
Mediastinum
Cystic lesions
Bronchogenic cyst
Editorial Board Member: Carolyn Glass, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 9 November 2022
Last staff update: 10 November 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed search: Bronchogenic cyst lung pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Briski LM, Konopka K. Bronchogenic cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mediastinumbronchogenic.html. Accessed April 1st, 2025.
Definition / general
- Benign congenital malformation of tracheobronchial tree
Essential features
- Benign congenital malformation arising from abnormal budding of primitive foregut during gestation
- Occurs in mediastinum, lung, head and neck, skin, abdomen, retroperitoneum
- Unilocular cyst lined by respiratory type epithelium
- Cyst wall recapitulates bronchial wall with variable amounts of seromucinous glands, cartilage and smooth muscle
- Excellent prognosis with complete surgical excision
Terminology
- Bronchial cyst
- Noncommunicating bronchopulmonary foregut malformation
ICD coding
Epidemiology
- Rare; prevalence of approximately 1 per 42,000 and 1 per 68,000 admissions in 2 hospital series (Ann Thorac Surg 1987;44:491, Ann Surg 1952;136:777)
- Most commonly pediatric patients
- Several cases reported in adults (Acta Otorhinolaryngol Ital 2009;29:36)
- No definite sex predilection reported overall
- For neck lesions, M:F = 3 - 4:1 (Arch Otolaryngol Head Neck Surg 2008;134:1165, Acta Otorhinolaryngol Ital 2009;29:36)
Sites
- Depends on stage of development when malformation occurs
- Most common in thorax: mediastinum (early in gestation), lung (later in gestation)
- Ectopic locations: head and neck (usually midline; less commonly lateral or subcutaneous), abdomen, retroperitoneum (Acta Otorhinolaryngol Ital 2009;29:36, Am Surg 2005;71:1034)
Pathophysiology
- Arises from abnormal budding of primitive ventral foregut
- Usually occurs between 26 - 40 days of gestation
Etiology
- No known causes or risk factors
Clinical features
- Most present with symptomatic disease
- Approximately 50% present with pain (Lung 2008;186:55, Am Surg 2005;71:1034)
- Respiratory symptoms (cough, dyspnea, hemoptysis) (Lung 2008;186:55)
- Respiratory distress may result from tracheal compression
- Gastrointestinal symptoms (dysphagia, nausea, vomiting)
- Occasionally fever, other constitutional symptoms or infection
- Asymptomatic presentation uncommon
- True prevalence of asymptomatic disease unknown
Diagnosis
- Radiologic imaging (US, CT, MRI)
- Cytology (FNA) (J Bronchology Interv Pulmonol 2015;22:195)
- Histopathology (surgical excision)
Radiology description
- Solitary well circumscribed cyst
- Multiple modalities may be utilized (US, MRI, CT)
- US demonstrates fluid - fluid level with anechoic upper part and hyperechoic lower part (J Bronchology Interv Pulmonol 2017;24:153)
- MRI demonstrates high signal intensity on both T1 weighted image and T2 weighted image (Clin Radiol 2019;74:976.e19)
Radiology images
Images hosted on other servers:

Fluid filled mediastinal mass

Mediastinal mass with high signal intensity on T1 and T2

Mediastinal bronchogenic cyst

Well circumscribed
intrapulmonary
bronchogenic cyst

Esophageal bronchogenic cyst
Prognostic factors
- Excellent long term prognosis with complete excision
- Incomplete excision increases risk of local recurrence
- Rarely life threatening due to tracheal compression, pericardial location
- Rare reported cases of carcinoma arising in bronchogenic cysts (Ann Thorac Cardiovasc Surg 2018;24:247, Arch Bronconeumol 2017;53:523, Laryngoscope 2011;121:1446)
Case reports
- 6 month old girl with acute respiratory distress due to compression of trachea by mediastinal bronchogenic cyst (Front Pediatr 2020;8:101)
- 6 year old girl with cervical bronchogenic cyst presenting as an asymptomatic lump in the lateral neck (Srp Arh Celok Lek 2015;143:317)
- 39 year old man with ileal bronchogenic cyst discovered on abdominal CT (World J Clin Cases 2018;6:807)
- 70 year old man with exertional dyspnea due to intrapulmonary bronchogenic cyst (Respirol Case Rep 2018;6:e00350)
- 77 year old woman presented with ventricular fibrillation due to a bronchogenic cyst of the atrioventricular septum (HeartRhythm Case Rep 2017;3:389)
Treatment
- Complete surgical excision recommended for symptomatic patients
- Aspiration or ablation for nonresectable lesions / high risk patients (J Bronchology Interv Pulmonol 2015;22:195)
- Observation acceptable for asymptomatic patients
Clinical images
Images hosted on other servers:

Submucosal esophageal bronchogenic cyst

Polypoid endobronchial bronchogenic cyst
Gross description
- Unilocular thin walled cyst with smooth surface
- Filled with serous or mucinous fluid
- May be turbid or hemorrhagic if infected or previously aspirated / biopsied
- Reference: Semin Pediatr Surg 2003;12:17
Gross images
Images hosted on other servers:

Unilocular cyst with mucoid material
Microscopic (histologic) description
- Cyst lined by respiratory type epithelium
- Ciliated pseudostratified columnar cells
- Variable numbers of goblet cells
- Filled with serous or mucinous material
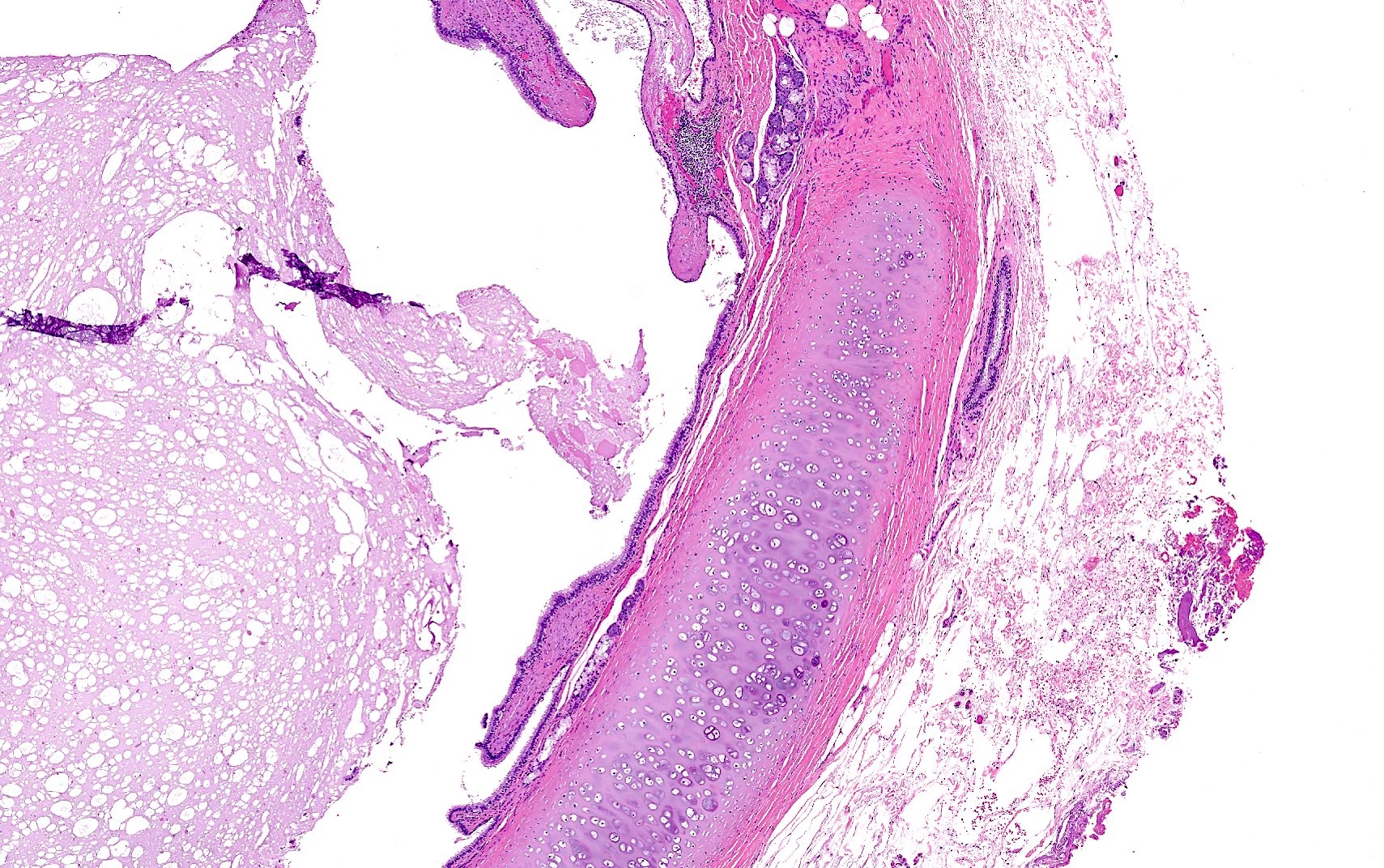
- Cyst wall components (variable)
- Seromucinous glands
- Hyaline cartilage
- Smooth muscle
- Changes associated with infection or prior procedure
- Acute and chronic inflammation with epithelial denudation
- Hemorrhage with hemosiderin laden macrophages
- Squamous metaplasia
- Cholesterol clefts
- Fibrosis
- Reference: Semin Pediatr Surg 2003;12:17
Microscopic (histologic) images
Contributed by Laurence M. Briski, M.D.
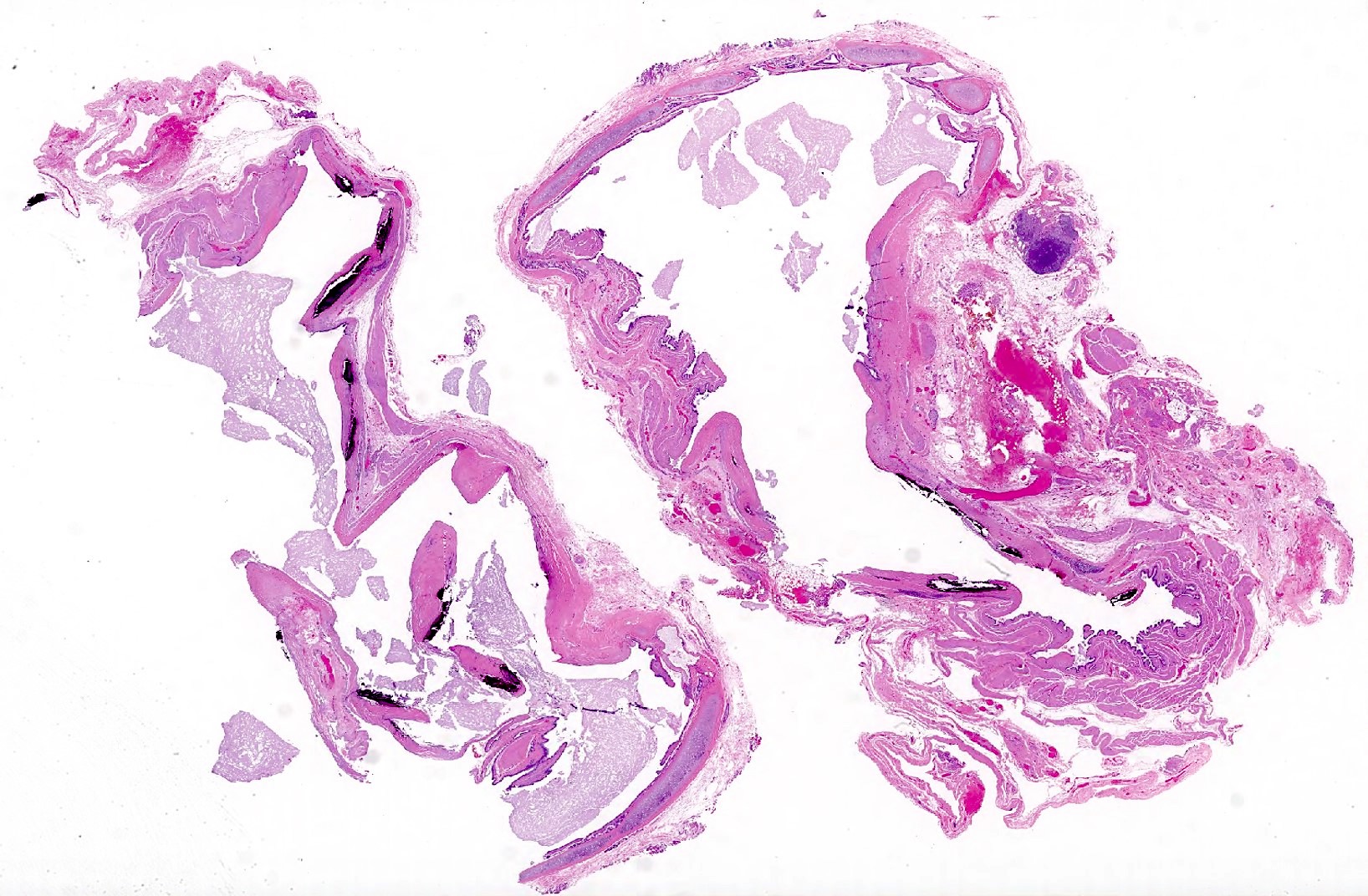
Unilocular cyst

Recapitulation of bronchial structure
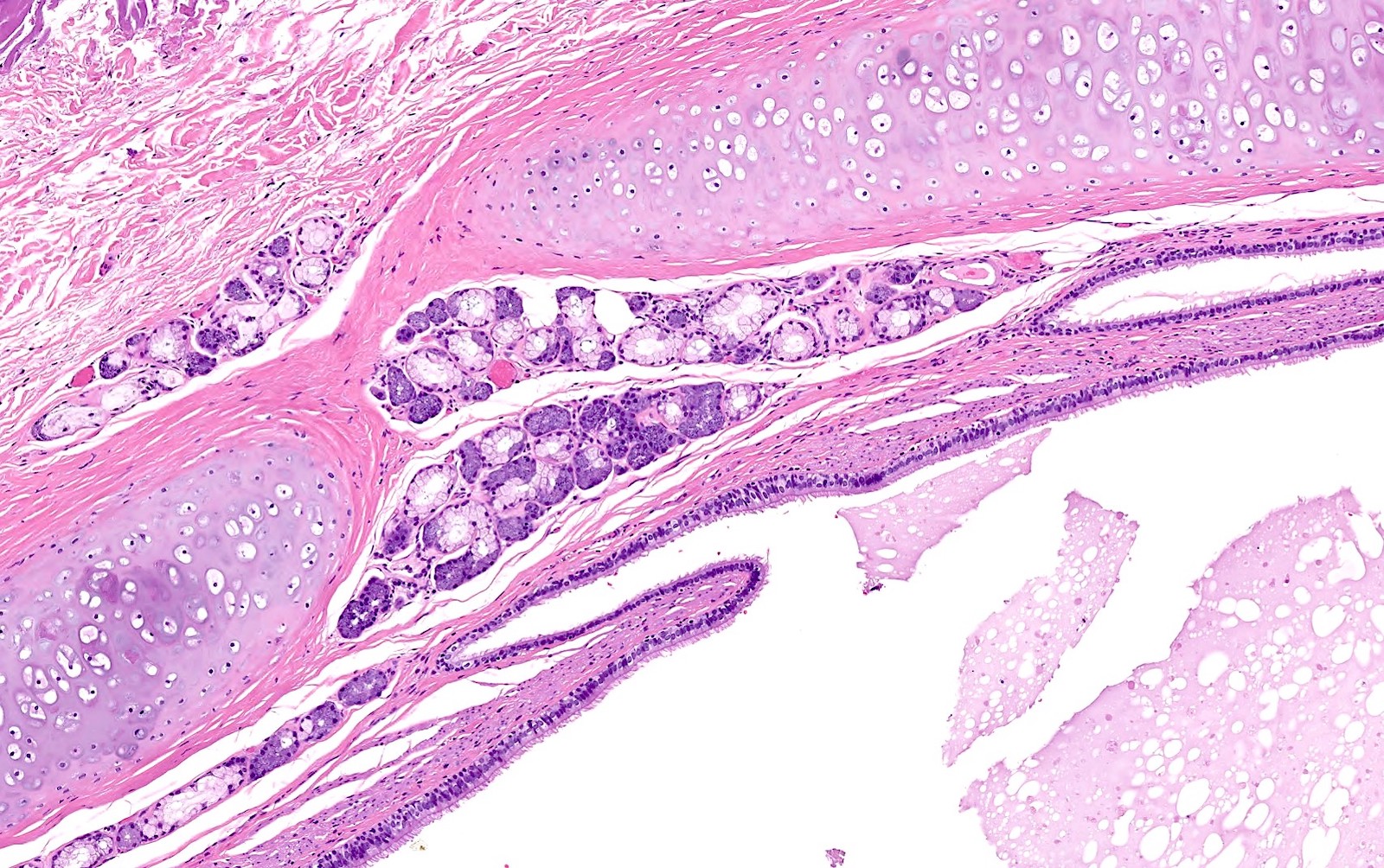
Cyst wall components

Foci of smooth muscle
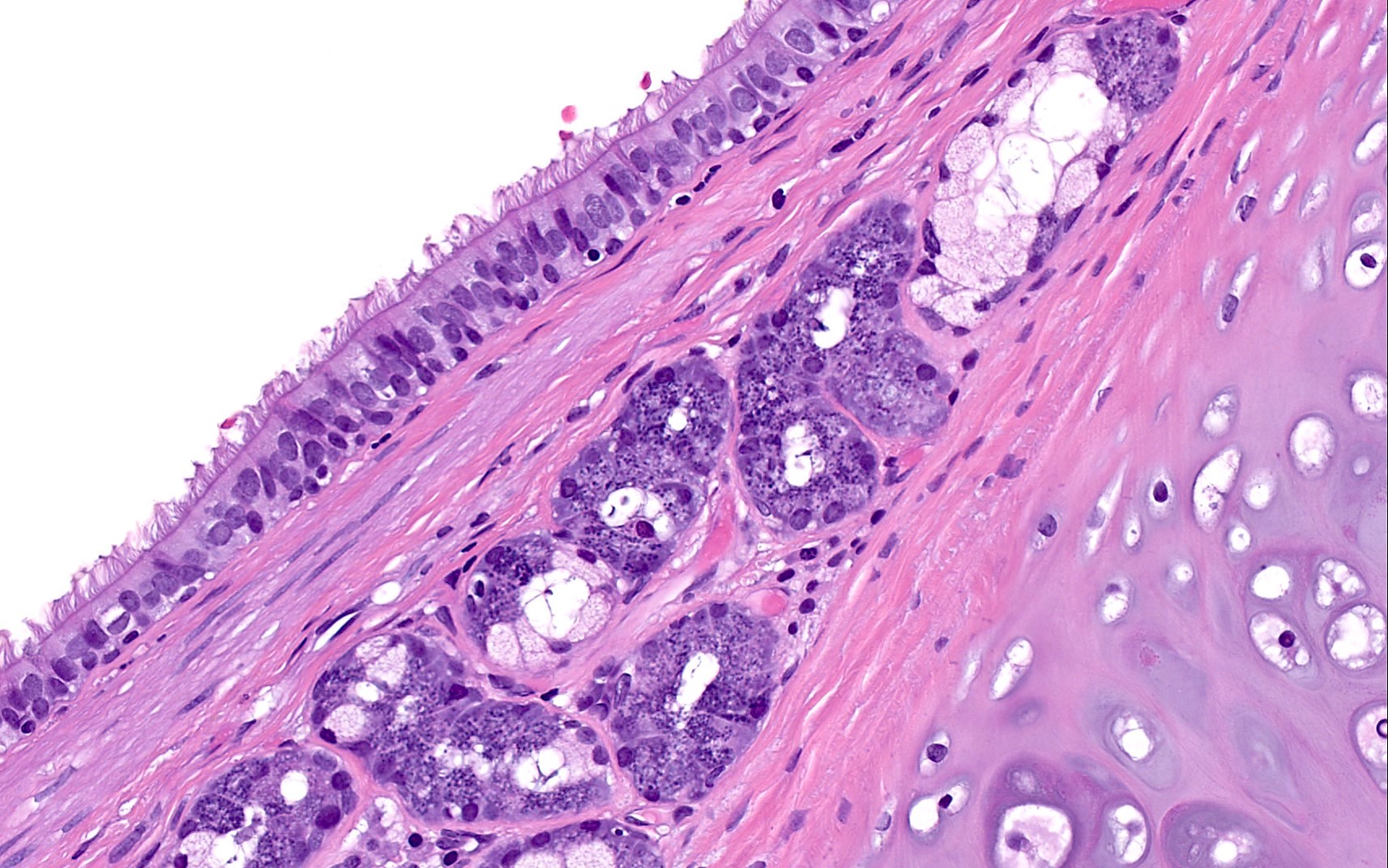
Ciliated respiratory epithelium
Cytology description
- Ciliated columnar (respiratory type) epithelial cells
- Macrophages (and other cystic contents)
- Acute and chronic inflammatory cells
- Serous or mucinous material
- Rarely cartilage or smooth muscle spindle cells
- Reference: J Bronchology Interv Pulmonol 2015;22:195
Cytology images
Images hosted on other servers:

Cystic contents (Diff-Quik stain)
Positive stains
- Cytokeratin 7 (100%, based on one series of 22 bronchogenic cysts) (Am J Clin Pathol 2008;130:265)
Negative stains
- CDX2 (0%) (Am J Clin Pathol 2008;130:265)
- Chromogranin (9%)
- TTF1 (18%)
- Cytokeratin 20 (41%) (rare cells)
Sample pathology report
- Soft tissue, thorax, excision:
- Bronchogenic cyst
Differential diagnosis
- Cystic teratoma:
- Usually has a solid component
- Lined by variable mixtures of gastrointestinal, squamous and respiratory epithelium
- Contains tissues derived from all 3 germ cell layers
- Some cases contain immature tissues, nuclear atypia or tumor necrosis
- Thyroglossal duct cyst:
- Lined by respiratory, cuboidal or squamous epithelium
- Contains thyroid tissue (follicles) in cyst wall
- Lacks cartilage and smooth muscle
- Esophageal duplication cyst:
- Lined by stratified squamous or gastrointestinal epithelium
- Contains double smooth muscle layer
- Attached to esophageal wall
- Branchial cleft cyst:
- Typically lined by stratified squamous epithelium
- Contains lymphoid aggregates with reactive germinal centers
- Often filled with keratinaceous debris
- Lacks cartilage and smooth muscle
- Dermoid cyst:
- Lined by stratified squamous epithelium
- Contains hair and skin appendages
- Filled with keratinaceous or sebaceous material
- Lacks cartilage and smooth muscle
- Abscess:
- No true lining; may contain foci of squamous metaplasia
- Filled with suppurative inflammation
- Lacks cartilage and smooth muscle
Additional references
Board review style question #1
A 1 month old girl presents with acute respiratory distress and failure to thrive. Imaging studies reveal a 3.5 cm cystic mediastinal mass compressing her trachea. The lesion is excised and shown above.
Which of the following statements accurately describes this lesion?
- Congenital cyst arising from abnormal budding of the primitive ventral foregut
- Congenital cyst derived from remnants of the second branchial apparatus
- Congenital cyst derived from the thyroglossal duct
- Mature germ cell tumor derived from all 3 germ cell layers
Board review style answer #1
A. Congenital cyst arising from abnormal budding of the primitive ventral foregut. The lesion shown is a bronchogenic cyst. Teratomas are mature germ cell tumors derived from all 3 germ cell layers (answer D); branchial cleft cysts are derived from remnants of the second branchial apparatus (answer B); thyroglossal duct cysts are derived from the thyroglossal duct (answer C).
Comment Here
Reference: Bronchogenic cyst
Comment Here
Reference: Bronchogenic cyst
Board review style question #2
Each of the following immunohistochemical markers may be positive in cystic teratomas of the mediastinum. Which is most reliably negative in bronchogenic cysts and therefore useful in the distinction between these 2 entities?
- CDX2
- Cytokeratin 7
- Cytokeratin 20
- TTF1
Board review style answer #2
A. CDX2. Based on one series of 22 bronchogenic cysts, CDX2 was negative in all 22 cases. The other listed immunohistochemical stains had varying levels of positivity in this cohort (from positivity with CK7 in 100% of cases to positivity with TTF1 in 18% of cases) (Am J Clin Pathol 2008;130:265).
Comment Here
Reference: Bronchogenic cyst
Comment Here
Reference: Bronchogenic cyst
