
Lymphoma & related disorders
Mature T/NK cell disorders
Pediatric NK/T cell disorders
Systemic EBV+ T cell lymphoma of childhood
Editorial Board Member: Mario L. Marques-Piubelli, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 22 March 2024
Last staff update: 22 March 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Systemic EBV+ T cell lymphoma of childhood
See also: Hydroa vacciniforme-like lymphoma (HVL)

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Stone M, Jeon YK, Murga-Zamalloa C. Systemic EBV+ T cell lymphoma of childhood. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomanonBchild.html. Accessed April 1st, 2025.
Definition / general
- Often rapid and fulminant disease within the spectrum of childhood Epstein-Barr virus (EBV) positive T cell lymphomas
Essential features
- Clinically characterized by systemic involvement, including the bone marrow, lymph nodes, spleen and lungs; most patients have a rapid, often fatal, clinical course
- Neoplastic elements are EBV+ T cell lymphocytes identified in biopsies from end organ damage biopsy sites; EBV+ T cell lymphocytes predominantly have a cytotoxic immunophenotype
- Neoplastic elements are mostly small lymphocytes without cytological atypia or effacement of the background tissue architecture
- It occurs in pediatric and young adult immunocompetent patients and there is an overlap in symptoms, clinical outcomes, laboratory findings and histomorphological features with the other 2 EBV+ T / NK lymphoproliferative disorders of childhood: EBV+ hemophagocytic lymphohistiocytosis (EBV+ HLH) and T / NK systemic form chronic active EBV disease (T / NK sCAEBV)
- These 3 entities represent different ends of a spectrum of end organ damage secondary to EBV infected hyperactivated T cell lymphocytes
Terminology
- No longer recommended
- Fulminant T cell lymphoproliferative disease
- Sporadic fatal infectious mononucleosis
- Fatal infectious mononucleosis
- Fulminant EBV+ T cell lymphoproliferative disorder of childhood
- Lethal hemophagocytic lymphohistiocytosis
- Fulminant hemophagocytic syndrome in children
- Severe chronic active EBV disease (CAEBV)
ICD coding
Epidemiology
- More commonly affects people in Asia, Mexico, Central America and South America
- Affects immunocompetent patients
- Most commonly occurs in children and young adults; rare cases have been reported in older adults
- References: Pediatr Blood Cancer 2019;66:e27798, Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443, Leuk Lymphoma 2020;61:808
Sites
- Liver (40%), spleen (70%), bone marrow (40%), lung (50%), and lymph nodes (60%) (Pediatr Blood Cancer 2019;66:e27798, Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443)
Pathophysiology
- Disease develops from EBV infected T cell lymphocytes (Pediatr Blood Cancer 2019;66:e27798, Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443)
Etiology
- Epstein-Barr virus (EBV) is latent in memory type B cells of healthy carriers (Pediatr Blood Cancer 2019;66:e27798, Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443, Blood 2001;98:280)
- However, patients who develop aggressive T cell lymphomas associated with EBV infection feature T or NK cells with latent EBV infection
- Mechanisms involved in the proliferation and expansion of T / NK cell types infected with EBV are not understood
- However, it is proposed that a subset of EBV+ T / NK cells may evade immune surveillance
Clinical features
- Symptoms include hepatosplenomegaly, fever, lymphadenopathy, malaise and upper respiratory tract symptoms
- Often, there is rapid development of multiorgan failure, sepsis and death within a few days to a few months in immunocompetent patients
- Proposed as a diagnosis of exclusion in EBV positive T / NK lymphoproliferative disorders of childhood that do not fulfill the criteria for T / NK sCAEBV or EBV positive HLH
- References: Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443
Diagnosis
- Histologic, immunohistochemical, molecular and cytogenetic analysis of involved tissues and clinical correlation
Laboratory
- Hyperferritinemia, elevated liver enzymes, elevated lactate dehydrogenase (LDH), bicytopenias or pancytopenias
- Increased EBV DNA in the peripheral blood (> 1 x 102.5 copies/μg)
- References: Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443
Prognostic factors
- Overall poor prognosis with a high mortality rate (66 - 90%) (Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53)
Case reports
- 16 year old girl with fatal disease course (Indian J Pathol Microbiol 2020;63:78)
- 30 year old woman with systemic EBV positive T cell lymphoma of childhood developing following systemic CAEBV disease (Diagn Pathol 2023;18:111)
- 68 year old woman with disease involving bone marrow and soft tissue (Pathol Int 2022;72:376)
Treatment
- HLH 2004 protocol or other etoposide containing regimens followed by hematopoietic stem cell transplant (Leuk Lymphoma 2017;58:53, Diagn Pathol 2021;16:48, Pediatr Hematol Oncol 2018;35:121)
Microscopic (histologic) description
- More frequently, there is a mild expansion of small to medium sized T cell lymphocytes without cytological atypia or effacement of the background target tissue architecture
- When involved, the spleen shows depletion of the white pulp, lymphocyte infiltration of the red pulp and prominent hemophagocytosis
- When the liver is involved, findings include a sinusoidal and portal lymphocytic infiltrate; additional reported findings include cholestasis, steatosis and variable degrees of liver necrosis
- Bone marrow shows a scattered to diffuse, medium / large atypical lymphocytic infiltrate and increased histiocytes and hemophagocytosis
- Lymph nodes, when involved, usually show preserved architecture with open sinuses, expanded paracortical regions, sinus histiocytosis and hemophagocytosis (Pediatr Blood Cancer 2019;66:e27798, Blood 2000;96:443)
- Few cases with diffuse sheets of atypical medium to large lymphocytes involving the liver, bone marrow, spleen, lung or lymph node have been reported
- References: Diagn Pathol 2021;16:48, Leuk Lymphoma 2017;58:53, Blood 2000;96:443, Pediatr Blood Cancer 2019;66:e27798
Microscopic (histologic) images
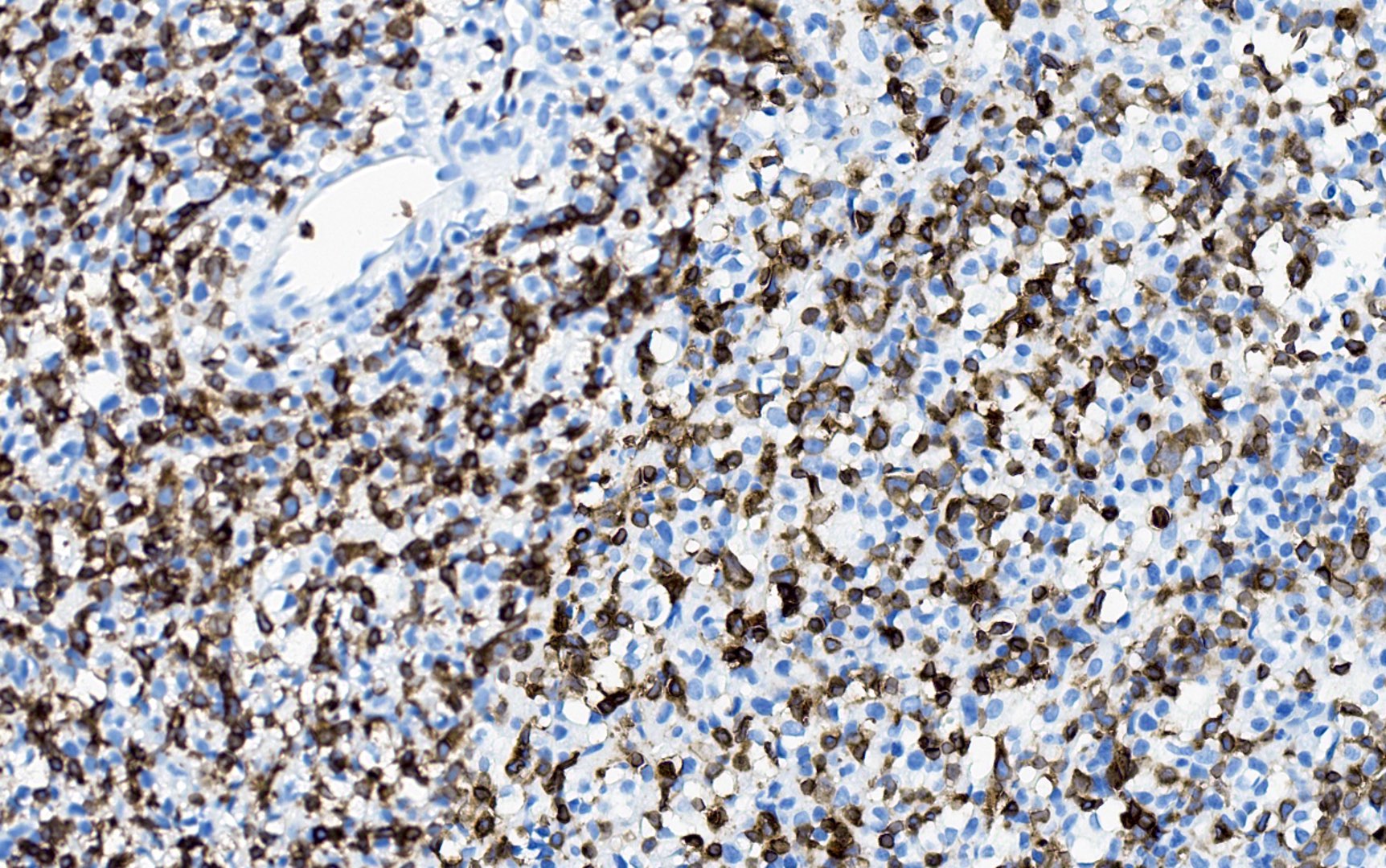
Contributed by Yoon Kyung Jeon, M.D.
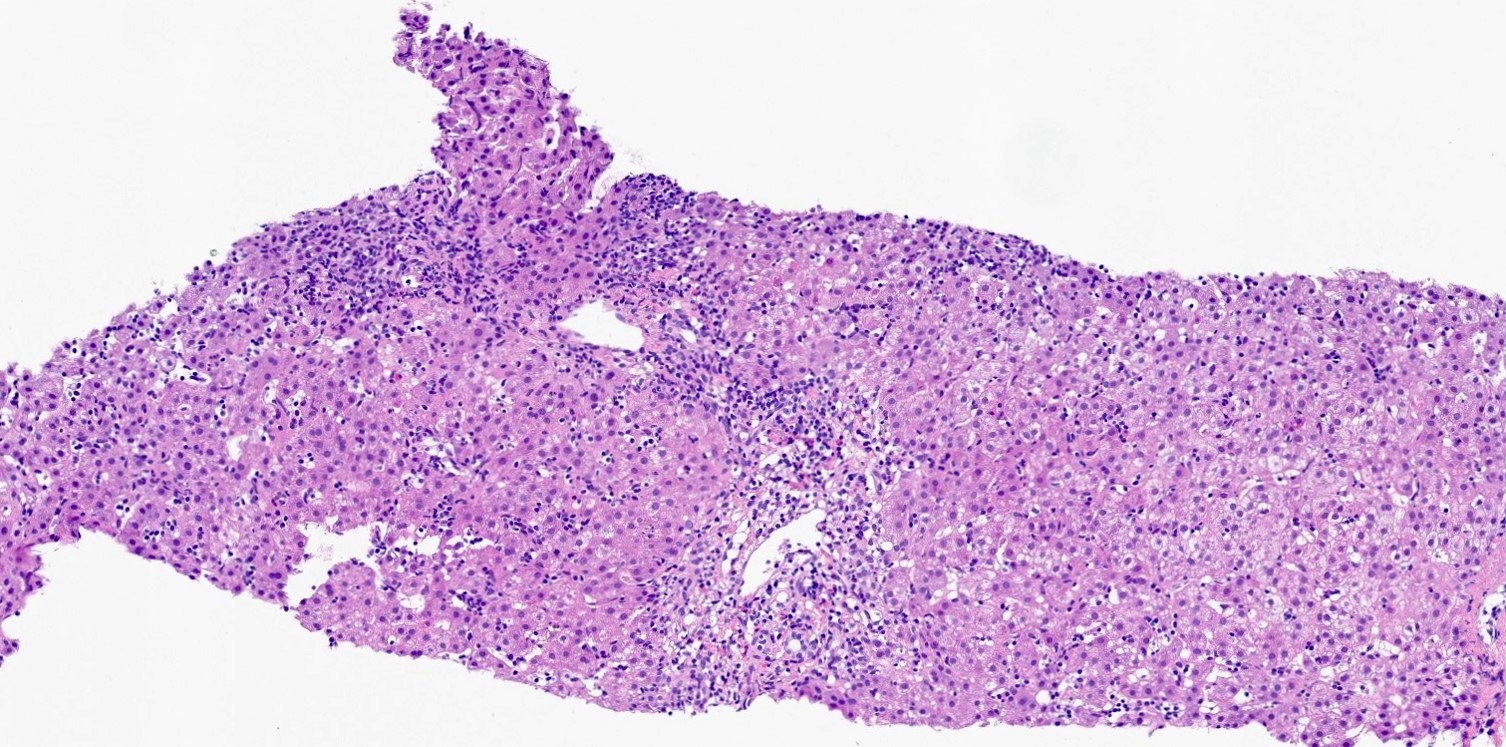
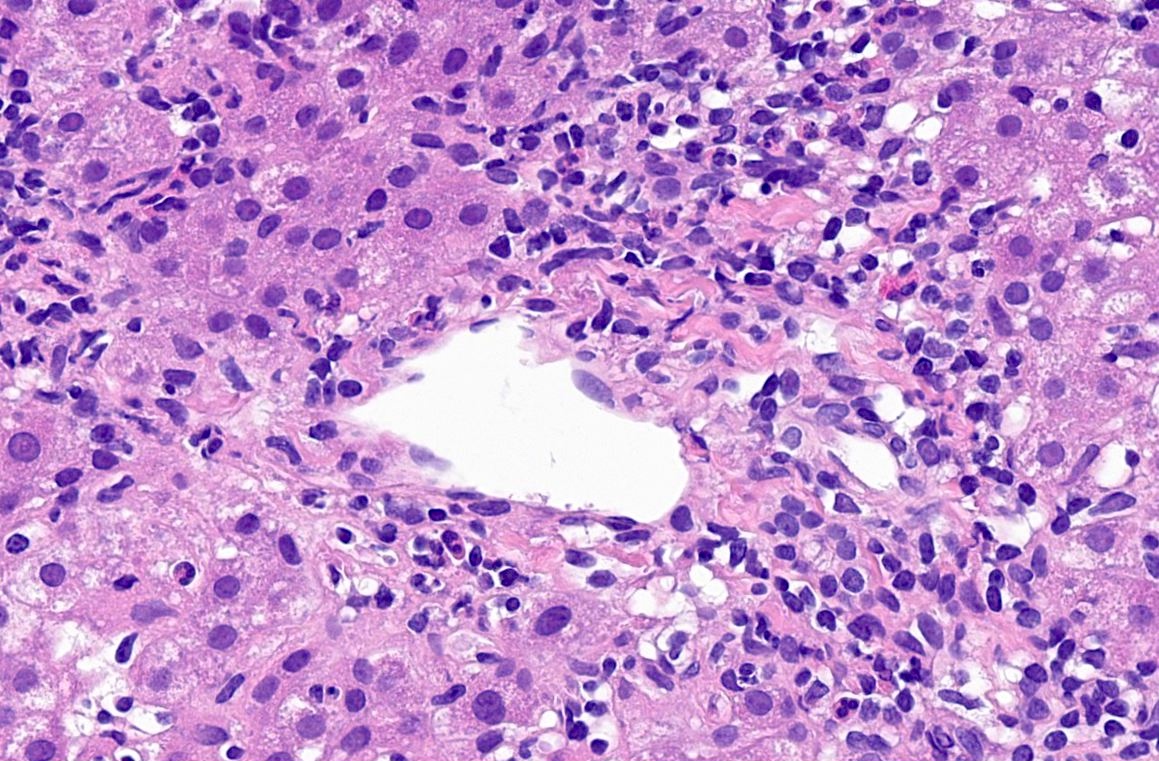
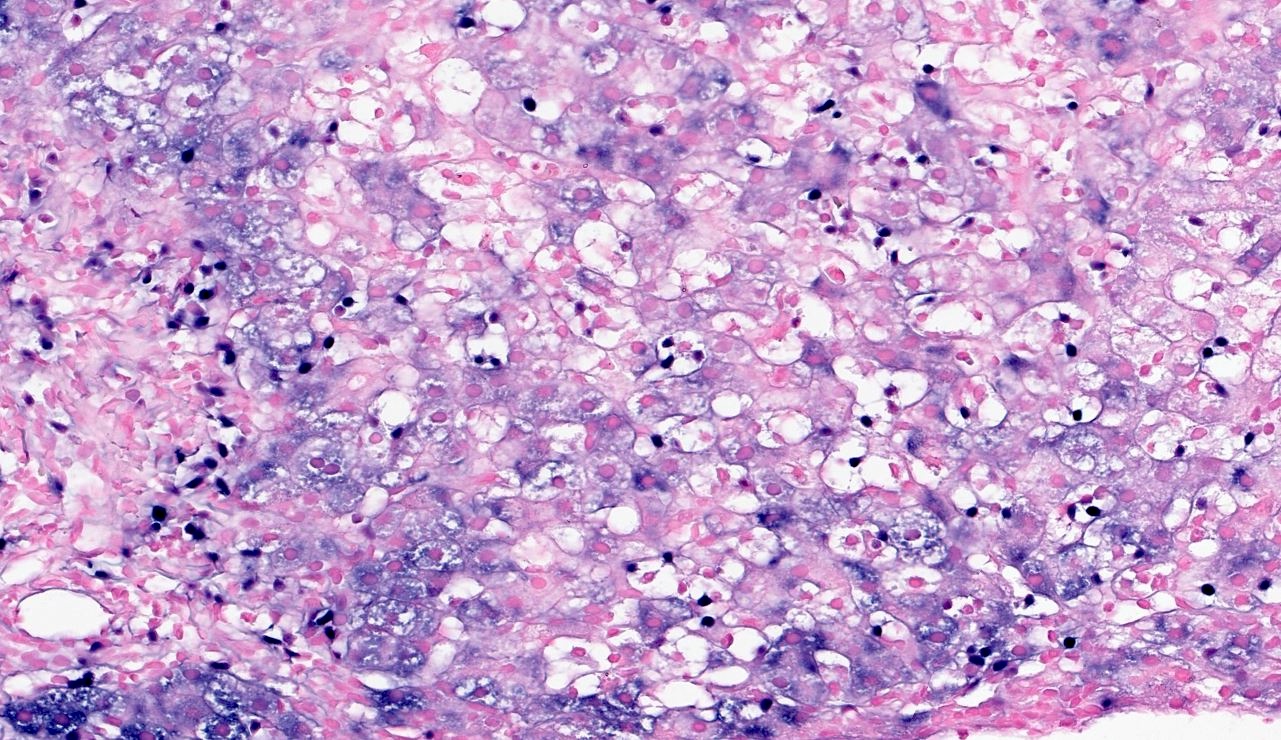
Lymphocytic infiltrates in the liver
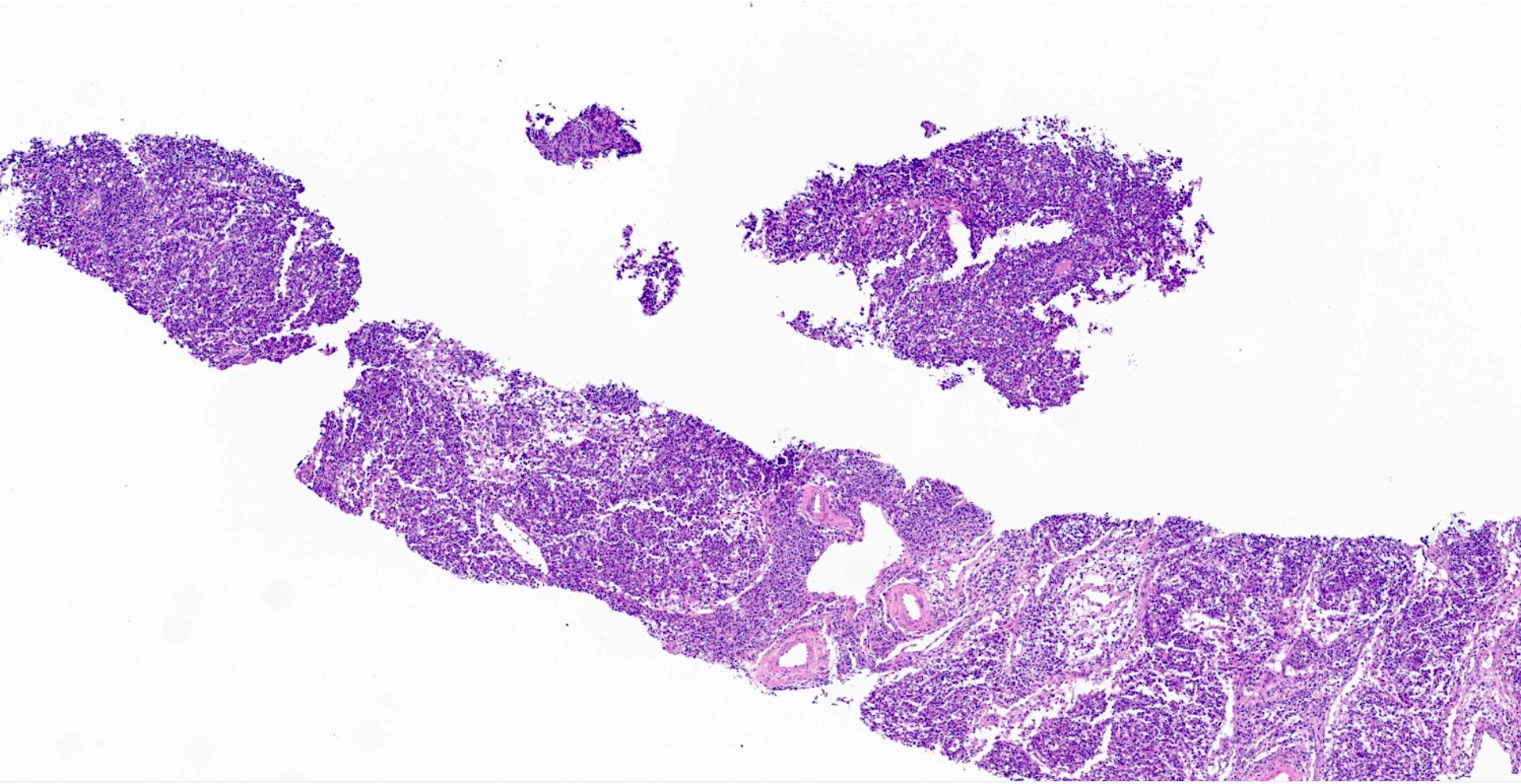
Lymph node, atypical infiltrates
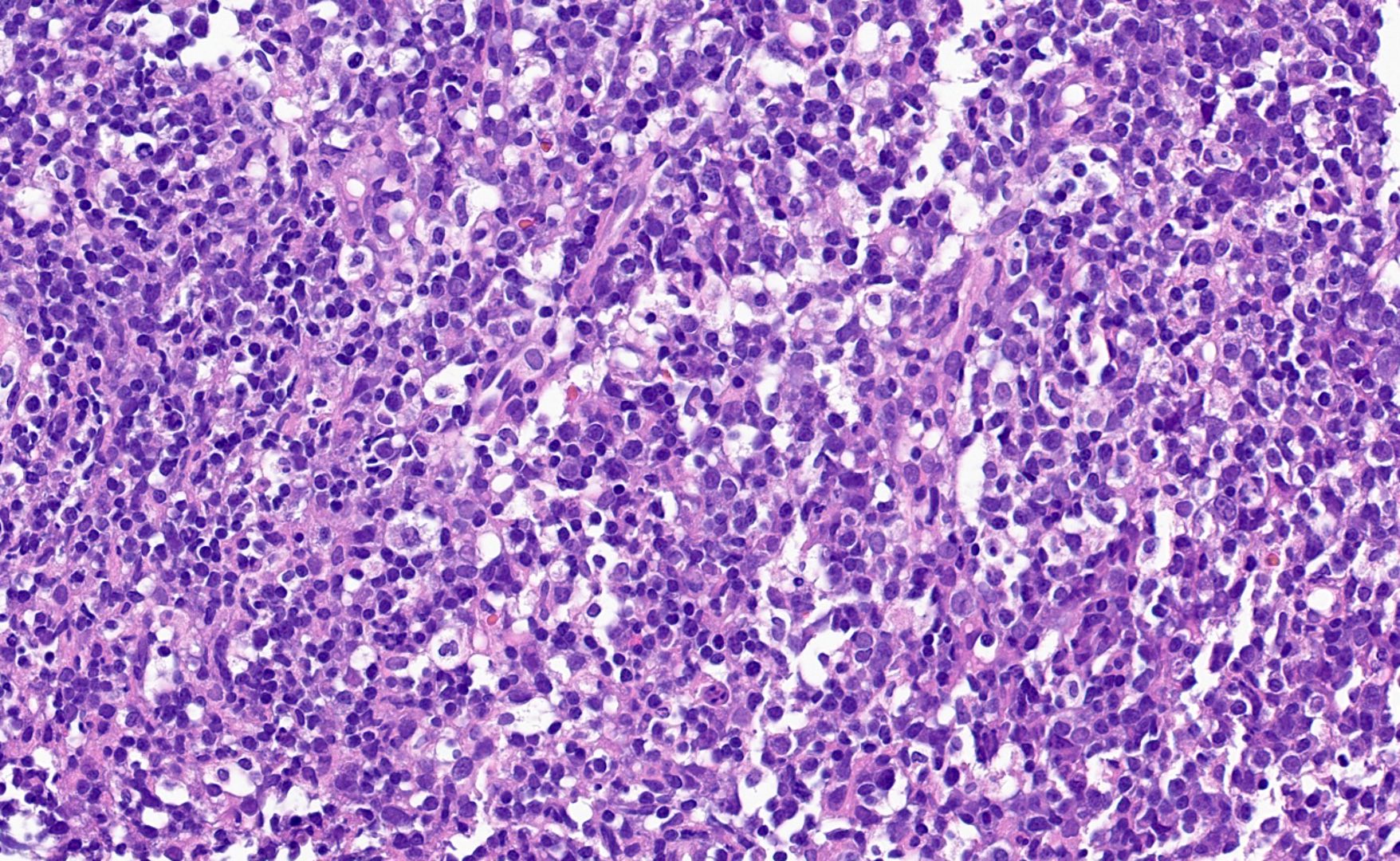
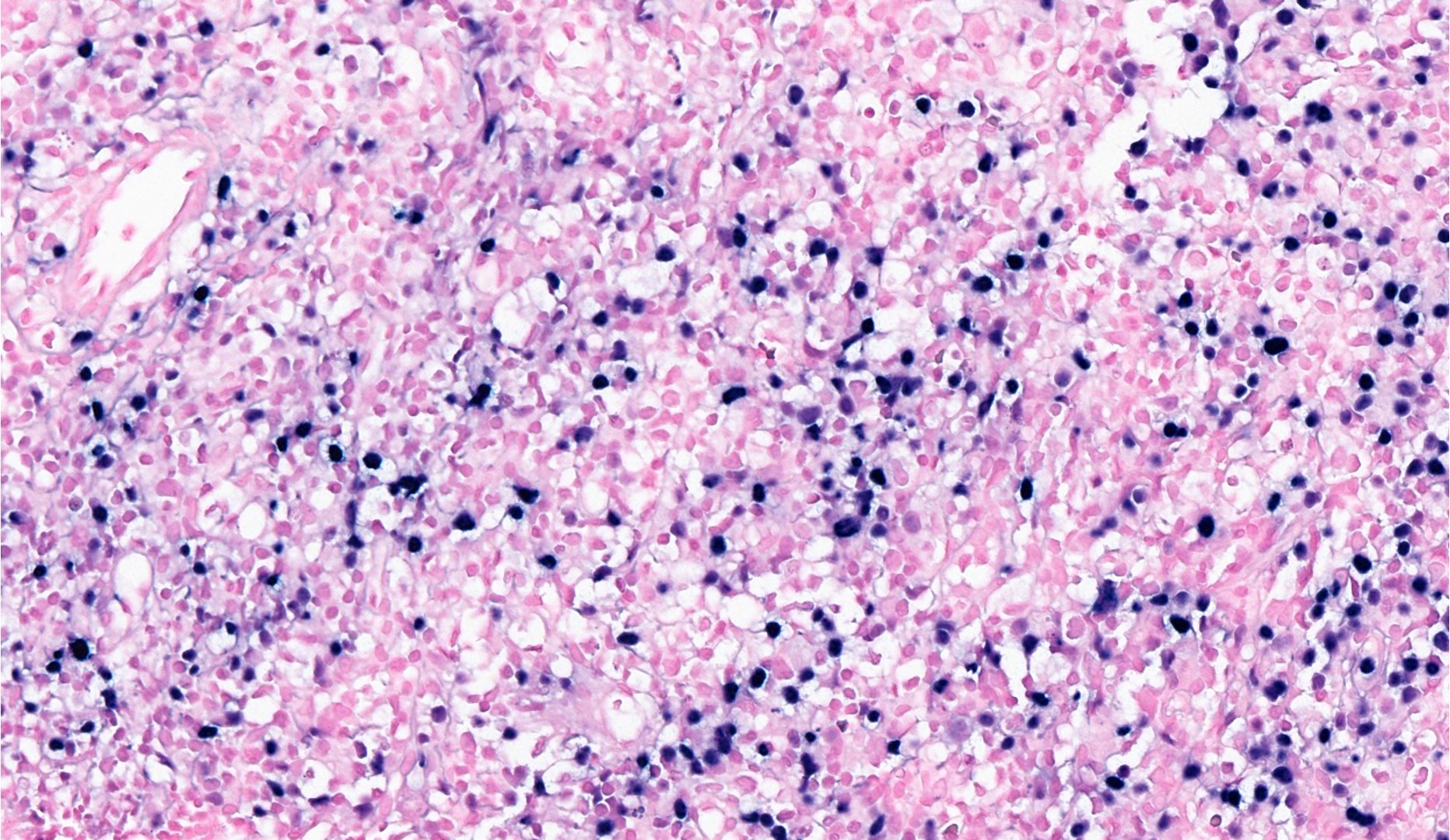
Lymph node, atypical infiltrates
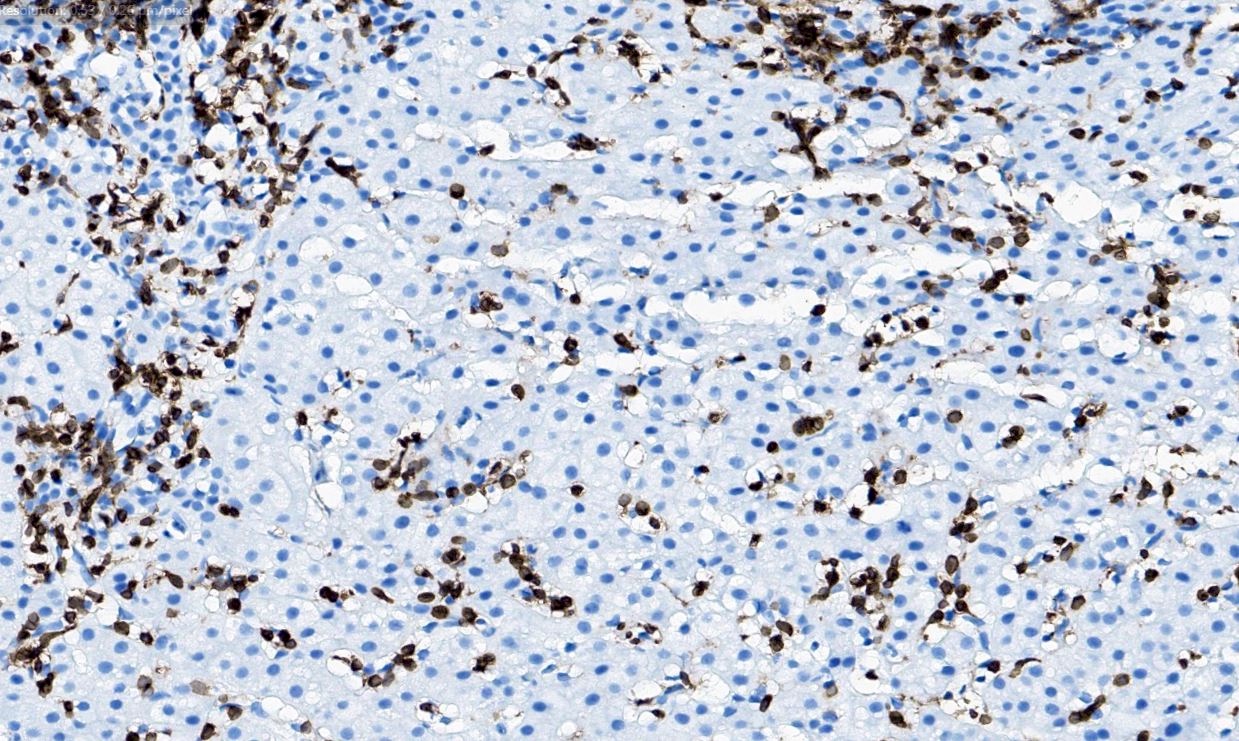
Lymphocytic infiltrates in the liver (CD3)
Positive stains
- CD3+ / CD8+
- CD3+, CD4+ (CD8 negative) in cases following systemic CAEBV disease
- EBER in situ hybridization (ISH)
- TIA1
- CXCR3 (60% of cases)
- CD2
- References: Leuk Lymphoma 2017;58:53, Blood 2000;96:443, Diagn Pathol 2021;16:48, Pediatr Blood Cancer 2019;66:e27798, Indian J Pathol Microbiol 2020;63:78, Diagn Pathol 2023;18:111
Negative stains
Molecular / cytogenetics description
- Monoclonal TCR gene rearrangements by PCR or EBV clonality testing (Int J Clin Exp Pathol 2014;7:5738, Blood 2000;96:443, Diagn Pathol 2021;16:48)
- Clonal cytogenetic abnormalities have been reported including inv(7) (Int J Clin Exp Pathol 2014;7:5738)
Molecular / cytogenetics images
Images hosted on other servers:

PCR for TCR gamma gene
Sample pathology report
- Bone marrow core biopsy, touch imprints, aspirate and clot:
- Hypercellular bone marrow with atypical EBV positive T cell lymphocytic infiltrates (see comment)
- Comment: The T cell lymphocytic infiltrates feature aberrant loss of CD5 and concurrent T cell receptor rearrangement studies are consistent with a monoclonal T cell population. In the proper clinical context, these findings can be consistent with systemic EBV positive T cell lymphoma of childhood.
Differential diagnosis
- Aggressive natural killer cell leukemia (ANKL) (Cancers (Basel) 2020;12:2900, Blood Cancer J 2017;7:660, Blood 2012;119:673):
- Primarily a leukemic disease by definition, with secondary hepatosplenomegaly and bone marrow involvement
- Positive expression of CD56, CD16, EBER and cytoplasmic CD3ε with lack of surface CD3 expression
- Lack of expression of surface T cell receptor and monoclonal TCR gene rearrangements
- Aggressive clinical course, overall survival is < 1 year after diagnosis
- Chronic active EBV disease of T / NK cell type, systemic form (T / NK sCAEBV) (Blood Adv 2020;4:2918, Blood 2012;119:673, Pathogens 2018;7:28, Semin Diagn Pathol 2020;37:32, Am J Clin Pathol 2024 Feb 12 [Epub ahead of print]):
- Persistent high EBV titers and infectious mononucleosis symptoms for > 3 months
- Positive EBV infection of T or NK cells in peripheral blood or involved tissues
- Most commonly, it involves the spleen, liver and bone marrow
- By definition, EBV infected T or NK cells lack cytological atypia and do not efface the background tissue architecture
- T cell type (59% of cases) (CD4 > CD8)
- NK cell type (CD56 positive of 41% of cases)
- It often shows monoclonality by TCR gene rearrangement or EBV clonality testing; fewer cases are oligoclonal or polyclonal
- Can develop following EBV negative HLH; it is proposed that cases of EBV+ HLH that do not respond to initial therapies with persistent high EBV counts may constitute T / NK sCAEBV
- EBV+ hemophagocytic lymphohistiocytosis (EBV+ HLH) (J Clin Invest 1993;92:1444, Int J Clin Exp Pathol 2014;7:5738, Br J Haematol 2022;196:31, Semin Diagn Pathol 2020;37:32, Pediatr Blood Cancer 2007;48:124):
- Diagnosis requires meeting the HLH 2004 diagnostic criteria, including 5 out of 9 clinical and laboratory findings
- Hemophagocytosis is detected in the bone marrow, liver or lymph nodes
- Small numbers of EBV+ T cell lymphocytes are identified
- T cells do not show cytologic atypia or effacement of the background architecture
- Lack of clonal cytogenetic abnormality
- EBV+ T cells are CD8+ / CD4-
- Lack of monoclonal TCR gene rearrangement
- EBV+ nodal T and NK cell lymphoma (Hum Pathol 2015;46:981, Am J Surg Pathol 2015;39:462, Int J Hematol 2016;104:591, Histopathology 2012;61:186, J Clin Exp Hematop 2020;60:30, Pathol Res Pract 2013;209:448, Haematologica 2018;103:278):
- Primarily, it is a nodal disease with limited extranodal disease, including the bone marrow, spleen or liver
- Diffuse effacement of the lymph node architecture by lymphocytes with marked cytological atypia; the atypical lymphocytes are most commonly medium to large with pleomorphism
- Most cases show a CD3+ / CD8+ phenotype (~90%)
- Positive for EBER (in at least 30% of the tumor cells) and cytotoxic markers (TIA1, granzyme B)
- Monoclonal TCR gene rearrangement (75 - 85%)
Table 1: Comparison of the clinical and laboratory findings between the entities included in the differential diagnosis of systemic EBV+ T cell lymphoma of childhood (adapted from Am J Clin Pathol 2024 Feb 12 [Epub ahead of print])
| Epstein-Barr virus associated hemolymphohistiocytosis (EBV HLH) | Chronic active EBV disease of T / NK cell type systemic form (T / NK sCAEBV) | Systemic EBV positive T cell lymphoproliferative disorder of childhood | Nodal EBV positive T / NK cell lymphoma | Aggressive NK cell leukemia | |
| Morphological features | Small T cell lymphocytes with no definitive cytological atypia | The infiltrates are predominantly composed by lymphocytes and plasma cells with no effacement or distortion of the background tissue and without morphological atypia; HRS-like cells may be present | Variable expansion of lymphocytic infiltrates composed by small to medium sized T cells with no morphological atypia | Effacement of the nodal architecture by medium to large lymphocytes with marked cytological atypia | Medium sized atypical lymphocytes, frequently with prominent nucleoli |
| Immunophenotype | A subset of T cells are EBV and CD8 positive; loss of pan T cell markers may be observed | The HRS-like cells are CD30 positive with variable expression of PAX5 and CD20; the EBV positive T cells are predominantly CD4 positive with loss of pan T cell markers (rare EBV+ CD8 T cells have been reported) | Majority of cases are composed by CD8 positive neoplastic T cells (CD4+ cases are rare) | A minimum of 30% EBV positive T cell lymphocytes is required; majority of the cases are composed by CD8 positive neoplastic cells | Cytoplasmic CD3 expression and positive expression of CD2, CD56 and CD16; negative for CD57 |
| Anatomical sites of presentation | Bone marrow and liver | Liver, bone marrow and spleen | Bone marrow, liver, lymph nodes, spleen | Lymph nodes | Peripheral blood and bone marrow |
| Age at diagnosis | Predominantly pediatric population | Predominantly pediatric population | Predominantly pediatric population | Adult populations | Peak incidence between 21 and 30 year old |
| Relevant clinical features | Meets diagnostic criteria for HLH; good responses to etoposide based regimens | Persistent mononucleosis-like symptoms and high EBV titers for at least 3 months; good responses to systemic chemotherapy and hematopoietic stem cell transplantation is curative in most of pediatric patients; dismal clinical course in adult populations | Rapid development of multiorgan failure and end organ damage including liver failure, hepatosplenomegaly and pancytopenia, with high mortality rates | Aggressive clinical course and poor responses to current chemotherapeutic agents | Fulminant clinical course with a median overall survival of < 2 months |
| Relevant clinical features and prognosis | Meets diagnostic criteria for HLH; overall good prognosis with good responses to etoposide based regimens | Persistent mononucleosis-like symptoms and high EBV titers for at least 3 months; pediatric patients display good responses to systemic chemotherapy and hematopoietic stem cell transplantation is curative in most of pediatric patients; adult patients are characterized by dismal clinical course and poor prognosis | Rapid development of multiorgan failure and end organ damage including liver failure, hepatosplenomegaly and pancytopenia, with high mortality rates and poor prognosis | Aggressive clinical course, poor responses to current chemotherapeutic agents and bad prognosis | Fulminant clinical course, median overall survival of < 2 months and dismal prognosis |
Board review style question #1
Which of the following features supports a diagnosis of systemic EBV+ T cell lymphoma of childhood over EBV+ hemophagocytic lymphohistiocytosis (EBV+ HLH)?
- EBER positivity in CD8+ T cells
- Lack of cytologic atypia
- Onset of disease in childhood
- Presence of a clonal cytogenetic abnormality
Board review style answer #1
D. Presence of a clonal cytogenetic abnormality. Clonal cytogenetic abnormalities are found in systemic EBV+ T cell lymphoma of childhood but not EBV+ HLH. Answer A is incorrect because both systemic EBV+ T cell lymphoma of childhood and EBV+ HLH show EBER positivity in CD8+ T cells in most cases. Answer B is incorrect because systemic EBV+ T cell lymphoma of childhood and EBV+ HLH show no cytologic atypia; however, the presence of cytologic atypia would favor a diagnosis of systemic EBV+ T cell lymphoma of childhood. Answer C is incorrect because systemic EBV+ T cell lymphoma of childhood and EBV+ HLH most commonly occur in children and young adults (Int J Clin Exp Pathol 2014;7:5738).
Comment Here
Reference: Systemic EBV+ T cell lymphoma of childhood
Comment Here
Reference: Systemic EBV+ T cell lymphoma of childhood
Board review style question #2
Which of the following is correct regarding EBV+ T cell lymphoproliferative neoplasms of childhood?
- An indolent clinical course characterizes EBV+ T cell lymphoproliferative neoplasms
- Diagnosis can be established only after documentation of T cell receptor clonality studies
- Distinction between systemic EBV+ T cell lymphoma and chronic active EBV disease of T / NK cell type, systemic form (T / NK sCAEBV) can be established solely on morphological analysis of the lymphocytic infiltrates
- These groups of diseases constitute a continuum with similar histological features and overlap in clinical and laboratory findings
Board review style answer #2
D. These groups of diseases constitute a continuum with similar histological features and overlap in clinical and laboratory findings. Systemic EBV+ T cell lymphoma, T / NK sCAEBV and HLH EBV overlap in clinical features, are indistinguishable in histological features and can precede one another. Answer A is incorrect because these entities usually have an aggressive clinical course. Answer B is incorrect because T cell receptor clonality studies are not positive in all cases and its presence is not required to establish the diagnosis. Answer C is incorrect because the histological features between systemic EBV+ T cell lymphoma and T / NK sCAEBV are similar (Leuk Lymphoma 2017;58:53, Am J Clin Pathol 2024 Feb 12 [Epub ahead of print]).
Comment Here
Reference: Systemic EBV+ T cell lymphoma of childhood
Comment Here
Reference: Systemic EBV+ T cell lymphoma of childhood
