

Mandible & maxilla
Cysts of the jaw
Residual cyst
Last author update: 1 April 2014
Last staff update: 8 July 2020
Copyright: 2004-2019, PathologyOutlines.com, Inc.
PubMed Search: Residual cyst [title]



Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Treatment | Microscopic (histologic) description | Differential diagnosis | Additional referencesCite this page: Morrison A. Residual cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillaresidualcyst.html. Accessed December 27th, 2024.
Definition / general
- Inflammatory fibrous and granulation tissue at the apex / periapical region of a tooth not removed / curetted at the time of dental extraction may give rise to residual cyst
Terminology
- Odontogenic cysts: All odontogenic cysts found within the jawbones are inflammatory, developmental or less commonly (and more controversially) neoplastic
- Source epithelium from which odontogenic cysts derive include:
- Rests of Malassez
- Dental lamina rests
- Reduced enamel epithelium
- Degenerated enamel organ
- Rarely crevicular epithelium, or even surface epithelium
- In general, inflammatory odontogenic cysts have proliferative epithelium, and developmental odontogenic cysts have a more uniform epithelium, although inflammation may lead to epithelial proliferation
- Inflammatory odontogenic cysts appear to arise in response to inflammation
- Clinicoradiographic variants include:
- Apical (or periapical cyst, or radicular cyst) radicular cyst: present at root apex
- Lateral radicular cyst: present at the opening of lateral accessory root canals
- Residual cyst remains even after extraction of offending tooth
- Buccal bifurcation cyst
- Clinicoradiographic variants include:
- Developmental odontogenic cysts: have unclear pathogenesis
- Inflammatory odontogenic cysts appear to arise in response to inflammation
- Dental pulp:
- Unmineralized tissue composed of connective tissue, vascular, lymphatic and nervous elements
- Occupies the central cavity of each tooth
- Is a loose connective tissue (Wikipedia: Pulp (tooth) [Accessed 11 June 2018])
- Apical foramen: small opening at the apex of the tooth root that allows passage of neural and vascular supply of tooth
- Periapical granuloma:
- Apical / periapical acute or chronic inflammation admixed with fibrous or granulation tissue
- Is devoid of epithelium (i.e. no cyst lining) which distinguishes it from a periapical cyst
- Periapical granuloma is located at the apex of a necrotic or partially necrotic tooth
- Epithelial rests of Malassez: discrete clusters of residual cells derived from Hertwig epithelial root sheath
- Small spherules of 6 - 8 epithelial cells with high nuclear to cytoplasmic ratio
- Little or no reverse polarity of cells
- Reduced enamel epithelium (REE): ameloblastic and epithelial cells from the outer enamel that overly an unerrupted tooth, as the REE degenerates the underlying tooth is exposed
- Dental lamina: band of epithelium that invades the underlying ectomesenchyme of the future dental arches at 6th week gestation
- Is major component contributing to future tooth formation
- Enamel organ: one recognizable step / stage in the formation of teeth
- Formed from dental lamina
- Crevicular epithelium: epithelium lining the inner aspect of the gingival sulcus
- Source epithelium from which odontogenic cysts derive include:
Epidemiology
- 8% of all jaw cysts
Sites
- Tooth bearing regions (or if dental extraction completed, former tooth bearing region) of maxilla and mandible
Pathophysiology
- Pathophysiology of apical cyst and residual cyst similar
- Activated T cells in periapical granulomas produce cytokines that act on rests of Malassez causing proliferation and altered differentiation leading to cyst formation
- The proliferating epithelial masses become edematous, accumulate fluid and coalesce, forming microcysts containing epithelial and inflammatory cells
- Cyst walls appear to have properties of a semi-permeable membrane, so osmosis contributes to increasing the size of cysts
- Lytic products of the epithelial and inflammatory cells in the cyst cavity provide the greater numbers of smaller molecules which raise the osmotic pressure of the cyst fluid
Etiology
- Trauma, carious lesion or bacterial colonization of developmental anomaly affecting tooth irreversibly injures dental pulp
- Tooth pulp degenerates, inflammation ensues, and inflammatory products escape from tooth via apical foramen and access the surrounding / supporting periapical region of the jaw
Clinical features
- Variable: range from asymptomatic and only incidentally detected on imaging, to expansion of affected jaw region, to pain and drainage
Diagnosis
- By definition, the offending tooth has been removed, therefore the radiographic and clinical differential diagnosis of a radiolucent lesion in the jaws without a documented association to a tooth is broad
- Diagnosis confirmed via removal of lesion and submission for microscopic examination
- Ideal if have radiographic evidence of a necrotic or carious tooth (prior to dental extraction) to correlate
Radiology description
- Round to oval radiolucency of variable size within the tooth bearing regions of jaws at the site of a previous tooth extraction
- As the cyst ages, degeneration of the cellular contents within the lumen occasionally leads to dystrophic calcifications and radiographic opacities
Radiology images
Images hosted on other servers:
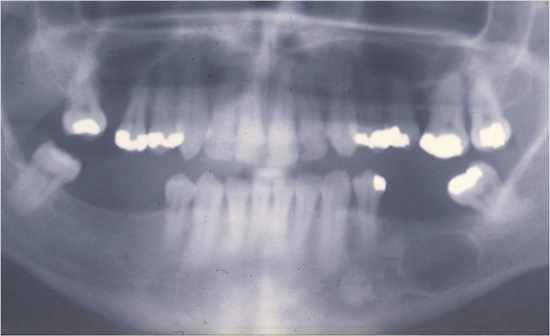
Residual jaw cyst
Prognostic factors
- Vast majority have excellent prognosis
- True residual cysts do not recur after appropriate treatment and are not premalignant - they have no increased risk of squamous cell carcinoma
- Occasionally a secondary pathology, such as squamous cell carcinoma, arises from the epithelial lining of radicular, or other (odontogenic) gnathic cysts; careful patient questioning and clinical examination are necessary to exclude a primary oral mucosal neoplasm or metastases
- Must also rule out an epithelial neoplasm which underwent secondary cystic change
- Histological evidence of cyst lining with transition to epithelial dysplasia and infiltrating squamous carcinoma provides acceptable proof
Treatment
- Any number of odontogenic and nonodontogenic cysts and tumors can mimic the appearance of a residual periapical cyst, therefore, these lesions should be excised surgically, even in the absence of symptoms
- Residual cysts do not recur after appropriate management
- Intraosseous fibrous scars are possible, especially when both cortical plates have been lost; this can give the appearance of a persistent radiolucent lesion
Microscopic (histologic) description
- Epithelial lining of cyst: stratified squamous epithelium which may demonstrate exocytosis, spongiosis, or hyperplasia
- Epithelium may be discontinuous in part and range in thickness from 1 to 50 cell layers
- The majority are 6 - 20 cell layers thick
- The nature of the lining may depend on the age or stage of development of the cyst, or on the intensity of the inflammation
- In early cysts, the epithelial lining may be proliferative and show arcading with an intense associated inflammatory process but, as the cyst enlarges, the lining becomes quiescent and fairly regular with a certain degree of differentiation to resemble a simple stratified squamous epithelium
- Rarely, scattered mucous cells or areas of ciliated pseudostratified columnar epithelium are noted
- Cyst epithelium may also demonstrate:
- Linear or arch shaped calcifications known as Rushton bodies
- The bodies measure up to about 0.1 mm and are linear, straight or curved or of hairpin shape and sometimes they are concentrically laminated
- Although the origin of hyaline bodies remains obscure, it is generally now thought that they represent a secretory product of odontogenic epithelium
- Dystrophic calcifications
- Linear or arch shaped calcifications known as Rushton bodies
- Cyst lumen may demonstrate fluid and cellular debris
- Cyst lumen or wall may demonstrate:
- Cholesterol clefts with multinucleated giant cells, red blood cells and areas of hemosiderin pigmentation
- In histological sections, the cholesterol crystals are dissolved out and clefts are seen surrounded by dense aggregations of multinucleate giant cells
- The cholesterol may be due to disintegrating red blood cells in a form that readily crystallizes and incites a foreign body giant cell reaction
- Cyst wall may demonstrate
- Dense fibrous connective tissue, often with an inflammatory infiltrate containing lymphocytes variably intermixed with neutrophils, plasma cells, histiocytes, and (rarely) mast cells and eosinophils
- Occasionally will contain scattered hyaline bodies (pulse granuloma giant cell hyaline angiopathy)
- These bodies appear as small circumscribed pools of eosinophilic material that exhibits a corrugated periphery of condensed collagen often surrounded by lymphocytes and multinucleated giant cells
- Spicules of remodeling bone
- Russell bodies are commonly seen
Differential diagnosis
- Parameters:
- Radiograph demonstrates radiolucent lesion in toothbearing region of jaws without a close association to the periapical region of tooth
- Histology shows benign hyperplastic squamous epithelium
- May or may not show spongiosis or acanthosis
- Acute or chronic inflammation may be present
- Unicystic ameloblastoma, inflamed
- Odontogenic keratocyst, inflamed
- Glandular odontogenic keratocyst, inflamed
- Lateral periodontal cyst, inflamed
- Maxillary surgical ciliated cyst, inflamed
Additional references
- Woo: Oral Pathology: A Comprehensive Atlas and Text, 1st Edition, 2012, Regezi: Oral Pathology: Clinical Pathologic Correlations, 6th Edition, 2011, Shear: Cysts of the Oral and Maxillofacial Regions, 4th Edition, 2007, Univ of Missouri - Kansas City, School of Dentistry: Cysts of the Jaws [Accessed 11 June 2018]

