

Mandible & maxilla
Cysts of the jaw
Lateral periodontal cyst and botryoid odontogenic cyst
Last author update: 1 December 2013
Last staff update: 5 December 2021
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Lateral periodontal cyst [title]



Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Pathophysiology | Clinical features | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosisCite this page: Morrison A. Lateral periodontal cyst and botryoid odontogenic cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillalateralperiodontalcyst.html. Accessed November 27th, 2024.
Definition / general
- Non-keratinizing, developmental odontogenic cyst which occurs along the lateral tooth root surface within bone
Terminology
- Epithelial rest of Malassez:
- Derived from Hertwig epithelial root sheath
- Small spherules of 6 - 8 epithelial cells with high nuclear to cytoplasmic ratio; little or no reverse polarity of cells
- Reduced enamel epithelium:
- Enamel is normally composed of two cell layers: inner layer of reduced or atrophied ameloblasts and external layer, probably stratum intermedium cells
- Reduced enamel epithelium is normally found overlying an unerupted, otherwise developed tooth
- Dental lamina:
- Band of epithelial tissue derived from ectoderm that initiates tooth development in utero
- After tooth development, the dental lamina disintegrates into small nests, most of which are reabsorbed, but some persist as dental lamina rests (rests of Serres)
- Gingival cyst:
- Lateral periodontal cyst (LPC) has been pathogenetically linked to the gingival cyst of the adult
- The former is believed to arise from dental lamina remnants within bone and the latter from dental lamina remnants in soft tissue between the oral epithelium and the periosteum (rests of Serres)
- The close relationship between the two entities is further supported by their similar distribution in sites containing a higher concentration of dental lamina rests and their identical histology
- Botryoid odontogenic cyst:
- Multicystic variant of lateral periodontal cyst (LPC), generally larger (5 - 45 mm) with higher recurrence rates (up to 33%) than LPC
- Controversial: some regard the botryoid odontogenic cyst (BOC) as a variant of LPC, others view BOC as distinct entity because it can be larger in size, has a polycystic radiographic appearance (occasionally can be unilocular) and has higher rate of recurrence
Epidemiology
- Usually 5th to 7th decade of life
- Rare in patients less than 30 years of age
- Favor males 2:1
- Accounts for less than 2% of all jaw cysts
- Very rarely multifocal
Sites
- Most common adjacent to roots of cuspid or bicuspid teeth
- 60 - 80% occur in mandibular premolar-canine-lateral incisor area, but favors premolar-canine region
- When occur in maxilla, usually involve this same tooth region but favors incisor area
Pathophysiology
- Origin of LPC still debated with histologic and developmental evidence from various researchers providing support for the lesion developing from either dental lamina, reduced enamel epithelium or epithelial rests of Malassez
- Most sources regard the cyst as originating from rests of dental lamina
Clinical features
- Usually asymptomatic
- Can cause painless expansion of bone
- Rarely perforates bone to communicate with gingival surface
- Associated with vital teeth, however prior endodontic treatment or tooth extraction can confound the diagnosis
Radiology description
- Radiographic appearance is not specific for LPC
- Well demarcated, round to elongated tear drop shaped radiolucent lesion associated with lateral aspect of tooth root
- Rare to exceed 1.0 cm in size
- Root divergence uncommon
- Most commonly is a solitary lesion, rarely affects multiple sites (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:225)
- Most cysts are unilocular but occasionally appear polycystic
- When polycystic, have been termed botryoid odontogenic cysts
Radiology images
Images hosted on other servers:

Tear dropshaped radiolucency

Orthopantamograph

Healing after 6 months

Radicular triangular radiolucency
Prognostic factors
- Good prognosis with rare recurrence
- Recurrence reported with botryoid odontogenic cyst
Case reports
- 13 year old girl with unusual clinicoradiographic presentation (J Dent (Tehran) 2012;9:265)
- 14 year old boy with bilateral lateral periodontal cyst (BMJ Case Rep 2013 May 10;2013)
- 38 year old man with pigmented lateral periodontal cyst and other pigmented odontogenic lesions (Oral Dis 1996;2:299)
Treatment
- Enucleation, curettage or excision with preservation of adjacent teeth is adequate for conventional LPC
Clinical images
Images hosted on other servers:

Intra oral swelling

Buccal cortical plate perforation
Gross description
- Thin walled cyst with nodular excrescences within cyst wall
Microscopic (histologic) description
- Thin, generally non-inflamed fibrous connective tissue wall
- Non-keratinized epithelial lining of cuboidal to stratified squamous cells
- Epithelium is 2 - 5 cells thick in most areas
- Foci of PAS+ glycogen rich clear cells interspersed among lining epithelial cells
- Focal nodular areas of epithelial thickening that may have a whorled, swirling architecture and appear in continuity with the epithelial lining
- These mural epithelial plaques extend into the fibrous connective cyst wall or may protrude into cyst lumen
- Epithelial rests (may or may not be clear cells) can be seen in fibrous wall
- LPC may be histologically unicystic or multicystic; microscopic presence of multiple cystic spaces may not correlate with the typical radiographic finding of a unilocular radiolucency
- Botryoid odontogenic cyst has more pronounced mural thickenings / protrusions, comprised of multilocular cysts with thin fibrous septations and typically has a multilocular, often larger radiographic appearance
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
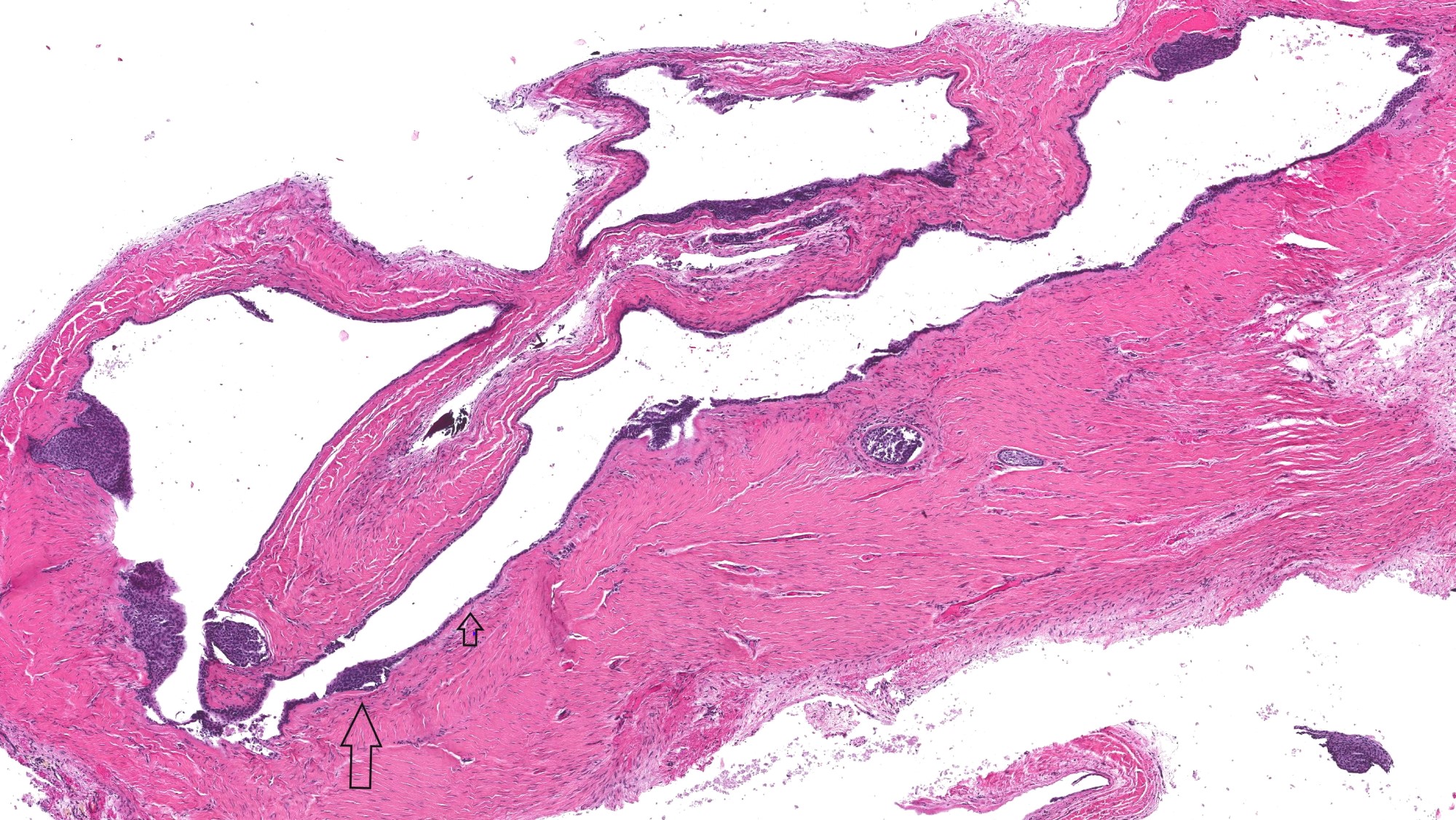
Lateral periodontal cyst
Images hosted on other servers:

Thick lining of a lateral periodontal cyst

Fragmented lining of a Botryoid odontogenic cyst

Typical luminal excrescence

Cystic lumen
Differential diagnosis
- Cystic degeneration of, or unicystic ameloblastoma
- Gingival cyst: represents the gingival soft tissue counterpart of LPC
- Glandular odontogenic cyst
- Odontogenic keratocyst (keratocystic odontogenic tumor)

