
Bone marrow neoplastic
Bone marrow - plasma cell and lymphoid neoplasms
Plasma cell neoplasms
Plasmacytoma
Author: Barina Aqil, M.D.
Editorial Board Members: Anamarija M. Perry, M.D., Alexa J. Siddon, M.D.

Last author update: 17 March 2025
Last staff update: 17 March 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Plasmacytoma

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Flow cytometry description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Aqil B. Plasmacytoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaplasmacytoma.html. Accessed March 30th, 2025.
Definition / general
- Solitary plasma cell neoplasm without the presence of multiple myeloma (MM) or features of end organ damage (CRAB: hypercalcemia, renal insufficiency, anemia and bone lesion)
Essential features
- 2 types: solitary plasmacytoma of bone (SPB) and extramedullary plasmacytoma (EMP)
- EMP commonly involves upper respiratory tract (nasal cavity, paranasal sinuses and nasopharynx)
- Positive stains include CD38, CD138 and MUM1
- Expression of cyclin D1 and CD56 in EMP is noted in older individuals
- Patients with SPB with minimal bone marrow involvement (< 10%) are more likely to develop multiple myeloma than those with no clonal plasma cells by flow cytometry or immunohistochemistry
- Plasmablastic morphology has been noted to have aggressive behavior (Ann Diagn Pathol 2015;19:117)
ICD coding
- ICD-11: 2A83.2 & XH4BL1 - solitary plasmacytoma & plasmacytoma, NOS
Epidemiology
- Occurs in older individuals (median age of 55 - 65 years) (ScientificWorldJournal 2012;2012:895765, BMC Cancer 2017;17:13)
- M > F (Cancer Med 2021;10:386, ScientificWorldJournal 2012;2012:895765, BMC Cancer 2017;17:13)
- SPB accounts for ~4 - 5% and EMP comprises 1 - 3% of plasma cell neoplasms (J Hematol Oncol 2018;11:10, Eur J Haematol 2017;99:216)
- Special form of EMP with IgA expression presents in lymph nodes of the head and neck region and occurs in younger patients with various forms of immune dysregulation
Sites
- SPB involves spine, pelvis, ribs, skull and long bones (Am J Hematol 2012;87:647, Ann Hematol 2012;91:1785, Cancer Med 2021;10:462)
- EMP most commonly affects upper respiratory tract and less commonly lungs, gastrointestinal tract, lymph nodes, skin and genitourinary tract (Cancer 1999;85:2305, J Pathol 2005;205:92, Clin Med (Lond) 2020;20:e191, J Cancer Res Clin Oncol 2021;147:1773, Am J Clin Pathol 2001;115:119, BMC Cancer 2017;17:13)
Pathophysiology
- Cytogenetically, EMP and multiple myeloma are closely related; however, the distribution of IGH translocation partners is different, with the notable absence of t(11;14) in EMP (Haematologica 2008;93:623, Am J Dermatopathol 2013;35:357)
Etiology
- Hypothesis behind its occurrence is chronic antigenic exposure
- It is also known to occur in patients with immunodeficiency or immune dysregulation (Am J Clin Pathol 2017;147:129)
Clinical features
- Depending on the location, the presenting features vary; features include pain, swelling, headache, dysphagia and fracture, vary (Ann Hematol 2012;91:1785)
- Some cases may have an associated paraneoplastic syndrome (Lancet 2020;396:e21, Am J Hematol 2021;96:872)
- TEMPI syndrome (telangiectasia, elevated erythropoietin and erythrocytosis, monoclonal gammopathy, perinephric fluid collection and intrapulmonary shunting)
- POEMS (polyneuropathy, organomegaly, endocrinopathy, myeloma protein and skin changes)
- AESOP syndrome (adenopathy and extensive skin patch overlying plasmacytoma)
Diagnosis
- Clonal plasma cells without associated monotypic B cells in a biopsy demonstrating involvement of bone or extramedullary site
- No other lesions detected on imaging studies
- < 10% monotypic plasma cells on bone marrow biopsy
- No evidence of end organ damage (CRAB)
- References: Mediterr J Hematol Infect Dis 2017;9:e2017052, Lancet Oncol 2014;15:e538
Laboratory
- Detection of serum or urine paraprotein on electrophoresis / immunofixation
- Increased free kappa or lambda light chains
- Most common paraproteins include IgG, IgA and light chains (Bence-Jones protein) (Ann Hematol 2012;91:1785, Int J Radiat Oncol Biol Phys 2020;106:589, Clin Med (Lond) 2020;20:e191)
- Elevated β2 microglobulin
- Evaluation to rule out multiple myeloma: serum calcium, creatinine and bone marrow biopsy
Radiology description
- Imaging shows solitary lytic bone lesion (in SPB) or an extramedullary mass (in EMP)
Prognostic factors
- Cytogenetic abnormalities similar to multiple myeloma are seen in plasmacytoma but they do not have much prognostic significance
- Progression risk to multiple myeloma is higher for SPB (60 - 85% after 10 years) than for EMP (12 - 35% after 10 years) but the presence of a minimal infiltrate of clonal plasma cells (< 10%) in the bone marrow (BM) as detected by flow cytometry or immunohistochemistry has a strong association (Blood 2014;124:1300, Blood 2014;124:1296, Lancet Oncol 2014;15:e538)
- 3 year progression rate to multiple myeloma is ~60% for SPB with the presence of clonal BM plasma cells versus 6 - 12% without, compared to ~20% for EMP with and 6% without clonal BM plasma cells
- Risk factors associated with progression to multiple myeloma (Hematology Am Soc Hematol Educ Program 2005;2005:373, BMC Cancer 2006;6:118, ScientificWorldJournal 2012;2012:895765, Clin Med (Lond) 2020;20:e191, Am J Clin Oncol 2020;43:709)
- Size of lesion > 5 cm
- Advanced age
- Persistent paraprotein > 1 year after therapy
- References: Cancer 1999;85:2305, Eur J Haematol 2017;99:216, Br J Haematol 2010;151:525, J Hematol Oncol 2018;11:10, J Pathol 2005;205:92
Case reports
- 33 year old woman presented with vertigo and peripheral facial nerve palsy (World Neurosurg 2020;134:10)
- 47 year old man, previously diagnosed with chronic osteomyelitis, presented with repeated discharge and ulceration in right tibia (Medicine (Baltimore) 2023;102:e33307)
- 54 year old woman with EMP of the right mainstem bronchus (Ann Thorac Surg 2019;108:e119)
- 71 year old man with progressive fatigue in the setting of diffuse hypermetabolic lymphadenopathy throughout his chest, abdomen and pelvis (J Med Case Rep 2019;13:153)
- 74 year old woman with EMP involving larynx (Radiologia (Engl Ed) 2022;64:69)
Treatment
- Treatment of plasmacytoma depends on the type (SPB or EMP) and the location
- SPB: radiation therapy (most common) or rarely surgery (kyphoplasty, vertebroplasty) (World Neurosurg 2020;134:e790)
- EMP: radiation, surgery, chemotherapy or immunotherapy
- Chemotherapy is considered for patients with persistent disease or tumors > 5 cm in size (Int J Radiat Oncol Biol Phys 2020;106:589, Ann Oncol 2021;32:309)
Gross description
- Soft gelatinous mass on cut section
Microscopic (histologic) description
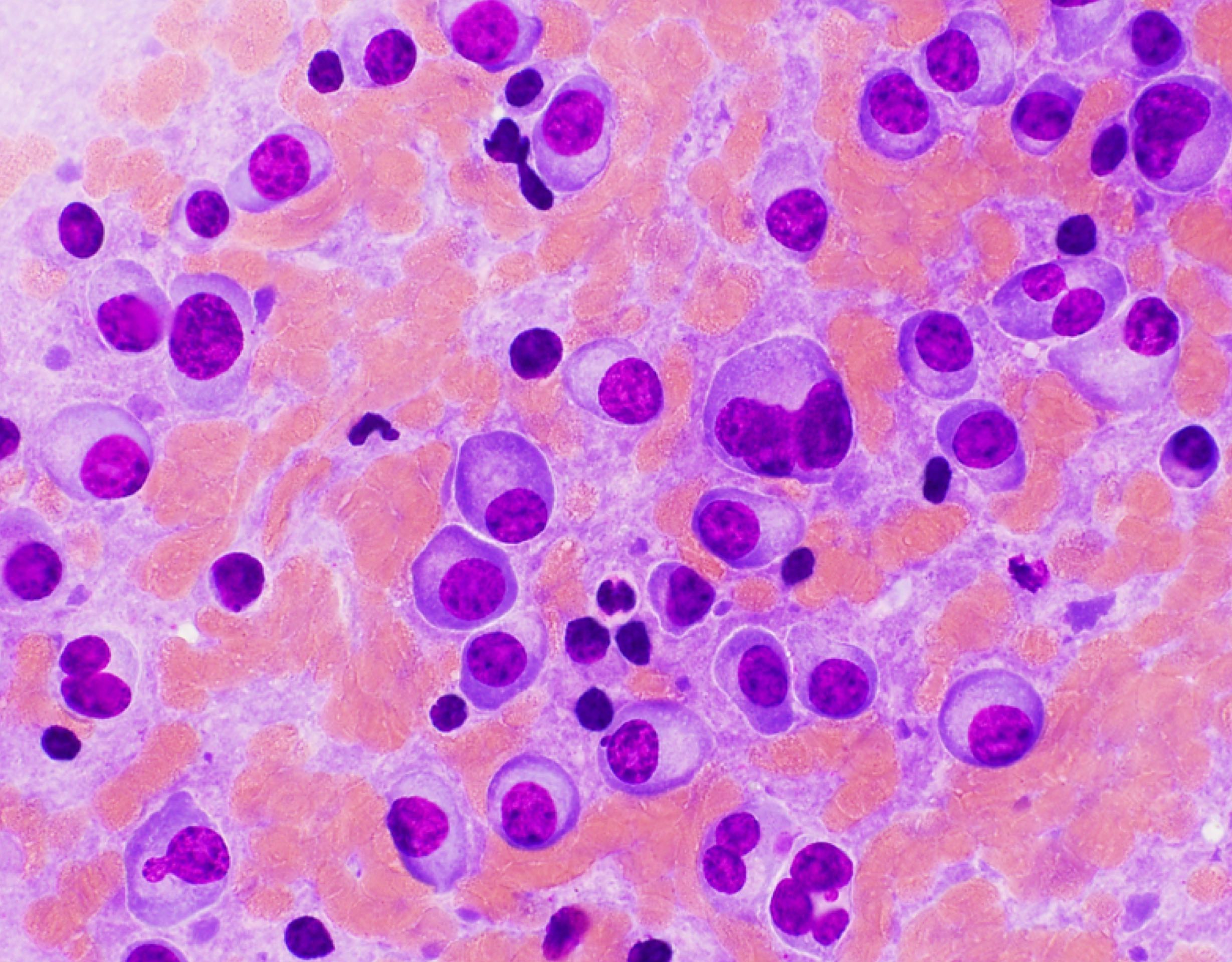
- Sheets of plasma cells with varying morphology ranging from normal appearing to large atypical plasma cells with prominent nucleoli to plasmablastic or anaplastic morphology (Am J Clin Pathol 2001;115:119, J Clin Oncol 2012;30:e91, Skeletal Radiol 2018;47:995)
- Russell or Dutcher bodies may be seen
- Associated amyloid deposition (Ann Diagn Pathol 2015;19:117)
Microscopic (histologic) images
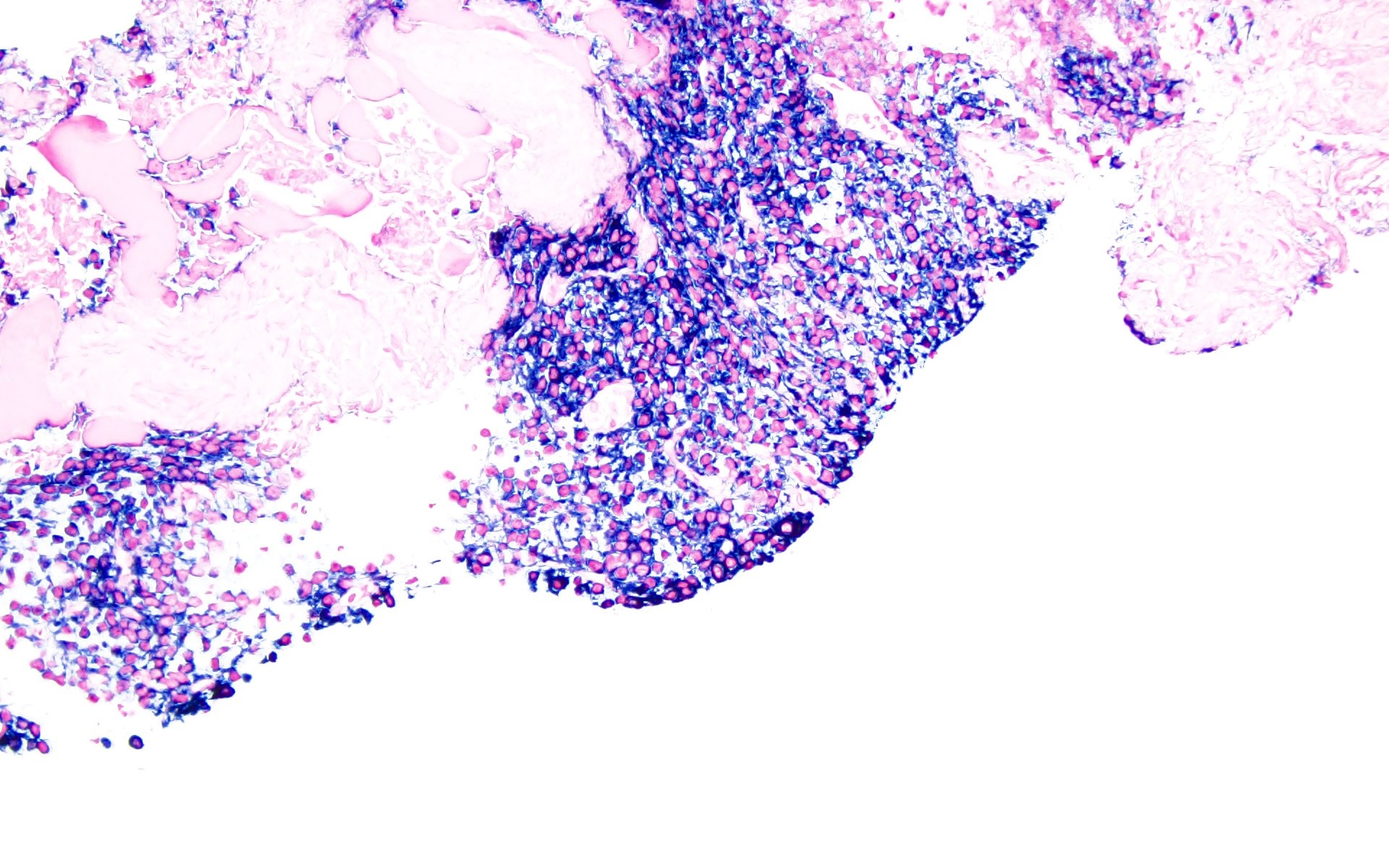
Contributed by Barina Aqil, M.D.

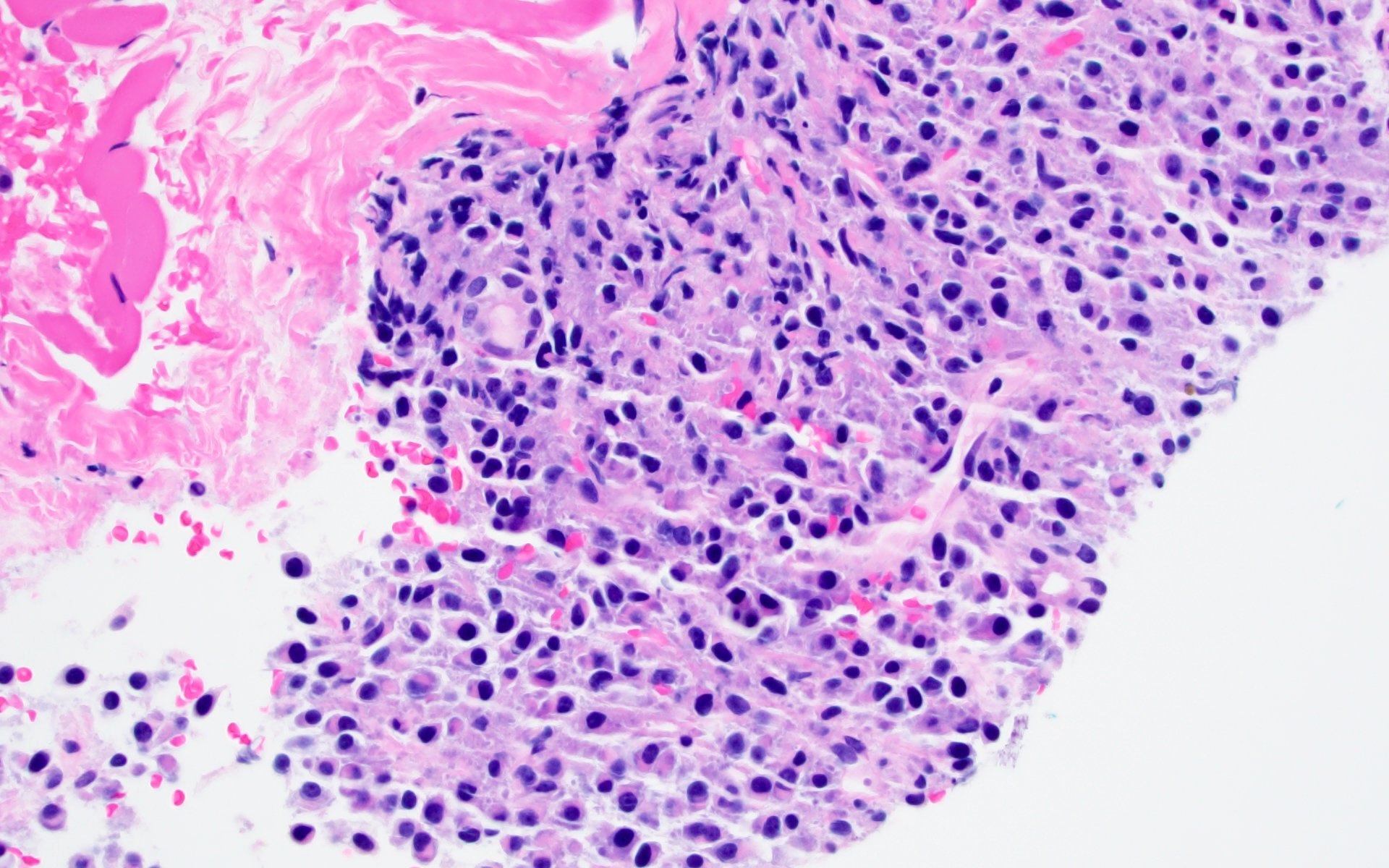
Plasma cell infiltrate

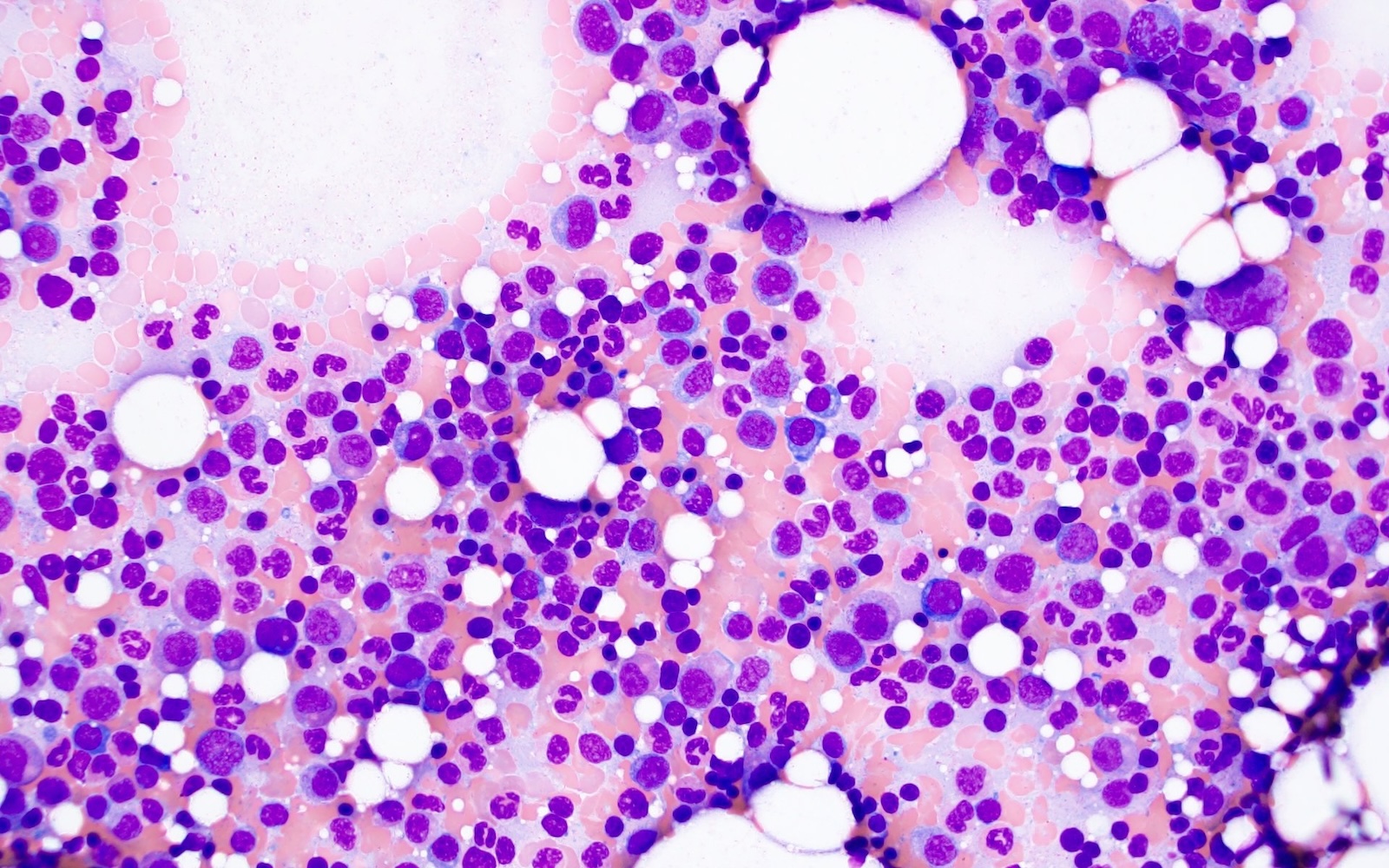
Bone marrow aspirate

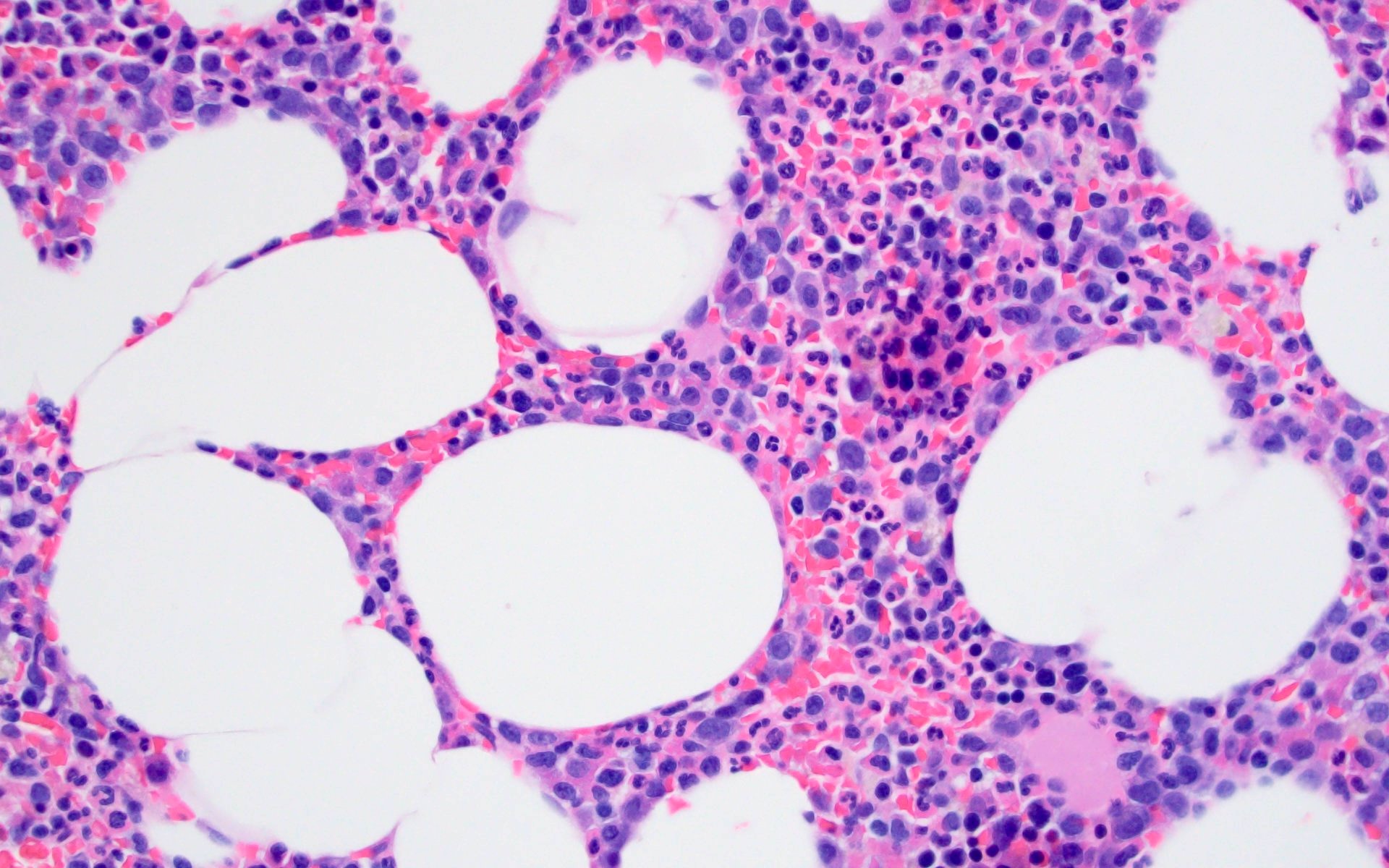
Bone marrow clot section
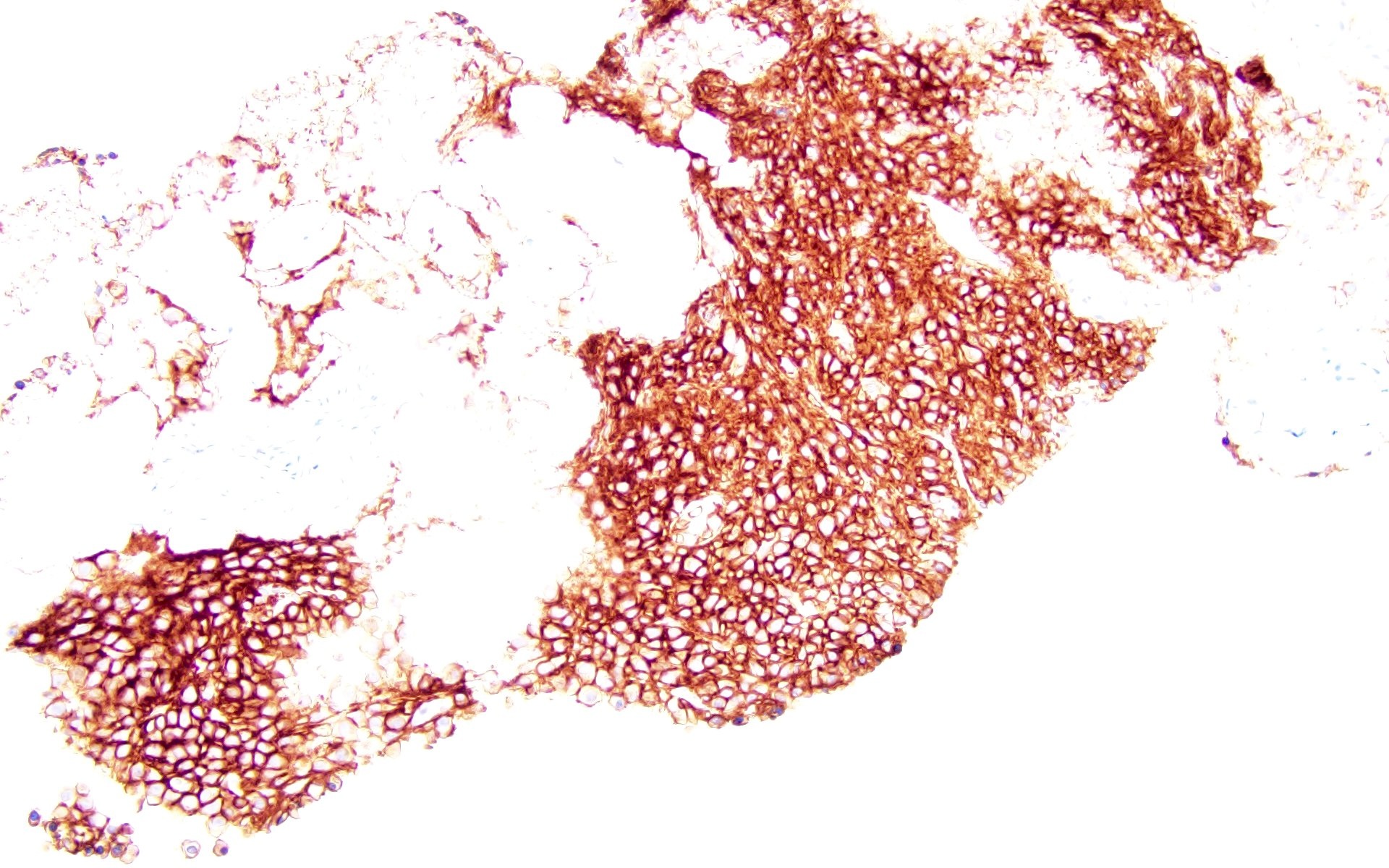
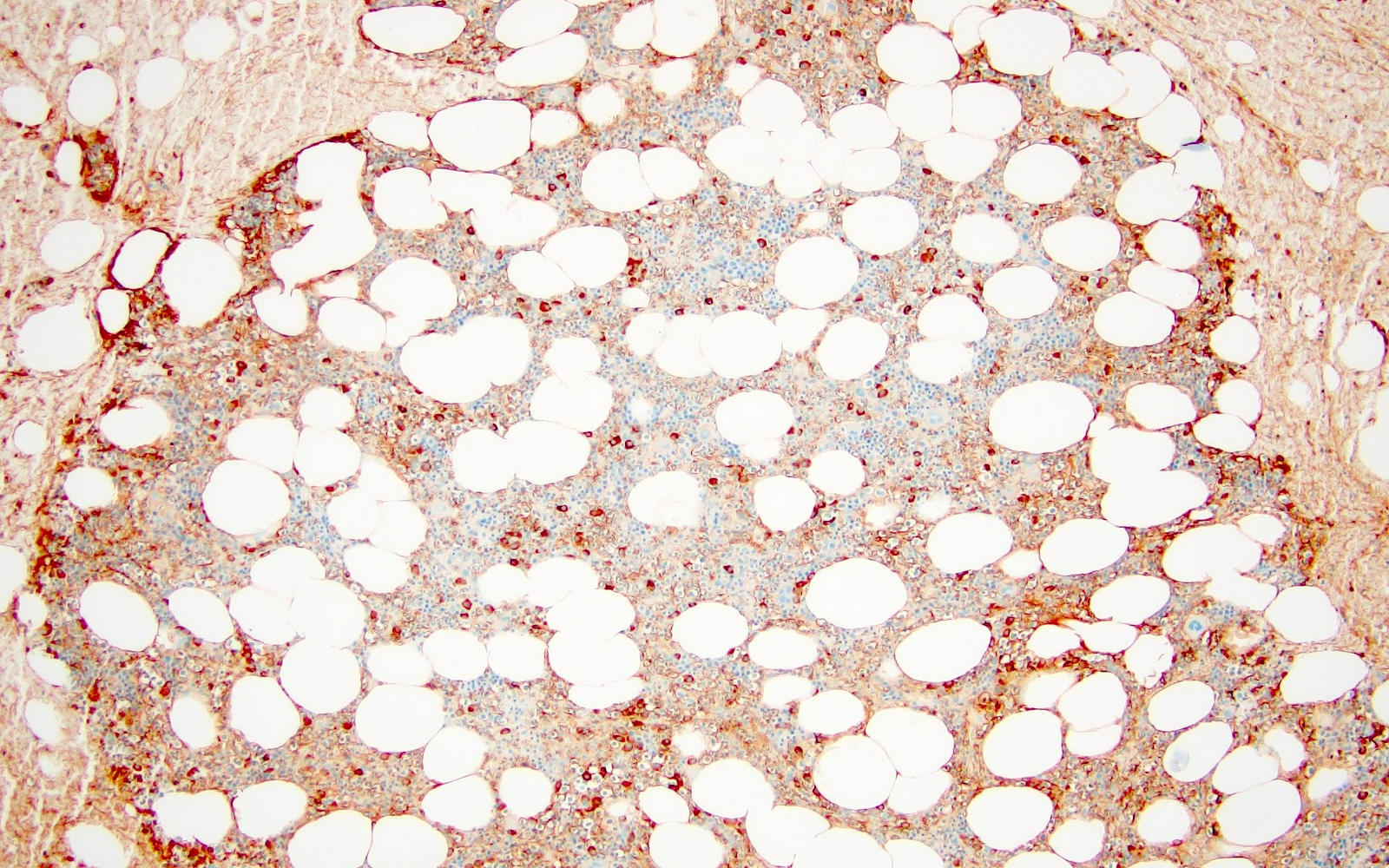
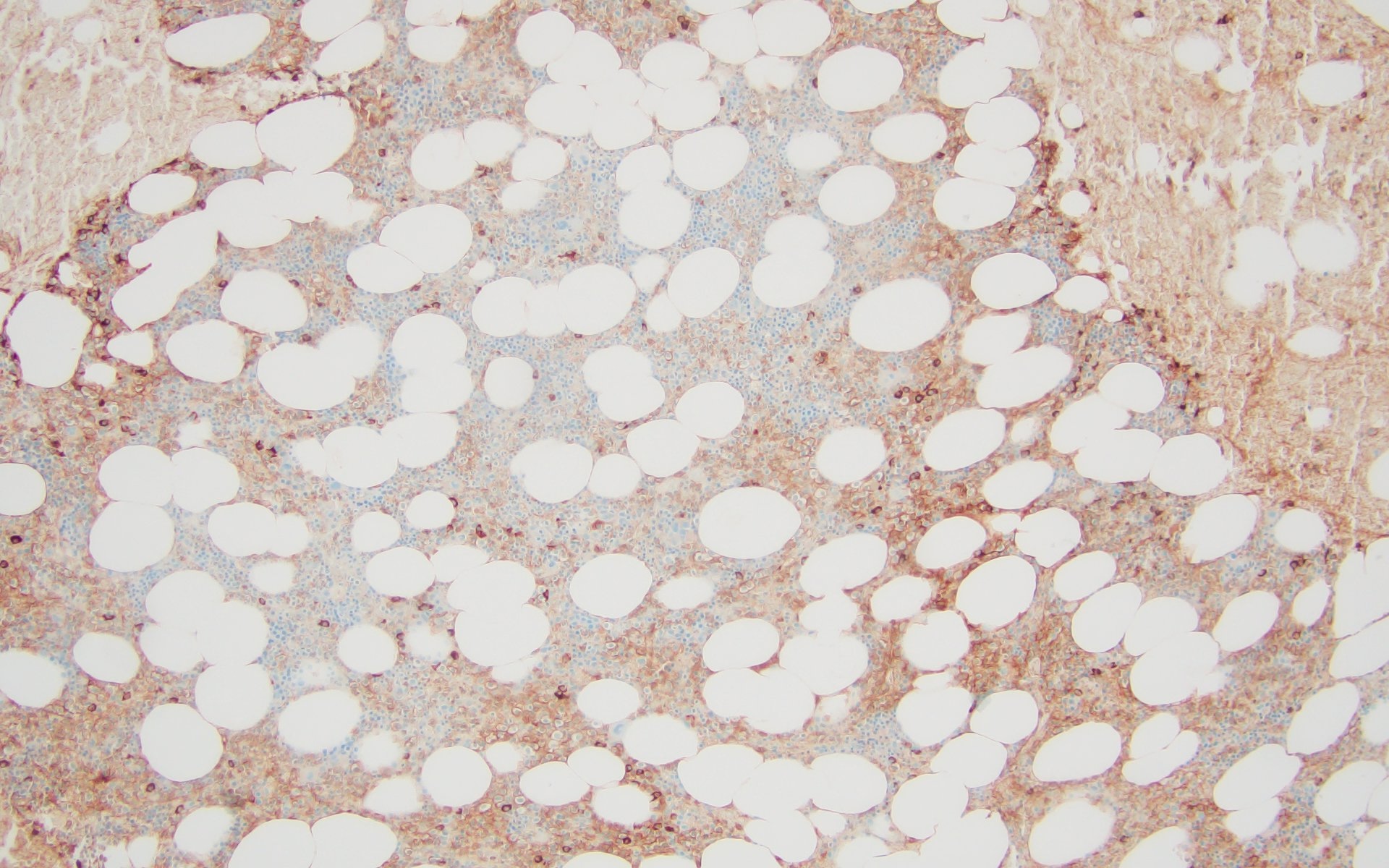
Positive for CD138
Kappa restricted
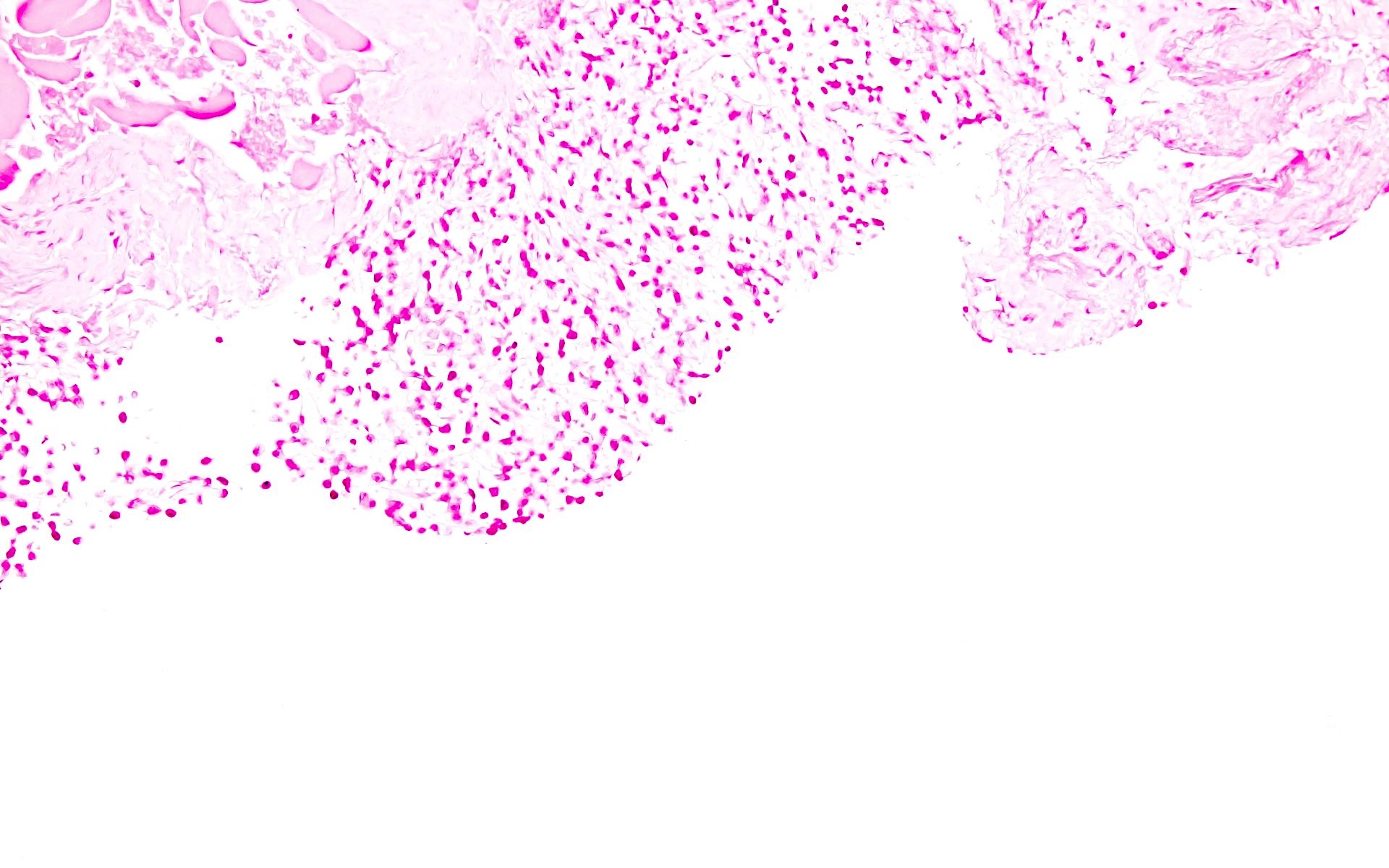
Negative for lambda

Negative for CD20

Negative for CD117

Negative for BCL1
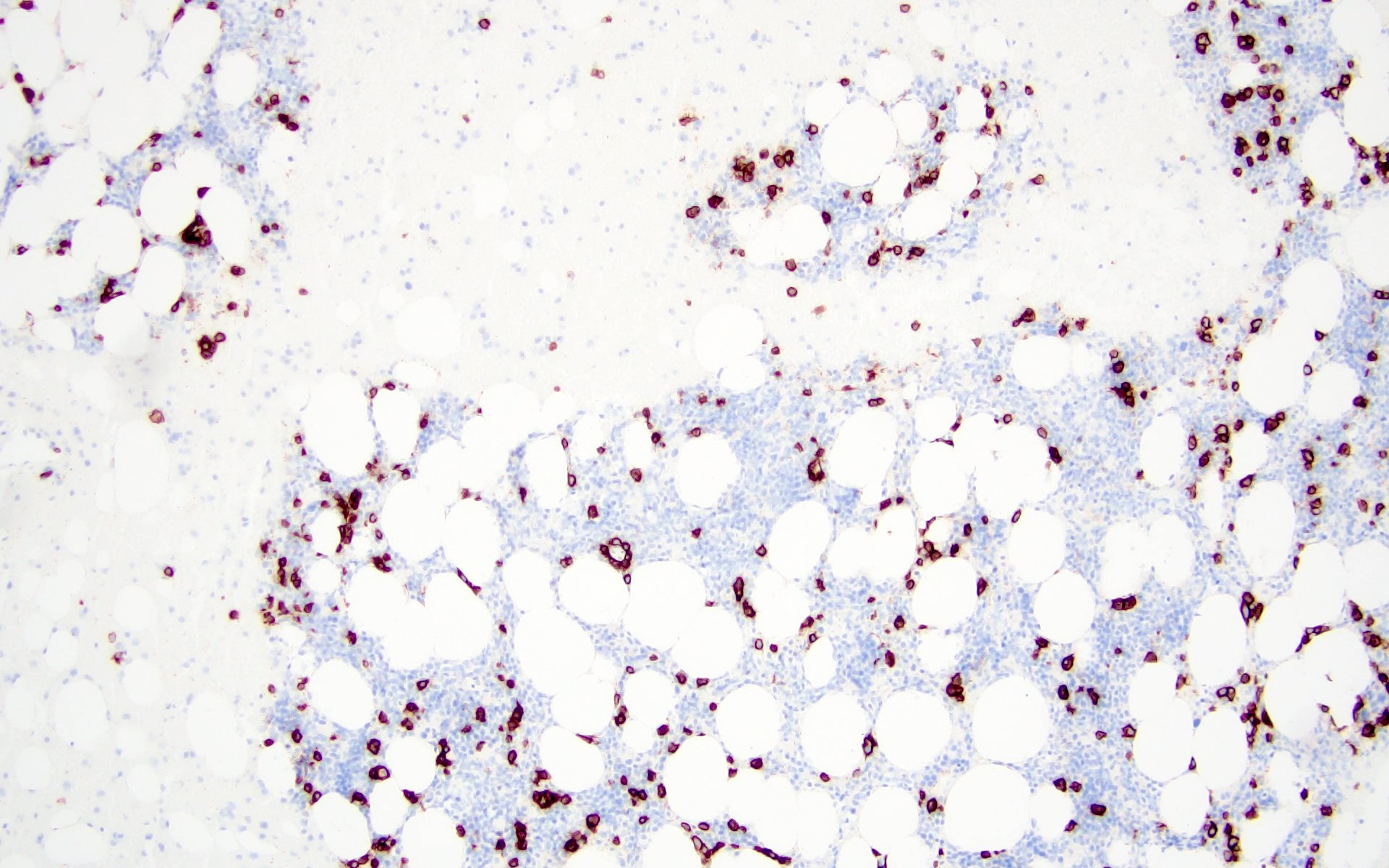
Plasma cells positive for CD138
Positive for kappa
Negative for lambda
Virtual slides
Contributed by Genevieve M. Crane, M.D., Ph.D.

EBV+ tumor
Cytology description
- Increased plasma cells with variable morphology, including small unremarkable plasma cells to atypical plasma cells (prominent nucleoli, plasmablastic / anaplastic morphology)
Cytology images
Contributed by Genevieve M. Crane, M.D., Ph.D.
Touch preparation
Positive stains
- CD38, CD138, MUM1, CD229, CD48, CD272, CD319 (Cytometry B Clin Cytom 2016;90:91, Cytometry B Clin Cytom 2019;96:338, Cytometry B Clin Cytom 2016;90:81)
- Some cases with expression CD117, CD20, CD33, CD10 (Haematologica 2006;91:1234, Cytometry B Clin Cytom 2010;78:239, Blood Cancer J 2018;8:e621)
- IgG, IgA (Cancer 1999;85:2305)
- Either kappa or lambda cytoplasmic immunoglobulin light chain expression
- Low Ki67 proliferative index
Negative stains
- CD19, CD45
- Cyclin D1 (J Pathol 2005;205:92)
- CD56
- EBV (mostly negative)
- Rare cases of EBV+ EMP in immunocompetent patients (EPIC) have been reported, which have brisk CD8+ and TIA1+ cytotoxic T cell infiltrate (Histopathology 2015;67:225)
Flow cytometry description
- Positive for CD138, CD38, restricted cytoplasmic light chain and negative for CD19
Molecular / cytogenetics description
- Positive for clonal immunoglobulin heavy chain gene rearrangement
- Negative for TP53 mutation (J Pathol 2005;205:92)
- Negative for MYC gene rearrangement
- Cytogenetic abnormalities (Blood 2016;127:2955, Am J Hematol 2016;91:719, Nat Rev Clin Oncol 2018;15:409, Br J Haematol 2000;111:1116, Leukemia 2001;15:981, Haematologica 2017;102:e364, Leukemia 2019;33:159, Blood 2006;108:1724, Leukemia 2006;20:2034, Blood Cancer J 2019;9:94)
- Hyperdiploidy: trisomies of odd numbered chromosomes (3, 5, 7, 9, 11, 15, 19 and 21)
- CCND translocations
- t(12;14) / CCND2::IGH
- t(6;14) / CCND3::IGH
- t(11;14) / CCND1::IGH (least commonly seen)
- MAF translocations
- t(14;16) / IGH::MAF
- t(8;14) / MAFA::IGH
- t(14;20) / IGH::MAFB
- NSD2 translocation
- t(4;14) / IGH::NSD2
- Alterations of chromosome 1 (+1q, -1p) and -17p
- Deletion of chromosome 13q (or monosomy 13)
Sample pathology report
- Nasal cavity, biopsy:
- Plasma cell neoplasm (see comment)
- Flow cytometric analysis revealed a cytoplasmic lambda light chain restricted monotypic plasma cell population (~23% of total CD45+ leukocytes) that is CD138+, CD38+, CD19-, CD20-, CD81-, partial CD27+, CD56- and CD117-. A polytypic B cell population is identified.
- Comment: The biopsy shows sheets of small plasma cells which are lambda restricted based on kappa / lambda in situ hybridization studies. EBER ISH is negative. Ki67 shows low proliferative index (< 5%). Clinical correlation with serology, imaging and bone marrow biopsy is suggested.
Differential diagnosis
| Extramedullary plasmacytoma (EMP) | Multiple myeloma (MM) with extramedullary disease | Lymphoplasmacytic lymphoma (LPL) | Extranodal marginal zone lymphoma (EMZL) | Plasmablastic lymphoma | |
| Presentation | Localized | Advanced stage of MM or at relapse | IgM paraprotein with macroglobulinemia | Localized | Aggressive disease, usually in immunocompromised patients (HIV) |
| Location | Upper respiratory tract | Localized / systemic disease | Systemic disease | Stomach, ocular adnexa, salivary gland, skin, lung, breast, thyroid | Nasal / oral cavity, gastrointestinal tract, lymph nodes |
| Precursor lesion | None | History of MM | IgM MGUS | Sites of chronic infection / inflammation (Sjögren syndrome and Hashimoto thyroiditis) | None |
| Morphology | Mostly mature appearing plasma cells | Variable normal to anaplastic / plasmablastic morphology | Small lymphocytes, plasmacytoid cells and plasma cells | Small lymphocytes, monocytoid cells and plasma cells | Large cells with round eccentric nucleus and prominent nucleoli |
| Phenotype | Cytoplasmic light chain restriction; CD38+, CD138+, MUM1+, CD19-, CD56 variable, CD20-, PAX5-, cyclin D1-, MYC-, no p53 overexpression | Cytoplasmic light chain restriction; CD38+, CD138+, MUM1+, CD19-, CD56 variable, CD20-, PAX5-, cyclin D1-/+, MYC and p53 overexpression | Surface light chain restriction; CD20+, PAX5+, CD43-/+, CD10-, CD5-/+, CD56-, CD117-, cyclin D1- | Surface light chain restriction; CD20+, PAX5+, CD43-/+, CD10-, CD5-/+, CD56-, CD117-, cyclin D1- | CD38+, CD138+, MUM1+, CD79a-/+, CD20-, PAX5-, CD45-, LANA-, ALK-, MYC and PDL1 overexpression |
| EBV | EBV variable (15% positive) | Negative | Negative | Negative | Positive (60 - 80%) |
| Bone marrow involvement | No / minimal (< 10%) | No / present | Present | Rare | No / present |
| Cytogenetics | IGH translocations with exception of t(11;14), hyperdiploidy | High risk cytogenetics and secondary alterations including del(17p), 1q gains, MYC rearrangement | Lacks MM hyperdiploidy and translocations | Lacks MM hyperdiploidy, trisomy of chromosomes 3 and 18, t(11;18)(q21;q21) / BIRC3::MALT1, t(1;14)(p22;q32) / IGH::BCL10, t(14;18)(q32;q21) / IGH::MALT1, t(3;14)(p14;q32) / IGH::FOXP1 | Lacks MM hyperdiploidy and translocations, MYC rearrangement |
| Molecular | Negative for MYC rearrangement and TP53 mutation | TP53 mutation | MYD88 L265P (> 90%), CXCR4 mutation (30 - 40%) | TNFAIP3 mutation, GPR34 mutation, TET2, CD274 and TNFRSF14 mutations | Mutations of JAK / STAT, MAPK / ERK and NOTCH pathways, TP53 mutation |
| Prognosis | Excellent | Poor | Good | Excellent | Poor |
Additional references
Board review style question #1
A 43 year old man presents with nasal obstruction and epistaxis. Imaging showed a 2.2 cm nasopharyngeal mass. Nasopharyngeal and bone marrow biopsies were performed (see images above). Which of the following risk factors in this patient increases the chances of progression to multiple myeloma?
- Age
- Bone marrow involvement
- Morphology
- Tumor size
Board review style answer #1
B. Bone marrow involvement is present in this case, which increases the risk of progression to multiple myeloma. Answers A, C and D are incorrect because the patient is young and the tumor size is < 5 cm with bland morphology (not plasmablastic / anaplastic), so none of the factors accounted for by these options increase risk of progression to multiple myeloma.
Comment Here
Reference: Plasmacytoma
Comment Here
Reference: Plasmacytoma
Board review style question #2
Which of the following genetic abnormalities is commonly associated with extramedullary plasmacytoma?
- MYC rearrangement
- t(11;14)
- t(12;14)
- TP53 mutation
Board review style answer #2
C. t(12;14). CCND translocations, which are seen in extramedullary plasmacytoma, include t(12;14) / CCND2::IGH and t(6;14) / CCND3::IGH. Answer B is incorrect because t(11;14) / CCND1::IGH is least commonly detected in extramedullary plasmacytoma. Answers A and D are incorrect because TP53 mutation is noted in multiple myeloma and both MYC rearrangement and TP53 mutation are identified in plasmablastic lymphoma.
Comment Here
Reference: Plasmacytoma
Comment Here
Reference: Plasmacytoma
