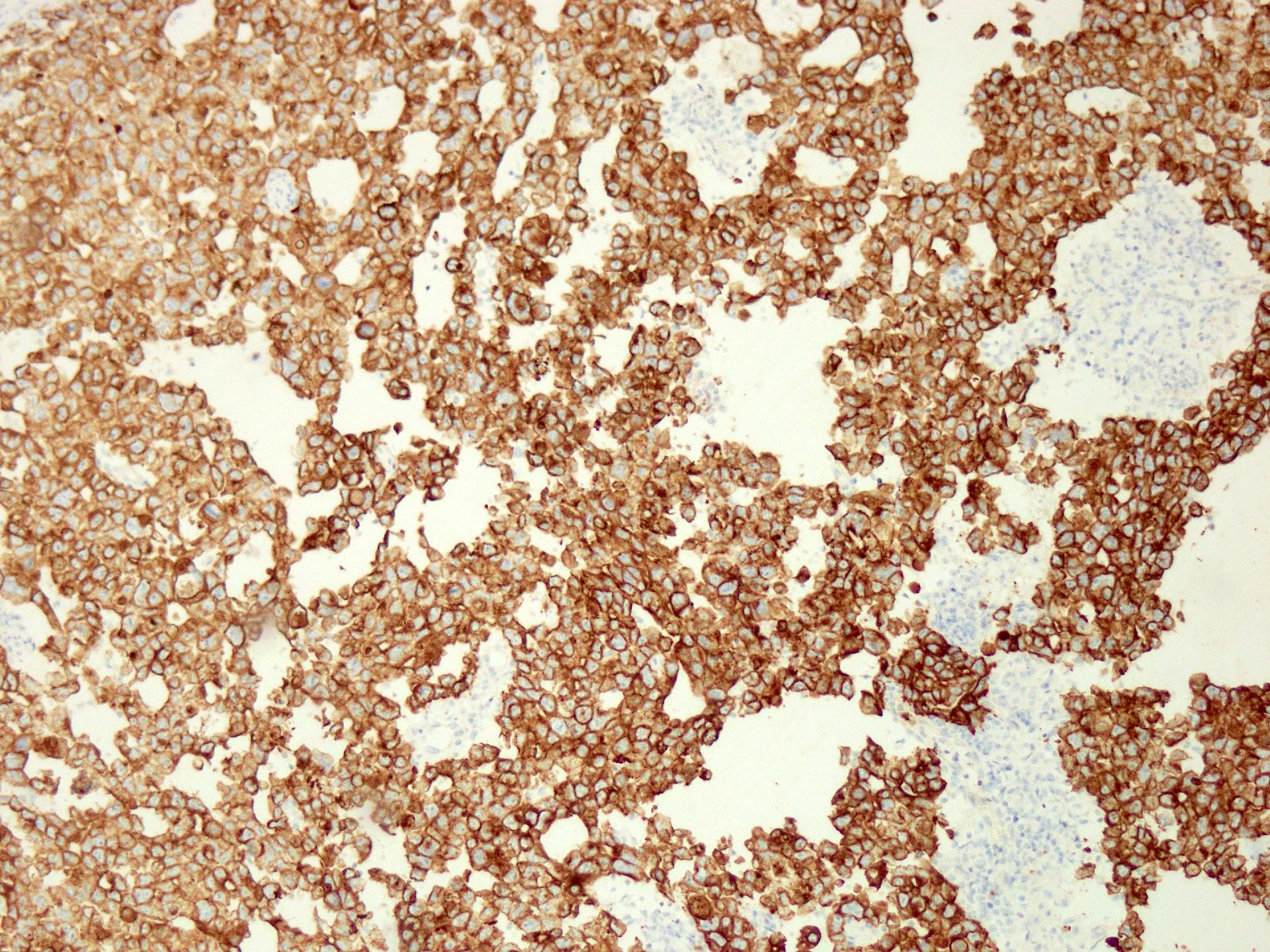
Microscopic (histologic) images
Contributed by Sarosh Moeen, M.B.B.S.
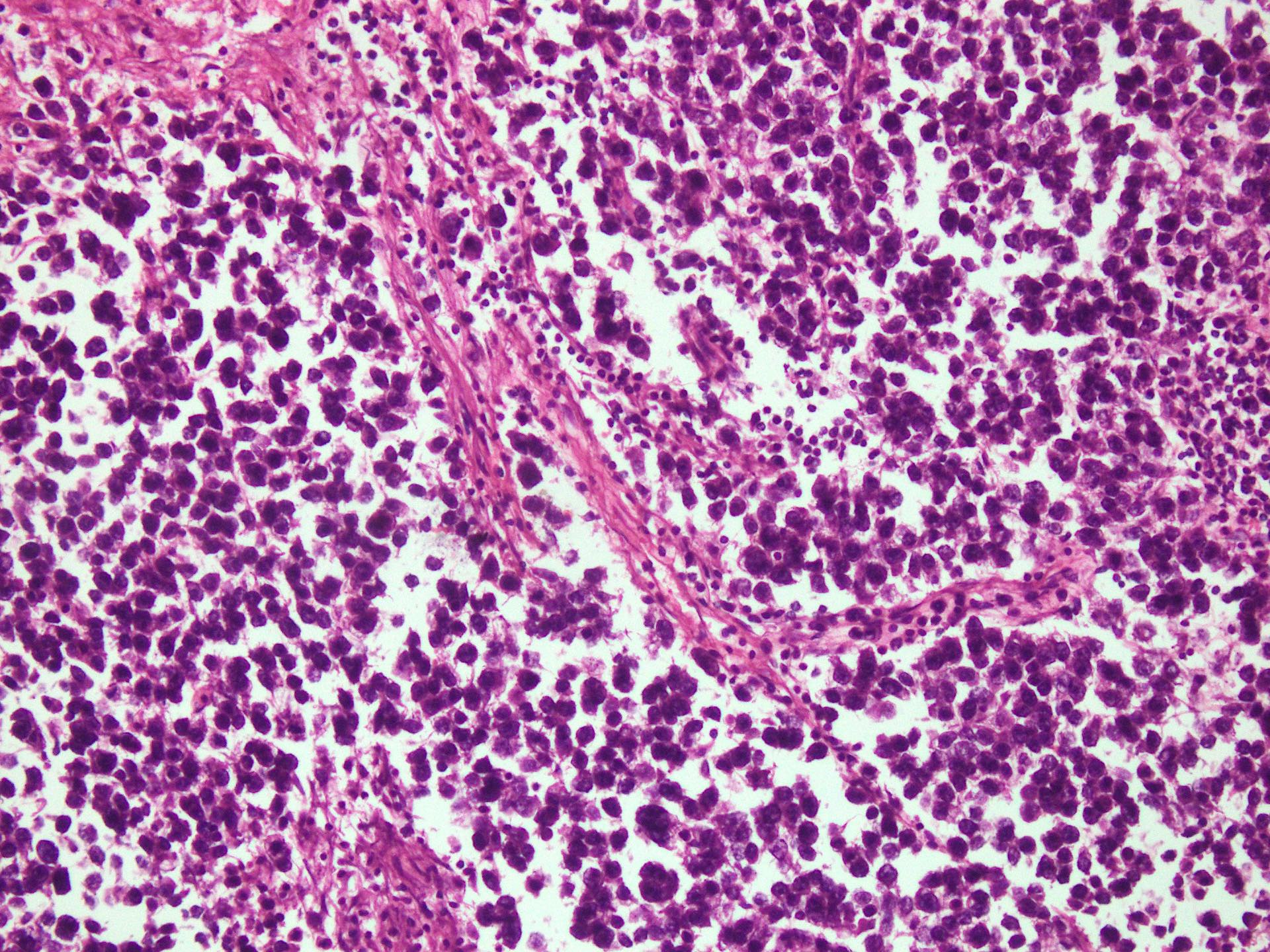
Uniform appearing cells
Cytology description
- Discohesive cells, round or polygonal nuclei, 1 or more prominent nucleoli, pale cytoplasm
- Lymphocytes, plasma cells and characteristic tigroid stripes
- Necrosis and giant cells may be present (Cancer 2008;114:504)
Cytology images
Images hosted on other servers:

Clusters of cells; tigroid background

Cytologic smear; cell block
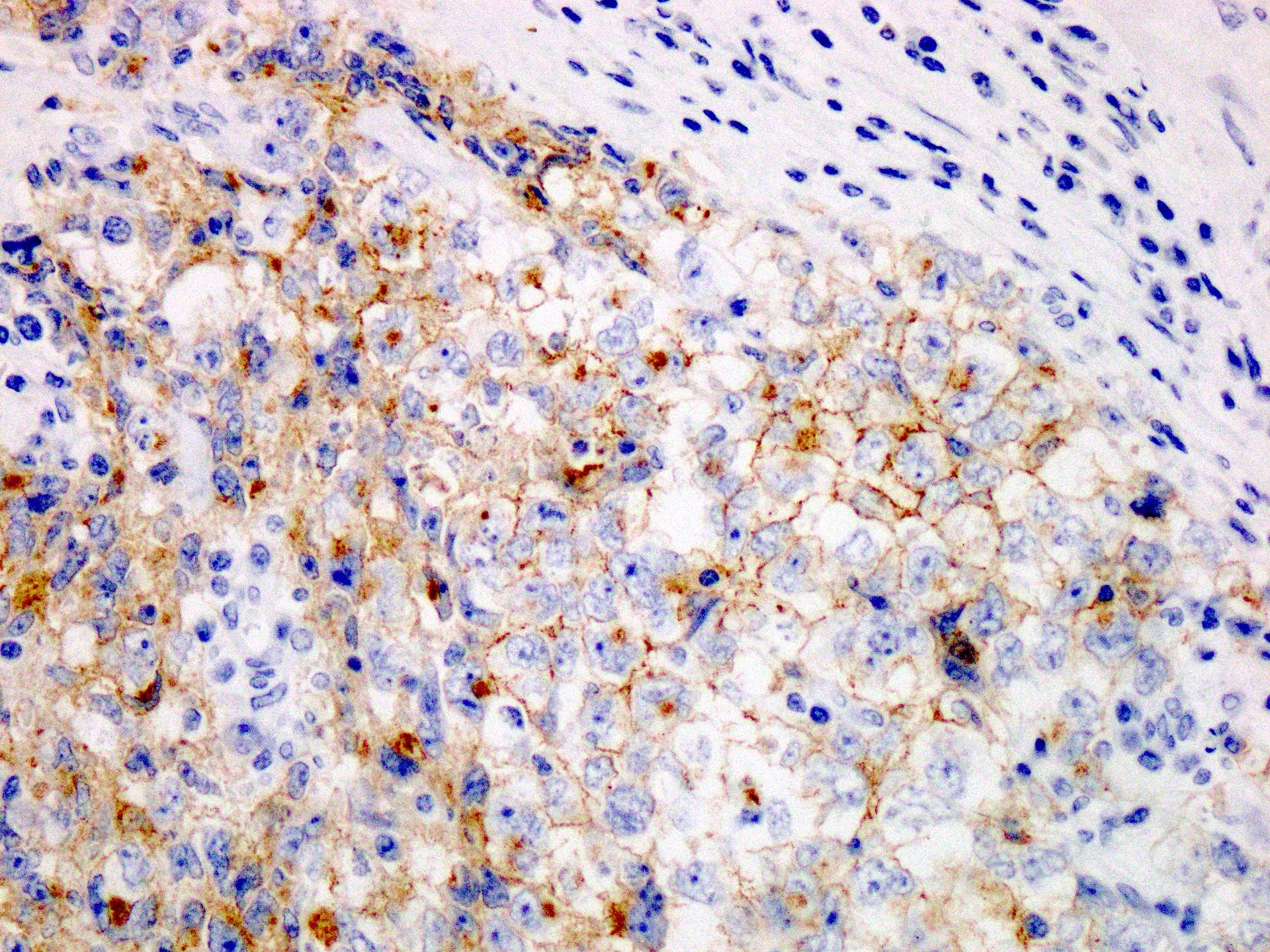
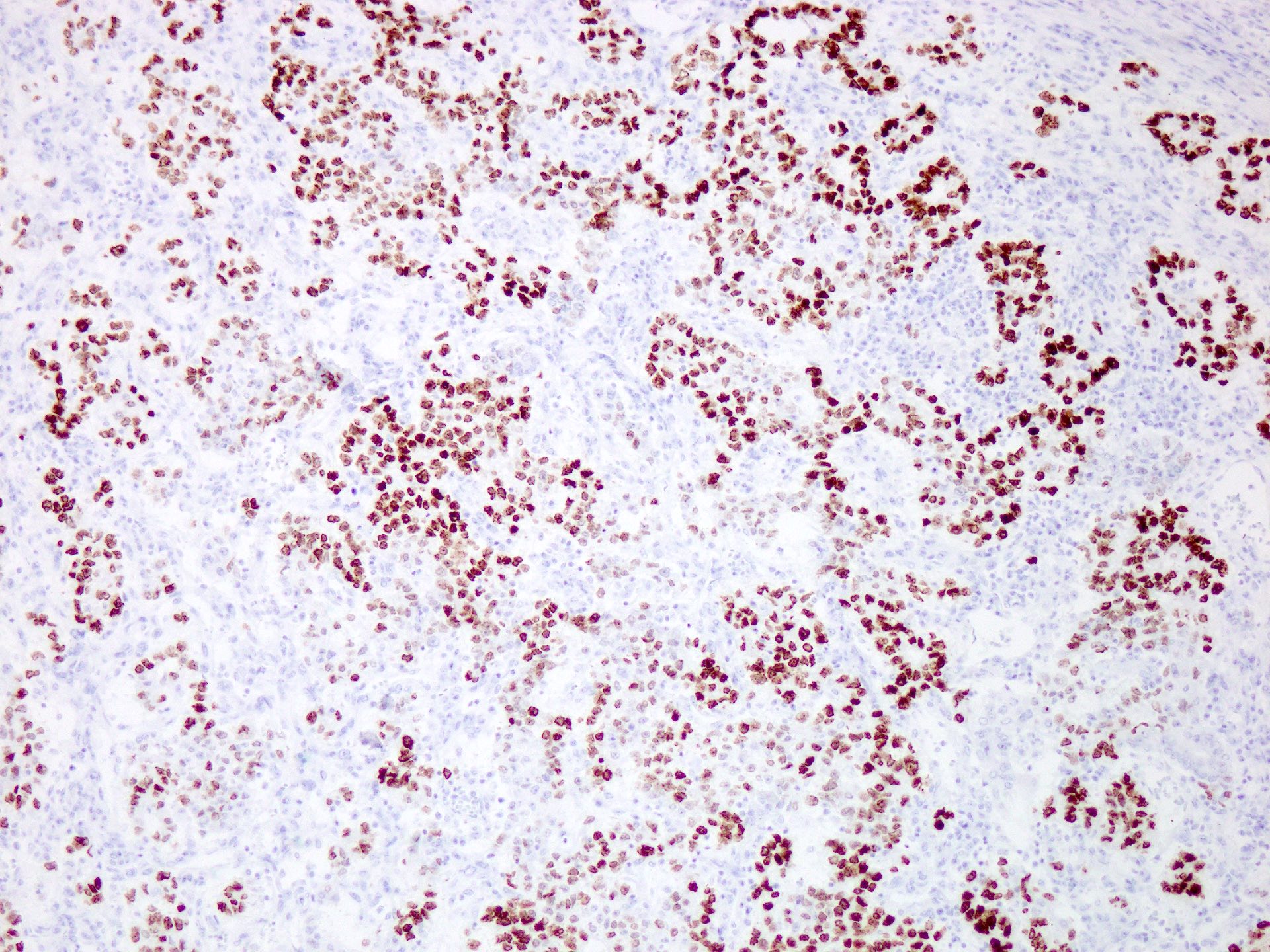
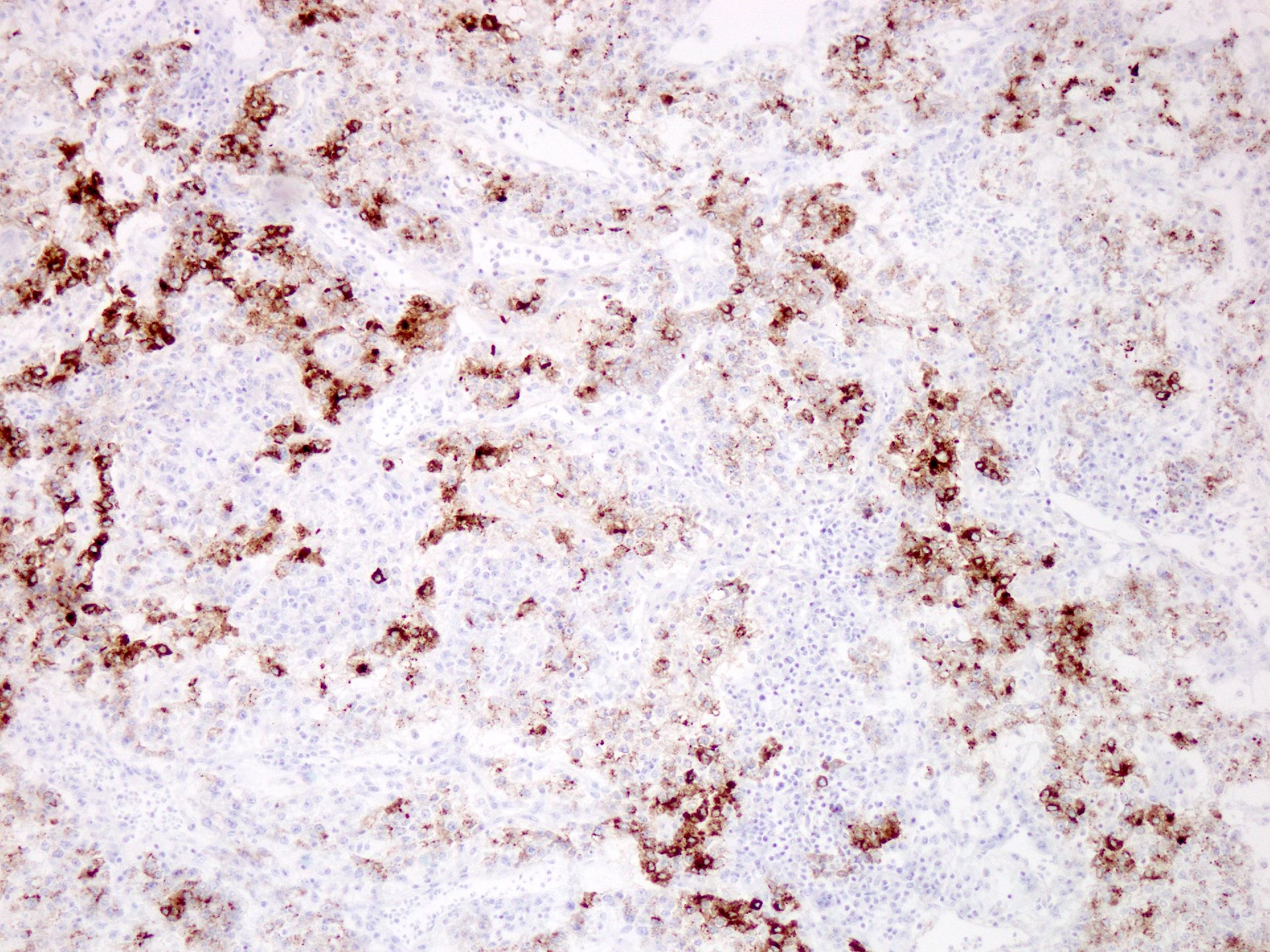
Positive stains
- SALL4, OCT4 (100%), KIT (CD117) (74%)
- D2-40, PLAP (43%) and CD99 frequently expressed
- Keratins focal or weakly expressed, usually dot-like paranuclear staining pattern (Int J Clin Exp Pathol 2019;12:3082)
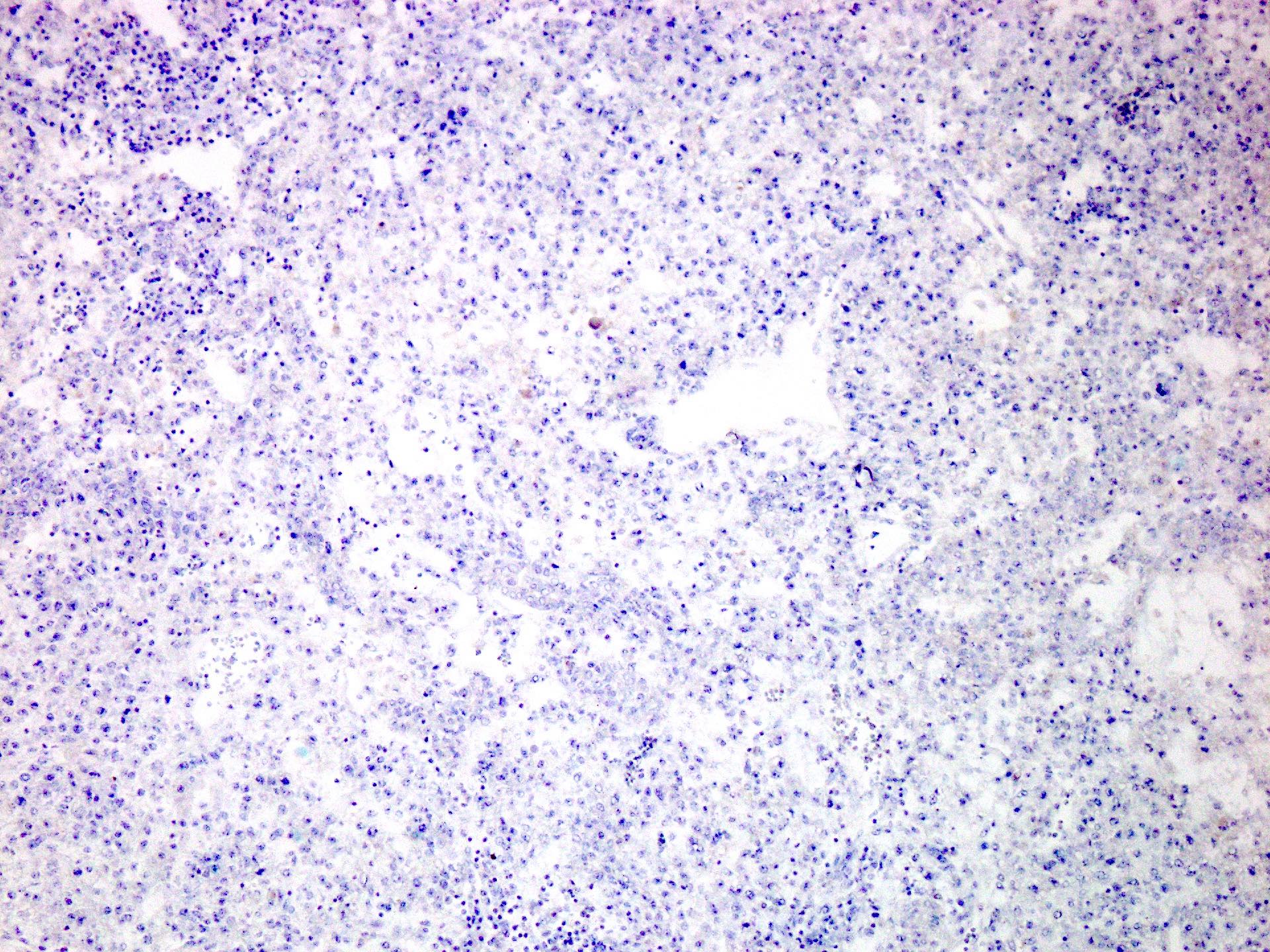
Negative stains
Sample pathology report
- Anterior mediastinal mass, core biopsy:
- Germ cell tumor with morphological and immunohistochemical profile favoring seminoma (see comment)
- Comment: A possibility of mixed germ cell tumor in the vicinity cannot be excluded.
Differential diagnosis
- Metastatic seminoma:
- Physical examination and radiological imaging to rule out metastasis from ovaries or testis
- Embryonal carcinoma:
- See Microscopic (histologic) description below
- Solid pattern yolk sac tumor:
- See Microscopic (histologic) description below
- Thymic carcinoma:
- Squamous differentiation and distinct cell borders for squamous subtype
- Glandular architecture and mucin containing cells for adenocarcinoma or mucoepidermoid carcinoma subtypes
- Mediastinal B cell lymphoma:
- Tumor cells are usually more discohesive with a distinct immunophenotype
- Melanoma:
- Prominent eosinophilic nucleoli, pigment if present and a characteristic immunoprofile
- Neoplasm of pluripotent cell origin that forms differentiated somatic type tissues, which may be exclusively mature (adult type), exclusively immature (embryonal or fetal) or a combination of both
Essential features
- Tumor composed entirely of differentiated somatic type tissue, may be mature, immature or combined
ICD coding
- ICD-O:
- ICD-11:
- 2C28.0 & XH3GV5 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & teratoma, benign
- 2C28.0 & XH7YZ9 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & teratoma, malignant, NOS
Epidemiology
- < 10% of all mediastinal masses
- Occur in both prepubertal and postpubertal patients with no gender predominance
- Can occur in fetuses (Pediatr Surg Int 2016;32:635)
- May be associated with other germ cell tumors
- Can occur in Klinefelter syndrome (Cancer Radiother 2018;22:255)
Sites
- Occurs in anterior mediastinum and rarely in posterior mediastinum
Etiology
- Limited data about molecular biology and genetic features of primary mediastinal teratomas
Clinical features
- Chest pain, shortness of breath, wheezing and cough due to compression of adjacent structures
- Superior vena cava syndrome, hemoptysis, dysphagia, nausea and hoarseness are less common
Diagnosis
- Incidental mass on radiological imaging in asymptomatic patients with serum tumor markers (AFP and beta hCG) not elevated
- More symptomatic in children
- Characteristic radiological findings of soft tissue, fat, fluid and calcifications in variable proportions
- Biopsy findings showing differentiated somatic type tissue, may be mature, immature or combined
Laboratory
- Serum tumor markers AFP and beta hCG are not elevated
Radiology description
- Mature teratomas are well demarcated with multilocular cysts
- Heterogenous attenuation with a combination of soft tissue, fluid, fat and calcification
- Bone and teeth pathognomonic
- Immature teratomas are often solid masses (AJR Am J Roentgenol 2010;195:W274, Radiol Case Rep 2020;15:1058)
Radiology images
Images hosted on other servers:

Huge posterior mediastinal mass

Anterior mediastinal mass
Prognostic factors
- Mature teratomas are benign
- Immature teratomas have malignant potential and malignant behavior correlates with amount of immature tissue
- Somatic type malignancy may occur in mature teratomas, which determines the prognosis (Int J Surg Case Rep 2021;80:105680)
Case reports
- Newborn with intrapericardial teratoma (Ultraschall Med 2006;27:577)
- 24 year old man with multilocular thymic cyst and mature teratoma with a carcinoid component (Surg Case Rep 2022;8:24)
- 30 year old woman with mature mediastinal teratoma and somatic type malignancy including neuroblastoma and intestinal type adenocarcinoma (Int J Surg Case Rep 2021;80:105680)
Treatment
- Complete surgical excision in cases of benign teratoma
Clinical images
Images hosted on other servers:

En bloc tumor resection
Gross description
- Encapsulated masses with variegated cut surface and unilocular or multilocular cysts
- Cyst contents may include clear fluid, mucoid material, sebaceous and keratinaceous debris, hair, fat, cartilage and rarely teeth or bone
- Immature teratomas have soft to fleshy consistency or are extensively fibrous or cartilaginous
- Hemorrhage and necrosis common
Gross images
Images hosted on other servers:

Excised tumor with rib
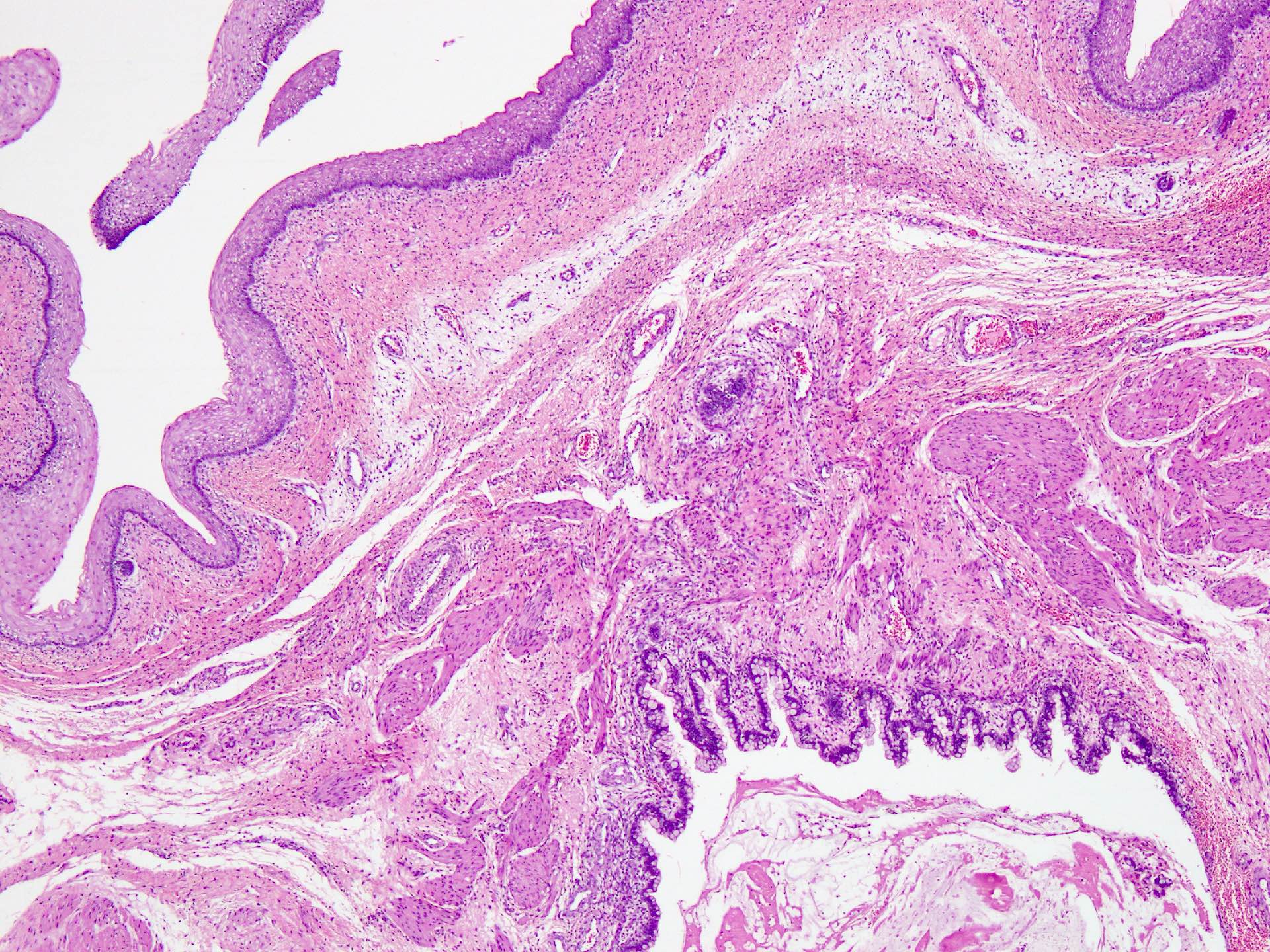
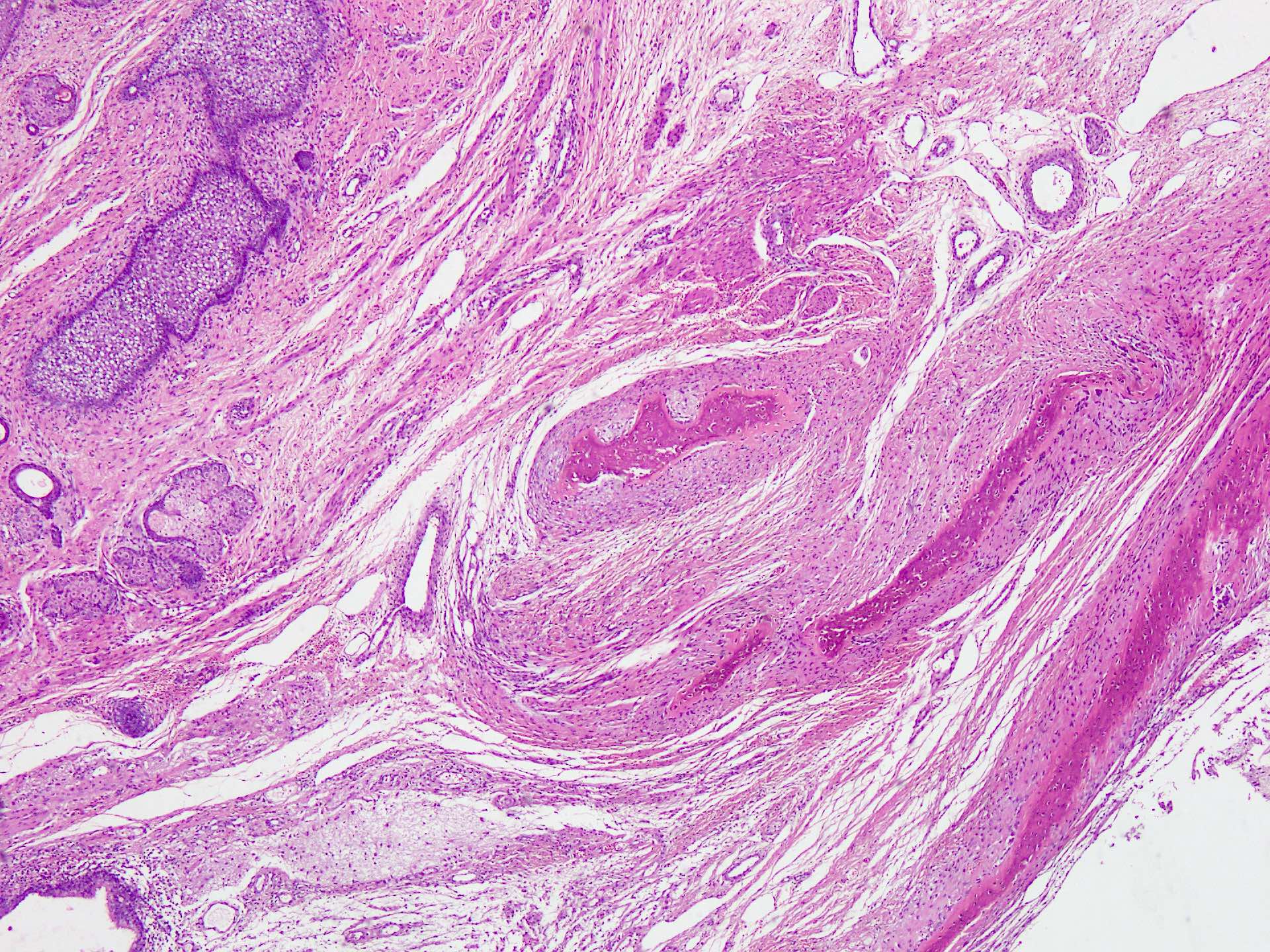
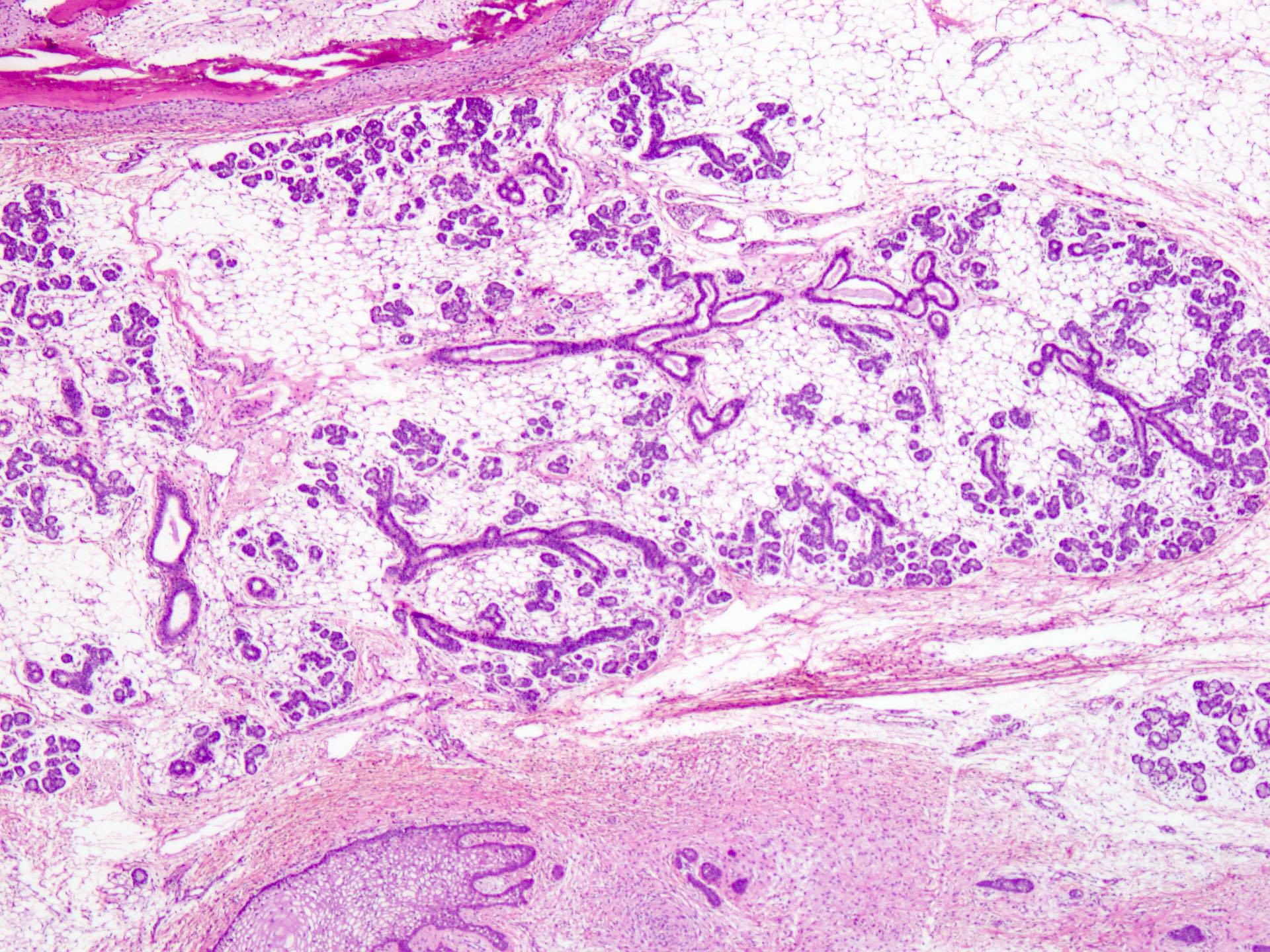
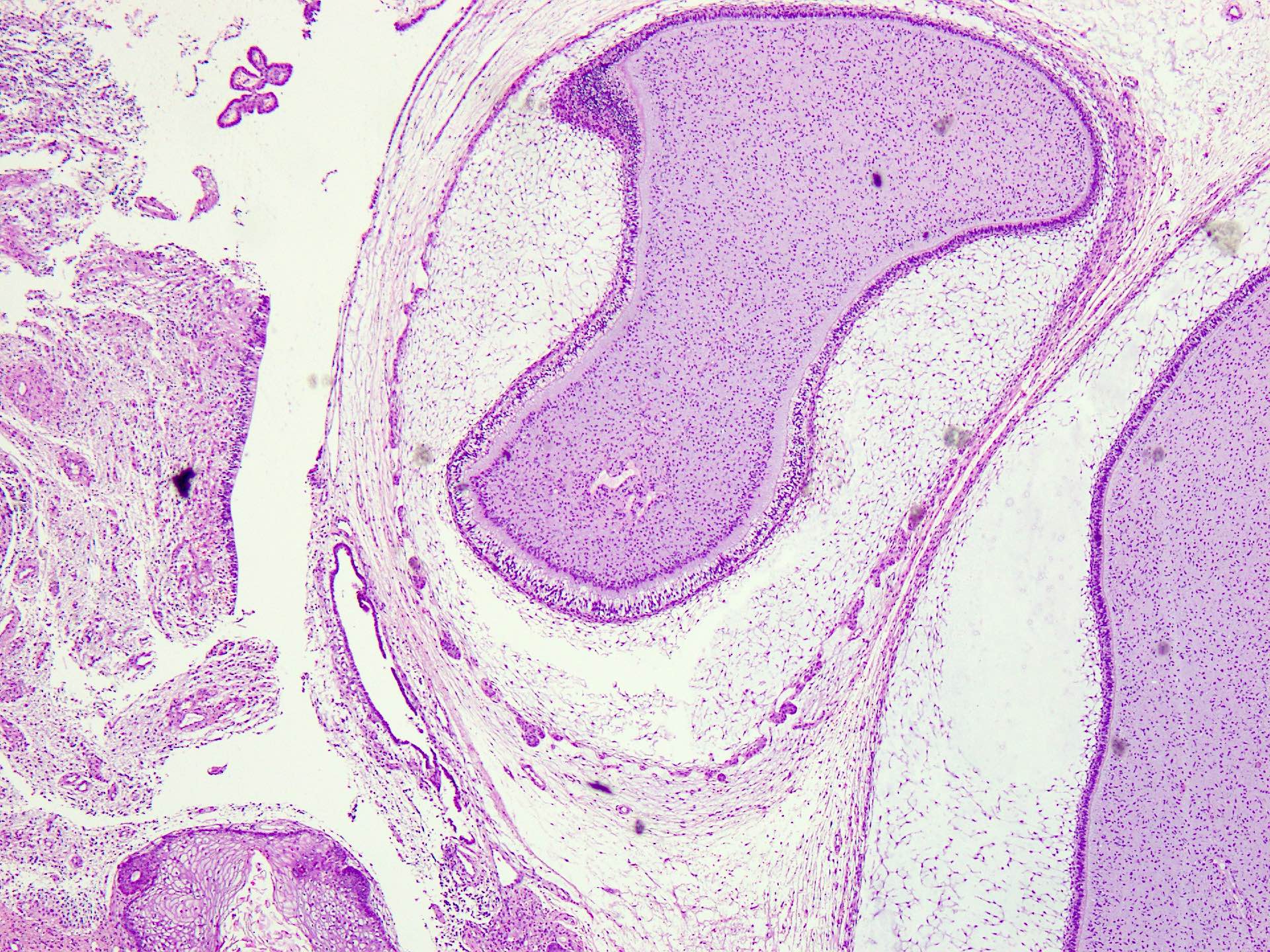
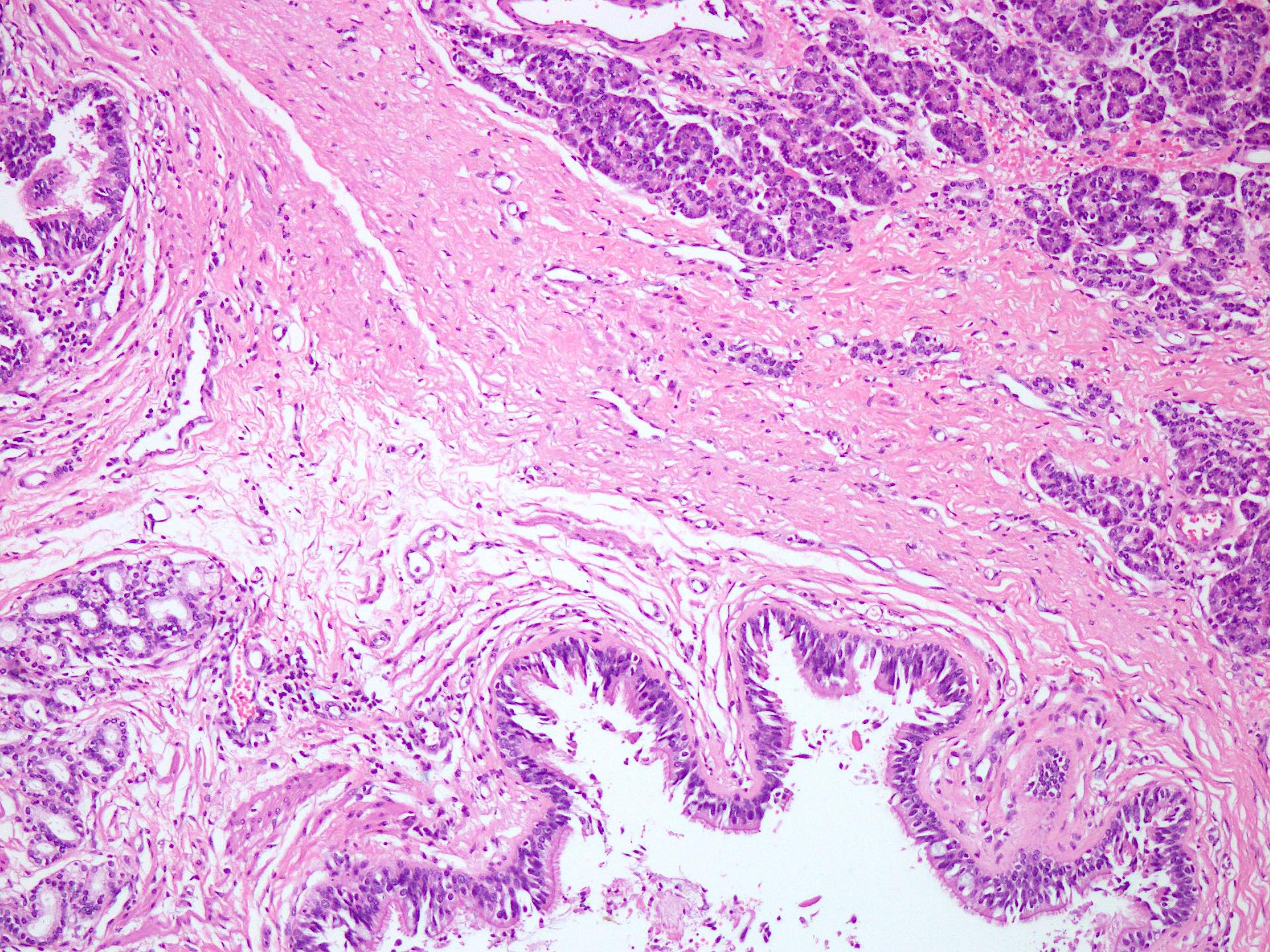
Microscopic (histologic) description
- Haphazard distribution of mature somatic tissue is hallmark
- Skin and cutaneous appendages are common, often lining cysts
- Bronchial mucosa, glands, gastrointestinal mucosa, nerves and mature brain tissue
- Smooth muscle, adipose tissue, mature pancreatic tissue
- Immature tissue corresponds to embryonal or fetal tissues either exclusively or in addition to mature tissue
- Most common immature tissue is neuroectodermal tissue with neuroepithelial cells forming tubules and rosettes (Mediastinum 2019;3:30)
- Fetal lung, mesenchyme, primitive cartilage, bone, rhabdomyoblasts may be seen
Microscopic (histologic) images
Contributed by Sarosh Moeen, M.B.B.S.
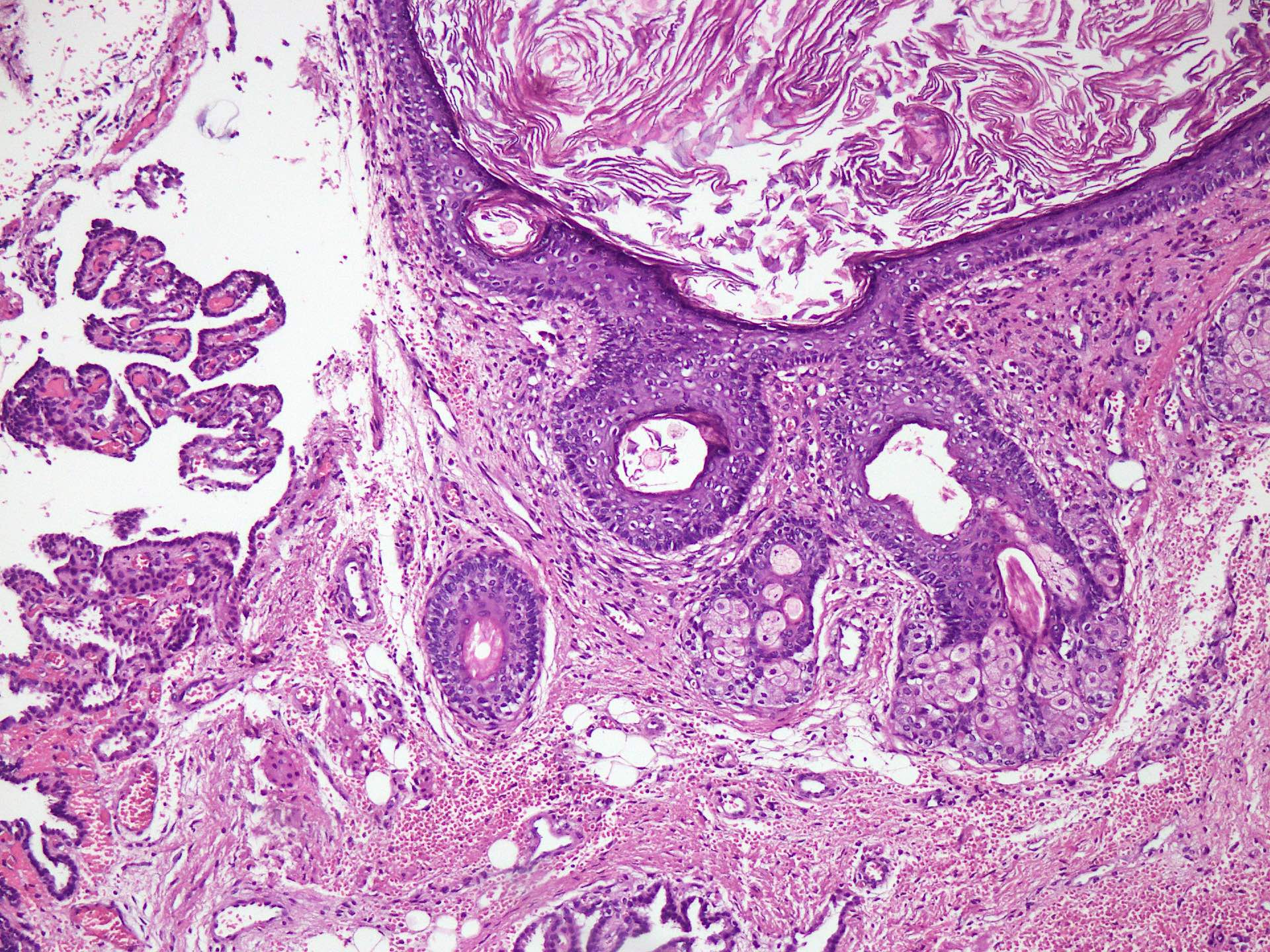
Skin and choroid plexus
Mucinous epithelium
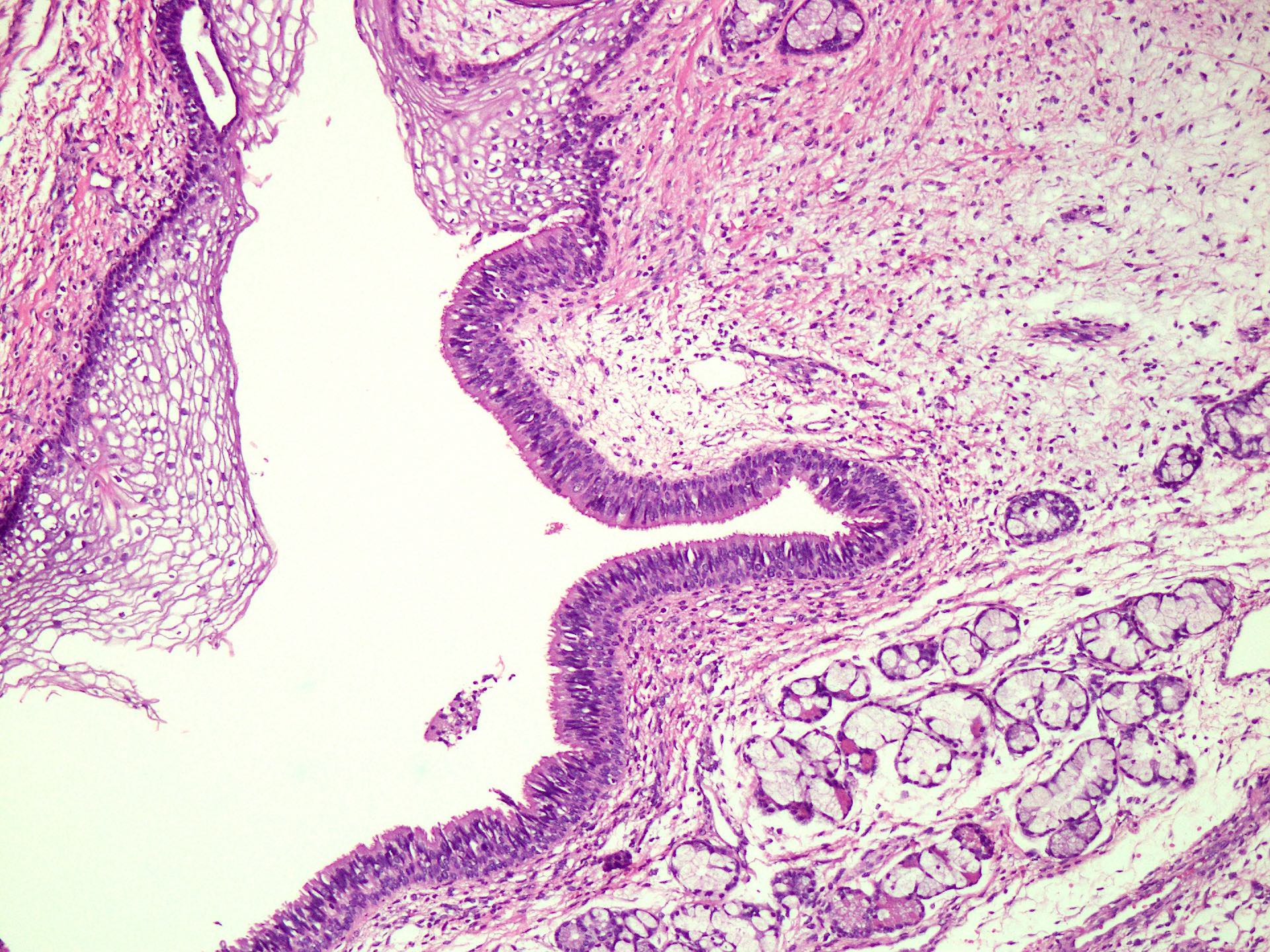
Respiratory and squamous epithelium
Glial tissue
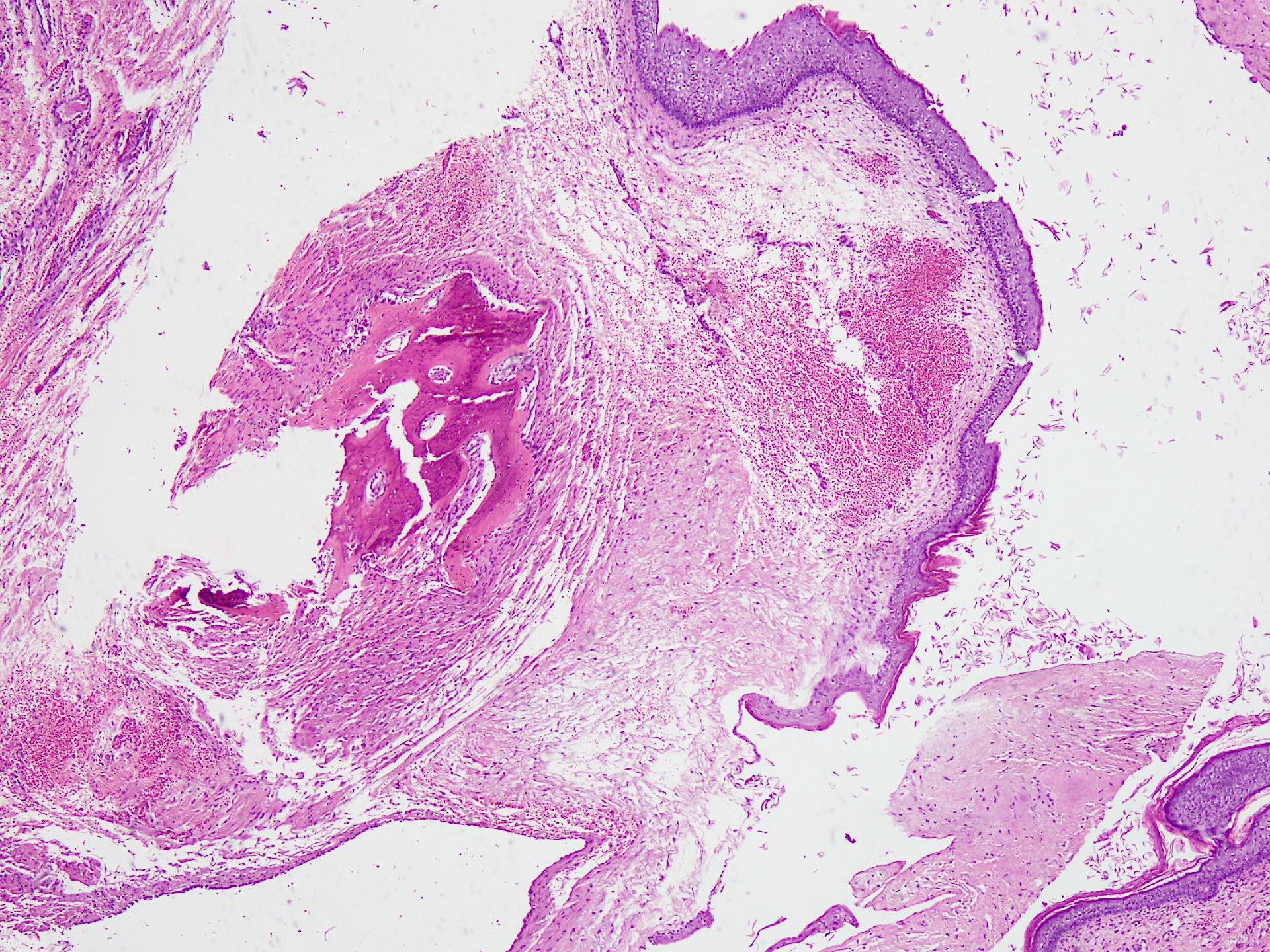
Mature bone
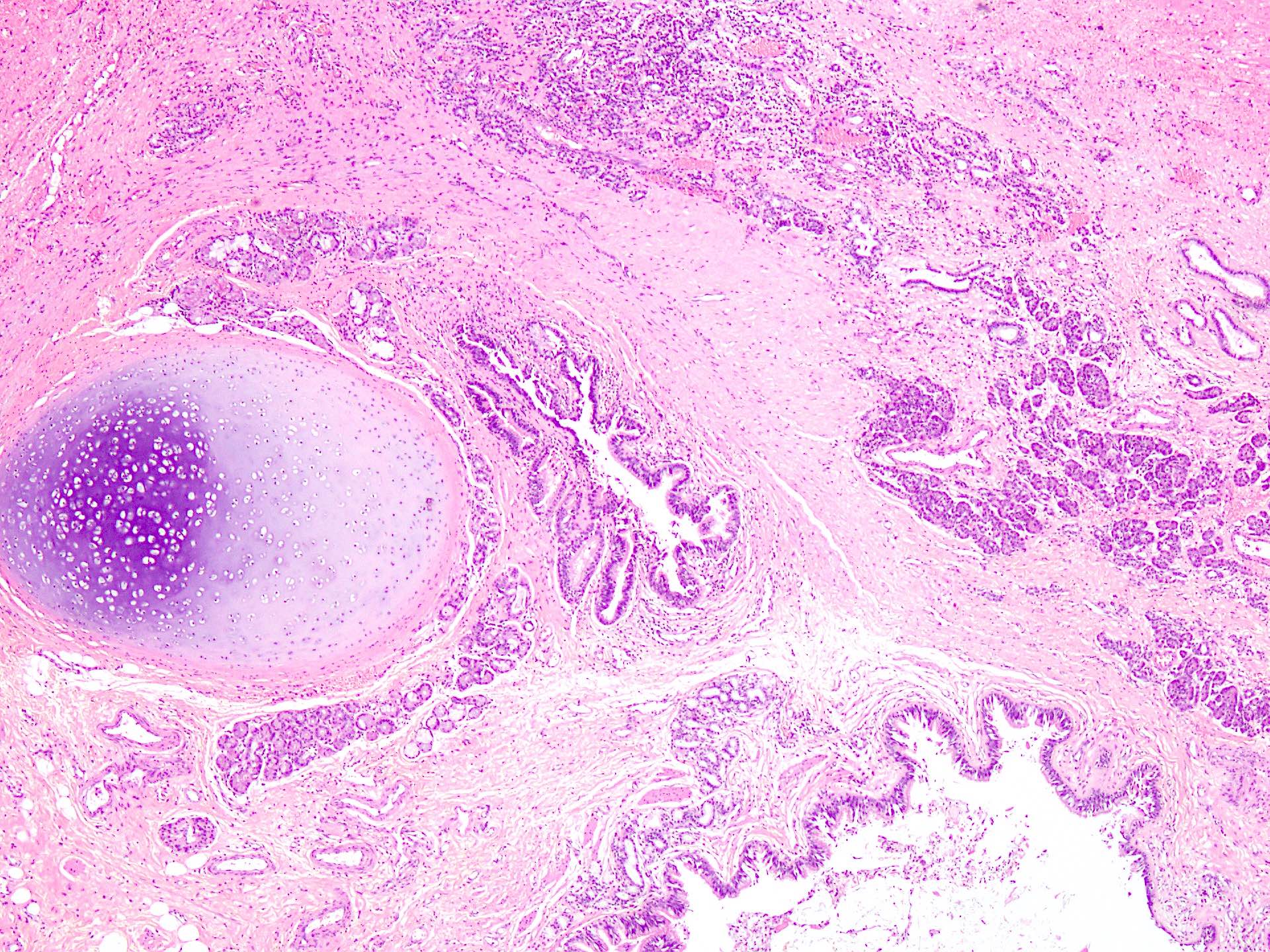
Cartilage lobule
Adipose tissue and acini
Odontogenic tissue
Pancreatic acini
Cytology description
- Anucleate squamous cells and macrophages in a cystic background
- Presence of ciliated bronchial epithelium, smooth muscle and cartilage may be mistaken for contamination
- Presence of pancreatic acini or intestinal type mucosa may be suggestive of a teratomatous lesion
- Careful correlation with imaging and serological studies to exclude mixed germ cell tumor (Cancer 2008;114:504)
Cytology images
Images hosted on other servers:

Mature and immature teratoma
Positive stains
- Not supportive in mature teratoma
Negative stains
Videos
Pathology mini tutorial for teratoma
Sample pathology report
- Anterior mediastinal mass, core biopsy:
- Germ cell tumor with features favoring mature teratoma (see comment)
- Comment: The microscopic features show skin adnexal structures, mature cartilage and a tiny focus of mature glial tissue.
- A possibility of immature component or mixed germ cell tumor in the vicinity cannot be excluded.
Differential diagnosis
- Bronchogenic cysts:
- In anterior and middle mediastinum
- Foregut duplication cysts:
- In posterior mediastinum
- Malignant nonseminomatous germ cell tumor characterized by numerous patterns that recapitulate the yolk sac, allantois and extraembryonic mesenchyme
Terminology
- Endodermal sinus tumor (not recommended)
ICD coding
- ICD-O: 9071/3 - yolk sac tumor
- ICD-11: 2C28.0 & XH09W7 - malignant germ cell neoplasms of heart, mediastinum or nonmesothelioma of pleura & yolk sac tumor
Epidemiology
- Restricted to males after puberty and strong female preponderance in children
- Peak incidence at third decade of life in adults
- Pure yolk sac tumor 2 - 12% of mediastinal germ cell tumor in adults
- Yolk sac tumor is virtually the only malignant germ cell tumor of the mediastinum in children up to 5 years of age (Turk Pediatri Ars 2019;54:185, Ann Diagn Pathol 2021;53:151763)
Sites
- Most commonly anterior mediastinum
Etiology
- Klinefelter syndrome is a risk factor after puberty (Int J Pediatr Endocrinol 2020;2020:18)
- Genetic losses at 1p, 4q and 6q and gains at 1q, 3, 20q and 20 reported in mediastinal yolk sac tumors in patients < 8 years of age
- After 8 years of age, isochromosome 12p, gain of chromosome 21 and X and loss of chromosome 13
Clinical features
- Chest pain, dyspnea, chills, fever and superior vena cava syndrome
Diagnosis
- FDG PET may detect tiny occult primary tumor or recurrences
Laboratory
- Serum AFP levels always elevated
- Beta hCG normal (Thorac Cancer 2018;9:491)
Radiology description
- Large solid - cystic mass with intratumoral hemorrhage, capsular tear, marked heterogeneous enhancement and enlarged intratumoral vessels on CT scan (Acta Radiol 2016;57:98)
Radiology images
Images hosted on other servers:

CT scan of chest
Prognostic factors
- No significant difference between yolk sac tumor and mixed germ cell tumor
- Complete surgical resection is the most favorable prognostic factor
Case reports
- 15 year old boy with mediastinal yolk sac tumor infiltrating the heart (Exp Oncol 2018;40:82)
- 20 year old man with yolk sac tumor of anterior mediastinum presenting as acute pericarditis (Am J Case Rep 2022;23:e932616)
- 47 year old man presented with conus medullaris syndrome due to metastatic primary mediastinal yolk sac tumor (Int J Spine Surg 2015;9:59)
Treatment
- Chemotherapy (platinum based) and surgical resection (Thorac Cancer 2018;9:491)
Gross description
- Solid or cystic with soft pale gray cut surface and gelatinous or mucoid consistency
- Hemorrhage and necrosis after neoadjuvant therapy
- Cyst formation may be treatment related or may indicate a mixed germ cell tumor
Gross images
Images hosted on other servers:

Firm, solid white mass
Microscopic (histologic) description
- Different histologic patterns: microcystic (reticular), macrocystic, glandular - alveolar, endodermal sinus (pseudopapillary), myxomatous, hepatoid, enteric, polyvesicular - vitelline, solid and spindle
- Loose network of cystic spaces and channels lined by flat or cuboidal cells with scant cytoplasm in a microcystic / reticular pattern
- Pseudopapillary structures and Schiller-Duval bodies in endodermal sinus pattern (Kaohsiung J Med Sci 2005;21:395)
- Cysts lined by cuboidal to flat tumor cells surrounded by dense fibrous stroma in a polyvesicular / vitelline pattern (Mediastinum 2019;3:30)
- Solid pattern resembles seminoma and embryonal carcinoma
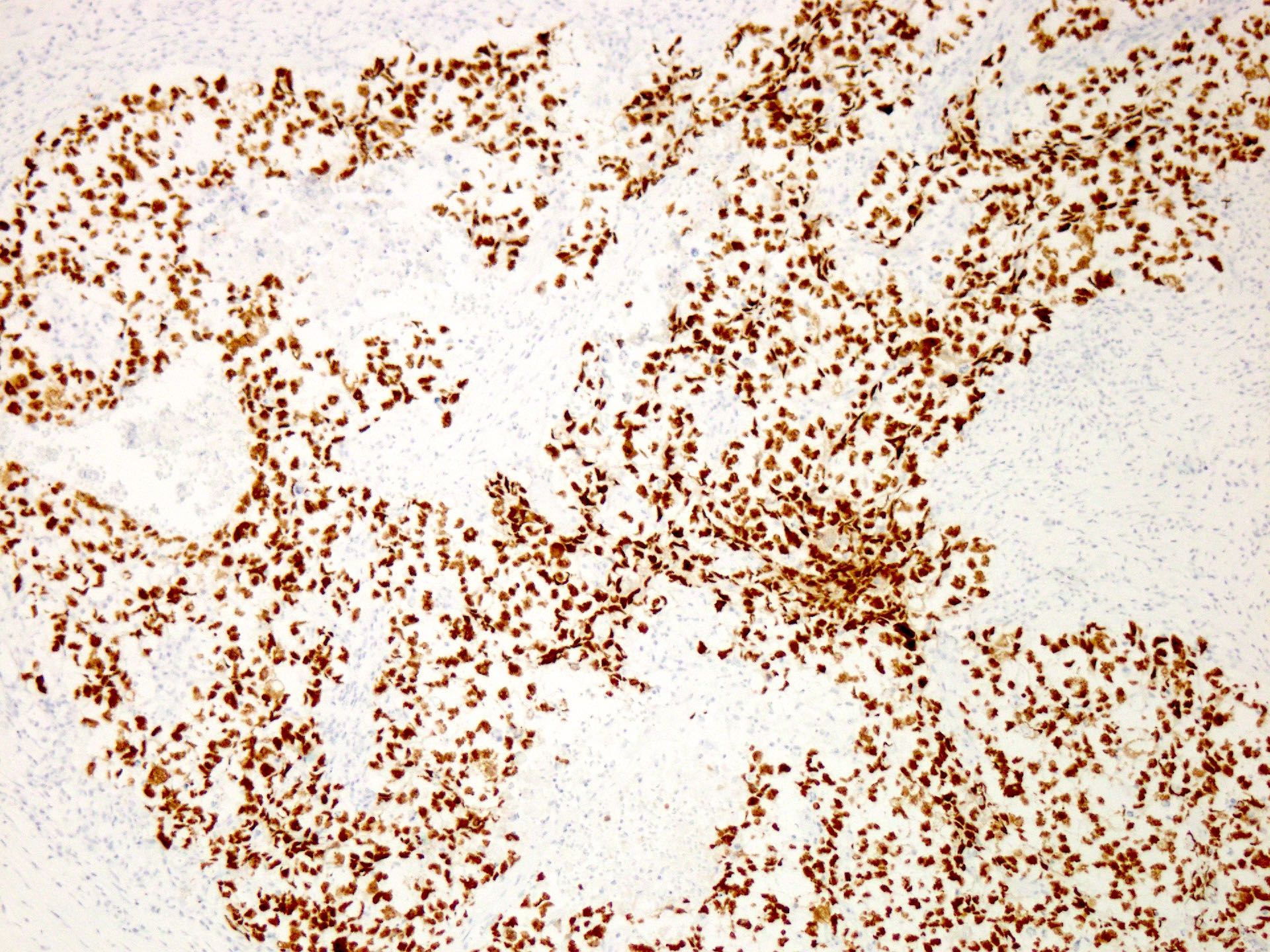
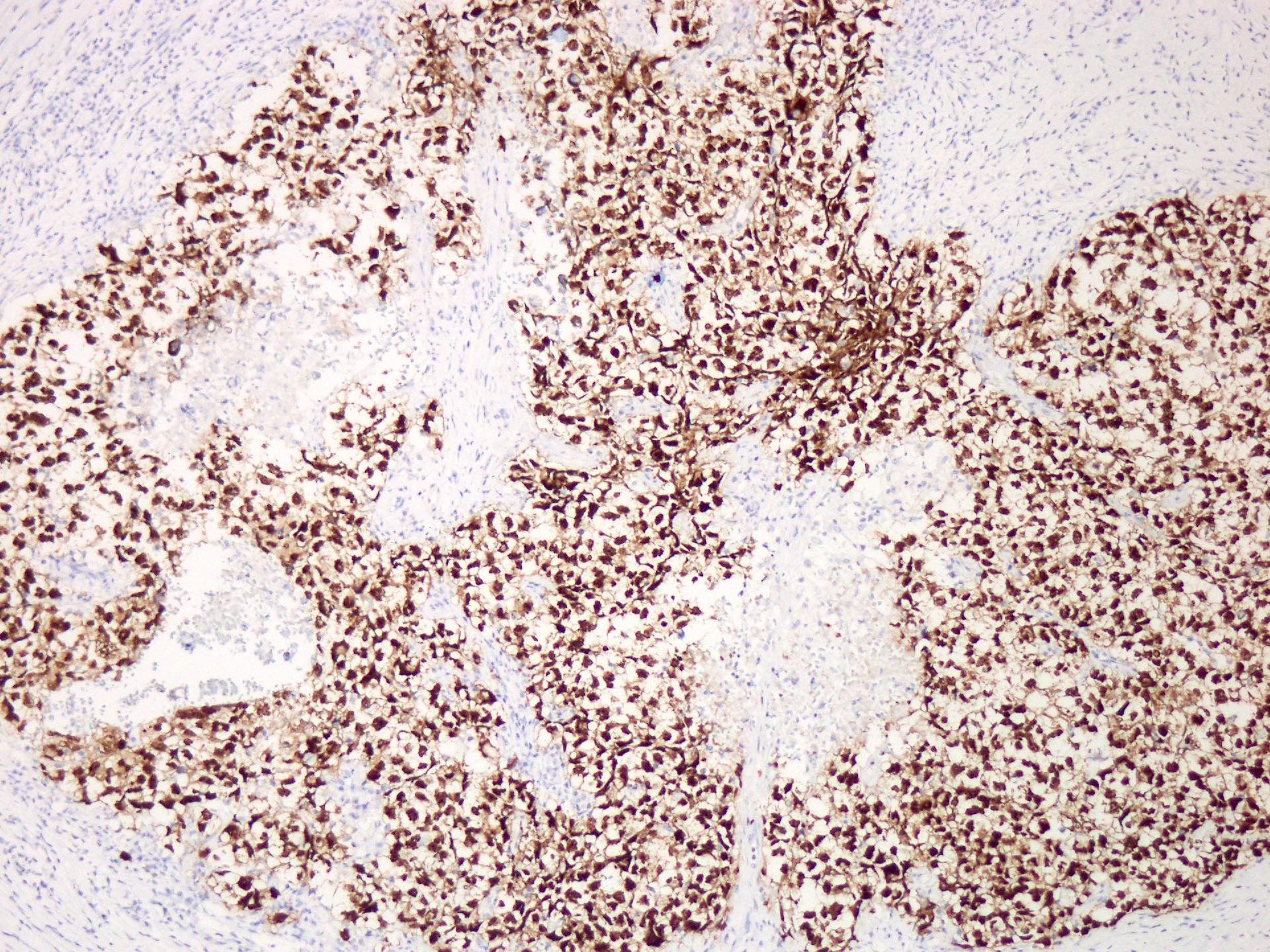
Microscopic (histologic) images
Contributed by Sarosh Moeen, M.B.B.S.
Sheet-like growth of cells
Marked pleomorphism
SALL4
OCT3/4
Glypican 3
Cytology description
- Aggregates of medium to large cells with variable nuclei and prominent nucleoli
- Cytoplasm moderate to abundant
- Background debris or mucoid material
- Presence of hyaline globules is typical (Cancer 2008;114:504)
Cytology images
Images hosted on other servers:

Pap; Giemsa
Positive stains
- Glypican 3
- SALL4
- LIN28
- Cytokeratins (AE1 / AE3)
- AFP, PLAP, CD117 (variable expression)
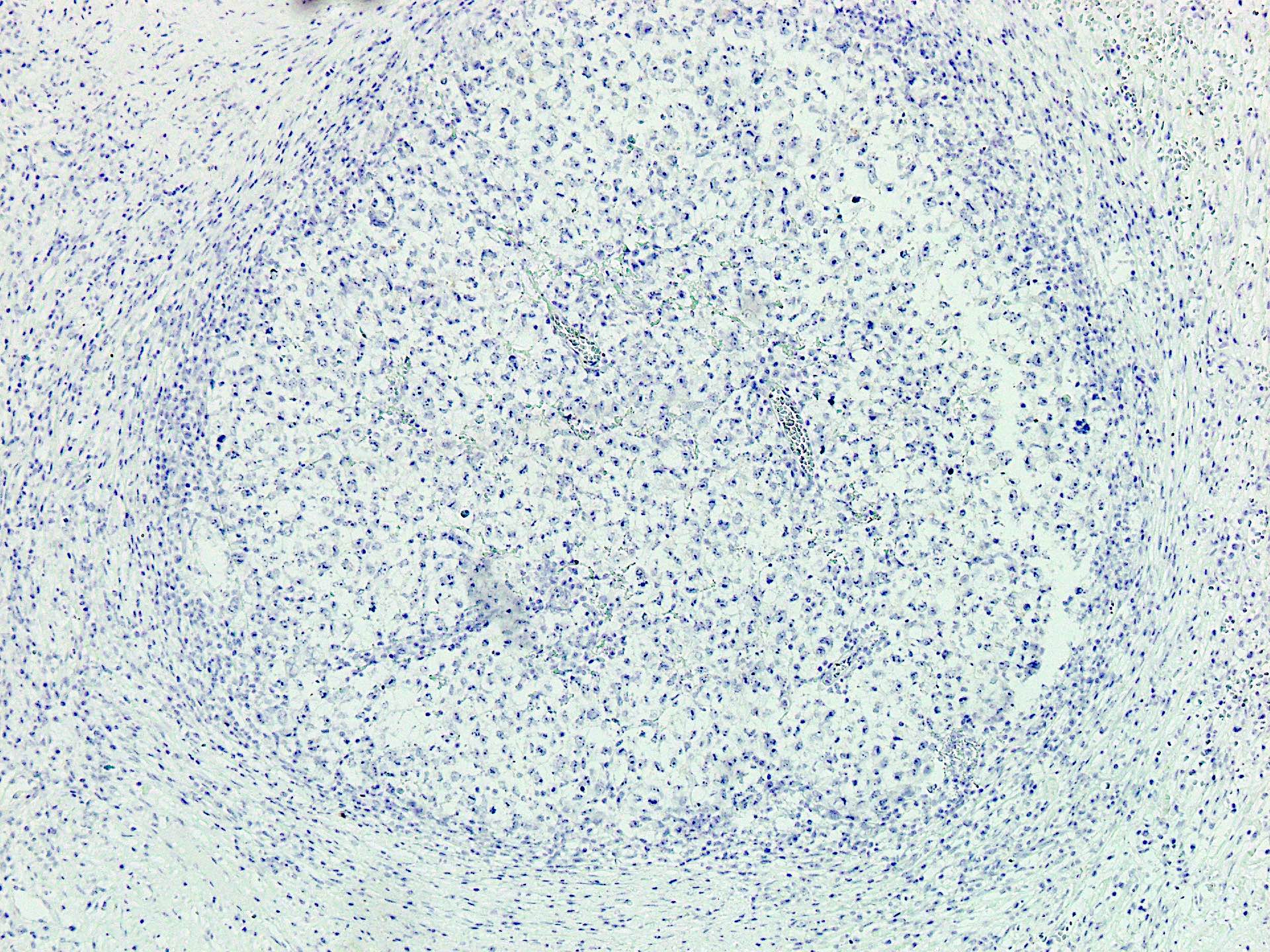
Negative stains
- OCT4
- NANOG
- SOX2
- D2-40
- CD30 (expressed in 11% cases)
- EMA (positive in the minority of cases) (Mediastinum 2019;3:30)
Sample pathology report
- Anterior mediastinal mass, core biopsy:
- Germ cell tumor with immunohistochemical profile favoring yolk sac tumor (see comment)
- Comment: A possibility of mixed germ cell tumor in the vicinity cannot be excluded.
Differential diagnosis
- Seminoma:
- See Microscopic (histologic) description in seminoma section
- Embryonal carcinoma:
- See Microscopic (histologic) description in embryonal carcinoma section
- Choriocarcinoma:
- See Microscopic (histologic) description in choriocarcinoma section
- Immature teratoma:
- Immature teratoma may mimic yolk sac tumor due to varied growth pattern but presence of neuroepithelium indicates former
- Thymic carcinoma:
- Can mimic solid growth pattern of yolk sac tumor
- CD117 positive but SALL4, glypican 3, AFP negative
- Metastatic carcinoma:
- Metastatic gonadal yolk sac tumor
- Other metastatic carcinomas may be distinguished on morphology and immunohistochemical profile
- Lymphoma:
- Discohesive and homogenous tumor cells
- Lacks cytokeratin expression, positive for lymphoid markers
- CD30 is positive in some mediastinal lymphomas
A 35 year old man presented with signs and symptoms of superior vena cava syndrome. On radiology, a mass was found in the anterior mediastinum, pushing on to the great vessels. It was resected. The photomicrograph above shows the histologic features. The tumor stained with SALL4 and OCT3/4 and was negative for CD30. What is the most likely diagnosis in this case?
- Embryonal carcinoma
- Seminoma
- Teratoma
- Yolk sac tumor
Comment Here
Reference: Germ cell tumors
- Embryonal carcinoma
- Immature teratoma
- Mature teratoma
- Seminoma
- Yolk sac tumor
Comment Here
Reference: Germ cell tumors
