
Lymphoma & related disorders
Mature B cell neoplasms
Mantle cell lymphoma
In situ mantle cell neoplasm
Authors: Cameron Neely, M.D., Kyle Bradley, M.D., M.S.
Editorial Board Member: Julie Feldstein, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.

Last author update: 4 January 2024
Last staff update: 4 January 2024
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: In situ mantle cell neoplasm

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Flow cytometry description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Neely C, Bradley K. In situ mantle cell neoplasm. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaisMCN.html. Accessed April 1st, 2025.
Definition / general
- Cyclin D1 positive B cells with CCND1 rearrangements restricted to the mantle zones of reactive appearing lymphoid tissue (Blood 2016;127:2375)
Essential features
- Lymphoid architecture preserved with slight or no mantle zone expansion (Blood 2016;127:2375, Semin Diagn Pathol 2018;35:76)
- Cyclin D1 positive B cells with CCND1 rearrangement restricted to mantle zones (Blood 2016;127:2375, Mod Pathol 2012;25:1629)
- Rare; usually an incidental finding (Blood 2016;127:2375)
- Typically a stable disease with indolent behavior and long term survival, even without therapy (Blood 2016;127:2375)
- Infrequent (< 10%) progression to overt mantle cell lymphoma (Blood 2016;127:2375, Haematologica 2012;97:270)
Terminology
- In situ mantle cell neoplasia is accepted terminology
- Previous terms are not recommended: in situ mantle cell lymphoma, in situ involvement by mantle cell lymphoma-like cells or mantle cell lymphoma-like B cells of uncertain / undetermined significance (Semin Diagn Pathol 2018;35:76)
ICD coding
- ICD-10: C83.1 - mantle cell lymphoma (Western Australian Coding Rule: 1215/02 Mantle Cell Lymphoma In Situ [Accessed 1 May 2023])
Epidemiology
- Median age: 65 - 66 years (Haematologica 2012;97:270, Int J Clin Exp Pathol 2014;7:1042)
- Rare; usually an incidental finding (Blood 2016;127:2375)
- 2 cases of isolated and incidental in situ mantle cell neoplasia were identified in lymph nodes resected from 341 patients (0.6%) with colorectal or breast adenocarcinoma (Am J Surg Pathol 2016;40:943)
- 0 cases of in situ mantle cell neoplasia were identified in 1,292 reactive lymph nodes from 131 patients without evidence of lymphoma (Mod Pathol 2012;25:1629)
Sites
- Frequently nodal but may be seen in extranodal locations, including appendix, gallbladder, lacrimal gland, lung, nasopharynx, small intestine, oropharynx, spleen and urinary bladder (Haematologica 2012;97:270, Head Neck 2013;35:E333, J Hematop 2012;5:169)
- Involvement of more than 1 tissue site does not exclude the diagnosis (Blood 2016;127:2375)
- Peripheral blood involvement is permitted
- 5 of 17 patients showed peripheral blood or bone marrow involvement (Haematologica 2012;97:270)
Pathophysiology
- t(11;14) IGH::CCND1 translocation results in overexpression of cyclin D1 and dysregulation of the cell cycle (J Clin Invest 2012;122:3416)
- Low levels of B cells with t(11;14) translocation have been identified in peripheral blood of healthy individuals (Mod Pathol 2012;25:1629)
- Cyclin D1 positive B cells with CCND1 rearrangements may colonize the mantle zones of lymphoid follicles (Blood 2016;127:2375)
- Risk of progression is very low (Blood 2016;127:2375)
Etiology
- Unclear
Clinical features
- Indolent behavior (Blood 2011;117:3954, Haematologica 2012;97:270)
- Infrequent (< 10%) progression to overt mantle cell lymphoma (Blood 2016;127:2375, Semin Diagn Pathol 2018;35:76)
- May be identified in association with another lymphoma, including chronic lymphocytic leukemia / small lymphocytic lymphoma, marginal zone lymphoma and follicular lymphoma (Haematologica 2012;97:270)
Diagnosis
- Usually an incidental finding discovered when cyclin D1 immunohistochemistry is performed on a lymph node
Radiology description
- No specific radiologic findings
Case reports
- Man in his 40s with involved cervical lymph node and follicular lymphoma and man in his 70s with involved cervical lymph node (Histopathology 2008;52:256)
- 52 year old man and 65 year old woman with in situ mantle cell lymphoma in cervical lymph nodes (Int J Clin Exp Pathol 2014;7:1042)
- 58 year old man with involved inguinal node and marginal zone lymphoma (Am J Clin Pathol 2015;143:274)
- 65 year old man with involved mesenteric node and follicular lymphoma (Case Rep Hematol 2014;2014:145129)
- 70 year old woman with involved nasopharynx (Head Neck 2013;35:E333)
- 75 year old woman with composite follicular lymphoma and in situ mantle cell neoplasm (Pathol Res Pract 2020;216:153067)
Treatment
- Treatment guided by the presence or absence of coexistent overt lymphoma (Blood 2011;117:3954)
- In the absence of coexistent overt lymphoma, watchful waiting is appropriate (Semin Diagn Pathol 2018;35:76)
Microscopic (histologic) description
- Lymphoid architecture preserved with no or slight mantle zone expansion (Blood 2016;127:2375, Semin Diagn Pathol 2018;35:76)
- Cyclin D1 positive B cells identified within the mantle zone (Blood 2016;127:2375, Virchows Arch 2016;468:245, Haematologica 2012;97:270)
- Usually restricted to the inner mantle zone
- Rarely scattered throughout the mantle zone or present in the outer mantle zone
- Very rarely intrafollicular or focally within germinal centers
- May involve multiple follicles in a lymph node (Am J Surg Pathol 2016;40:943)
- May be identified in association with another lymphoma (Blood 2016;127:2375)
Microscopic (histologic) images
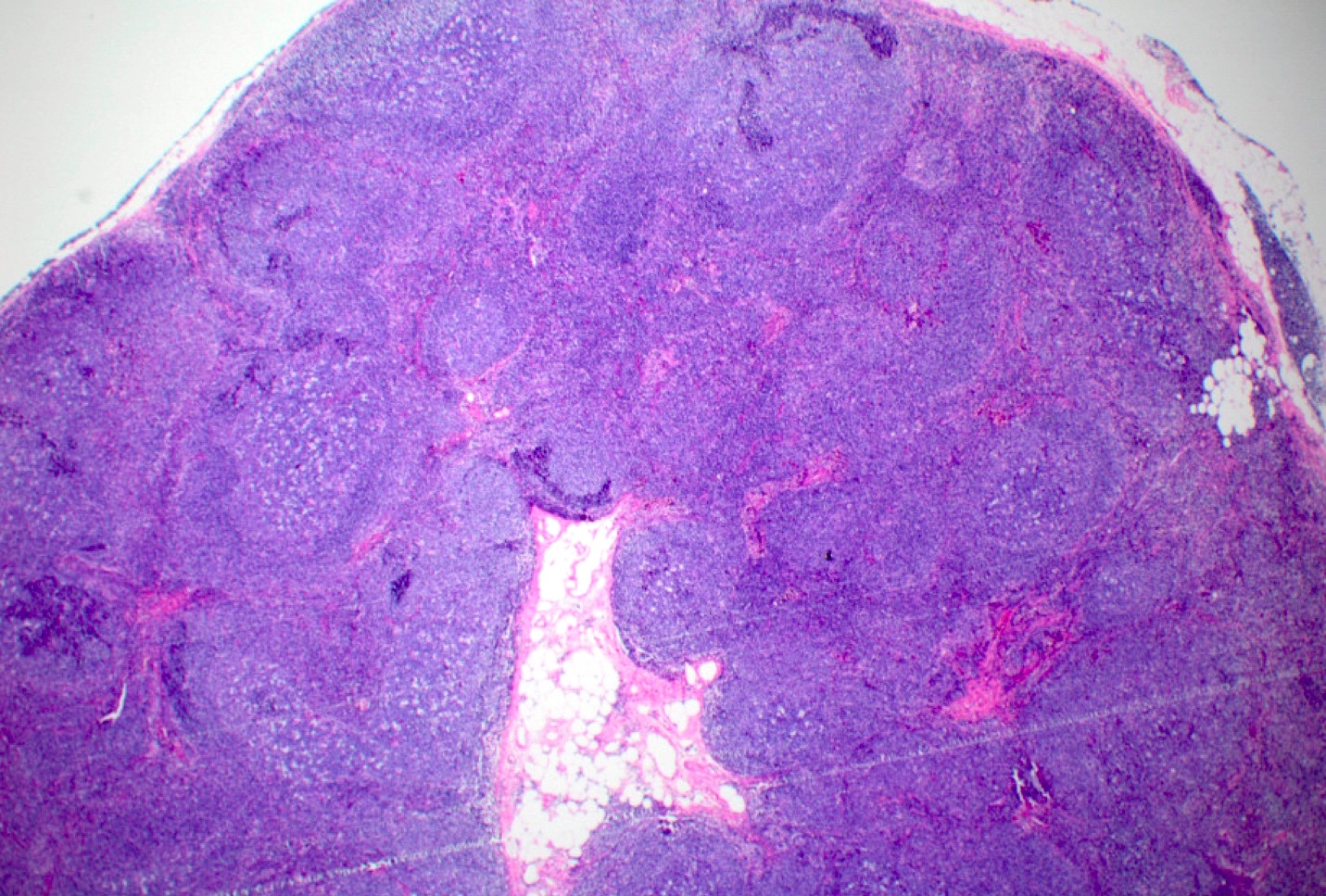
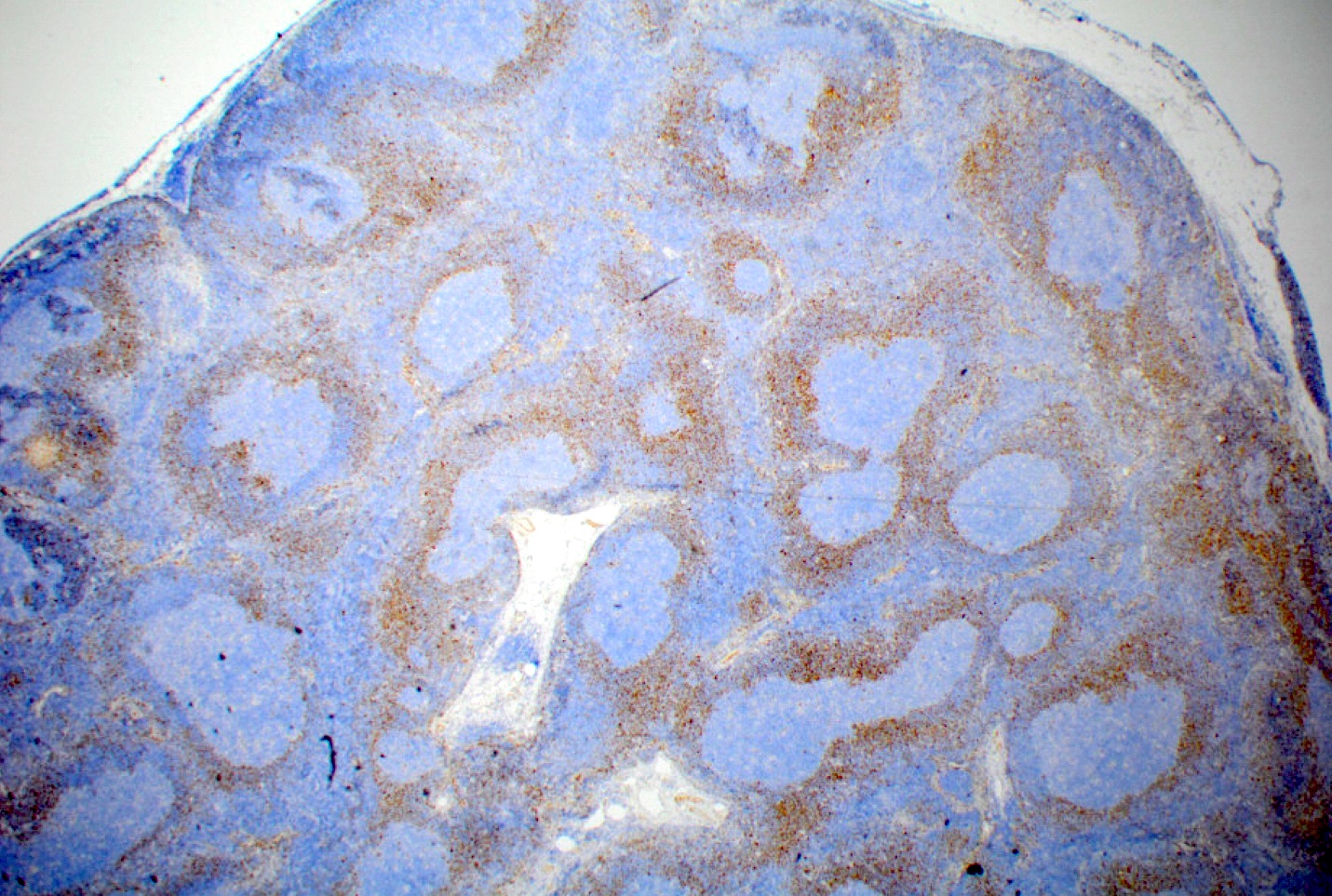
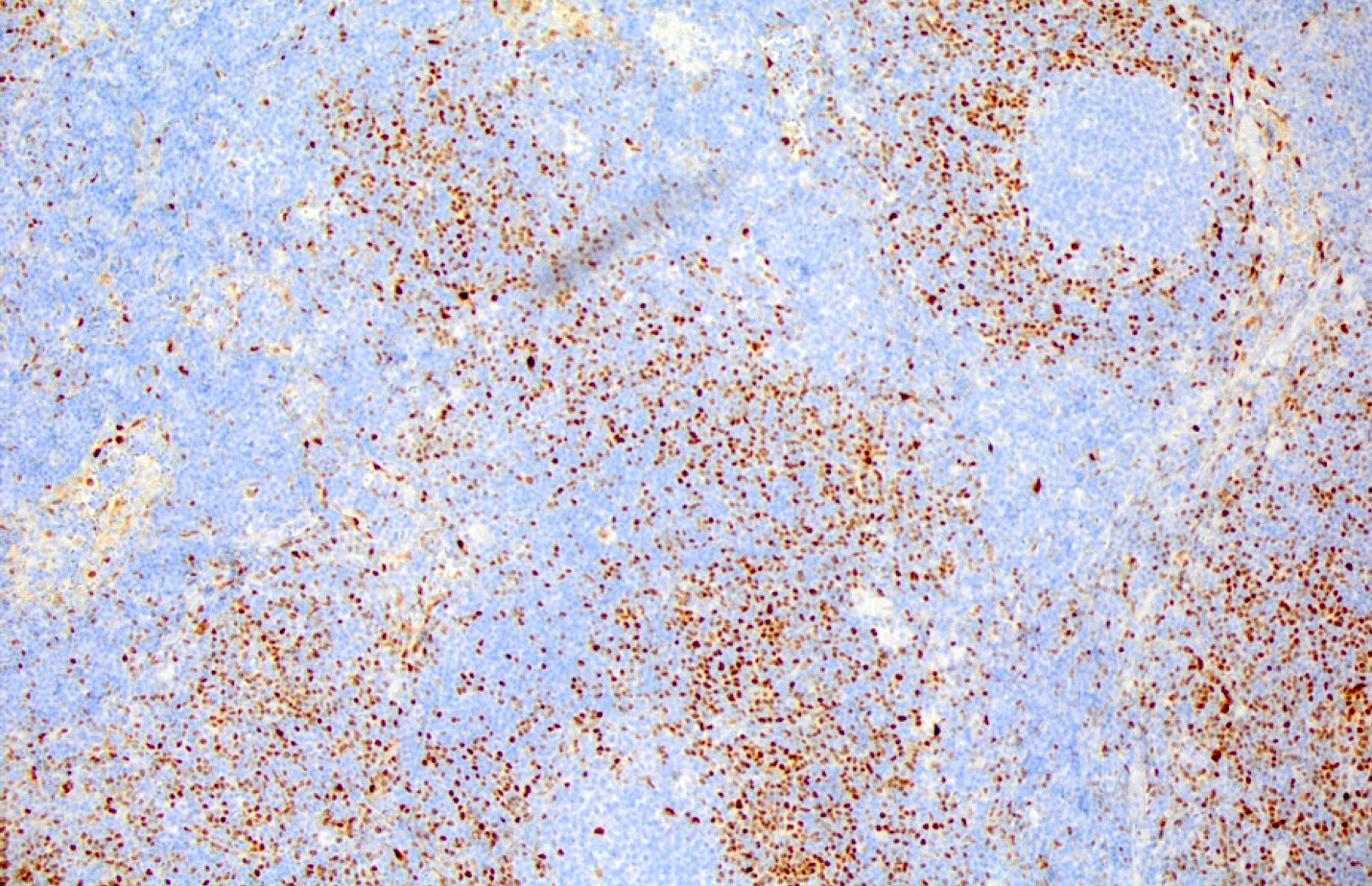
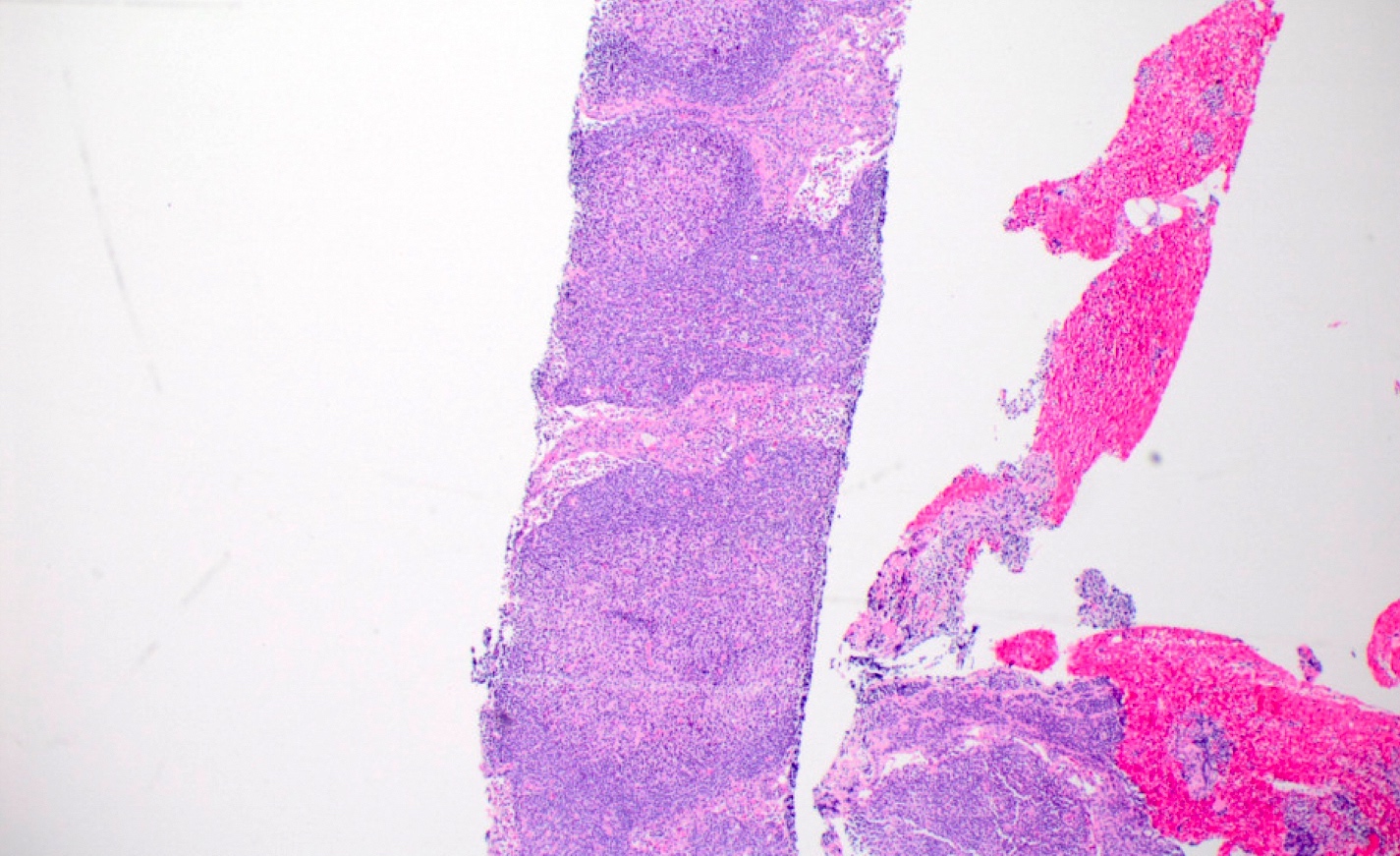
Contributed by Kyle Bradley, M.D.
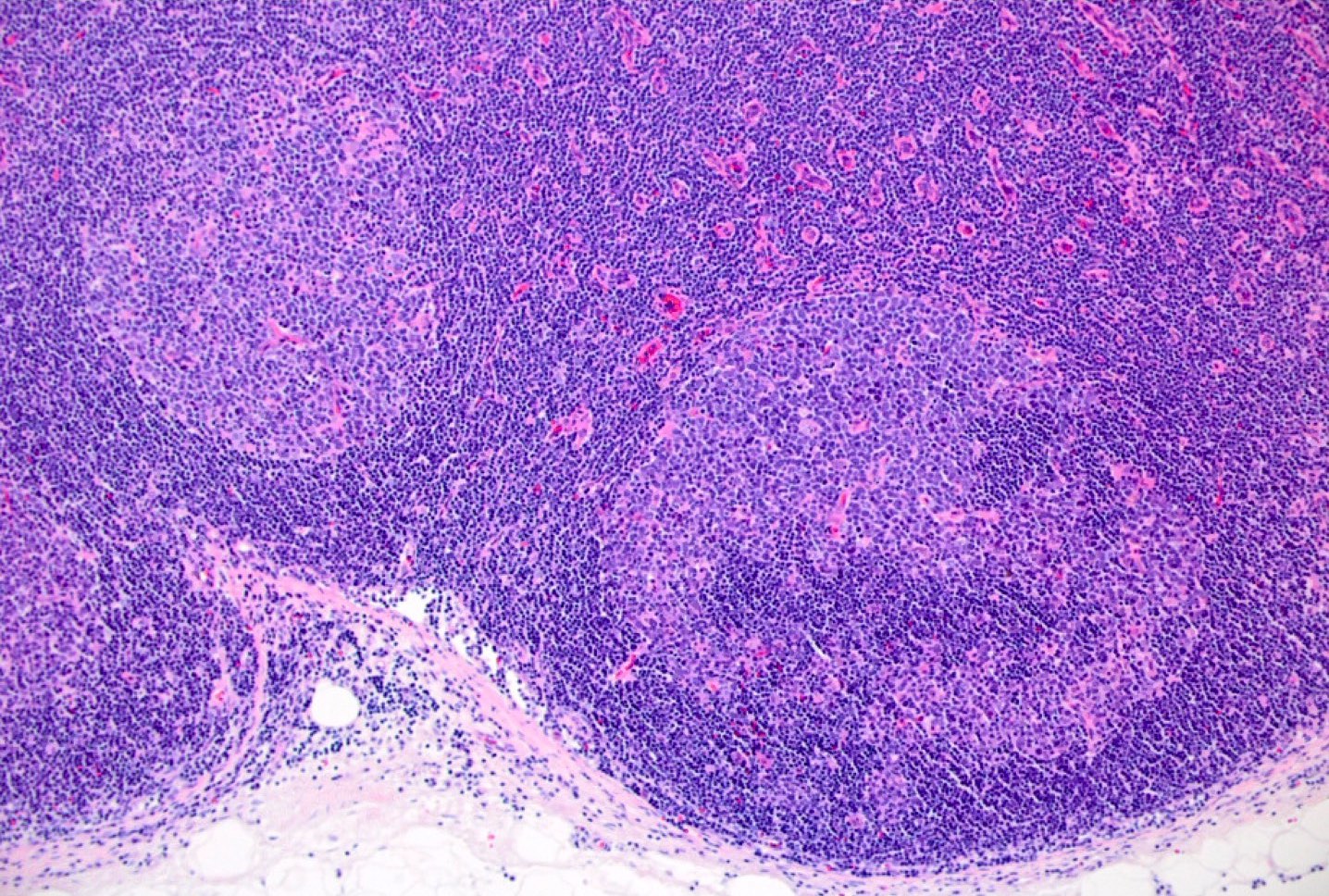
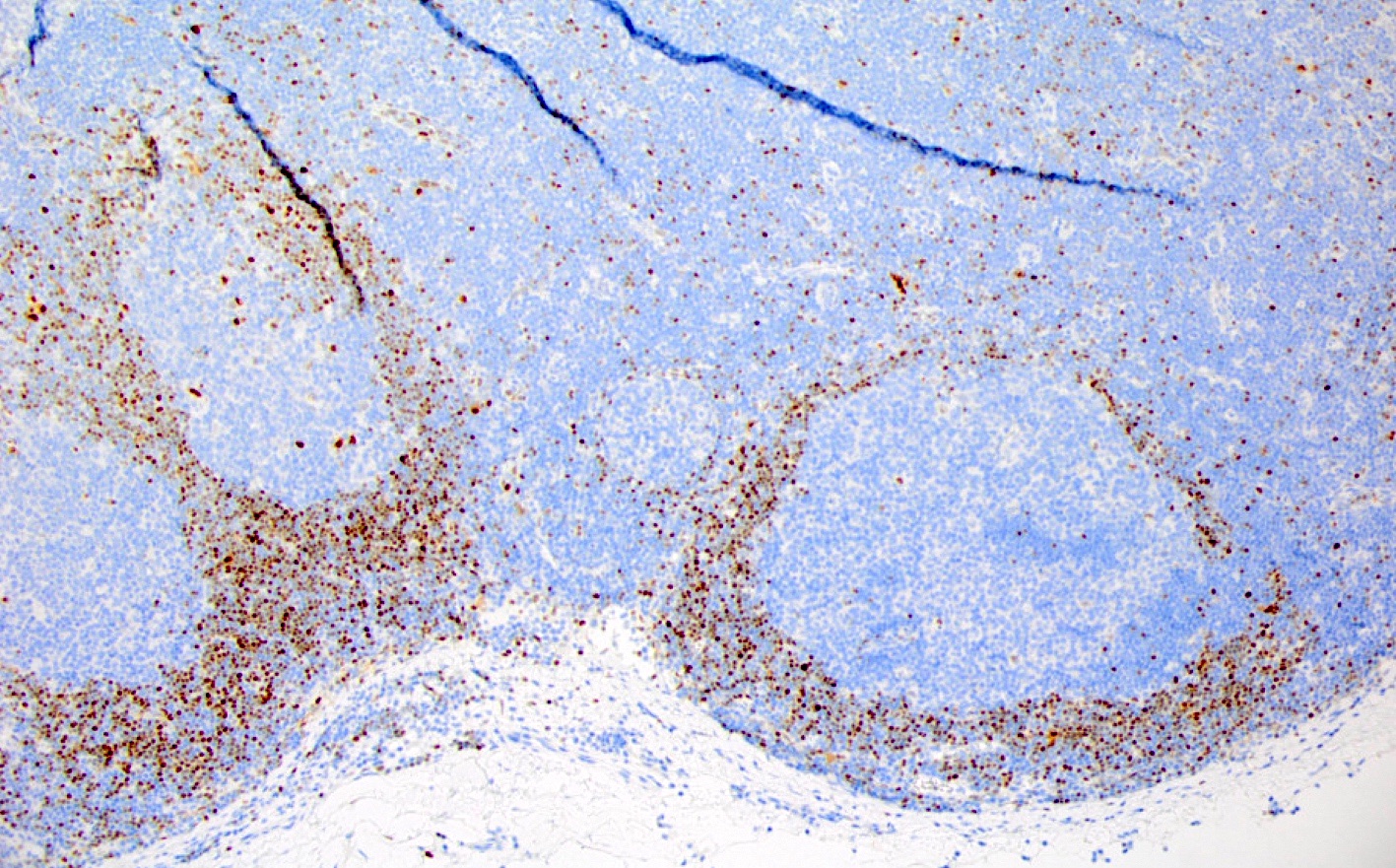
Mantle zone and interfollicular involvement
Early lymph node involvement by mantle cell lymphoma
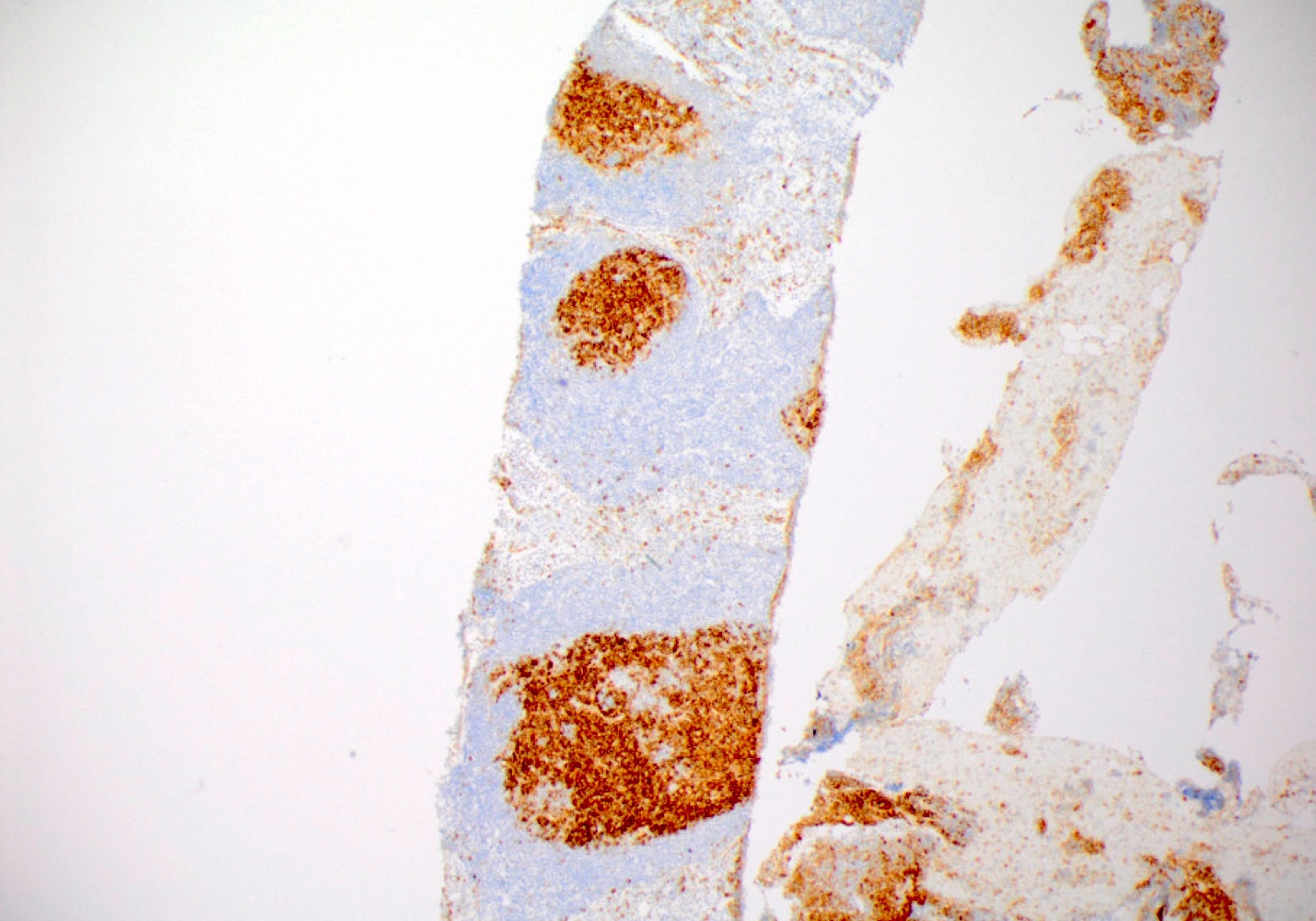
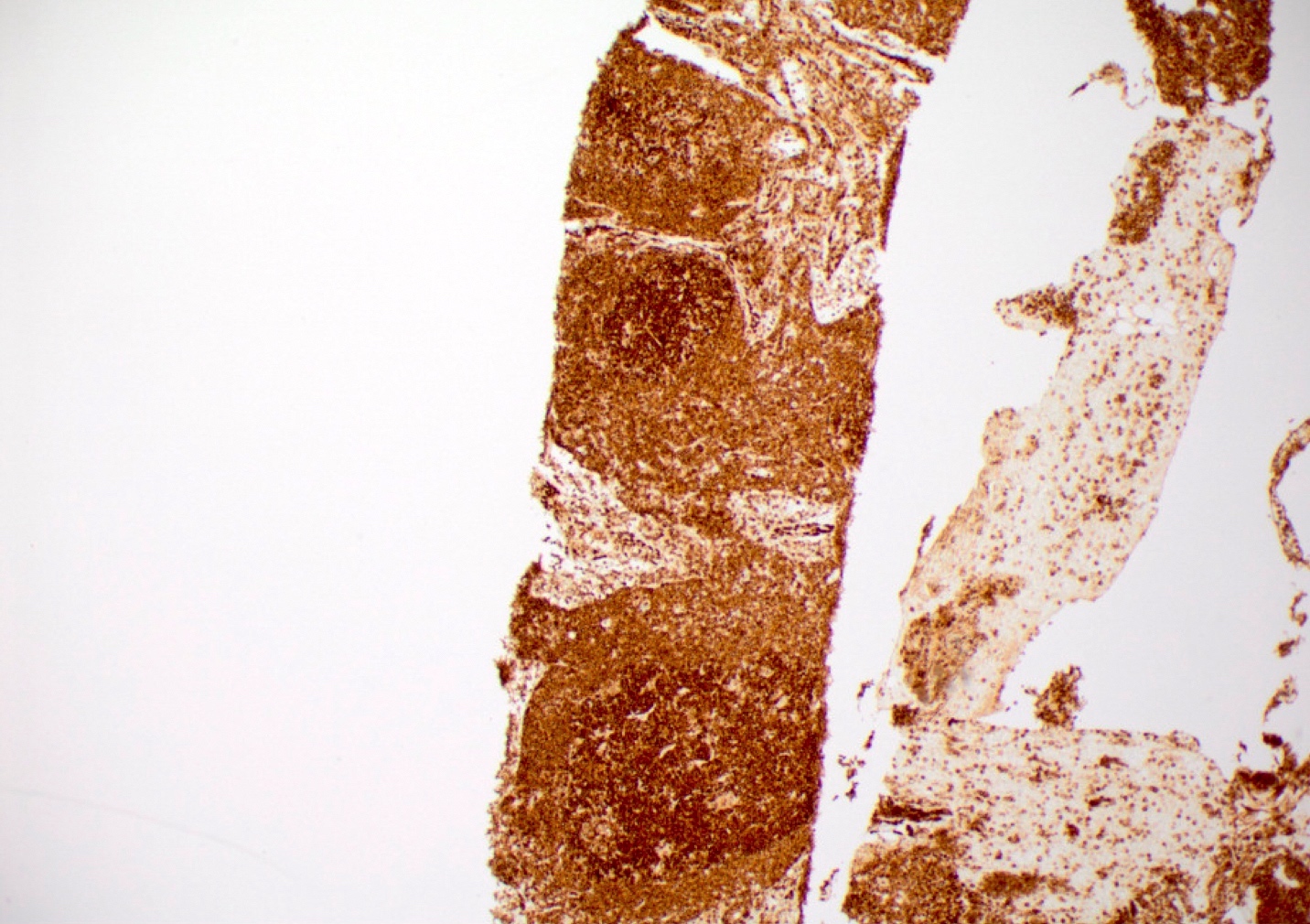
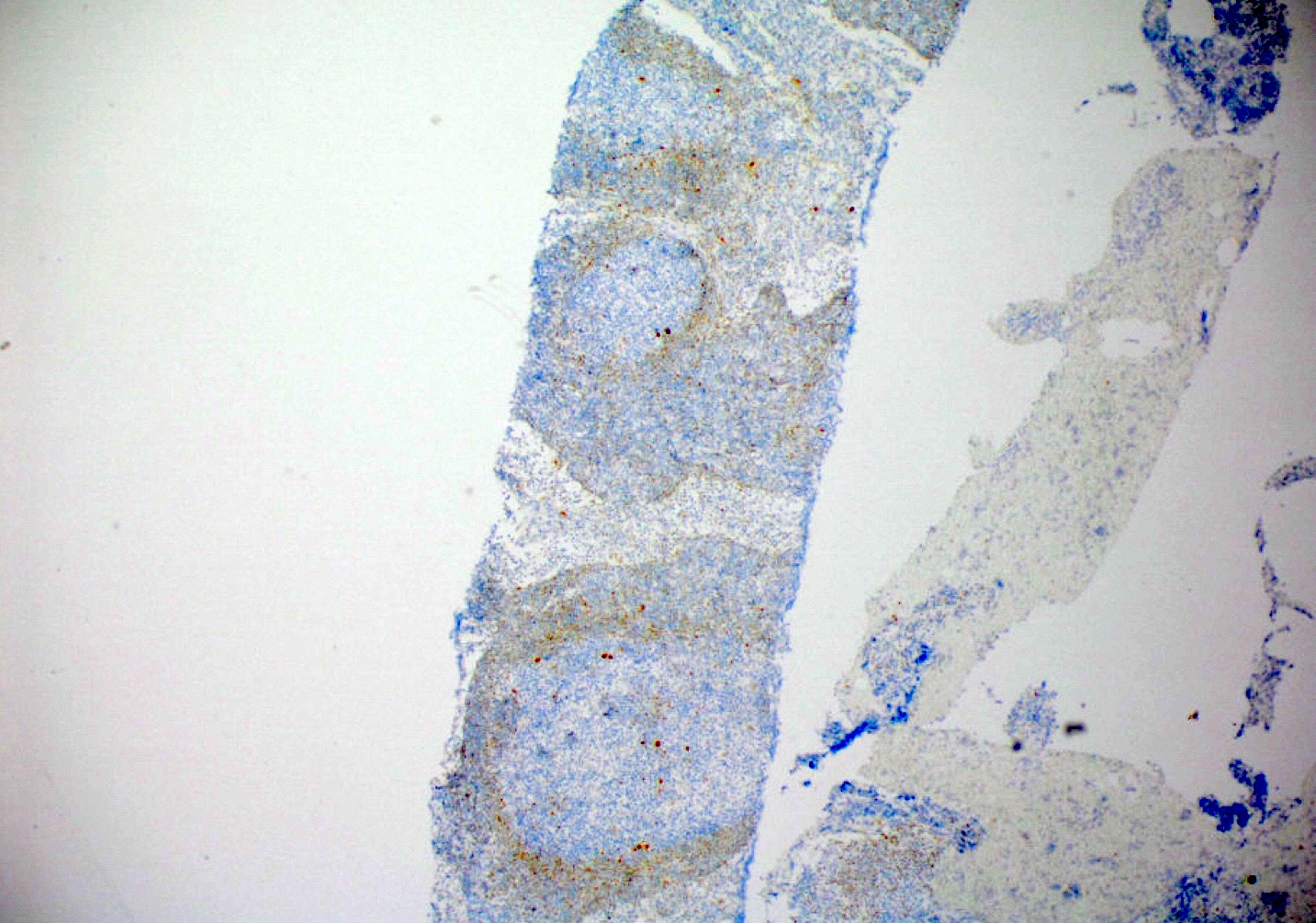
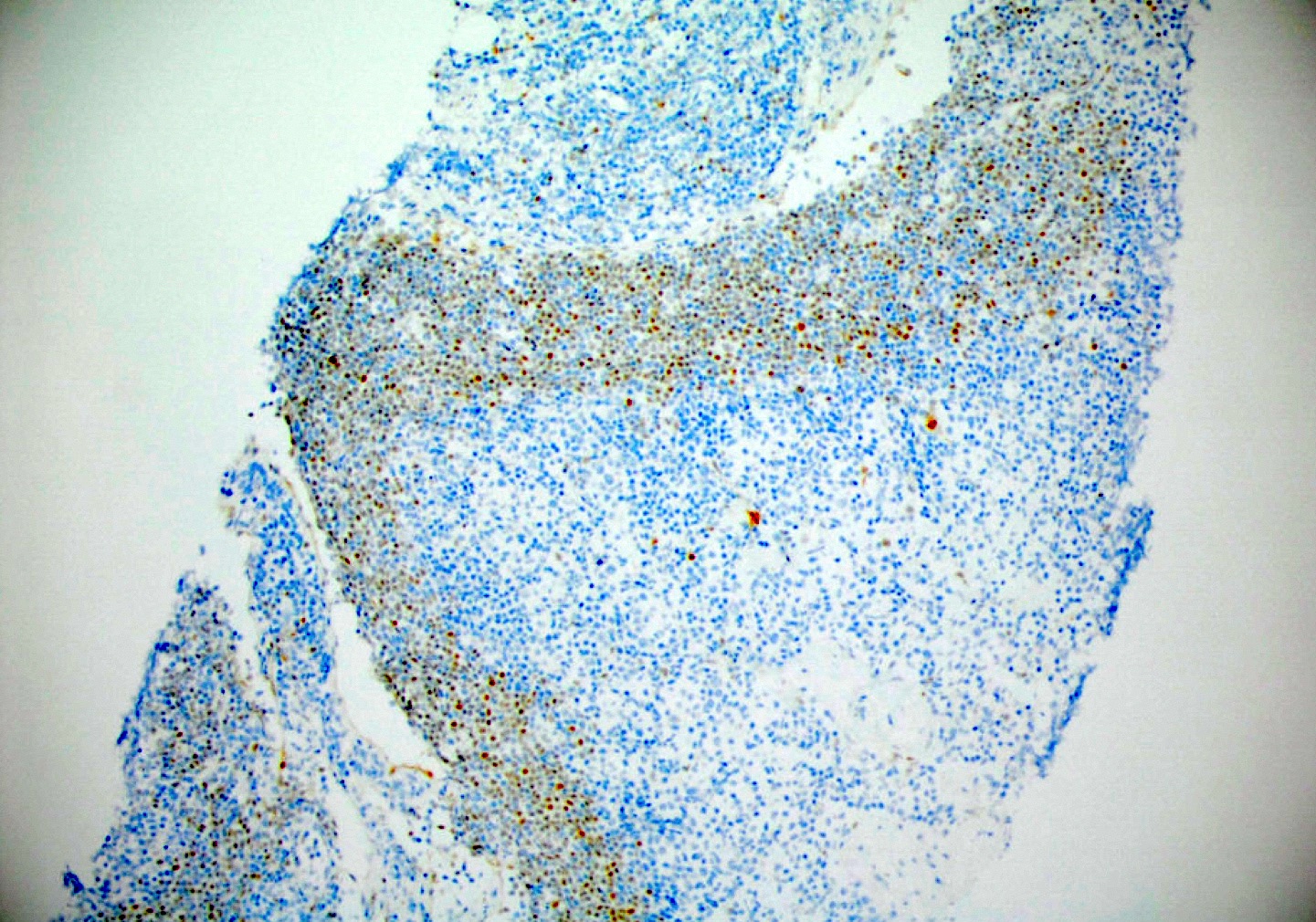
Follicular lymphoma with concurrent in situ mantle cell neoplasia
Positive stains
- B cell markers (e.g., CD20, PAX5, CD79a, BOB1, OCT2), cyclin D1, BCL2, IgD (J Hematop 2012;5:169)
- Usually CD5 and CD43
- More frequently CD5 negative and CD43 negative than overt mantle cell lymphoma (Semin Diagn Pathol 2018;35:76, J Hematop 2012;5:169)
- Variable SOX11
- 7/16 cases (44%) (Haematologica 2012;97:270)
- 100% (number of cases not clearly specified) (J Hematop 2012;5:169)
Flow cytometry description
- Clonal in situ mantle cell neoplasm cells may be detected by flow cytometry but this may require careful gating strategies due to the presence of nonclonal B cells present in involved lymph nodes
- Phenotype is indistinguishable from typical mantle cell lymphoma
- Reference: Am J Clin Pathol 2015;143:274
Molecular / cytogenetics description
- Characteristic translocation t(11;14) IGH::CCND1 results in overexpression of cyclin D1 (Virchows Arch 2016;468:245)
Sample pathology report
- Lymph node, right axilla, excision:
- In situ mantle cell neoplasm (see comment)
- Comment: The H&E stained sections show morphologic features consistent with a benign lymph node with follicular hyperplasia. A cyclin D1 immunohistochemical stain demonstrates cyclin D1 positive cells confined to the inner mantle zones of lymphoid follicles without mantle zone expansion. These findings are consistent with a diagnosis of in situ mantle cell neoplasm. In situ mantle cell neoplasm typically follows an indolent course; however, rare cases may progress to overt mantle cell lymphoma.
Differential diagnosis
- Mantle cell lymphoma with mantle zone growth pattern (Semin Diagn Pathol 2018;35:76):
- Expansion of the mantle zone, complete replacement of the mantle zone or significant extension into the interfollicular region or germinal centers by cyclin D1 positive B cells warrants a diagnosis of mantle cell lymphoma rather than in situ mantle cell neoplasm (Blood 2016;127:2375)
- Reactive follicular hyperplasia (Semin Diagn Pathol 2018;35:76):
- Reactive follicular hyperplasia lacks cyclin D1 positive cells within the mantle zones (Semin Diagn Pathol 2018;35:76)
Board review style question #1
In situ mantle cell neoplasm is characterized by which of the following translocations?
- t(8;14) MYC::IGH
- t(9;22) BCR::ABL1
- t(11;14) IGH::CCND1
- t(14;18) BCL2::IGH
Board review style answer #1
C. t(11;14) IGH::CCND1. The characteristic translocation of in situ mantle cell neoplasia is t(11;14) IGH::CCND1, resulting in overexpression of cyclin D1. Answer B is incorrect because t(9;22) BCR::ABL1 is the Philadelphia chromosome associated with AML, CML and B ALL. Answer D is incorrect because t(14;18) BCL2::IGH is associated with follicular lymphoma. Answer A is incorrect because t(8;14) MYC::IGH is associated with Burkitt lymphoma.
Comment Here
Reference: In situ mantle cell neoplasm
Comment Here
Reference: In situ mantle cell neoplasm
Board review style question #2
In a lymph node biopsy, which of the following features supports a diagnosis of in situ mantle cell neoplasm?
- Cyclin D1 positive B cells extending into the interfollicular region
- Mantle zones prominently expanded by cyclin D1 positive B cells
- Monoclonal proliferation of BCL2 positive B cells confined to germinal centers
- Preserved lymphoid architecture
Board review style answer #2
D. Preserved lymphoid architecture. In situ mantle cell neoplasm is characterized by cyclin D1 positive B cells restricted to the mantle zone of reactive appearing lymphoid tissue. Lymphoid architecture is preserved. Answers A and B are incorrect because prominent expansion of the mantle zone, complete replacement of the mantle zone or significant extension into the interfollicular region or germinal center by cyclin D1 positive B cells warrants a diagnosis of mantle cell lymphoma rather than in situ mantle cell neoplasm. Answer C is incorrect because a monoclonal proliferation of BCL2 positive B cells confined to germinal centers in a hyperplastic appearing lymphoid follicle is consistent with in situ follicular B cell neoplasm.
Comment Here
Reference: In situ mantle cell neoplasm
Comment Here
Reference: In situ mantle cell neoplasm
Board review style question #3
Which of the following is true of in situ mantle cell neoplasm?
- Characterized by aggressive behavior
- May be seen in extranodal locations
- Peripheral blood involvement is not permitted
- Usually progresses to overt mantle cell lymphoma
Board review style answer #3
B. May be seen in extranodal locations. In situ mantle cell neoplasm is a rare finding that is most commonly seen in lymph nodes but may be seen in extranodal locations. Answer C is incorrect because peripheral blood involvement is permitted. Answers A and D are incorrect because it is typically a stable disease with indolent behavior and infrequent (< 10%) progression to overt mantle cell lymphoma.
Comment Here
Reference: In situ mantle cell neoplasm
Comment Here
Reference: In situ mantle cell neoplasm
